
Pain Assessment–Can it be Done with a Computerised System? A Systematic Review and Meta-Analysis

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Questions
2.2. Inclusion and Exclusion Criteria
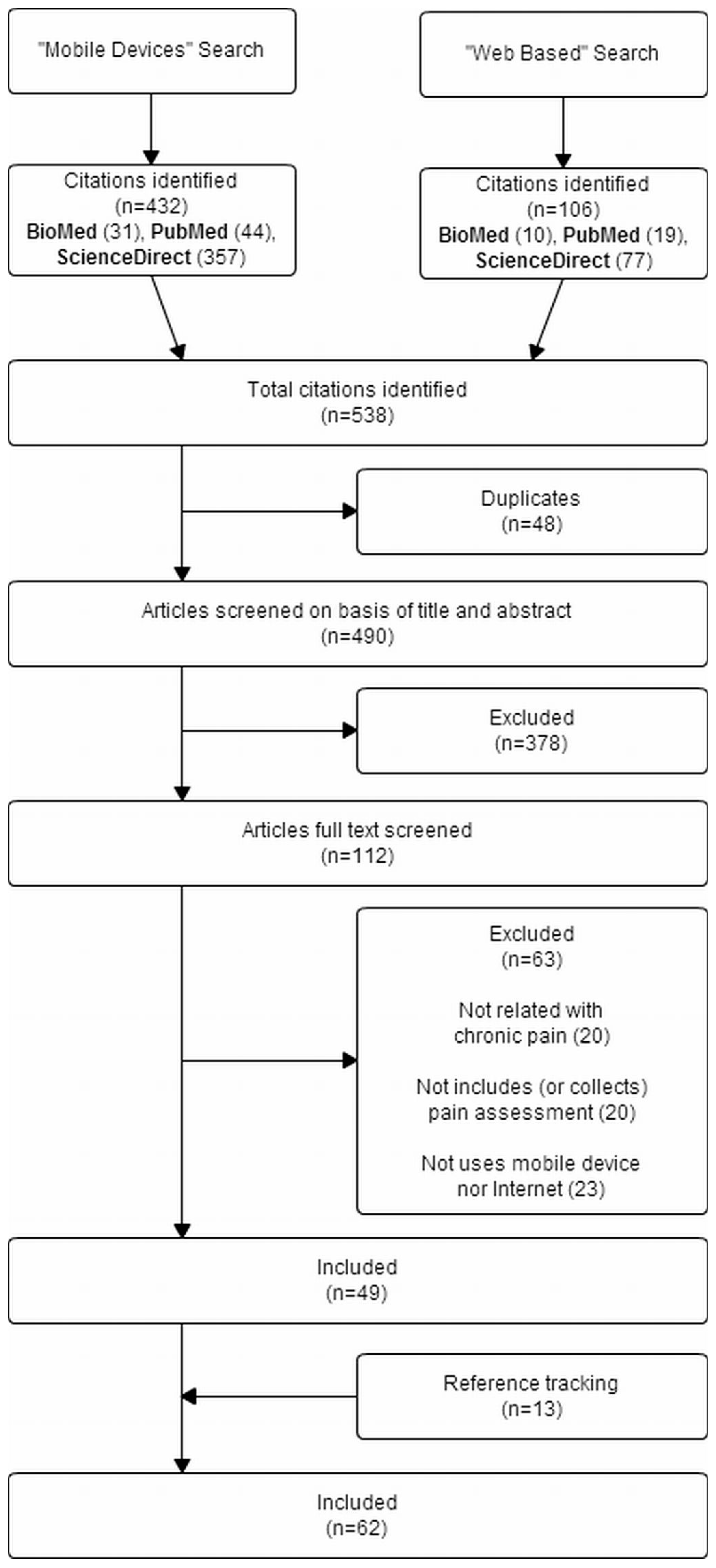
2.3. Search Strategy
2.4. Extraction of Study Characteristics
2.5. Quality Assessment
2.6. Risk of Bias Assessment
2.7. Mathematical Analysis
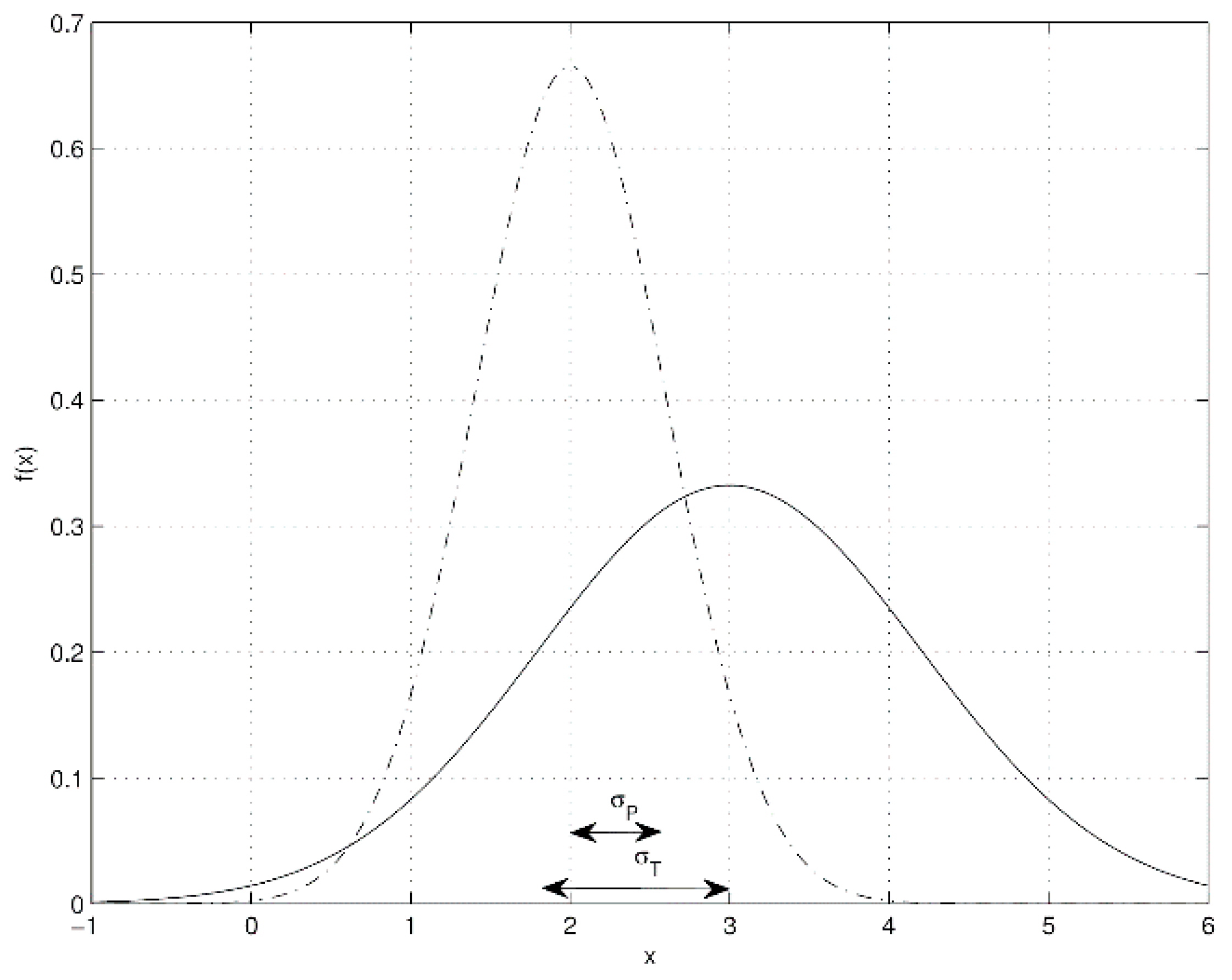
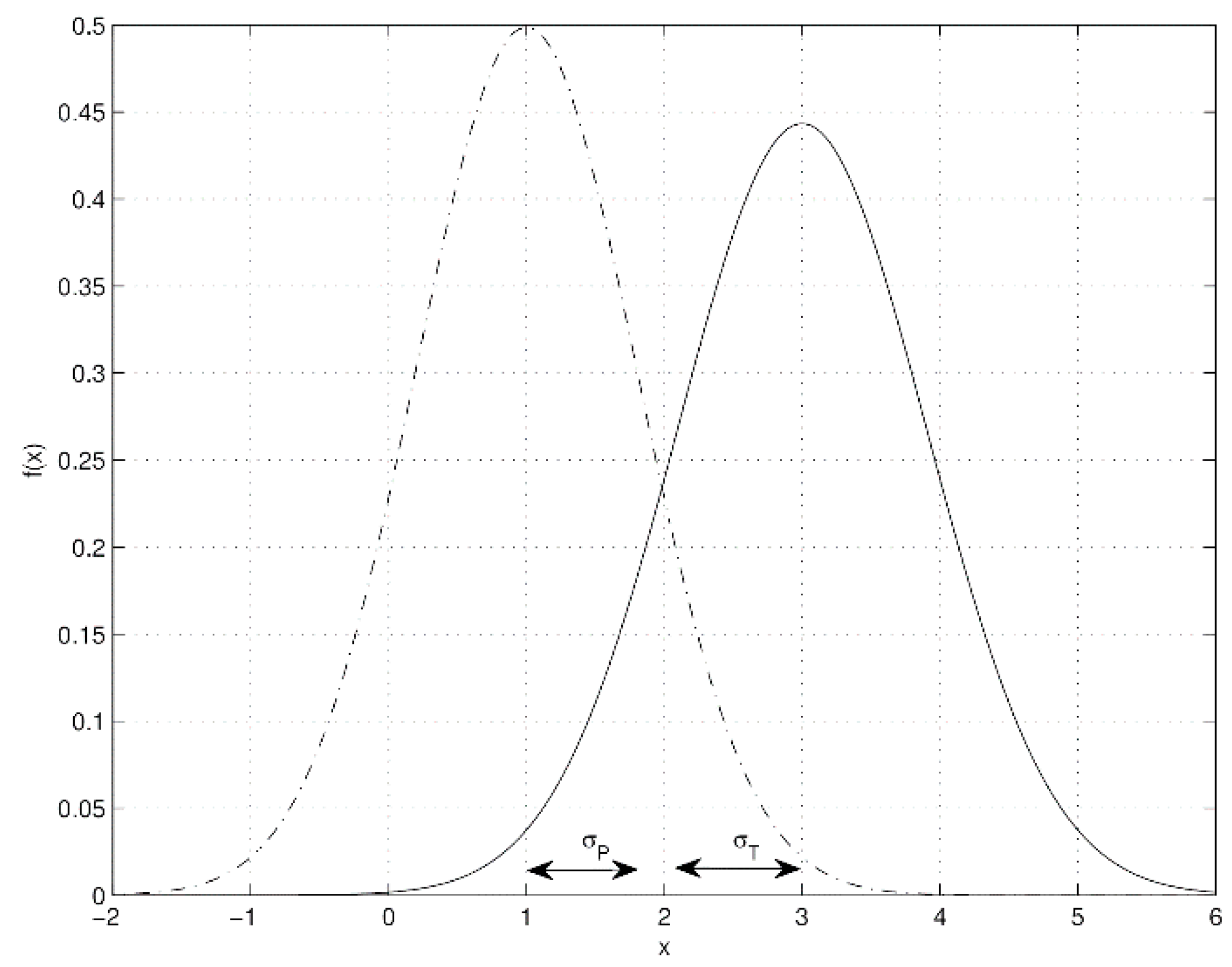
2.7.1. Statistical Data Fusion
2.7.2. Qualitative Analysis
2.7.3. Considerations for the Analysis
3. Results
3.1. Mobile Systems
3.2. Web-Based Systems
3.3. Meta-Analysis
4. Discussion
5. Conclusions
Limitations
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| CBT | Cognitive-behavioural Therapy |
| CG | Control Group |
| ED | Electronic pain diaries |
| EMA | Ecological Momentary Assessment |
| IdT | Internet-delivery treatment |
| IG | Intervention Group |
| PD | Paper pain diaries |
| PHR | Personal Health Record |
| RCT | Randomised controlled trial |
| SD | Standard Deviation |
Appendix A1

{kind=link}
{kind=link}
{kind=link}
| Study/Year | Population Participants (Mean Age, SD) | Patient Home | Data | Quality | ||
|---|---|---|---|---|---|---|
| As a Complement to the System | Collected through the Use of System | Transmission | ||||
| Mobile systems | ||||||
| Allen [84,85], 2009 | 157 (61.7 ± 10.6) | Yes | Pre: CSQ | Pain intensity (VAS), immediately after waking, then approximately every 2 h throughout the day (in order to complete at least 7 pain ratings per day) and immediately before going to sleep (to recall the average pain during the day) | NR | L |
| Anatchkova [86], 2009 | 100 | No | Pain intensity (NRS), computer adaptive dynamic assessment of The Chronic Pain Impact Item Bank [87], and SF-12, in the medical appointment | NR | L | |
| Axen [69,70], 2011 | 262 (44) | Yes | Pre: Pain intensity (NRS), location, duration and frequency, self-rated general health (5-point Likert scale). EuroQoL 5 (EQ5D) Post: EQ5D and self-rated general health (6-months follow up) | Pain intensity (NRS), once a week using SMS | Instant | L |
| Badr [88], 2010 | 54 patients (49.4 ± 10.8) 48 partners (51.3 ± 11.5) | Yes | Patients: pain intensity (NRS), mood, medication taken and pain relief, 6 times per day between 9 a.m. and 9 p.m. Perceptions of relationship functioning in the last assessment of the day. Partners: patients’ pain, own mood and perceptions of relationship functioning, at similar time points | Instant | L | |
| Baron-Mahn [89,90], 2009 | 2094 painful radiculopathy (59.4 ± 14.4) 1623 painful diabetic neuropathy (61.9 ± 13.0) 498 postherpetic neuralgia (60.6 ± 15.4) | No | MOS-SS, PHQ, PD-Q and pain location (pinpointed in 3D mannequin) in the medical appointment | Delayed | L | |
| Broderick-Schneider [50,91,92], 2008 | 83 (56.2 ± 11.1) | Yes | Treatment: 10 random recalls pain assessment via phone interview (interactive voice recording was used) Post: Pain Intensity (VAS) | SF-36, BPI, BFI, MPQ, 7 times per day during the patients’ waking hours | Delayed | L |
| Clauw [34], 2008 | 399 IG 100 mg/day (49.5 ± 10.9) 396 IG 200 mg/day (50.4 ± 10.6) 401 CG (50.7 ± 10.4) | Yes | Pre: FIQ, MASQ, MOS-SS, MDHAQ, MFI, BDI, and ASEX Treatment: 3, 7, 11 and 15 week visit: PGIC, SF-36, FIQ, MASQ, MOS-SS, MDHAQ, MFI. BDI and ASEX only at week 15 | Diary: pain intensity (VAS), 5 times per day (morning, 3 during day and evening) Weekly: pain, fatigue, influence of pain in self-care (VAS) | Instant | H |
| Connelly [93], 2010 | 9 (12.3 ± 3.4) | Yes | Children: pain intensity (VAS), PANAS-C, CALQ, 3 times per day (morning, afternoon, and evening) Parents: PANAS, ARCS at the same time points, using a separate PDA | Delayed | L | |
| Gaertner [94], 2004 | 24 (49.9 ± 15.1) Crossover randomized between IG and CG | Yes | Pain intensity (NRS), once a day and symptom assessment (fatigue, nausea, dyspnea, weakness…), once a week | Delayed | L | |
| Ghinea [95], 2008 | 45 (46.1) | Yes | Pain intensity (VAS) and location (pinpointed in 3D mannequin), 3 times a day | Instant | L | |
| Giske [72], 2010 | 50 (50.0 ± 11.0) | Yes | Pre: HSCL-25, FIQ Post: Pain intensity (VAS) and pain location | Pain intensity (NRS), 5 times a day between 9 a.m. and 9 p.m., using SMS | Instant | L |
| Heiberg [96], 2007 | 38 (58.4 ± 12.9) | Yes | Diary: pain intensity (VAS), fatigue, and patient global evaluation of their disease, RADAI, 4 times per day Weekly: MHAQ, SF-36 | Instant | H | |
| Jamison [28], 2001 | 20 IG (42.1 ± 5.0) 16 CG (43.3 ± 9.2) | Yes | Pre: CPEQ, SCL-90 Treatment: MPQ-SF (once a month). Pain reported weekly by phone interview Post: SCL-90 | Pain intensity (VAS) and pain ratings of the previous 16 waking hours, once a day (bedtime) | Delayed | H |
| Jamison [97], 2002 | 24 (34.4) | No | Pain intensity (VAS) | Delayed | L | |
| Jamison [98], 2006 | 21 (42.0 ± 4.9) | Yes | Pre: CPEQ, SF-36, MPQ-SF, SCL-90 Treatment: Pain reported weekly by phone interview | Pain intensity (VAS), at least once a day | Delayed | H |
| Jamison-Wasan [26,27], 2010 | 21 IG ED + CBT (47.0 ± 7.8) 21 CG #1 ED (46.6 ± 6.8) 20 CG #2 ED (49.6 ± 6.8) | Yes | Pre and Post: ABC, BPI, COMM, HADS, MINI, PDI, SOAPP-R Post: PDUQ | BPI, pain location once a month at clinic visit Wasan’s study, also includes four questions to assess craving for prescription opioids over the past 24 h (14 days ED at patients' home) CBT: Group educational sessions (e.g., opioid addiction risks and medication compliance, making lifestyle changes...) and individual motivational counseling (review of medication adherence, support for patients’ efforts, education on pain management and drug misuse...) | Delayed | H |
| Jespersen [71], 2012 | 188 (44.4 ± 9.0) | Yes | Pre: AMS | AMS, IPAQ, once a week using SMS | Instant | H |
| Koroschetz [99], 2011 | 1623 painful diabetic neuropathy (61.9 ± 13.0) 1434 fibromyalgia (51.9 ± 10.8) | No | MOS-SS, PHQ, PD-Q and pain location (pinpointed in 3D mannequin) in the medical appointment | Delayed | L | |
| Kvien [100], 2005 | 30 (61.6) | No | Pain intensity (VAS), fatigue, and patient global evaluation of their disease, RADAI, MHAQ, SF-36, at 2 medical appointments | Instant | L | |
| Lewandowski [101], 2010 | 39 chronic pain (15.3 ± 1.5) 58 healthy participants (14.7 ± 1.8) | Yes | Pre: CES-D | Sleep quality (NRS) in the morning and pain intensity (NRS) in the evening. Integrated with wrist actigraphy to monitorize the sleep | Delayed | L |
| Levin [102], 2006 | 24 | Yes | Pain intensity (NRS), location, duration reported via automated speech telephony delivery (a.k.a automated speech recognition) | Instant | L | |
| Li [103], 2010 | 60 (69.0 ± 10.0) | Yes | Pre and Post: MPQ-SF | MPQ-SF, 8 times per day (hourly between 2 and 9 p.m.) | Delayed | H |
| Lind [104], 2008 | 12 (67.5 ± 7.8) | Yes | Pain intensity (VAS), 3 times a day (8 a.m., 1 p.m., 8 p.m.) | Instant | L | |
| Litt [44], 2009 | 32 IG 22 CG Overall (41.0 ± 11.9) | Yes | Pre and Post: MPI, CES-D | Pan location, unpleasantness experienced, perceived control over pain, catastrophization and coping, 4 times per day (from 8 a.m. to 10 p.m.). Interactive voice recording was used CBT: relaxation training, cognitive restructuring and stress management | Instant | H |
