
Associations of Breast Cancer Risk Factors with Premenopausal Sex Hormones in Women with Very Low Breast Cancer Risk

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Hormone Assays
2.4. Statistical Analysis
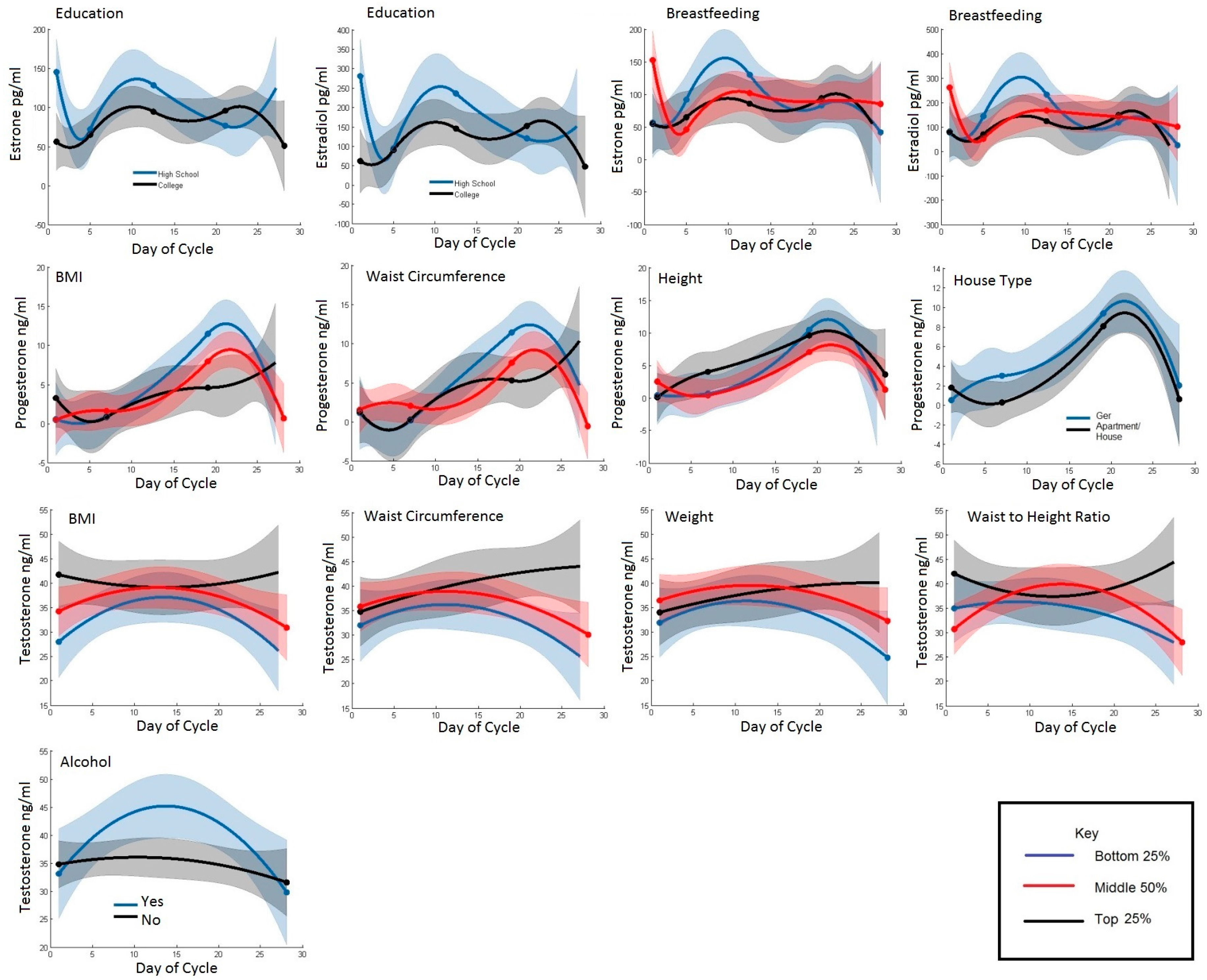
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Ervik, M.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. GlOBOCAN 2012 v 1.0, Cancer Incidence and Mortality Worldwide. IARC CancerBase No. 11 [Internet]; International Agency for Research on Cancer: Lyon, France, 2013. [Google Scholar]
- Troisi, R.; Altantsetseg, D.; Davaasambuu, G.; Rich-Edwards, J.; Davaalkham, D.; Tretli, S.; Hoover, R.N.; Frazier, A.L. Breast cancer incidence in Mongolia. Cancer Causes Control 2012, 23, 1047–1053. [Google Scholar] [CrossRef] [PubMed]
- Ghiasvand, R.; Adami, H.O.; Harirchi, I.; Akrami, R.; Zendehdel, K. Higher incidence of premenopausal breast cancer in less developed countries; myth or truth? BMC Cancer 2014. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, R.G.; Hoover, R.N.; Pike, M.C.; Hildesheim, A.; Nomura, A.M.; West, D.W.; Wu-Williams, A.H.; Kolonel, L.N.; Horn-Ross, P.L.; Rosenthal, J.F.; et al. Migration patterns and breast cancer risk in Asian-American women. J. Natl. Cancer Inst. 1993, 85, 1819–1827. [Google Scholar] [CrossRef] [PubMed]
- Kaaks, R.; Berrino, F.; Key, T.; Rinaldi, S.; Dossus, L.; Biessy, C.; Secreto, G.; Amiano, P.; Bingham, S.; Boeing, H.; et al. Serum sex steroids in premenopausal women and breast cancer risk within the European Prospective Investigation into Cancer and Nutrition (EPIC). J. Natl. Cancer Inst. 2005, 97, 755–765. [Google Scholar] [CrossRef] [PubMed]
- Key, T.J.; Appleby, P.N.; Reeves, G.K.; Travis, R.C.; Alberg, A.J.; Barricarte, A.; Berrino, F.; Krogh, V.; Sieri, S.; Brinton, L.A.; et al. Sex hormones and risk of breast cancer in premenopausal women: A collaborative reanalysis of individual participant data from seven prospective studies. Lancet Oncol. 2013, 14, 1009–1019. [Google Scholar] [PubMed]
- Yoshimoto, N.; Nishiyama, T.; Toyama, T.; Takahashi, S.; Shiraki, N.; Sugiura, H.; Endo, Y.; Iwasa, M.; Fujii, Y.; Yamashita, H. Genetic and environmental predictors, endogenous hormones and growth factors, and risk of estrogen receptor-positive breast cancer in Japanese women. Cancer Sci. 2011, 102, 2065–2072. [Google Scholar] [CrossRef] [PubMed]
