
Profile of HIV-Infected Hispanics with Pancytopenia

Abstract
:1. Introduction
2. Experimental Section
2.1. Participants and Setting of the Study
2.2. Data Collection Methods and Definition of Pancytopenia and Other Variables Studied
2.3. Data Analysis
3. Results
3.1. Description of Participants of the Study and Prevalence of Hematological Disorders
3.2. Socio-Demographic, Immunological and Clinical Characteristics by Pancytopenia Status

{kind=link}
{kind=link}
| Variables | % |
|---|---|
| Males | 67.6 |
| Age, mean (SD) | 40.3 (10.1) |
| Intravenous drugs use | 34.9 |
| Unemployment | 73.9 |
| CD4 cell count <200 cells/μL | 41.0 |
| Clinical AIDS | 8.6 |
| ART use | 62.6 |
| Anemia | 38.2 |
| Leucopenia | 29.8 |
| Thrombocytopenia | 21.4 |
| Pancytopenia | 8.7 |
| Variables | Pancytopenia (n = 105) | No Pancytopenia (n = 1097) | p-Value |
|---|---|---|---|
| Males, % | 67.6 | 67.6 | 0.997 |
| Age, mean (SD) | 41.7 (8.9) | 40.1 (10.2) | 0.088 |
| Education, % | |||
| < HS | 35.6 | 30.9 | 0.606 |
| HS | 37.5 | 39.4 | |
| College | 26.9 | 29.7 | |
| Unemployment, % | 87.5 | 72.5 | 0.001 |
| Intravenous drugs use, % | 37.1 | 34.6 | 0.607 |
| Alcohol use, % | 56.7 | 50.0 | 0.187 |
| BMI, mean (SD) | 22.0 (4.0) | 25.1 (5.3) | < 0.001 |
| CD4 cell count, mean (SD) | 111.7 (140.7) | 345.1 (293.0) | < 0.001 |
| CD4 cell count (cells/μL), % | |||
| 0–100 | 68.4 | 23.1 | < 0.001 |
| 101–199 | 14.3 | 14.2 | |
| ≥200 | 17.3 | 62.7 | |
| HIV viral load (copies/mL), % | |||
| <10,000 | 10.0 | 35.3 | < 0.001 |
| 10,000–100,000 | 25.0 | 31.6 | |
| >100,000 | 65.0 | 33.1 | |
| Clinical AIDS, % | 24.8 | 7.0 | < 0.001 |
| ART use, % | 72.4 | 61.6 | 0.030 |
| Variables | ART+ | ART− | ||||
|---|---|---|---|---|---|---|
| Pancytopenia (n = 76) | No pancytopenia (n = 676) | p-Value | Pancytopenia (n = 29) | No Pancytopenia (n = 421) | p-Value | |
| BMI, mean (SD) | 22.5 (3.9) | 24.8 (4.9) | < 0.001 | 20.7 (4.7) | 25.8 (5.8) | < 0.001 |