| Luckmann [76], 2010 | 4 | Yes | Pain intensity (NRS), location, activity and treatment completed each 2–4 waking hours. Acute pain registered when happens. Sleep report in the morning and end of day report before sleep. Data integration with PHR | Instant | L | |
| Marceau [105], 2010 | 67 IG (48.5 ± 11.6) 67 CG (50.5 ± 11.0) | No | BPI at each monthly clinic visit. Pre and post-treatment and 5-month follow up: BPI, PCS, ODI, CES-D | Instant | H | |
| McClellan [29], 2009 | 9 IG 10 CG Overall (13.4 ± 2.9) | Yes | Pain intensity at morning and evening (10-point Likert scale), pain location, sleep quality, and functional limitations once a day CBT: coping skills program, once a day. Parents presence is allowed | Instant | H | |
| Oerlemans [38], 2011 | 37 IG (35.9 ± 11.7) 39 CG (40.6 ± 15.5) | Yes | Pre and Post (upon treatment and 3-month follow up): Pain intensity (5-point Likert scale), CFSBD, IBS-QoL, PCS | Pain intensity (5-point Likert scale) 3 times per day (morning, afternoon and evening). Sleep quality and intended activities for the day. (morning), accomplished activities, cognitions, and feelings (afternoon), and satisfaction with activity level and achievements of that day (evening) CBT: situational feedback on their diaries from a psychologist | Instant | H |
| Okifuji [106], 2011 | 81 (28.8 ± 6.2) | Yes | Overall pain (7-point Likert scale), fatigue, head pain, emotional distress, abdominal pain, sense of relaxation, muscle pain, and sense of swelling, 3 times per day (morning, early afternoon, late afternoon) | Delayed | L | |
| Page [107], 2010 | 14 (65.1) | No | Pre: PDQ-39, BDI-II, UPDRS | MPQ, in the medical appointment | Delayed | L |
| Palermo [33], 2004 | 30 IG (12.3 ± 2.4) 30 CG (12.3 ± 3.0) | Yes | Pre: CALI | Pain intensity (Faces pain scale [108]), pain symptoms (occurrence, location, duration, and emotional upset), CSI, and CALI, once a day | Delayed | H |
| Peters [109], 2000 | 80 (40.6 ± 6.7) | Yes | Pre: MPI, SF-36, BSI Post: CSQ (6 months follow up) | Pain intensity (7-point scale) and signal controlled diary (items: pain cognition, pain coping, sleep quality...), 4 times per day between 8 a.m. and 9:30 p.m. | Delayed | H |
| Roelofs [110], 2004 | 40 (46.4 ± 9.9) | Yes | Pre: TSK, QBPDS | Pain intensity (PVAQ), TSK, 8 times per day between 8 a.m. (weekend 9 a.m.) and 10 p.m. | Delayed | L |
| Schurman [35], 2010 | 10 IG 10 CG Overall (12.2 ± 2.8) | Yes | Pre and Post: BASC, PedsQL, completed by children and parents | Pain intensity (Faces pain scale Revised), once per day (bedtime) CBT: relaxation sessions, such as abdominal breathing, progressive muscle relaxation, imagery, and autogenic hand-warming. Multimedia content for home practice | Delayed | H |
| Sorbi [111], 2007 | 5 | Yes | Pain intensity (VAS). 1st test run: 4–5 times per day. 2nd test run: 2–3 times per day CBT: migraine headache, medication use, attack precursors, self relaxation and other preventive behaviour | Instant | L | |
| Stinson [112], 2008 | Study 1 76 (13.4 ± 2.5) Study 2 36 (12.6 ± 2.4) | Yes | Post: PedsQL, PCQ | Pain intensity, pain unpleasantness, pain’s interference with aspects of quality of life and other symptoms (e.g., stiffness and fatigue) (VAS), 3 times per day (upon waking, after school, and before bed) | Instant | H |
| Stinson [113], 2012 | 24 children (5.9 ± 0.9) 77 youth (13.5 ± 3.1) | No | Pain intensity: faces pain scale (children), NRS (youth), in the medical appointment | Instant | H | |
| Stone [31], 2003 | 40 IG (43.0 ± 9.0) 40 CG (48.0 ± 10.8) | Yes | Pre: MPQ-SF | BPI, PD-IIP, HAQ, 3 times per day (10 p.m., 4 a.m., 8 a.m.) | Delayed | H |
| Stone-Kelly [30,32], 2003 | 22 IG 3 prompts/day (49.0 ± 10.7) 22 IG 6 prompts/day (53.5 ± 10.4) 24 IG 12 prompts/day (50.3 ± 10.3) 23 CG (49.8 ± 12.5) | Yes | Pre: Questionnaire to assess anxiety, stress, pain, health, and quality of life Pre/Treatment: Questionnaire, once a week, to assess pain and mood, the momentary and the occurred over the last 7 days Treatment: Questionnaire once a week to assess interference of ED with participants' daily routines | Pain intensity (VAS), and other questions related to sensory, affective and physical aspects, 3, 6 or 12 times a day. Kelly’s study includes all the IGs | Delayed | H |
| Turner [47], 2005 | 61 IG (39.3 ± 11.1) 65 CG (35.4 ± 10.5) | Yes | Pre: GCPS | Pain intensity (NRS), pain-related activity interference, jaw use limitations, and several questions adapted from CSQ, SOPA, PCS, and DCI, 3 times per day (morning, afternoon, and evening) CBT: At each session activity goals were recommended (correct jaw posture, progressive relaxation practice, breathing exercises, physical exercise...) | Delayed | H |
| Wallasch [114], 2012 | 545 (43.1 ± 12.9) | Yes | MIDAS, GCPS, HADS, SF-12 | Delayed | L | |
| Weering [115], 2012 | 16 (40.7 ± 13.8). | Yes | Pre: RMDQ, SoC | Pain intensity (VAS), 3 times a day (noon, 4 p.m., 8 p.m.). Integration with Body Area Network (BAN) | Instant | L |
| Younger [116], 2009 | 10 (46.5 ± 10.3) | Yes | Treatment: FIQ every 2 weeks | Fibromyalgia severity, average pain intensity, highest pain, and other symptoms (fatigue, sadness, stress, sleep quality, ability to think and remember…), once a day (night) | NR | L |
| Web-based systems | ||||||
| Berman [41], 2009 | 41 IG (64.3) 37 CG (67.5) | Pre and Post: BPI, PSEQ, CED-S, STAI, PAQ, HDM | Pain intensity (BPI), after logon and before logoff in the site CBT: abdominal breathing, relaxation, writing about experiences (positives or negatives), creative visual expression and positive thinking. Audio, visual and textual content related to pain | H | ||
| Buhrman [36], 2004 | 22 IG (43.5 ± 10.3) 29 CG (45.0 ± 10.7) | Pre: HADS | Pain intensity (VAS), 3 times per day (morning, noon and evening). PAIRS, MPI, CSQ and HADS once a week CBT: several modules (pain, stress, physical activities, problem solving...) and slideshows and sound files for download | H | ||
| Devineni [42], 2005 | 39 IG (43.6 ± 12.0) 47 CG (41.0 ± 11.8) | Frequency, duration, and severity of pain, once a day Pre/Post/Follow up: HSQ, CES-D, STAI, HDI CBT: muscle relaxation program, and stress coping therapy | H | |||
| Hicks [43], 2006 | 25 IG (12.1 ± 2.0) 22 CG (11.3 ± 2.2) | Pre: PedsQL Post: PedsQL (1-month and 3-month follow up) | Pain intensity (NRS), 4 times per day CBT: relaxation techniques, lifestyle (diet, exercise), information related to pain | H | ||
| Hunt [51], 2009 | 28 IG (39.0 ± 10.0) 26 CG (38.0 ± 12.0) | GSRS-IBS, IBS-QoL, ASI, GAD-Q and CPSQ, conducted at pre-and post-treatment and 3-month follow-up CBT: gastrointestinal symptoms and stress and on relaxation training, stress management, catastrophic thinking, exposure therapy and the social consequences of IBS | H | |||
| Kristjansdottir [52], 2011 | 6 (36.3) | Pre and Post: CPAQ, PCS | Pain intensity, interference of pain, planned and achieved activities, feelings, pain-related fear, avoidance, catastrophizing and acceptance, 3 times per day (morning, evening and a time randomly chosen between 11:30 a.m. and 2 p.m.) CBT: feedback SMS with praise, encouragement messages, and exercises | L | ||