- Dai, Q.; Franke, A.A.; Yu, H.; Shu, X.O.; Jin, F.; Hebert, J.R.; Custer, L.J.; Gao, Y.T.; Zheng, W. Urinary phytoestrogen excretion and breast cancer risk: Evaluating potential effect modifiers endogenous estrogens and anthropometrics. Cancer Epidemiol. Biomarkers Prev. 2003, 12, 497–502. [Google Scholar] [PubMed]
- Eliassen, A.H.; Missmer, S.A.; Tworoger, S.S.; Spiegelman, D.; Barbieri, R.L.; Dowsett, M.; Hankinson, S.E. Endogenous steroid hormone concentrations and risk of breast cancer among premenopausal women. J. Natl. Cancer Inst. 2006, 98, 1406–1415. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, L.; Yuan, J.M.; Ross, R.K.; Pike, M.C.; Hanisch, R.; Lobo, R.; Stanczyk, F.; Gao, Y.T.; Henderson, B.E. Serum hormone levels in pre-menopausal Chinese women in Shanghai and white women in Los Angeles: Results from two breast cancer case-control studies. Cancer Causes Control 1990, 1, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Key, T.J.; Chen, J.; Wang, D.Y.; Pike, M.C.; Boreham, J. Sex hormones in women in rural China and in Britain. Br. J. Cancer 1990, 62, 631–636. [Google Scholar] [CrossRef] [PubMed]
- Goldin, B.R.; Adlercreutz, H.; Gorbach, S.L.; Woods, M.N.; Dwyer, J.T.; Conlon, T.; Bohn, E.; Gershoff, S.N. The relationship between estrogen levels and diets of caucasian American and oriental immigrant women. Am. J. Clin. Nutr. 1986, 44, 945–953. [Google Scholar] [PubMed]
- Hoover, R.N. That recognised risk factors can explain past and present international differences in breast cancer incidence: Misconceptions 5. Br. J. Cancer 2012, 107, 408–410. [Google Scholar] [CrossRef] [PubMed]
- Ganmaa, D.; Rich-Edwards, J.W.; Frazier, L.A.; Davaalkham, D.; Oyunbileg, G.; Janes, C.; Potischman, N.; Hoover, R.; Troisi, R. A comparison of migrants to, and women born in, urban Mongolia: Demographic, reproductive, anthropometric and lifestyle characteristics. Int. Health 2013, 5, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Troisi, R.; Ganmaa, D.; dos Santos Silva, I.; Davaalkham, D.; Rosenberg, P.S.; Rich-Edwards, J.; Frasier, L.; Houghton, L.; Janes, C.; Stanczyk, F.; et al. The role of hormones in the differences in the incidence of breast cancer between Mongolia and the United Kingdom. PLoS ONE 2014, 9, e114455. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Global Physical Activity Questionnaire. Available online: http://www.who.int/chp/steps/GPAQ/en/index.html (accessed on 27 June 2008).
