
Mitigating Stress and Supporting Health in Deprived Urban Communities: The Importance of Green Space and the Social Environment

 ,
,
Abstract
:1. Introduction
- (a)
- What measures of quantity or use of local green space are associated with differences in stress levels in deprived urban communities?
- (b)
- Are physical activity or social wellbeing variables also associated with differences in stress levels in deprived urban communities, and how do these relate to green space variables?
- (c)
- Are any relationships between quantity or use of local green space and stress also found for general health as an outcome?
- (d)
- Do physical activity or social wellbeing variables play a role in predicting general health?
2. Materials and Methods
2.1. Study Design
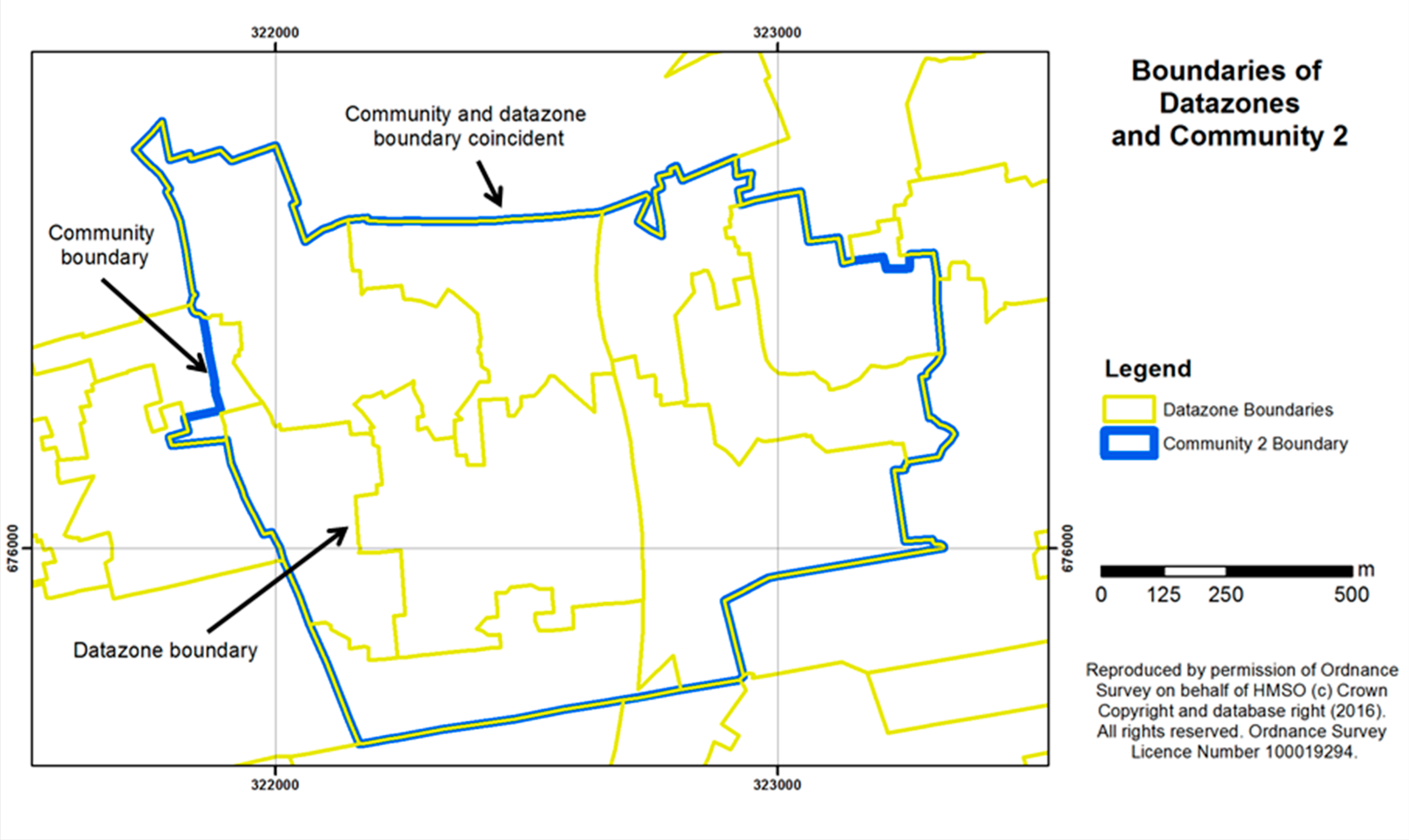
2.2. Choice of Study Sites
2.3. Recruitment of Sample
2.4. Measures
2.4.1. Individual Level Health and Wellbeing Variables
2.4.2. Other Individual Characteristics
2.4.3. Area-Level Deprivation
2.4.4. Self-Reported Access to Green Space
2.4.5. Objective Measures of Green Space
2.5. Characteristics of the Sample
2.6. Approach to Analysis
3. Results
3.1. Predicting Stress
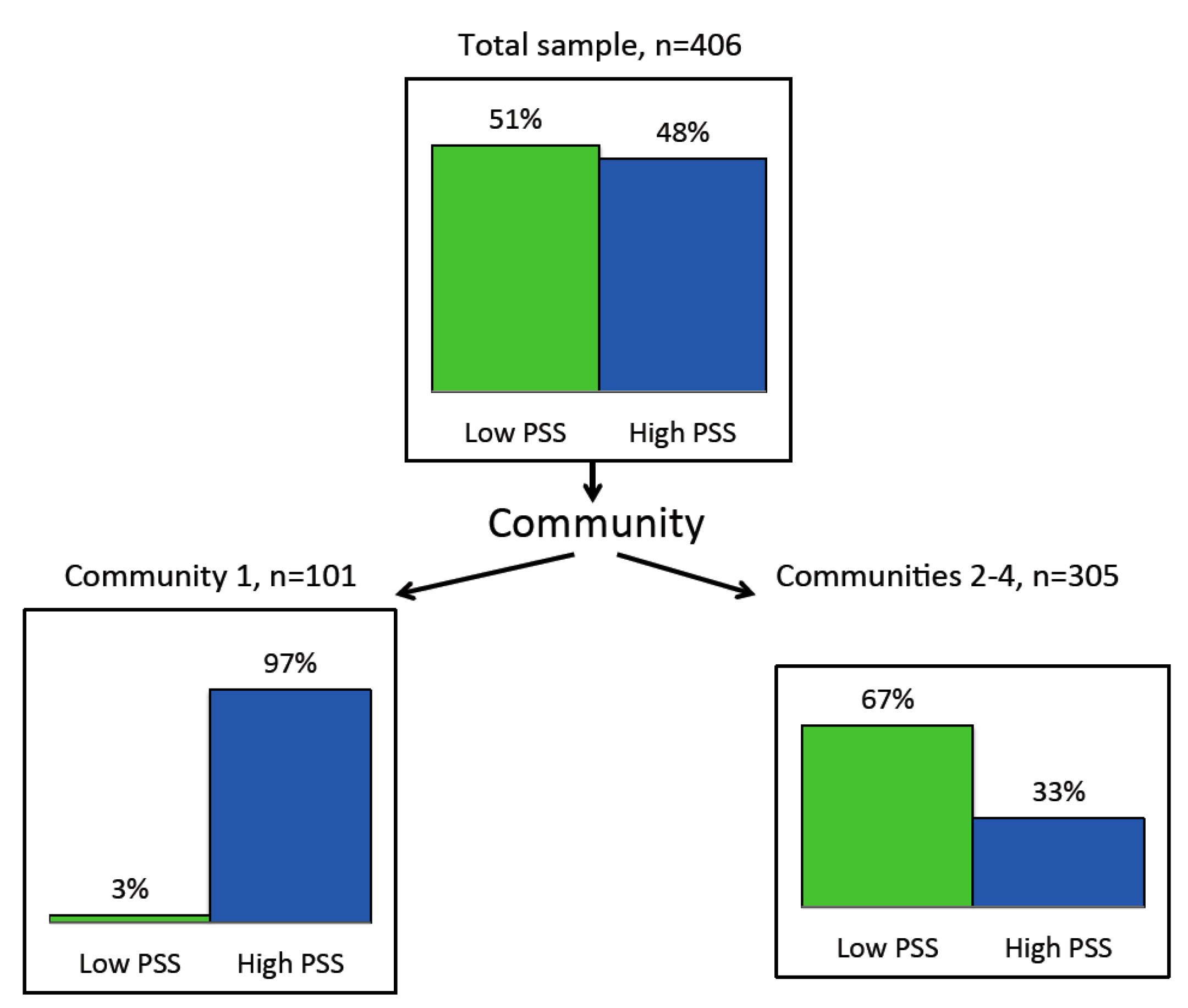
3.1.1. Segments in the Sample