| Ljótsson [45], 2010 | 42 IG (36.4 ± 10.1) 43 CG (32.8 ± 8.6) | Treatment: Gastrointestinal symptom diary | GSRS-IBS, IBS-QoL, VSI, MADRS-S and SDS conducted at pre-and post treatment. 3-month follow up: VSI, IBS-QoL and 2 weekly GSRS-IBS CBT: mindfulness exercises program, and lifestyle strategies (diet, exercise) | H | ||
| Lorig [39], 2008 | 422 IG (52.2 ± 10.9) 433 CG (52.5 ± 12.2) | Pre and post treatment, and 6/12 months follow up: pain intensity and fatigue (NRS), distress, activities limitations, disabilities and HAQ CBT: tailored exercises programmes and medication diaries | H | |||
| Palermo [37], 2009 | 26 IG (14.3 ± 2.1) 22 CG (15.3 ± 1.8) | Pre and Post: RCADS, ARCS | Pain intensity (NRS), CALI CBT: two separate websites, one for child access and one for parent access. The child access comprised eight treatment modules (education about chronic pain, recognizing stress and negative emotions, relaxation, distraction, cognitive skills, sleep hygiene and lifestyle, staying active, relapse prevention). Download of multimedia content. | H | ||
| Ruehlman [46], 2012 | 162 IG (19~78) 143 CG (19~78) | CES-D, DASS, PCP-S and PCP-EA at pre-treatment, 7-weeks and 14-weeks follow-up CBT: several content such as interactive activity, relaxation sessions | H | |||
| Strom [40], 2000 | 20 IG (41.5) 25 CG (39.2) | Pre: Pain intensity (VAS), duration, BDI, HDI, MLPC. Treatment: Number of times and the total time used for training relaxation. Post: Pain intensity (VAS) | CBT: several modules concerning relaxation | H | ||
| Williams [48], 2010 | 59 IG (50.2 ± 12.3) 59 CG (50.8 ± 10.6) | Pre: MINI, PD-IIP | SF-36, BPI, MFI, MOS-SS, CES-D, STPI and PGIC at pre and post-treatment CBT: multimedia content following topics: educational lectures, symptom management and adaptive life style | H | ||
Appendix A2
Appendix A3
| Study/Year | Sequence Generation | Allocation Concealment | Blinding of Participants, Personnel and Outcome Assessors | Incomplete Outcome Data | Free of Selective Outcome Reporting | Free of Other Sources of Bias |
|---|---|---|---|---|---|---|
| Berman [41], 2009 | Yes | No | No | Yes | Yes | No |
| Buhrman [36], 2004 | Yes | Yes | No | Yes | Yes | Yes |
| Devineni [42], 2005 | No | Yes | No | Yes | Yes | Yes |
| Hicks [43], 2006 | Yes | Yes | No | No | Yes | Yes |
| Hunt [51], 2009 | Yes | Yes | No | No | Yes | No |
| Litt [44], 2009 | Yes | Yes | No | Unclear | Yes | Yes |
| Ljótsson [45], 2010 | Yes | Yes | No | Unclear | Yes | Yes |
| Lorig [39], 2008 | Yes | Yes | No | No | Yes | Yes |
| Marceau [105], 2010 | Yes | Yes | No | No | Yes | Yes |
| Oerlemans [38], 2011 | Yes | Yes | No | Unclear | Yes | No |
| Palermo [37], 2009 | Yes | Yes | No | Yes | Yes | Yes |
| Ruehlman [46], 2012 | Yes | Yes | No | Yes | Yes | No |
| Schurman [35], 2010 | Yes | Yes | No | Yes | Yes | Yes |
| Strom [40], 2000 | Yes | Yes | No | Yes | Yes | No |
| Turner [47], 2005 | No | Yes | No | Yes | Yes | Yes |
| Williams [48], 2010 | Yes | Yes | No | Unclear | Yes | Yes |
References
- Committee on Advancing Pain Research, Care, Institute of Medicine (U.S.). Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education, and Research; The National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Ashburn, M.A.; Staats, P.S. Management of chronic pain. Lancet 1999, 353, 1865–1869. [Google Scholar] [CrossRef]
- Langley, P.; Muller-Schwefe, G.; Nicolaou, A.; Liedgens, H.; Pergolizzi, J.; Varrassi, G. The impact of pain on labor force participation, absenteeism and presenteeism in the European Union. J. Med. Econ. 2010, 13, 662–672. [Google Scholar] [CrossRef] [PubMed]
- Stewart, W.F.; Ricci, J.A.; Chee, E.; Hahn, S.R.; Morganstein, D. Cost of lost productive work time among U.S. workers with depression. JAMA 2003, 289, 3135–3144. [Google Scholar] [CrossRef] [PubMed]
- Apkarian, A.V.; Baliki, M.N.; Geha, P.Y. Towards a theory of chronic pain. Prog. Neurobiol. 2009, 87, 81–97. [Google Scholar] [CrossRef] [PubMed]
- Mackintosh, C.; Elson, S. Chronic pain: Clinical features, assessment and treatment. Nurs. Stand. 2008, 23, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Thomas, T.; Robinson, C.; Champion, D.; McKell, M.; Pell, M. Prediction and assessment of the severity of post-operative pain and of satisfaction with management. Pain 1998, 75, 177–185. [Google Scholar] [CrossRef]
- Hirsh, A.T.; George, S.Z.; Robinson, M.E. Pain assessment and treatment disparities: A virtual human technology investigation. Pain 2009, 143, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Giordano, J.; Abramson, K.; Boswell, M.V. Pain assessment: Subjectivity, objectivity, and the use of neurotechnology. Pain Phys. 2010, 13, 305–315. [Google Scholar]
- Nekolaichuk, C.L.; Bruera, E.; Spachynski, K.; MacEachern, T.; Hanson, J.; Maguire, T.O. A comparison of patient and proxy symptom assessments in advanced cancer patients. Palliat. Med. 1999, 13, 311–323. [Google Scholar] [CrossRef] [PubMed]
- Pautex, S.; Berger, A.; Chatelain, C.; Herrmann, F.; Zulian, G.B. Symptom assessment in elderly cancer patients receiving palliative care. Crit. Rev. Oncol. Hematol. 2003, 47, 281–286. [Google Scholar] [CrossRef]
- Weingarten, S.R.; Henning, J.M.; Badamgarav, E.; Knight, K.; Hasselblad, V.; Gano, A., Jr.; Ofman, J.J. Interventions used in disease management programmes for patients with chronic illnesswhich ones work? Meta-analysis of published reports. BMJ 2002, 325, 925. [Google Scholar] [CrossRef] [PubMed]
- Escarrabill, J.; Marti, T.; Torrente, E. Good morning, doctor Google. Rev. Port. Pneumol. 2011, 17, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Keogh, E.; Rosser, B.A.; Eccleston, C. e-Health and chronic pain management: Current status and developments. Pain 2010, 151, 18–21. [Google Scholar] [CrossRef] [PubMed]
- Rosser, B.A.; Vowles, K.E.; Keogh, E.; Eccleston, C.; Mountain, G.A. Technologically-assisted behaviour change: A systematic review of studies of novel technologies for the management of chronic illness. J. Telemed. Telecare 2009, 15, 327–338. [Google Scholar] [CrossRef] [PubMed]
- Ong, K.S.; Seymour, R.A. Pain measurement in humans. Surgeon 2004, 2, 15–27. [Google Scholar] [CrossRef]
- Melzack, R.; Casey, K.L. Sensory, motivational, and central control determinants of pain: A new conceptual model. Skin Senses 1968, 423–443. [Google Scholar]
- Fernandez, E.; Turk, D.C. Sensory and affective components of pain: Separation and synthesis. Psychol. Bull. 1992, 112, 205–217. [Google Scholar] [CrossRef] [PubMed]
- Holroyd, K.A.; Talbot, F.; Holm, J.E.; Pingel, J.D.; Lake, A.E.; Saper, J.R. Assessing the dimensions of pain: A multitrait-multimethod evaluation of seven measures. Pain 1996, 67, 259–265. [Google Scholar] [CrossRef]
- Kornbluth, I.D.; Freedman, M.K.; Holding, M.Y.; Overton, E.A.; Saulino, M.F. Interventions in chronic pain management. 4. Monitoring progress and compliance in chronic pain management. Arch. Phys. Med. Rehabil. 2008, 89, S51–S55. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011); Higgins, J.P.T., Green, S., Eds.; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bar-shalom, Y.; Li, X. Multitarget-Multisensor Tracking: Principles and Techniques; Yaakov Bar-Shalom: Storrs, CT, USA, 1995. [Google Scholar]