- Goebelsmann, U.; Horton, R.; Mestman, J.H.; Arce, J.J.; Nagata, Y.; Nakamura, R.M.; Thorneycroft, I.H.; Mishell, D.R., Jr. Male pseudohermaphroditism due to testicular 17-hydroxysteroid dehydrogenase deficiency. J. Clin. Endocrinol. Metab. 1973, 36, 867–879. [Google Scholar] [CrossRef] [PubMed]
- Goebelsmann, U.; Bernstein, G.S.; Gale, J.A.; Kletzky, O.A.; Nakamura, R.M.; Coulson, A.H.; Korelitz, J.J. Serum Gonadotropin, Testosterone, Estradiol and Estrone Levels Prior to and Following Bilateral Vasectomy; Academic Press: New York, NY, USA, 1979. [Google Scholar]
- Probst-Hensch, N.M.; Ingles, S.A.; Diep, A.T.; Haile, R.W.; Stanczyk, F.Z.; Kolonel, L.N.; Henderson, B.E. Aromatase and breast cancer susceptibility. Endocr. Relat. Cancer 1999, 6, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Hastie, T.; Tibshirani, R.; Friedman, J.H. The Elements of Statistical Learning: Data Mining, Inference, and Prediction; Springer: New York, NY, USA, 2001. [Google Scholar]
- Randolph, J.F., Jr.; Sowers, M.; Bondarenko, I.V.; Harlow, S.D.; Luborsky, J.L.; Little, R.J. Change in estradiol and follicle-stimulating hormone across the early menopausal transition: Effects of ethnicity and age. J. Clin. Endocrinol. Metab. 2004, 89, 1555–1561. [Google Scholar] [CrossRef] [PubMed]
- Hankinson, S.E.; Eliassen, A.H. Circulating sex steroids and breast cancer risk in premenopausal women. Horm. Cancer 2010, 1, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Nagata, C.; Wada, K.; Nakamura, K.; Hayashi, M.; Takeda, N.; Yasuda, K. Associations of body size and reproductive factors with circulating levels of sex hormones and prolactin in premenopausal Japanese women. Cancer Causes Control 2011, 22, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Fortner, R.T.; Hankinson, S.E.; Schairer, C.; Xu, X.; Ziegler, R.G.; Eliassen, A.H. Association between reproductive factors and urinary estrogens and estrogen metabolites in premenopausal women. Cancer Epidemiol. Biomarkers Prev. 2012, 21, 959–968. [Google Scholar] [CrossRef] [PubMed]
- Tworoger, S.S.; Eliassen, A.H.; Missmer, S.A.; Baer, H.; Rich-Edwards, J.; Michels, K.B.; Barbieri, R.L.; Dowsett, M.; Hankinson, S.E. Birthweight and body size throughout life in relation to sex hormones and prolactin concentrations in premenopausal women. Cancer Epidemiol. Biomarkers Prev. 2006, 15, 2494–2501. [Google Scholar] [CrossRef] [PubMed]