3.1.2. Predictors of Perceived Stress in Community 1
3.1.3. Predictors of Perceived Stress in Communities 2, 3 and 4
3.2. Predicting General Health
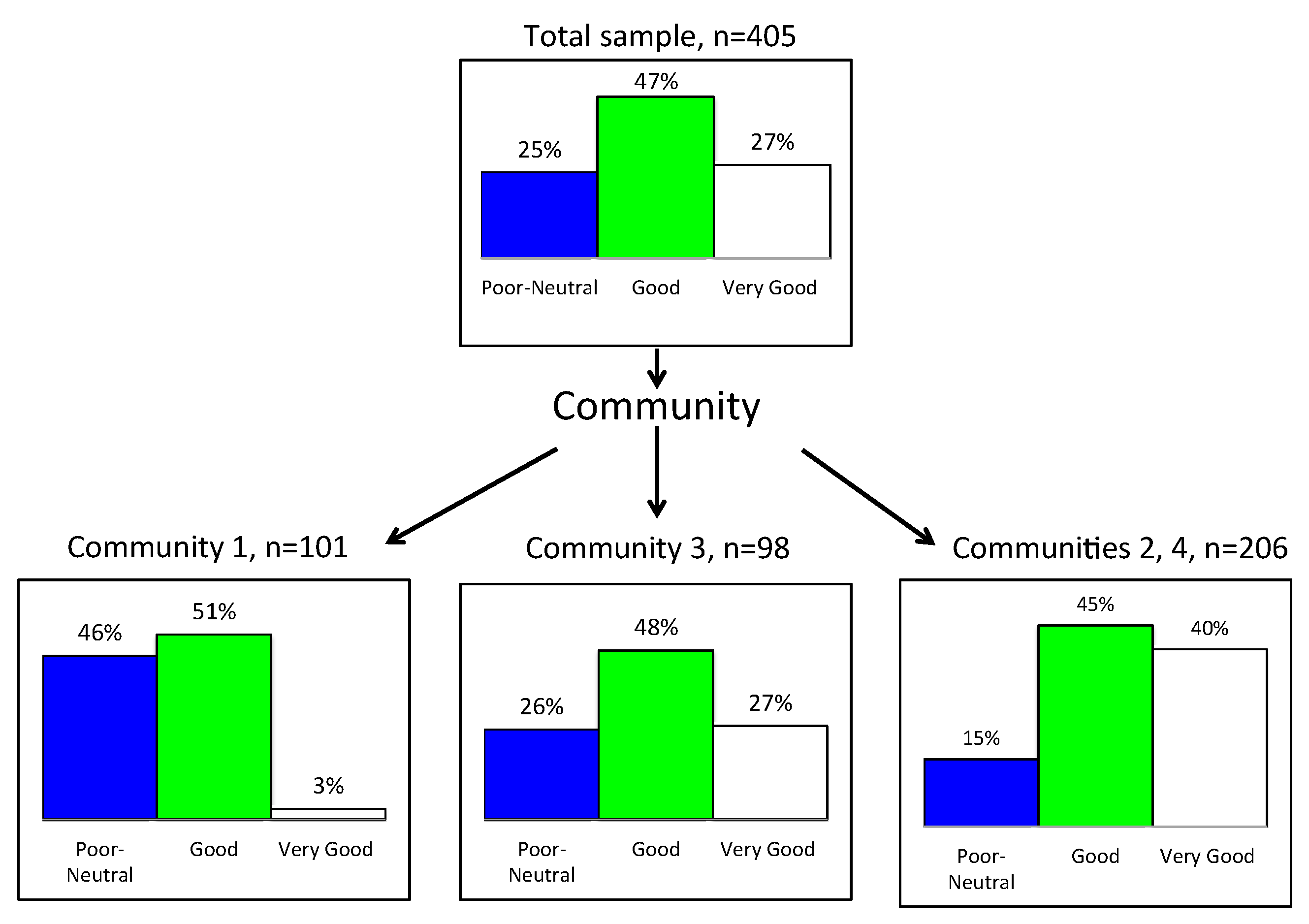
3.2.1. Segments in the Sample
3.2.2. Predictors of General Health in Community 1
3.2.3. Predictors of General Health in Community 3
3.2.4. Predictors of General Health in Communities 2 and 4
3.3. Potential Mediation between Green Space Variables and Perceived Stress
3.3.1. Percentage Green Space Area and Stress
3.3.2. Having a Garden or Allotment and Stress
3.3.3. Having a View of Green Space or Hills from the Home and Stress
4. Discussion
4.1. Characteristics of Access to Green Space Associated with Differences in Perceived Stress Levels
4.2. Physical Activity or Social Wellbeing Variables Associated with Differences in Perceived Stress Levels
4.3. Relationships between Access to Local Green Space and General Health
4.4. Different Sub-Groups in the Sample
4.5. Links to Underlying Mechanisms or Pathways
- The restorative qualities offered by views of green and natural places may contribute to general health (as exemplified in Community 1 by the role of views to green space and hills) via physiological responses that have been demonstrated