- Bar-Shalom, Y.; Campo, L. The effect of the common process noise on the two-sensor fused-track covariance. IEEE Trans. Aerosp. Electron. Syst. 1986, AES-22, 803–805. [Google Scholar] [CrossRef]
- Shin, V.; Shevlyakov, G.; Kim, K. A new fusion formula and its application to continuous-time linear systems with multisensor environment. Comput. Stat. Data Anal. 2007, 52, 840–854. [Google Scholar] [CrossRef]
- Jamison, R.N.; Ross, E.L.; Michna, E.; Chen, L.Q.; Holcomb, C.; Wasan, A.D. Substance misuse treatment for high-risk chronic pain patients on opioid therapy: A randomized trial. Pain 2010, 150, 390–400. [Google Scholar] [CrossRef] [PubMed]
- Wasan, A.D.; Ross, E.L.; Michna, E.; Chibnik, L.; Greenfield, S.F.; Weiss, R.D.; Jamison, R.N. Craving of prescription opioids in patients with chronic pain: A longitudinal outcomes trial. J. Pain 2012, 13, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Jamison, R.N.; Raymond, S.A.; Levine, J.G.; Slawsby, E.A.; Nedeljkovic, S.S.; Katz, N.P. Electronic diaries for monitoring chronic pain: 1-year validation study. Pain 2001, 91, 277–285. [Google Scholar] [CrossRef]
- McClellan, C.B.; Schatz, J.C.; Puffer, E.; Sanchez, C.E.; Stancil, M.T.; Roberts, C.W. Use of handheld wireless technology for a home-based sickle cell pain management protocol. J. Pediatr. Psychol. 2009, 34, 564–573. [Google Scholar] [CrossRef] [PubMed]
- Stone, A.A.; Broderick, J.E.; Schwartz, J.E.; Shiffman, S.; Litcher-Kelly, L.; Calvanese, P. Intensive momentary reporting of pain with an electronic diary: Reactivity, compliance, and patient satisfaction. Pain 2003, 104, 343–351. [Google Scholar] [CrossRef]
- Stone, A.A.; Shiffman, S.; Schwartz, J.E.; Broderick, J.E.; Hufford, M.R. Patient compliance with paper and electronic diaries. Control. Clin. Trials 2003, 24, 182–199. [Google Scholar] [CrossRef]
- Litcher-Kelly, L.; Stone, A.A.; Broderick, J.E.; Schwartz, J.E. Associations among pain intensity, sensory characteristics, affective qualities, and activity limitations in patients with chronic pain: A momentary, within-person perspective. J. Pain 2004, 5, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Palermo, T.M.; Valenzuela, D.; Stork, P.P. A randomized trial of electronic versus paper pain diaries in children: Impact on compliance, accuracy, and acceptability. Pain 2004, 107, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Clauw, D.J.; Mease, P.; Palmer, R.H.; Gendreau, R.M.; Wang, Y. Milnacipran for the treatment of fibromyalgia in adults: A 15-week, multicenter, randomized, double-blind, placebo-controlled, multiple-dose clinical trial. Clin. Ther. 2008, 30, 1988–2004. [Google Scholar] [CrossRef] [PubMed]
- Schurman, J.V.; Wu, Y.P.; Grayson, P.; Friesen, C.A. A pilot study to assess the efficacy of biofeedback-assisted relaxation training as an adjunct treatment for pediatric functional dyspepsia associated with duodenal eosinophilia. J. Pediatr. Psychol. 2010, 35, 837–847. [Google Scholar] [CrossRef] [PubMed]
- Buhrman, M.; Fältenhag, S.; Ström, L.; Andersson, G. Controlled trial of Internet-based treatment with telephone support for chronic back pain. Pain 2004, 111, 368–377. [Google Scholar] [CrossRef] [PubMed]
- Palermo, T.M.; Wilson, A.C.; Peters, M.; Lewandowski, A.; Somhegyi, H. Randomized controlled trial of an internet-delivered family cognitive-behavioral therapy intervention for children and adolescents with chronic pain. Pain 2009, 146, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Oerlemans, S.; van Cranenburgh, O.; Herremans, P.-J.; Spreeuwenberg, P.; van Dulmen, S. Intervening on cognitions and behavior in irritable bowel syndrome: A feasibility trial using PDAs. J. Psychosom. Res. 2011, 70, 267–277. [Google Scholar] [CrossRef] [PubMed]
- Lorig, K.R.; Ritter, P.L.; Laurent, D.D.; Plant, K. The internet-based arthritis self-management program: A one-year randomized trial for patients with arthritis or fibromyalgia. Arthritis Care Res. 2008, 59, 1009–1017. [Google Scholar] [CrossRef] [PubMed]
- Strom, L.; Pettersson, R.; Andersson, G. A controlled trial of self-help treatment of recurrent headache conducted via the Internet. J. Consult. Clin. Psychol. 2000, 68, 722–727. [Google Scholar] [CrossRef] [PubMed]
- Berman, R.L.H.; Iris, M.A.; Bode, R.; Drengenberg, C. The Effectiveness of an online mind-body intervention for older adults with chronic pain. J. Pain 2009, 10, 68–79. [Google Scholar] [CrossRef] [PubMed]
- Devineni, T.; Blanchard, E.B. A randomized controlled trial of an internet-based treatment for chronic headache. Behav. Res. Ther. 2005, 43, 277–292. [Google Scholar] [CrossRef] [PubMed]
- Hicks, C.L.; von Baeyer, C.L.; McGrath, P.J. Online Psychological treatment for pediatric recurrent pain: A randomized evaluation. J. Pediatr. Psychol. 2006, 31, 724–736. [Google Scholar] [CrossRef] [PubMed]
- Litt, M.D.; Shafer, D.M.; Ibanez, C.R.; Kreutzer, D.L.; Tawfik-Yonkers, Z. Momentary pain and coping in temporomandibular disorder pain: Exploring mechanisms of cognitive behavioral treatment for chronic pain. Pain 2009, 145, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Ljótsson, B.; Falk, L.; Vesterlund, A.W.; Hedman, E.; Lindfors, P.; Rück, C.; Hursti, T.; Andréewitch, S.; Jansson, L.; Lindefors, N.; Andersson, G. Internet-delivered exposure and mindfulness based therapy for irritable bowel syndrome—A randomized controlled trial. Behav. Res. Ther. 2010, 48, 531–539. [Google Scholar] [CrossRef] [PubMed]
- Ruehlman, L.S.; Karoly, P.; Enders, C. A randomized controlled evaluation of an online chronic pain self management program. Pain 2012, 153, 319–330. [Google Scholar] [CrossRef] [PubMed]
- Turner, J.A.; Mancl, L.; Aaron, L.A. Brief cognitive-behavioral therapy for temporomandibular disorder pain: Effects on daily electronic outcome and process measures. Pain 2005, 117, 377–387. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.A.; Kuper, D.; Segar, M.; Mohan, N.; Sheth, M.; Clauw, D.J. Internet-enhanced management of fibromyalgia: A randomized controlled trial. Pain 2010, 151, 694–702. [Google Scholar] [CrossRef] [PubMed]
- Macea, D.D.; Gajos, K.; Calil, Y.A.D.; Fregni, F. The efficacy of web-based cognitive behavioral interventions for chronic pain: A systematic review and meta-analysis. J. Pain 2010, 11, 917–929. [Google Scholar] [CrossRef] [PubMed]
- Broderick, J.E.; Schwartz, J.E.; Vikingstad, G.; Pribbernow, M.; Grossman, S.; Stone, A.A. The accuracy of pain and fatigue items across different reporting periods. Pain 2008, 139, 146–157. [Google Scholar] [CrossRef] [PubMed]
- Hunt, M.G.; Moshier, S.; Milonova, M. Brief cognitive-behavioral internet therapy for irritable bowel syndrome. Behav. Res. Ther. 2009, 47, 797–802. [Google Scholar] [CrossRef] [PubMed]