- Sowers, M.F.; Beebe, J.L.; McConnell, D.; Randolph, J.; Jannausch, M. Testosterone concentrations in women aged 25–50 years: Associations with lifestyle, body composition, and ovarian status. Am. J. Epidemiol. 2001, 153, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Kirschner, M.A.; Samojlik, E.; Drejka, M.; Szmal, E.; Schneider, G.; Ertel, N. Androgen-estrogen metabolism in women with upper body versus lower body obesity. J. Clin. Endocrinol. Metab. 1990, 70, 473–479. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | N | Mean (SD) or Percent | Min | Max |
|---|---|---|---|---|
| Lifestyle and Demographic | ||||
| Age (y) | 314 | 34.9 (4.8) | 24.0 | 45.0 |
| Education | ||||
| Some/graduated high school | 110 | 35% | ||
| Some/graduated college | 204 | 65% | ||
| House Type | ||||
| Ger (yurt) | 103 | 33% | ||
| Apartment or House | 211 | 67% | ||
| Previously lived as nomad | 41 | 13% | ||
| Physical Activity Level | ||||
| Low | 52 | 16.6% | ||
| Moderate | 77 | 24.5% | ||
| Vigorous | 184 | 58.6% | ||
| Ever Smokers | 54 | 17.2% | ||
| Consume Alcohol | 70 | 22.3% | ||
| Reproductive | ||||
| Age at menarche (y) | 314 | 14.8 (1.5) | 11.0 | 20.0 |
| Total number of months breastfed | 314 | 39.2 (30.7) | 0.0 | 168 |
| Average months breastfed each child | 314 | 19.3 (13.9) | 0.0 | 72.0 |
| Anthropometrics | ||||
| Weight (kg) | 314 | 62.6 (12.0) | 35.8 | 119 |
| Height (cm) | 314 | 157.2 (5.6) | 138.6 | 172 |
| Body mass index (kg/m2) | 314 | 25.3 (4.5) | 16.4 | 46.3 |
| Waist circumference (cm) | 314 | 81.7 (11.0) | 57.0 | 121 |
| Weight at 18 (kg) | 313 | 54.4 (7.6) | 37.0 | 78.0 |
| BMI at 18 (kg/m2) | 313 | 22.0 (3.1) | 15.2 | 34.8 |
| Hormones | ||||
| Androstenedione (ng/mL) | 314 | 1.0 (0.4) | 0.3 | 2.50 |
| Testosterone (ng/dL) | 314 | 32.1 (13.6) | 9.9 | 103 |
| Progesterone (ng/mL) | 297 | 5.1 (6.9) | 0.1 | 33.3 |
| Estrone (pg/mL) | 314 | 85.1 (50.1) | 18.5 | 458 |
| Estradiol (pg/mL) | 314 | 133 (103) | 7.5 | 995 |
| Characteristic | n | Androstenedione ng/mL | Testosterone ng/dL | Progesterone ng/mL | Estrone pg/mL | Estradiol pg/mL |
|---|---|---|---|---|---|---|
| Lifestyle and Demographic | ||||||
| Age (Years) | ||||||
| 24–31 | 61 | 1.2 (0.05) | 35.0 (1.8) | 1.1 (0.9) | 90.4 (10.5) | 147 (24) |