| CD4 cell count, mean (SD) | 95.6 (100.4) | 256.7 (245.5) | < 0.001 | 167.6 (226.3) | 491.6 (306.5) | < 0.001 |
| CD4 cell count(cells/μL), % | ||||||
| 0–100 | 71.0 | 31.2 | < 0.001 | 59.1 | 9.6 | < 0.001 |
| 101–199 | 14.5 | 18.2 | 13.6 | 7.7 | ||
| ≥200 | 14.5 | 50.6 | 27.3 | 82.7 | ||
| HIV viral load (copies/mL), % | ||||||
| <10,000 | 9.3 | 30.2 | < 0.001 | 12.0 | 43.6 | < 0.001 |
| 10,000–100,000 | 24.0 | 28.9 | 28.0 | 36.2 | ||
| >100,000 | 66.7 | 40.9 | 60.0 | 20.2 | ||
| Clinical AIDS, % | 17.1 | 8.3 | 0.012 | 44.8 | 5.0 | < 0.001 |
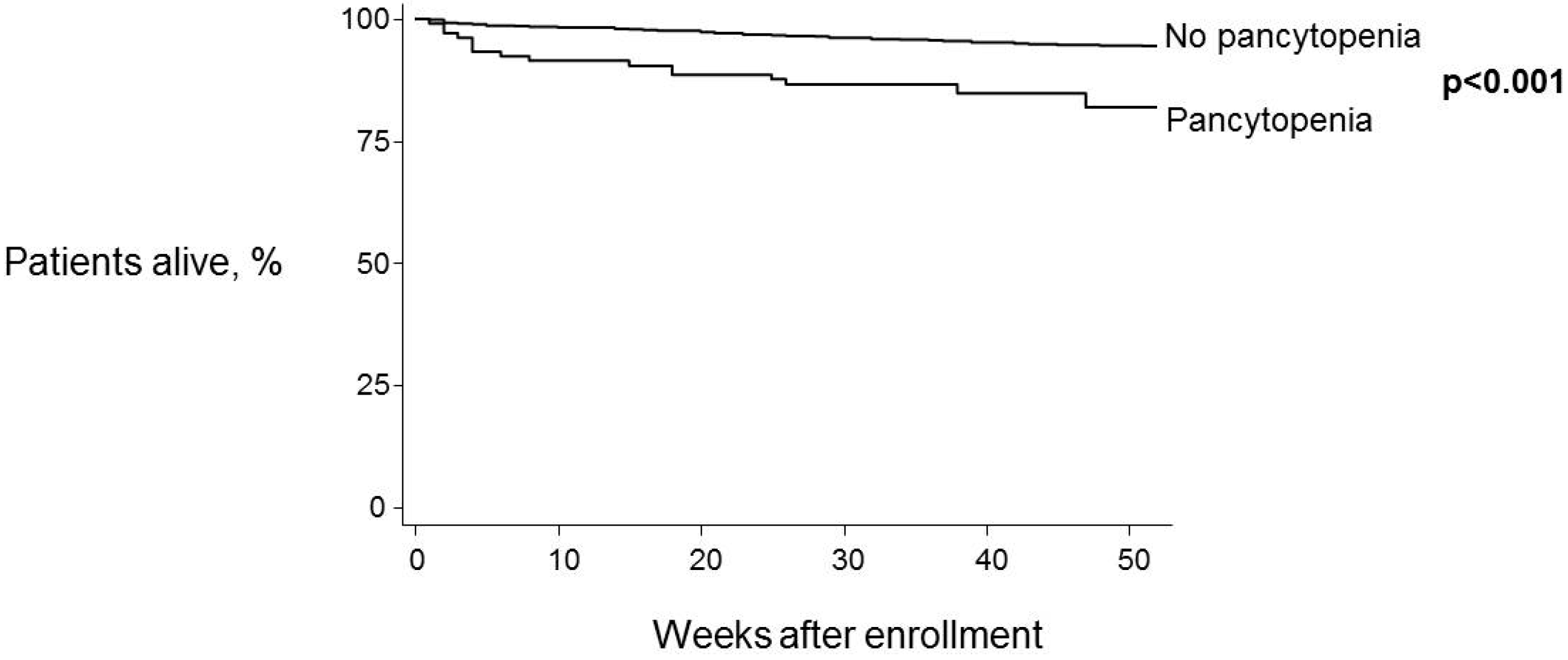
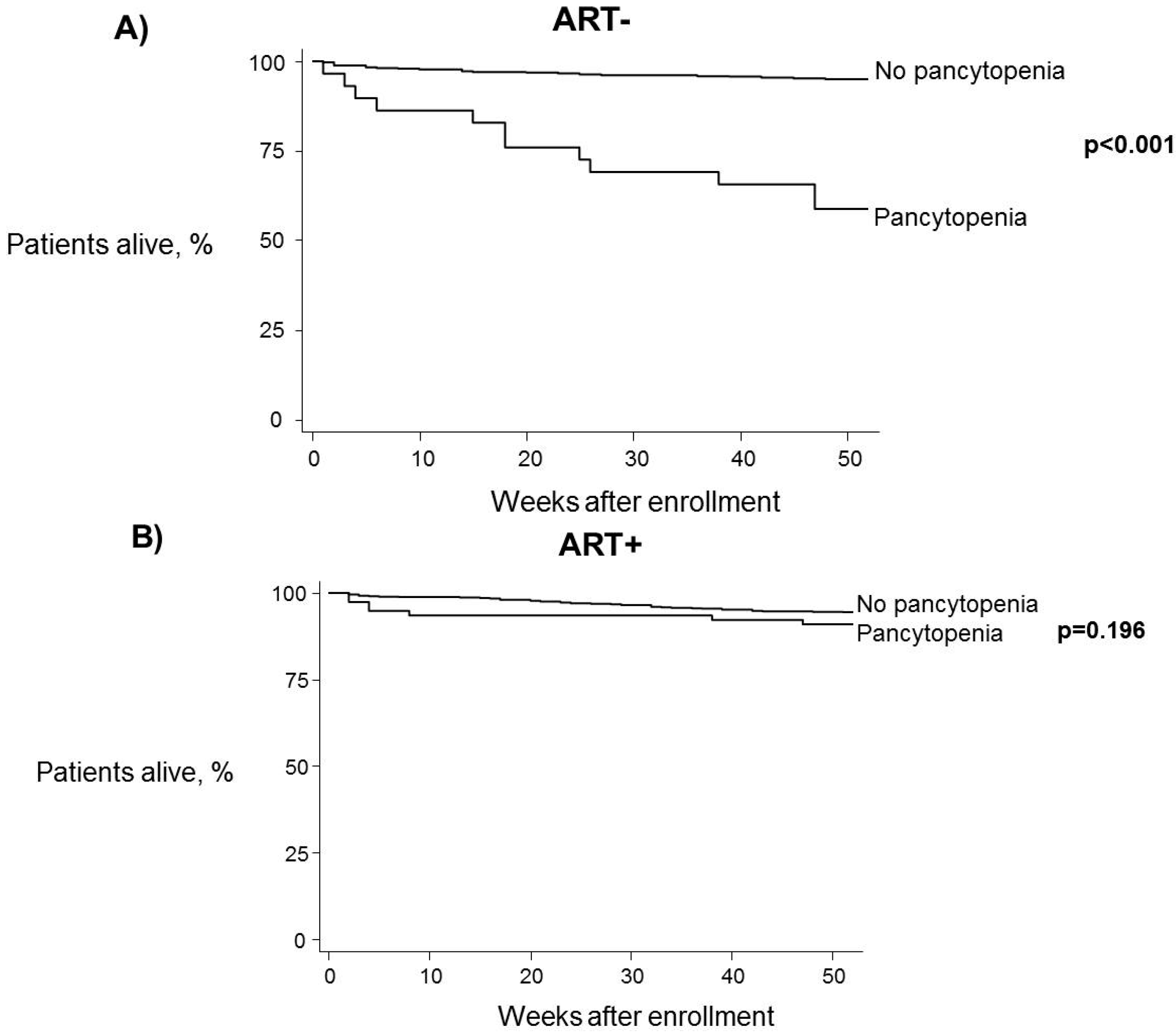
3.3. Relationship between One-Year Mortality, Pancytopenia and ART


4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Jain, A.; Naniwadekar, M. An etiological reappraisal of pancytopenia—Largest series reported to date from a single tertiary care teaching hospital. BMC Hematol. 2013, 11. [Google Scholar] [CrossRef] [PubMed]
- Kyeyune, R.; Saathoff, E.; Ezeamama, A.E.; Loscher, T.; Fawzi, W.; Guwatudde, D. Prevalence and correlates of cytopenias in HIV-infected adults initiating highly active antiretroviral therapy in Uganda. BMC Infect. Dis. 2014, 9. [Google Scholar] [CrossRef] [PubMed]
- Zell, S.C.; Peterson, K. Long-term remission of HIV-associated thrombocytopenia parallels ongoing suppression of viral replication. West. J. Med. 1997, 167, 433–435. [Google Scholar] [PubMed]
- Evans, R.H.; Scadden, D.T. Haematological aspects of HIV infection. Baillieres Best Pract. Res. Clin. Haematol. 2000, 13, 215–230. [Google Scholar] [CrossRef] [PubMed]
- Sultan, J.; Gaur, S.; Sandhaus, L.; Frenkel, L.D.; Ettinger, L.J. Human immunodeficiency virus infection presenting as pancytopenia in an infant. Am. J. Pediatr. Hematol. Oncol. 1994, 16, 334–337. [Google Scholar] [PubMed]
- Enawgaw, B.; Alem, M.; Addis, Z.; Melku, M. Determination of hematological and immunological parameters among HIV positive patients taking highly active antiretroviral treatment and treatment naive in the antiretroviral therapy clinic of Gondar University Hospital, Gondar, Northwest Ethiopia: A comparative cross-sectional study. BMC Hematol. 2014, 3. [Google Scholar] [CrossRef]