- Kristjansdottir, O.; Fors, E.; Eide, E.; Finset, A.; van Dulmen, S.; Wigers, S.; Eide, H. Written online situational feedback via mobile phone to support self-management of chronic widespread pain: A usability study of a web-based intervention. BMC Musculoskelet. Disord. 2011, 12, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dearnley, C.; Haigh, J.; Fairhall, J. Using mobile technologies for assessment and learning in practice settings: A case study. Nurse Educ. Pract. 2008, 8, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Dworkin, R.H.; Turk, D.C.; Peirce-Sandner, S.; Burke, L.B.; Farrar, J.T.; Gilron, I.; Jensen, M.P.; Katz, N.P.; Raja, S.N.; Rappaport, B.A.; et al. Considerations for improving assay sensitivity in chronic pain clinical trials: IMMPACT recommendations. Pain 2012, 153, 1148–1158. [Google Scholar] [CrossRef] [PubMed]
- Burton, C.; Weller, D.; Sharpe, M. Are electronic diaries useful for symptoms research? A systematic review. J. Psychosom. Res. 2007, 62, 553–561. [Google Scholar] [CrossRef] [PubMed]
- Palermo, T.M.; Eccleston, C.; Lewandowski, A.S.; Williams, A.C.; Morley, S. Randomized controlled trials of psychological therapies for management of chronic pain in children and adolescents: An updated meta-analytic review. Pain 2010, 148, 387–397. [Google Scholar] [CrossRef] [PubMed]
- Kar, N. Cognitive behavioral therapy for the treatment of post-traumatic stress disorder: A review. Neuropsychiatr. Dis. Treat. 2011, 7, 167–181. [Google Scholar] [CrossRef] [PubMed]
- Hay, E.M.; Mullis, R.; Lewis, M.; Vohora, K.; Main, C.J.; Watson, P.; Dziedzic, K.S.; Sim, J.; Lowe, C.M.; Croft, P.R. Comparison of physical treatments versus a brief pain-management programme for back pain in primary care: A randomised clinical trial in physiotherapy practice. Lancet 2005, 365, 2024–2030. [Google Scholar] [CrossRef]
- Morley, S.; Eccleston, C.; Williams, A. Systematic review and meta-analysis of randomized controlled trials of cognitive behaviour therapy and behaviour therapy for chronic pain in adults, excluding headache. Pain 1999, 80, 1–13. [Google Scholar] [CrossRef]
- Marhold, C.; Linton, S.J.; Melin, L. A cognitive-behavioral return-to-work program: Effects on pain patients with a history of long-term versus short-term sick leave. Pain 2001, 91, 155–163. [Google Scholar] [CrossRef]
- Ektor-Andersen, J.; Ingvarsson, E.; Kullendorff, M.; Orbaek, P. High cost-benefit of early team-based biomedical and cognitive-behaviour intervention for long-term pain-related sickness absence. J. Rehabil. Med. 2008, 40, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Schonauer, C.; Pintaric, T.; Kaufmann, H.; Jansen-Kosterink, S.; Vollenbroek-Hutten, M. Chronic pain rehabilitation with a serious game using multimodal input. In Proceedings of the International Conference on Virtual Rehabilitation (ICVR), Zurich, Switzerland, 27–29 June 2011; pp. 1–8.
- Fuchslocher, A.; Niesenhaus, J.; Krämer, N. Serious games for health: An empirical study of the game “Balance” for teenagers with diabetes mellitus. Entertain. Comput. 2011, 2, 97–101. [Google Scholar] [CrossRef]
- Georgoulis, S.; Eleftheriadis, S.; Tzionas, D.; Vrenas, K.; Petrantonakis, P.; Hadjileontiadis, L.J. Epione: An innovative pain management system using facial expression analysis, biofeedback and augmented reality-based distraction. In Proceedings of the 2010 2nd International Conference on Intelligent Networking and Collaborative Systems (INCOS), Thessaloniki, Greece, 24–26 November 2010; pp. 259–266.
- Hoffman, H.G.; Patterson, D.R.; Carrougher, G.J. Use of virtual reality for adjunctive treatment of adult burn pain during physical therapy: A controlled study. Clin. J. Pain 2000, 16, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Lewis, M. Analysis of the roles of “serious games” in helping teach health-related knowledge and skills and in changing behavior. J. Diabetes Sci. Technol. 2007, 1, 918–920. [Google Scholar] [CrossRef] [PubMed]
- Howell, J.; Conatser, R.; Williams, R.; Burns, J.; Eland, D. The virtual haptic back: A simulation for training in palpatory diagnosis. BMC Med. Educ. 2008, 8, 14. [Google Scholar] [CrossRef] [PubMed]
- Kew, S. Text messaging: An innovative method of data collection in medical research. BMC Res. Notes 2010, 3, 342. [Google Scholar] [CrossRef] [PubMed]
- Axén, I.; Bodin, L.; Bergström, G.; Halasz, L.; Lange, F.; Lövgren, P.; Rosenbaum, A.; Leboeuf-Yde, C.; Jensen, I. Clustering patients on the basis of their individual course of low back pain over a six month period. BMC Musculoskelet. Disord. 2011, 12, 99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Axén, I.; Bodin, L.; Bergström, G.; Halasz, L.; Lange, F.; Lövgren, P.W.; Rosenbaum, A.; Leboeuf-Yde, C.; Jensen, I. The use of weekly text messaging over 6 months was a feasible method for monitoring the clinical course of low back pain in patients seeking chiropractic care. J. Clin. Epidemiol. 2012, 65, 454–461. [Google Scholar] [CrossRef] [PubMed]
- Jespersen, T.; Jorgensen, M.; Hansen, J.; Holtermann, A.; Sogaard, K. The relationship between low back pain and leisure time physical activity in a working population of cleaners—A study with weekly follow-ups for 1 year. BMC Musculoskelet. Disord. 2012, 13, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giske, L.; Sandvik, L.; Røe, C. Comparison of daily and weekly retrospectively reported pain intensity in patients with localized and generalized musculoskeletal pain. Eur. J. Pain 2010, 14, 959–965. [Google Scholar] [CrossRef] [PubMed]
- Dijkstra, A.; de Vries, H. The development of computer-generated tailored interventions. Patient Educ. Counsel. 1999, 36, 193–203. [Google Scholar] [CrossRef]
- Suggs, L.S. A 10-year retrospective of research in new technologies for health communication. J. Health Commun. 2006, 11, 61–74. [Google Scholar] [CrossRef] [PubMed]
- Trevena, L.J.; Barratt, A.; Butow, P.; Caldwell, P. A systematic review on communicating with patients about evidence. J. Eval. Clin. Pract. 2006, 12, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Luckmann, R.; Vidal, A. Design of a handheld electronic pain, treatment and activity diary. J. Biomed. Inform. 2010, 43, S32–S36. [Google Scholar] [CrossRef] [PubMed]
- Handel, M.J. mHealth (Mobile Health)—Using Apps for health and wellness. Explore 2011, 7, 256–261. [Google Scholar] [CrossRef] [PubMed]
- Rosser, B.A.; Eccleston, C. Smartphone applications for pain management. J. Telemed. Telecare 2011, 17, 308–312. [Google Scholar] [CrossRef] [PubMed]
- Ozdalga, E.; Ozdalga, A.; Ahuja, N. The smartphone in medicine: A review of current and potential use among physicians and students. J. Med. Internet Res. 2012, 14, e128. [Google Scholar] [CrossRef] [PubMed]
- Greysen, S.R.; Kind, T.; Chretien, K. Online professionalism and the mirror of social media. J. Gen. Internal Med. 2010, 25, 1227–1229. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.; Abdullah, A. Telemedicine in a cloud—A review. In Proceedings of the 2011 IEEE Symposium on Computers Informatics (ISCI), Kuala Lumpur, Malaysia, 20–23 March 2011; pp. 776–781.
- Pombo, N.; Araújo, P.; Viana, J.; Junior, B.; Serrano, R. Contribution of web services to improve pain diaries experience. In Proceedings of The International MultiConference of Engineers and Computer Scientists, Hong Kong, China, 14–16 March 2012; Volume 1, pp. 589–592.