| 31–39 | 174 | 0.9 (0.05) | 29.8 (1.9) | 2.3 (1.1) | 94.5 (14.1) | 165 (32) |
| 39–45 | 79 | 0.7 (0.06) | 25.3 (2.0) | 2.4 (1.0) | 90.0 (11.6) | 151 (26) |
| p | <0.01 | <0.01 | 0.36 | 0.89 | 0.69 | |
| Education | ||||||
| High School | 110 | 1.2 (0.06) | 35.7 (2.2) | 2.1 (1.2) | 105 (16) | 178 (35) |
| College | 204 | 1.1 (0.05) | 33.6 (1.6) | 1.0 (0.8) | 84.3 (9.1) | 131 (21) |
| p | 0.22 | 0.20 | 0.13 | 0.02 | 0.02 | |
| House Type | ||||||
| Ger | 103 | 1.1 (0.07) | 35.0 (2.3) | 2.5 (1.3) | 97.1 (16.2) | 164 (37) |
| Apartment/House | 211 | 1.1 (0.05) | 34.1 (1.7) | 1.1 (0.8) | 91.5 (9.5) | 146 (22) |
| p | 0.53 | 0.62 | 0.08 | 0.56 | 0.42 | |
| Previously lived as Nomad | ||||||
| No | 41 | 1.1 (0.06) | 34.4 (2.0) | 1.5 (1.2) | 95.1 (14.8) | 156 (34) |
| Yes | 273 | 1.1 (0.07) | 34.6 (2.3) | 0.4 (1.1) | 78.6 (12.8) | 118 (29) |
| p | 0.44 | 0.92 | 0.29 | 0.20 | 0.19 | |
| Physical Activity Level | ||||||
| Low | 52 | 1.1 (0.08) | 34.4 (2.6) | 0.5 (1.4) | 84.2 (17.3) | 134 (39) |
| Moderate | 77 | 1.1 (0.07) | 34.7 (2.4) | 2.0 (1.1) | 98.9 (13.9) | 160 (31) |
| Vigorous | 184 | 1.1 (0.06) | 34.3 (2.1) | 1.6 (1.0) | 94.7 (12.0) | 156 (27) |
| p | 0.99 | 0.98 | 0.38 | 0.56 | 0.66 | |
| Smoking | ||||||
| No | 260 | 1.1 (0.06) | 34.2 (2.1) | 1.4 (1.0) | 93.5 (11.8) | 151 (27) |
| Yes | 54 | 1.1 (0.08) | 35.2 (2.6) | 1.8 (1.4) | 91.6 (17.9) | 157 (41) |
| p | 0.97 | 0.64 | 0.71 | 0.87 | 0.81 | |
| Alcohol | ||||||
| No | 244 | 1.2 (0.07) | 38.3 (2.5) | 1.3 (1.3) | 104 (17) | 160 (39) |
| Yes | 70 | 1.1 (0.05) | 33.4 (1.8) | 1.5 (0.9) | 90.9 (10.5) | 150 (24) |
| p | 0.01 | 0.01 | 0.87 | 0.22 | 0.68 | |
| Anthropometrics | ||||||
| Weight (kg) | ||||||
| 36–55 | 81 | 1.1 (0.05) | 31.2 (1.9) | 2.0 (0.9) | 87.8 (10.6) | 153 (24) |
| 55–70 | 159 | 1.2 (0.06) | 35.6 (2.1) | 1.8 (1.2) | 98.3 (15.5) | 163 (35) |
| 70+ | 74 | 1.1 (0.06) | 35.5 (1.9) | 0.4 (0.9) | 90.4 (11.0) | 132 (25) |
| p | 0.18 | 0.05 | 0.23 | 0.56 | 0.45 | |
| Height (cm) | ||||||
| 139–153 | 75 | 1.2 (0.06) | 35.3 (1.9) | 1.6 (0.9) | 91.4 (10.8) | 148 (25) |
| 153–161 | 161 | 1.1 (0.06) | 32.6 (2.1) | 0.6 (1.2) | 91.7 (15.5) | 149 (35) |
| 161+ | 78 | 1.2 (0.06) | 36.3 (1.9) | 2.4 (0.9) | 95.9 (10.9) | 157 (25) |
| p | 0.06 | 0.11 | 0.12 | 0.92 | 0.94 | |
| Body mass index (kg/m2) | ||||||
| 16–22 | 48 | 1.1 (0.05) | 31.1 (1.8) | 2.4 (0.9) | 91.0 (10.6) | 153 (24) |