in a number of studies [4,6,21] The quantity of green space in the neighbourhood, perhaps including views of green space, appears to contribute to place belonging (as exemplified in Communities 2, 3 and 4) and may thereby also contribute to general health, although this link is more tenuous. The fact that percentage of green space was more strongly associated with perceived stress levels than the frequency of visits to green space suggests that it may be green space experienced in moving about the residential neighbourhood while focused on goals other than visiting green space, that is the important factor here. Such findings support earlier studies showing links between chronic stress and percentage green space or natural environment in the residential area [7,8,67].
- The support that parks, open space and allotments offer for neighbourhood contact and maintenance of community connections, which reduce social isolation and enhance place belonging, may explain the association between the percentage of green space in the neighbourhood and lower perceived stress levels. This confirms earlier findings on links between social cohesion or belonging and residential green space [35,36] and supports evidence from neuroscience that sense of place and place identity, in which the social and natural environment have particular roles, are important dimensions for human health [68]. Future research could usefully distinguish between the value of private gardens versus shared gardens and allotments, where greater social interaction with neighbours is likely. The mediating role of social wellbeing variables may explain why, in our study, views of green space or hills from the home were not associated with stress, while percentage of residential green space and gardens or allotments were.
- The support that parks and open space offer for year-round physical activity and outdoor recreational access, especially in winter months, may explain the relationship between access to green space and general health (as exemplified in Communities 2, 3 and 4). Several studies have shown a positive association between frequency of visits to, and/or time spent in, nearby green space and levels of physical activity [69,70], which in turn predict health [23], although the international evidence for associations between green space and levels of physical activity, remains equivocal, suggesting that the relationship may vary considerably between countries and population sub-groups [37].