- Spivak, J.L.; Selonick, S.E.; Quinn, T.C. Acquired immune deficiency syndrome and pancytopenia. J. Am. Med. Assoc. 1983, 250, 3084–3087. [Google Scholar] [CrossRef]
- Spivak, J.L.; Bender, B.S.; Quinn, T.C. Hematologic abnormalities in the acquired immune deficiency syndrome. Am. J. Med. 1984, 77, 224–228. [Google Scholar] [CrossRef]
- Zota, V.; Braza, J.; Pantanowitz, L.; Dezube, B.J.; Pihan, G. A 57-year-old HIV-positive man with persistent fever, weight loss, and pancytopenia. Am. J. Hematol. 2009, 84, 443–446. [Google Scholar] [CrossRef] [PubMed]
- Dikshit, B.; Wanchu, A.; Sachdeva, R.K.; Sharma, A.; Das, R. Profile of hematological abnormalities of Indian HIV infected individuals. BMC Blood Disord. 2009, 8. [Google Scholar] [CrossRef] [PubMed]
- Firnhaber, C.; Smeaton, L.; Saukila, N.; Flanigan, T.; Gangakhedkar, R.; Kumwenda, J.; la Rosa, A.; Kumarasamy, N.; de Gruttola, V.; Hakim, J.G.; et al. Comparisons of anemia, thrombocytopenia, and neutropenia at initiation of HIV antiretroviral therapy in Africa, Asia, and the Americas. Int. J. Infect. Dis. 2010, 14, e1088–e1092. [Google Scholar] [CrossRef] [PubMed]
- Santiago-Rodriguez, E.J.; Mayor, A.M.; Fernandez-Santos, D.M.; Ruiz-Candelaria, Y.; Hunter-Mellado, R.F. Anemia in a cohort of HIV-infected Hispanics: Prevalence, associated factors and impact on one-year mortality. BMC Res. Notes 2014, 7. [Google Scholar] [CrossRef] [PubMed]
- Zon, L.I.; Arkin, C.; Groopman, J.E. Haematologic manifestations of the human immune deficiency virus (HIV). Br. J. Haematol. 1987, 66, 251–256. [Google Scholar] [CrossRef] [PubMed]
- De Santis, G.C.; Brunetta, D.M.; Vilar, F.C.; Brandao, R.A.; de Albernaz Muniz, R.Z.; de Lima, G.M.; Amorelli-Chacel, M.E.; Covas, D.T.; Machado, A.A. Hematological abnormalities in HIV-infected patients. Int. J. Infect. Dis. 2011, 15, e808–e811. [Google Scholar] [CrossRef] [PubMed]