| 22–28 | 218 | 1.1 (0.06) | 34.7 (2.1) | 1.3 (1.2) | 85.7 (15.5) | 138 (35) |
| 28+ | 48 | 1.2 (0.06) | 38.4 (1.9) | 0.8 (0.9) | 107 (11) | 171 (25) |
| p | 0.26 | <0.01 | 0.25 | 0.16 | 0.40 | |
| Waist circumference (cm) | ||||||
| 57–73 | 74 | 1.1 (0.05) | 31.2 (1.8) | 2.5 (0.9) | 89.7 (10.6) | 160 (24) |
| 73–89 | 161 | 1.1 (0.06) | 34.6 (2.1) | 1.3 (1.2) | 95.5 (15.5) | 159 (35) |
| 89+ | 79 | 1.2 (0.06) | 38.1 (2.0) | 0.7 (0.9) | 92.6 (11.4) | 131 (26) |
| p | 0.15 | 0.01 | 0.19 | 0.86 | 0.53 | |
| Waist/Height Ratio (cm/cm) | ||||||
| 0.35–0.47 | 85 | 1.1 (0.05) | 32.5 (1.9) | 1.8 (0.9) | 88.7 (10.6) | 151 (24) |
| 0.47–0.56 | 148 | 1.1 (0.06) | 34.1 (2.1) | 1.5 (1.2) | 88.6 (15.5) | 144 (35) |
| 0.56+ | 81 | 1.2 (0.06) | 38.5 (1.9) | 1.0 (0.9) | 107 (11) | 166 (25) |
| p | 0.51 | 0.02 | 0.71 | 0.22 | 0.67 | |
| Weight at 18 (kg) | ||||||
| 37–48 | 56 | 1.1 (0.05) | 33.8 (1.8) | 0.9 (0.9) | 89.4 (10.4) | 139 (24) |
| 48–60 | 164 | 1.1 (0.06) | 34.8 (2.1) | 1.8 (1.2) | 95.7 (15.1) | 159 (34) |
| 60+ | 93 | 1.0 (0.06) | 34.0 (2.1) | 0.8 (1.0) | 88.4 (12.0) | 142 (27) |
| p | 0.33 | 0.85 | 0.46 | 0.75 | 0.64 | |
| BMI at 18 (kg/m2) | ||||||
| <20 | 48 | 1.2 (0.06) | 34.9 (1.9) | 1.5 (0.9) | 94.9 (10.8) | 151 (24) |
| 20–24 | 218 | 1.1 (0.06) | 34.0 (2.1) | 1.5 (1.2) | 89.4 (15.2) | 144 (35) |
| 24+ | 48 | 1.1 (0.06) | 35.9 (2.0) | 1.3 (0.9) | 104 (11) | 179 (25) |
| p | 0.41 | 0.62 | 0.98 | 0.43 | 0.38 | |
| Reproductive | ||||||
| Age at menarche (years) | ||||||
| 11–14 | 58 | 1.1 (0.05) | 33.4 (1.6) | 1.1 (0.8) | 88.9 (15.4) | 144 (21) |
| 14–16 | 155 | 1.2 (0.06) | 35.5 (2.2) | 1.8 (1.2) | 97.1 (15.4) | 159 (35) |
| 16–18 | 101 | 1.1 (0.08) | 35.0 (2.8) | 1.3 (1.3) | 93.7 (15.8) | 140 (36) |
| p | 0.26 | 0.43 | 0.61 | 0.68 | 0.72 | |
| Parity (number of live births) | ||||||
| 1 | 36 | 1.2 (0.06) | 35.0 (2.1) | 1.3 (1.2) | 92.4 (15.5) | 148 (35) |
| 1+ | 278 | 1.1 (0.06) | 33.6 (1.9) | 1.6 (0.9) | 94.4 (10.9) | 157 (25) |
| p | 0.12 | 0.48 | 0.78 | 0.85 | 0.72 | |
| Average months breastfed per child (months) | ||||||
| <9.5 | 78 | 1.1 (0.06) | 35.2 (1.9) | 2.0 (0.9) | 99.3 (10.8) | 167 (24) |
| 9.5–24 | 136 | 1.1 (0.06) | 34.5 (2.2) | 1.3 (1.2) | 98.9 (15.8) | 165 (36) |
| 24–72 | 100 | 1.1 (0.06) | 33.8 (1.9) | 1.2 (0.9) | 84.8 (10.8) | 131 (25) |
| p | 0.94 | 0.82 | 0.67 | 0.37 | 0.32 |