- Leow, J.J.; Pozo, M.E.; Groen, R.S.; Kushner, A.L. Social media in low-resource settings: A role for Twitter and Facebook in global surgery? Surgery 2012, 151, 767–769. [Google Scholar] [CrossRef] [PubMed]
- Allen, K.D.; Coffman, C.J.; Golightly, Y.M.; Stechuchak, K.M.; Keefe, F.J. Daily pain variations among patients with hand, hip, and knee osteoarthritis. Osteoarthr. Cartil. 2009, 17, 1275–1282. [Google Scholar] [CrossRef] [PubMed]
- Allen, K.D.; Coffman, C.J.; Golightly, Y.M.; Stechuchak, K.M.; Voils, C.I.; Keefe, F.J. Comparison of pain measures among patients with osteoarthritis. J. Pain 2010, 11, 522–527. [Google Scholar] [CrossRef] [PubMed]
- Anatchkova, M.D.; Saris-Baglama, R.N.; Kosinski, M.; Bjorner, J.B. Development and preliminary testing of a computerized adaptive assessment of chronic pain. J. Pain 2009, 10, 932–943. [Google Scholar] [CrossRef] [PubMed]
- Hahn, E.A.; Cella, D.; Bode, R.K.; Gershon, R.; Lai, J.S. Item banks and their potential applications to health status assessment in diverse populations. Med. Care 2006, 44, S189–S197. [Google Scholar] [CrossRef] [PubMed]
- Badr, H.; Laurenceau, J.-P.; Schart, L.; Basen-Engquist, K.; Turk, D. The daily impact of pain from metastatic breast cancer on spousal relationships: A dyadic electronic diary study. Pain 2010, 151, 644–654. [Google Scholar] [CrossRef] [PubMed]
- Mahn, F.; Hullemann, P.; Gockel, U.; Brosz, M.; Freynhagen, R.; Tölle, T.R.; Baron, R. Sensory symptom profiles and co-morbidities in painful radiculopathy. PLoS ONE 2011, 6, e18018. [Google Scholar] [CrossRef] [PubMed]
- Baron, R.; Tölle, T.R.; Gockel, U.; Brosz, M.; Freynhagen, R. A cross-sectional cohort survey in 2100 patients with painful diabetic neuropathy and postherpetic neuralgia: Differences in demographic data and sensory symptoms. Pain 2009, 146, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Broderick, J.E.; Schwartz, J.E.; Schneider, S.; Stone, A.A. Can end-of-day reports replace momentary assessment of pain and fatigue? J. Pain 2009, 10, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Schneider, S.; Stone, A.A.; Schwartz, J.E.; Broderick, J.E. Peak and end effects in patients’ daily recall of pain and fatigue: A within-subjects analysis. J. Pain 2011, 12, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Connelly, M.; Anthony, K.K.; Sarniak, R.; Bromberg, M.H.; Gil, K.M.; Schanberg, L.E. Parent pain responses as predictors of daily activities and mood in children with juvenile idiopathic arthritis: The utility of electronic diaries. J. Pain Symptom Manag. 2010, 39, 579–590. [Google Scholar] [CrossRef] [PubMed]
- Gaertner, J.; Elsner, F.; Pollmann-Dahmen, K.; Radbruch, L.; Sabatowski, R. Electronic pain diary: A randomized crossover study. J. Pain Symptom Manag. 2004, 28, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Ghinea, G.; Spyridonis, F.; Serif, T.; Frank, A.O. 3-D pain drawings-mobile data collection using a PDA. IEEE Trans. Inf. Technol. Biomed. 2008, 12, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Heiberg, T.; Kvien, T.K.; Dale, Ø.; Mowinckel, P.; Aanerud, G.J.; Songe-Møller, A.B.; Uhlig, T.; Hagen, K.B. Daily health status registration (patient diary) in patients with rheumatoid arthritis: A comparison between personal digital assistant and paper-pencil format. Arthritis Care Res. 2007, 57, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Jamison, R.N.; Gracely, R.H.; Raymond, S.A.; Levine, J.G.; Marino, B.; Herrmann, T.J.; Daly, M.; Fram, D.; Katz, N.P. Comparative study of electronic vs. paper VAS ratings: A randomized, crossover trial using healthy volunteers. Pain 2002, 99, 341–347. [Google Scholar] [CrossRef]
- Jamison, R.N.; Raymond, S.A.; Slawsby, E.A.; McHugo, G.J.; Baird, J.C. Pain assessment in patients with low back pain: Comparison of weekly recall and momentary electronic data. J. Pain 2006, 7, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Koroschetz, J.; Rehm, S.; Gockel, U.; Brosz, M.; Freynhagen, R.; Tölle, T.; Baron, R. Fibromyalgia and neuropathic pain—Differences and similarities. A comparison of 3057 patients with diabetic painful neuropathy and fibromyalgia. BMC Neurol. 2011, 11, 55. [Google Scholar] [CrossRef] [PubMed]
- Kvien, T.K.; Mowinckel, P.; Heiberg, T.; Dammann, K.L.; Dale, Ø.; Aanerud, G.J.; Alme, T.N.; Uhlig, T. Performance of health status measures with a pen based personal digital assistant. Ann. Rheum. Dis. 2005, 64, 1480–1484. [Google Scholar] [CrossRef] [PubMed]
- Lewandowski, A.S.; Palermo, T.M.; De la Motte, S.; Fu, R. Temporal daily associations between pain and sleep in adolescents with chronic pain versus healthy adolescents. Pain 2010, 151, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Levin, E.; Levin, A. Evaluation of spoken dialogue technology for real-time health data collection. J. Med. Internet Res. 2006, 8, e30. [Google Scholar] [CrossRef] [PubMed]
- Li, L. The effect of neuragen PN(R) on neuropathic pain: A randomized, double blind, placebo controlled clinical trial. BMC Complement. Altern. Med. 2010, 10, 22. [Google Scholar] [CrossRef] [PubMed]
- Lind, L.; Karlsson, D.; Fridlund, B. Patients’ use of digital pens for pain assessment in advanced palliative home healthcare. Int. J. Med. Informa. 2008, 77, 129–136. [Google Scholar] [CrossRef] [PubMed]
- Marceau, L.D.; Link, C.L.; Smith, L.D.; Carolan, S.J.; Jamison, R.N. In-clinic use of electronic pain diaries: Barriers of implementation among pain physicians. J. Pain Symptom Manag. 2010, 40, 391–404. [Google Scholar] [CrossRef] [PubMed]
- Okifuji, A.; Bradshaw, D.H.; Donaldson, G.W.; Turk, D.C. Sequential analyses of daily symptoms in women with fibromyalgia syndrome. J. Pain 2011, 12, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Page, D.B.; Weaver, F.; Wilkie, D.J.; Simuni, T. A computerized survey of pain in Parkinson’s disease patients: A pilot feasibility study. Parkinsonism Relat. Disord. 2010, 16, 139–141. [Google Scholar] [CrossRef] [PubMed]
- Bieri, D.; Reeve, R.A.; Champion, G.D.; Addicoat, L.; Ziegler, J.B. The faces pain scale for the self-assessment of the severity of pain experienced by children: Development, initial validation, and preliminary investigation for ratio scale properties. Pain 1990, 41, 139–150. [Google Scholar] [CrossRef]
- Peters, M.L.; Sorbi, M.J.; Kruise, D.A.; Kerssens, J.J.; Verhaak, P.F.M.; Bensing, J.M. Electronic diary assessment of pain, disability and psychological adaptation in patients differing in duration of pain. Pain 2000, 84, 181–192. [Google Scholar] [CrossRef]
- Roelofs, J.; Peters, M.L.; Patijn, J.; Schouten, E.G.W.; Vlaeyen, J.W.S. Electronic diary assessment of pain-related fear, attention to pain, and pain intensity in chronic low back pain patients. Pain 2004, 112, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Sorbi, J.M.; Mak, B.S.; Houtveen, H.J.; Kleiboer, M.A.; van Doornen, J.L. Mobile web-based monitoring and coaching: Feasibility in chronic migraine. J. Med. Internet Res. 2007, 9, e38. [Google Scholar] [CrossRef] [PubMed]
- Stinson, J.N.; Stevens, B.J.; Feldman, B.M.; Streiner, D.; McGrath, P.J.; Dupuis, A.; Gill, N.; Petroz, G.C. Construct validity of a multidimensional electronic pain diary for adolescents with arthritis. Pain 2008, 136, 281–292. [Google Scholar] [CrossRef] [PubMed]
- Stinson, J.; Connelly, M.; Jibb, L.; Schanberg, L.; Walco, G.; Spiegel, L.; Tse, S.; Chalom, E.; Chira, P.; Rapoff, M. Developing a standardized approach to the assessment of pain in children and youth presenting to pediatric rheumatology providers: A Delphi survey and consensus conference process followed by feasibility testing. Pediatr. Rheumatol. 2012, 10, 7. [Google Scholar] [CrossRef] [PubMed]
- Wallasch, T.-M.; Hermann, C. Validation of criterion-based patient assignment and treatment effectiveness of a multidisciplinary modularized managed care program for headache. J. Headache Pain 2012, 13, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Van Weering, M.; Vollenbroek-Hutten, M.; Hermens, H. Do personalized feedback messages about activity patterns stimulate patients with chronic low back pain to change their activity behavior on a short term notice? Appl. Psychophysiol. Biofeedback 2012, 37, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Younger, J.; Mackey, S. Fibromyalgia symptoms are reduced by low-dose naltrexone: A pilot study. Pain Med. 2009, 10, 663–672. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.M.; Compton, P.; Bolus, R.; Schieffer, B.; Pham, Q.; Baria, A.; van Vort, W.; Davis, F.; Shekelle, P.; Naliboff, B.D. The addiction behaviors checklist: Validation of a new clinician-based measure of inappropriate opioid use in chronic pain. J. Pain Symptom Manag. 2006, 32, 342–351. [Google Scholar] [CrossRef] [PubMed]
- Kuorinka, I.; Jonsson, B.; Kilbom, A.; Vinterberg, H.; Biering-Sørensen, F.; Andersson, G.; Jørgensen, K. Standardised nordic questionnaires for the analysis of musculoskeletal symptoms. Appl. Ergon. 1987, 18, 233–237. [Google Scholar] [CrossRef]
- Walker, L.S.; Levy, R.L.; Whitehead, W.E. Validation of a measure of protective parent responses to children’s pain. Clin. J. Pain 2006, 22, 712–716. [Google Scholar] [CrossRef] [PubMed]