- Kulkosky, J.; Bouhamdan, M.; Geist, A.; Nunnari, G.; Phinney, D.G.; Pomerantz, R.J. Pathogenesis of HIV-1 infection within bone marrow cells. Leuk. Lymphoma 2000, 37, 497–515. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, P.S.; Hanson, D.L.; Chu, S.Y.; Jones, J.L.; Ward, J.W. Epidemiology of anemia in human immunodeficiency virus (HIV)-infected persons: Results from the multistate adult and adolescent spectrum of HIV disease surveillance project. Blood 1998, 91, 301–308. [Google Scholar] [PubMed]
- Mocroft, A.; Kirk, O.; Barton, S.E.; Dietrich, M.; Proenca, R.; Colebunders, R.; Pradier, C.; Monforte, A.A.; Ledergerber, B.; Lundgren, J.D. Anaemia is an independent predictive marker for clinical prognosis in HIV-infected patients from across Europe. AIDS 1999, 13, 943–950. [Google Scholar] [CrossRef] [PubMed]
- Johannessen, A.; Naman, E.; Ngowi, B.J.; Sandvik, L.; Matee, M.I.; Aglen, H.E.; Gundersen, S.G.; Bruun, J.N. Predictors of mortality in HIV-infected patients starting antiretroviral therapy in a rural hospital in Tanzania. BMC Infect. Dis. 2008, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santiago-Rodríguez, E.J.; Mayor, A.M.; Fernández-Santos, D.M.; Hunter-Mellado, R.F. Profile of HIV-Infected Hispanics with Pancytopenia. Int. J. Environ. Res. Public Health 2016, 13, 38. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13010038
Santiago-Rodríguez EJ, Mayor AM, Fernández-Santos DM, Hunter-Mellado RF. Profile of HIV-Infected Hispanics with Pancytopenia. International Journal of Environmental Research and Public Health. 2016; 13(1):38. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13010038
Chicago/Turabian StyleSantiago-Rodríguez, Eduardo J., Angel M. Mayor, Diana M. Fernández-Santos, and Robert F. Hunter-Mellado. 2016. "Profile of HIV-Infected Hispanics with Pancytopenia" International Journal of Environmental Research and Public Health 13, no. 1: 38. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13010038