| Hormone Cycle Phase | Characteristic | Unadjusted Model | Mutually-Adjusted Model | ||
|---|---|---|---|---|---|
| % Difference a | p | % Difference a | p | ||
| Estrone | |||||
| Whole Cycle | Education (College vs. High school) | 19.8 | 0.02 | 18.2 | 0.03 |
| Follicular | Breastfeeding (<9.5 vs. 24+ months) | 97.2 | 0.02 | 40.6 | 0.07 |
| Estradiol | |||||
| Whole Cycle | Education (College vs. High school) | 26.3 | 0.02 | 23.6 | 0.03 |
| Follicular | Breastfeeding (<9.5 vs. 24+ months) | 239.1 | 0.003 | 63.7 | 0.01 |
| Progesterone | |||||
| Whole Cycle | House type (House or Apartment vs. Ger) | 55.8 | 0.08 | 42.3 b | 0.10 |
| Follicular | Height (161+ vs. <153 cm) | 176 | 0.01 | 237 c | 0.02 |
| Luteal | Waist circumference (89+ vs. <73 cm) | 50.4 | 0.02 | 43.4 c | 0.02 |
| Testosterone | |||||
| Whole Cycle | Weight (70+ vs. <55 kg) | 13.9 | 0.05 | 11.0 d | 0.07 |
| Whole Cycle | BMI (28+ vs. <22 kg/m2) | 23.7 | 0.001 | 17.1 d | 0.001 |
| Whole Cycle | Waist circumference (89+ cm vs. <73 cm) | 22.1 | 0.002 | 17.9 d | 0.005 |
| Whole Cycle | Waist to height ratio (0.56+ vs. <0.47) | 18.3 | 0.007 | 15.3 d | 0.01 |
| Whole Cycle | Alcohol (Yes vs. No) | 14.4 | 0.009 | 10.7 e | 0.01 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Houghton, L.C.; Ganmaa, D.; Rosenberg, P.S.; Davaalkham, D.; Stanczyk, F.Z.; Hoover, R.N.; Troisi, R. Associations of Breast Cancer Risk Factors with Premenopausal Sex Hormones in Women with Very Low Breast Cancer Risk. Int. J. Environ. Res. Public Health 2016, 13, 1066. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13111066
Houghton LC, Ganmaa D, Rosenberg PS, Davaalkham D, Stanczyk FZ, Hoover RN, Troisi R. Associations of Breast Cancer Risk Factors with Premenopausal Sex Hormones in Women with Very Low Breast Cancer Risk. International Journal of Environmental Research and Public Health. 2016; 13(11):1066. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13111066
Chicago/Turabian StyleHoughton, Lauren C., Davaasambuu Ganmaa, Philip S. Rosenberg, Dambadarjaa Davaalkham, Frank Z. Stanczyk, Robert N. Hoover, and Rebecca Troisi. 2016. "Associations of Breast Cancer Risk Factors with Premenopausal Sex Hormones in Women with Very Low Breast Cancer Risk" International Journal of Environmental Research and Public Health 13, no. 11: 1066. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13111066