- McGahuey, C.A.; Gelenberg, A.J.; Laukes, C.A.; Moreno, F.A.; Delgado, P.L.; McKnight, K.M.; Manber, R. The arizona sexual experience scale (ASEX): Reliability and validity. J. Sex Marital. Ther. 2000, 26, 25–40. [Google Scholar] [PubMed]
- Peterson, R.A.; Heilbronner, R.L. The anxiety sensitivity index: Construct validity and factor analytic structure. J. Anxiety Disord. 1987, 1, 117–121. [Google Scholar] [CrossRef]
- Reynolds, C.R. Behavior assessment system for children. In The Corsini Encyclopedia of Psychology; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2010. [Google Scholar]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [PubMed]
- Mendoza, T.R.; Wang, X.S.; Cleeland, C.S.; Morrissey, M.; Johnson, B.A.; Wendt, J.K.; Huber, S.L. The rapid assessment of fatigue severity in cancer patients: Use of the brief fatigue inventory. Cancer 1999, 85, 1186–1196. [Google Scholar] [CrossRef]
- Cleeland, C.S.; Ryan, K.M. Pain assessment: Global use of the brief pain inventory. Ann. Acad. Med. Singap. 1994, 23, 129–138. [Google Scholar] [PubMed]
- Derogatis, L.R.; Melisaratos, N. The brief symptom inventory: An introductory report. Psychol. Med. 1983, 13, 595–605. [Google Scholar] [CrossRef] [PubMed]
- Palermo, T.M.; Witherspoon, D.; Valenzuela, D.; Drotar, D.D. Development and validation of the Child activity limitations interview: A measure of pain-related functional impairment in school-age children and adolescents. Pain 2004, 109, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Hainsworth, K.R.; Davies, W.H.; Khan, K.A.; Weisman, S.J. Development and preliminary validation of the child activity limitations questionnaire: Flexible and efficient assessment of pain-related functional disability. J. Pain 2007, 8, 746–752. [Google Scholar] [CrossRef] [PubMed]
- Radloff, L.S. The CES-D scale. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- McCracken, L.M.; Vowles, K.E.; Eccleston, C. Acceptance of chronic pain: Component analysis and a revised assessment method. Pain 2004, 107, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Jamison, R.N. Mastering Chronic Pain: A Professional’s Guide to Behavioral Treatment; Professional Resource Exchange Inc.: Sarasota, FL, USA, 1996. [Google Scholar]
- Hunt, M.G.; Milonova, M.; Moshier, S. Catastrophizing the consequences of gastrointestinal symptoms in irritable bowel syndrome. J. Cogn. Psychother. 2009, 23, 160–173. [Google Scholar] [CrossRef]
- Butler, S.F.; Budman, S.H.; Fernandez, K.C.; Houle, B.; Benoit, C.; Katz, N.; Jamison, R.N. Development and validation of the current opioid misuse measure. Pain 2007, 130, 144–156. [Google Scholar] [CrossRef] [PubMed]
- Garber, J.; Walker, L.S.; Zeman, J. Somatization symptoms in a community sample of children and adolescents: Further validation of the children‘s somatization inventory. Psychol. Assess. 1991, 3, 588–595. [Google Scholar] [CrossRef]
- Rosenstiel, A.K.; Keefe, F.J. The use of coping strategies in chronic low back pain patients: Relationship to patient characteristics and current adjustment. Pain 1983, 17, 33–44. [Google Scholar] [CrossRef]
- Toner, B.B.; Stuckless, N.; Ali, A.; Downie, F.; Emmott, S.; Akman, D. The development of a cognitive scale for functional bowel disorders. Psychosom. Med. 1998, 60, 492–497. [Google Scholar] [CrossRef] [PubMed]
- Crawford, J.R.; Henry, J.D. The depression anxiety stress scales (DASS): Normative data and latent structure in a large non-clinical sample. Br. J. Clin. Psychol. 2003, 42, 111–131. [Google Scholar] [CrossRef] [PubMed]
- Stone, A.A.; Neale, J.M. New measure of daily coping: Development and preliminary results. J. Pers. Soc. Psychol. 1984, 46, 892–906. [Google Scholar] [CrossRef]
- EuroQol Group. EuroQol—A new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar]
- Burckhardt, C.S.; Clark, S.R.; Bennett, R.M. The fibromyalgia impact questionnaire: Development and validation. J. Rheumatol. 1991, 18, 728–733. [Google Scholar] [PubMed]
- Newman, M.G.; Zuellig, A.R.; Kachin, K.E.; Constantino, M.J.; Przeworski, A.; Erickson, T.; Cashman-McGrath, L. Preliminary reliability and validity of the generalized anxiety disorder questionnaire-IV: A revised self-report diagnostic measure of generalized anxiety disorder. Behav. Ther. 2002, 33, 215–233. [Google Scholar] [CrossRef]
- Korff, M.V.; Ormel, J.; Keefe, F.J.; Dworkin, S.F. Grading the severity of chronic pain. Pain 1992, 50, 133–149. [Google Scholar] [CrossRef]
- Svedlund, J.; Sjodin, I.; Dotevall, G. GSRS—A clinical rating scale for gastrointestinal symptoms in patients with irritable bowel syndrome and peptic ulcer disease. Dig. Dis. Sci. 1988, 33, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Patrick, D.; Drossman, D.; Frederick, I.; Dicesare, J.; Puder, K. Quality of life in persons with irritable bowel syndrome (development and validation of a new measure). Dig. Dis. Sci. 1998, 43, 400–411. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; Oja, P. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Ramey, D.R.; Raynauld, J.-P.; Fries, J.F. The health assessment questionnaire 1992. Status and review. Arthritis Rheum. 1992, 5, 119–129. [Google Scholar] [CrossRef]
- Jacobson, G.P.; Ramadan, N.M.; Aggarwal, S.K.; Newman, C.W. The henry ford hospital headache disability inventory (HDI). Neurology 1994, 44, 837–842. [Google Scholar] [CrossRef] [PubMed]
- Moriarty, D.; Zack, M.; Kobau, R. The centers for disease control and prevention’s healthy days measures—Population tracking of perceived physical and mental health over time. Health Qual. Life Outcomes 2003, 1, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Derogatis, L.R.; Lipman, R.S.; Rickels, K.; Uhlenhuth, E.H.; Covi, L. The hopkins symptom checklist (HSCL). A measure of primary symptom dimensions. Mod. Probl. Pharmacopsychiat. 1974, 7, 79–110. [Google Scholar]
- Arena, J.; Blanchard, E.; Andrasik, F.; Dudek, B. The headache symptom questionnaire: Discriminant classificatory ability and headache syndromes suggested by a factor analysis. J. Behav. Assess. 1982, 4, 55–69. [Google Scholar] [CrossRef]
- Svanborg, P.; Asberg, M. A new self-rating scale for depression and anxiety states based on the comprehensive psychopathological rating scale. Acta Psychiatr. Scand. 1994, 89, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Seidenberg, M.; Haltiner, A.; Taylor, M.A.; Hermann, B.B.; Wyler, A. Development and validation of a multiple ability self-report questionnaire. J. Clin. Exp. Neuropsychol. 1994, 16, 93–104. [Google Scholar] [CrossRef] [PubMed]
- Pincus, T.; Swearingen, C.; Wolfe, F. Toward a multidimensional health assessment questionnaire (MDHAQ): Assessment of advanced activities of daily living and psychological status in the patient-friendly health assessment questionnaire format. Arthritis Rheum. 1999, 42, 2220–2230. [Google Scholar] [CrossRef]
- Smets, E.M.; Garssen, B.; Bonke, B.; De Haes, J.C. The multidimensional fatigue inventory (MFI) psychometric qualities of an instrument to assess fatigue. J. Psychosom. Res. 1995, 39, 315–325. [Google Scholar] [CrossRef]
- Pincus, T.; Summey, J.A.; Soraci, S.A.; Wallston, K.A.; Hummon, N.P. Assessment of patient satisfaction in activities of daily living using a modified stanford health assessment questionnaire. Arthritis Rheum. 1983, 26, 1346–1353. [Google Scholar] [CrossRef] [PubMed]
- Stewart, W.F.; Lipton, R.B.; Whyte, J.; Dowson, A.; Kolodner, K.; Liberman, J.N.; Sawyer, J. An international study to assess reliability of the migraine disability assessment (MIDAS) score. Neurology 1999, 53, 988–994. [Google Scholar] [CrossRef] [PubMed]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The mini-international neuropsychiatric interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiat. 1998, 59, S22–S33. [Google Scholar]
- Kuile, M.; Linssen, A.C.; Spinhoven, P. The development of the multidimensional locus of pain control questionnaire (MLPC): Factor structure, reliability, and validity. J. Psychopathol. Behav. Assess. 1993, 15, 387–404. [Google Scholar] [CrossRef]
- Hays, R.D.; Martin, S.A.; Sesti, A.M.; Spritzer, K.L. Psychometric properties of the medical outcomes study sleep measure. Sleep Med. 2005, 6, 41–44. [Google Scholar] [CrossRef] [PubMed]
- Kerns, R.D.; Turk, D.C.; Rudy, T.E. The west haven-yale multidimensional pain inventory (WHYMPI). Pain 1985, 23, 345–356. [Google Scholar] [CrossRef]
- Melzack, R. The McGill pain questionnaire: Major properties and scoring methods. Pain 1975, 1, 277–299. [Google Scholar] [CrossRef]
- Johnson, C. Measuring pain. Visual analog scale versus numeric pain scale: What is the difference? J. Chiropr. Med. 2005, 4, 43–44. [Google Scholar] [CrossRef]
- Fairbank, J.C.; Pynsent, P.B. The oswestry disability index. Spine 2000, 25, 2940–2952. [Google Scholar] [CrossRef] [PubMed]
- Riley, J.F.; Ahern, D.K.; Follick, M.J. Chronic pain and functional impairment: Assessing beliefs about their relationship. Arch. Phys. Med. Rehabil. 1988, 69, 579–582. [Google Scholar] [PubMed]
- Laurent, J.; Catanzaro, S.J.; Joiner, T.E. Development and preliminary validation of the physiological hyperarousal scale for children. Psychol. Assess. 2004, 16, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Ruehlman, L.S.; Karoly, P.; Newton, C.; Aiken, L.S. The development and preliminary validation of the profile of chronic pain: Extended assessment battery. Pain 2005, 118, 380–389. [Google Scholar] [CrossRef] [PubMed]
- Ruehlman, L.S.; Karoly, P.; Newton, C.; Aiken, L.S. The development and preliminary validation of a brief measure of chronic pain impact for use in the general population. Pain 2005, 113, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Reid, G.J.; Gilbert, C.A.; McGrath, P.J. The pain coping questionnaire: Preliminary validation. Pain 1998, 76, 83–96. [Google Scholar] [CrossRef]
- Crombez, G.; Bijttebier, P.; Eccleston, C.; Mascagni, T.; Mertens, G.; Goubert, L.; Verstraeten, K. The child version of the pain catastrophizing scale (PCS-C): A preliminary validation. Pain 2003, 104, 639–646. [Google Scholar] [CrossRef]
- Stern, B.L.; Kim, Y.; Trull, T.J.; Scarpa, A.; Pilkonis, P. Inventory of interpersonal problems personality disorder scales: Operating characteristics and confirmatory factor analysis in nonclinical samples. J. Pers. Assess. 2000, 74, 459–471. [Google Scholar] [CrossRef] [PubMed]
- Freynhagen, R.; Baron, R.; Gockel, U.; Tölle, T.R. painDETECT: A new screening questionnaire to identify neuropathic components in patients with back pain. Curr. Med. Res. Opin. 2006, 22, 1911–1920. [Google Scholar] [CrossRef] [PubMed]
- Tait, R.C.; Pollard, C.A.; Margolis, R.B.; Duckro, P.N.; Krause, S.J. The pain disability index: Psychometric and validity data. Arch. Phys. Med. Rehabil. 1987, 68, 438–441. [Google Scholar] [PubMed]
- Jenkinson, C.; Fitzpatrick, R.; Peto, V.; Greenhall, R.; Hyman, N. The Parkinson’s disease questionnaire (PDQ-39): Development and validation of a Parkinson’s disease summary index score. Age Ageing 1997, 26, 353–357. [Google Scholar] [CrossRef] [PubMed]
- Compton, P.; Darakjian, J.; Miotto, K. Screening for addiction in patients with chronic pain and “problematic” substance use: Evaluation of a pilot assessment tool. J. Pain Symptom Manag. 1998, 16, 355–363. [Google Scholar] [CrossRef]
- Varni, J.W.; Seid, M.; Rode, C.A. The PedsQL: Measurement model for the pediatric quality of life inventory. Med. Care 1999, 37, 126–139. [Google Scholar] [CrossRef] [PubMed]
- Dworkin, R.H.; Turk, D.C.; Farrar, J.T.; Haythornthwaite, J.A.; Jensen, M.P.; Katz, N.P.; Kerns, R.D.; Stucki, G.; Allen, R.R.; Bellamy, N.; et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain 2005, 113, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Lowe, B.; Kroenke, K.; Herzog, W.; Grafe, K. Measuring depression outcome with a brief self-report instrument: Sensitivity to change of the patient health questionnaire (PHQ-9). J. Affect. Disord. 2004, 81, 61–66. [Google Scholar] [CrossRef]
- Nicholas, M.K. The pain self-efficacy questionnaire: Taking pain into account. Eur. J. Pain 2007, 11, 153–163. [Google Scholar] [CrossRef] [PubMed]
- McCracken, L.M. “Attention” to pain in persons with chronic pain: A behavioral approach. Behav. Ther. 1997, 28, 271–284. [Google Scholar] [CrossRef]
- Kopec, J.A.; Esdaile, J.M.; Abrahamowicz, M.; Abenhaim, L.; Wood-Dauphinee, S.; Lamping, D.L.; Williams, J.I. The quebec back pain disability scale. Measurement properties. Spine 1995, 20, 341–352. [Google Scholar] [CrossRef] [PubMed]
- Fransen, J.; Langenegger, T.; Michel, B.A.; Stucki, G. Feasibility and validity of the RADAI, a self-administered rheumatoid arthritis disease activity index. Rheumatology 2000, 39, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Chorpita, B.F.; Moffitt, C.E.; Gray, J. Psychometric properties of the revised child anxiety and depression scale in a clinical sample. Behav. Res. Ther. 2005, 43, 309–322. [Google Scholar] [CrossRef] [PubMed]
- Riddle, D.L.; Stratford, P.W. Roland-morris scale reliability. Phys. Ther. 2002, 82, 512–517. [Google Scholar] [PubMed]
- Derogatis, L.R.; Unger, R. Symptom Checklist-90-Revised. In The Corsini Encyclopedia of Psychology; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2010. [Google Scholar]
- Sheehan, K.H.; Sheehan, D.V. Assessing treatment effects in clinical trials with the discan metric of the sheehan disability scale. Int. Clin. Psychopharmacol. 2008, 23, 70–83. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Butler, S.F.; Budman, S.H.; Fernandez, K.; Jamison, R.N. Validation of a screener and opioid assessment measure for patients with chronic pain. Pain 2004, 112, 65–75. [Google Scholar] [CrossRef] [PubMed]
- Hellsten, L.A.; Nigg, C.; Norman, G.; Burbank, P.; Braun, L.; Breger, R.; Coday, M.; Elliot, D.; Garber, C.; Greaney, M.; et al. Accumulation of behavioral validation evidence for physical activity stage of change. Health Psychol. 2008, 27, 43–53. [Google Scholar] [CrossRef]
- Jensen, M.P.; Turner, J.A.; Romano, J.M.; Lawler, B.K. Relationship of pain-specific beliefs to chronic pain adjustment. Pain 1994, 57, 301–309. [Google Scholar] [CrossRef]
- Spielberger, C.D. State-trait anxiety inventory. In The Corsini Encyclopedia of Psychology; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2010. [Google Scholar]
- Spielberger, C.D.; Reheiser, E.C. Assessment of emotions: Anxiety, anger, depression, and curiosity. Appl. Psychol. Health Well-Being 2009, 1, 271–302. [Google Scholar] [CrossRef]
- Goubert, L.; Crombez, G.; van Damme, S.; Vlaeyen, J.W.; Bijttebier, P.; Roelofs, J. Confirmatory factor analysis of the Tampa Scale for Kinesiophobia: Invariant two-factor model across low back pain patients and fibromyalgia patients. Clin. J. Pain 2004, 20, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Shulman, L.M.; Gruber-Baldini, A.L.; Anderson, K.E.; Fishman, P.S.; Reich, S.G.; Weiner, W.J. The clinically important difference on the unified parkinson’s disease rating scale. Arch. Neurol. 2010, 67, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Carlsson, A.M. Assessment of chronic pain. I. Aspects of the reliability and validity of the visual analogue scale. Pain 1983, 16, 87–101. [Google Scholar] [CrossRef]
- Labus, J.S.; Bolus, R.; Chang, L.; Wiklund, I.; Naesdal, J.; Mayer, E.A.; Naliboff, B.D. The visceral sensitivity index: Development and validation of a gastrointestinal symptom-specific anxiety scale. Aliment. Pharmacol. Ther. 2004, 20, 89–97. [Google Scholar] [CrossRef] [PubMed]



| Pain intensity | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Study | Variable | Technology | Pen and Paper | Technology | Pen and Paper | Favourable To | ||||
| Pre Treatment | Post Treatment | Pre Treatment | Post Treatment | Aggregated Value | SD | Aggregated Value | SD | |||
| Value (SD) | Value (SD) | Value (SD) | Value (SD) | |||||||
| Berman [41] | BPI (mean) | 52 (19.40) | 45.60 (18.30) | 54.30 (17.40) | 47.30 (18.40) | 48.61 | 13.31 | 51 | 12.64 | Technology |
| Buhrman [36] | Pain (mean) | 37.40 (18.20) | 34.30 (16.80) | 44.4 (14.20) | 39.6 (16.30) | 35.73 | 12.34 | 42.33 | 10.71 | Technology |
| MP—pa in severity | 63.33 (31.67) | 40 (18.33) | 83.33 (28.33) | 53.33 (13.33) | 45.86 | 15.87 | 58.77 | 12.06 | Technology | |
| Devineni [42] | Headache pain | 31.80 (17) | 18.60 (13) | 35.50 (15.50) | 30.60 (14.70) | 23.47 | 10.33 | 32.92 | 10.67 | Technology |
| Hicks [43] | Pain (mean) | 48 (13) | 34 (24) | 43 (16) | 47 (22) | 44.82 | 11.43 | 44.38 | 12.94 | Pen-and-Paper |
| Litt [44] | MPI (mean) | 43.83 (21) | 20.50 (16.33) | 35.17 (14.33) | 25 (22.67) | 29.29 | 12.89 | 32.26 | 12.11 | Technology |
| Ljótsson [45] | Pain | 65 (42.50) | 35 (37.50) | 60 (37.50) | 60 (40) | 48.13 | 28.12 | 60 | 27.36 | Technology |
| Lorig [39] | Pain | 65.30 (22.70) | 58.60 (24.40) | 63.70 (22.20) | 63.40 (23.10) | 62.19 | 16.62 | 63.56 | 16.01 | Technology |
| Palermo [37] | Pain | 54.50 (22.50) | 35.40 (24.20) | 51.70 (16.50) | 47.60 (18.40) | 45.64 | 16.48 | 49.87 | 12.28 | Technology |
| Retrospective pain | 66.30 (18.70) | 49.60 (21.80) | 61.60 (18.40) | 54.50 (20.40) | 59.22 | 14.19 | 58.42 | 13.66 | Pen-and-Paper | |
| Ruehlman [46] | PCP-S—pain severity | 76.47 (9.72) | 71.10 (12.94) | 74.78 (10.91) | 71.66 (13.28) | 74.53 | 7.77 | 73.52 | 8.43 | Pen-and-Paper |
| Turner [47] | Pain (mean) | 43 (22) | 39 (24) | 43 (19) | 40 (22) | 41.17 | 16.22 | 41.72 | 14.38 | Technology |
| Williams [48] | BPI—pain severity | 51 (14) | 43 (16) | 49 (14) | 49 (15) | 47.53 | 10.54 | 49 | 10.23 | Technology |
| Fusion | value | 55.90 (4.80) | 40.57 (5.08) | 52.65 (4.56) | 49.02 (4.94) | 48.67 | 3.49 | 50.98 | 3.35 | Equivalent |
| alpha | 23.04 | 25.82 | 20.79 | 24.38 | ||||||
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pombo, N.; Garcia, N.; Bousson, K.; Spinsante, S.; Chorbev, I. Pain Assessment–Can it be Done with a Computerised System? A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2016, 13, 415. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13040415
Pombo N, Garcia N, Bousson K, Spinsante S, Chorbev I. Pain Assessment–Can it be Done with a Computerised System? A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2016; 13(4):415. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13040415
Chicago/Turabian StylePombo, Nuno, Nuno Garcia, Kouamana Bousson, Susanna Spinsante, and Ivan Chorbev. 2016. "Pain Assessment–Can it be Done with a Computerised System? A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 13, no. 4: 415. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13040415