- Of the individual characteristics, the variables associated both with perceived stress levels (in Communities 2, 3 and 4) and general health (in Community 1) were: employment, age, and whether or not there are children under 16 in the household. Unsurprisingly, being in full-time employment was associated with lower perceived stress and better health. However, older age was associated with lower stress but poorer general health. Other studies have shown that older age is associated with an increase in poor health and multi-morbidity, especially among deprived populations [71] but also that the relationship between the amount of green space and health is stronger among older people [72], with a significant association demonstrated between a green environment and levels of physical activity for those aged over 60 years [73]. Future research might usefully explore such interactions further in deprived urban communities. In our study, having children in the household was associated with higher stress but better general health; this latter finding may reflect participants’ younger age where there are children in the household. While caring for children may add to stress in adults, the importance for both parents and children of green space near the home is highlighted in recent research which identifies links between positive birth outcomes and access to green space [74,75], as well as between green space and children’s wellbeing [70,76,77]. Again, future research might usefully explore these interactions in deprived communities such as those of our study.
4.6. Limitations
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Mitchell, R.; Popham, F. Effect of exposure to natural environment on health inequalities: An observational population study. Lancet 2008, 372, 1655–1660. [Google Scholar] [CrossRef]
- Maas, J.; Verheij, R.A.; de Vries, S.; Spreeuwenberg, P.; Schellevis, F.G.; Groenewegen, P.P. Morbidity is related to a green living environment. J. Epidemiol. Commun. Health 2009, 63, 967–973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitchell, R.J.; Richardson, E.A.; Shortt, N.K.; Pearce, J.R. Neighborhood environments and socioeconomic inequalities in mental well-being. Am. J. Prev. Med. 2015, 49, 80–84. [Google Scholar] [CrossRef] [PubMed]
- Park, B.J.; Tsunetsugu, Y.; Kasetani, T.; Hirano, H.; Kagawa, T.; Sato, M.; Miyazaki, Y. Physiological effects of Shinrin-yoku (taking in the atmosphere of the forest)—Using salivary cortisol and cerebral activity as indicators. J. Physiol. Anthropol. 2007, 26, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Park, B.J.; Tsunetsugu, Y.; Kasetani, T.; Kagawa, T.; Miyazaki, Y. The physiological effects of Shinrin-Yoku (taking in the forest atmosphere or forest bathing): Evidence from field experiments in 24 forests across Japan. Environ. Health Prev Med. 2010, 15, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Park, B.J.; Tsunetsugu, Y.; Ohira, T.; Kagawa, T.; Miyazaki, Y. Effect of forest bathing on physiological and psychological responses in young Japanese male subjects. Public Health 2011, 125, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Ward Thompson, C.; Roe, J.; Aspinall, P.; Mitchell, R.; Clow, A.; Miller, D. More green space is linked to less stress in deprived communities: Evidence from salivary cortisol patterns. Landsc. Urban Plan. 2012, 105, 221–229. [Google Scholar] [CrossRef]
- Roe, J.J.; Thompson, C.W.; Aspinall, P.A.; Brewer, M.J.; Duff, E.I.; Miller, D.; Mitchell, R.; Clow, A. Green space and stress: Evidence from cortisol measures in deprived urban communities. Int. J. Environ. Res. Public Health 2013, 10, 4086–4103. [Google Scholar] [CrossRef] [PubMed]
- The Scottish Government. Place Standard. Available online: http://www.placestandard.scot/#/home (accessed on 19 November 2015).
- Szulczewska, B.; Giedych, R.; Borowski, J.; Kuchcik, M.; Sikorski, P.; Mazurkiewicz, A.; Stanczyk, T. How much green is needed for a vital neighbourhood? In search for empirical evidence. Land Use Policy 2014, 38, 330–345. [Google Scholar] [CrossRef]
- Jennings, V.; Johnson Gaither, C. Approaching environmental health disparities and green spaces: An ecosystem services perspective. Int. J. Environ. Res. Public Health 2015, 12, 1952–1968. [Google Scholar] [CrossRef] [PubMed]
- Jennings, V.; Larson, L.; Yun, J. Advancing sustainability through urban green space: Cultural ecosystem services, equity, and social determinants of health. Int. J. Environ. Res. Public Health 2016, 13. [Google Scholar] [CrossRef] [PubMed]
- Van Dillen, S.M.; de Vries, S.; Groenewegen, P.P.; Spreeuwenberg, P. Greenspace in urban neighbourhoods and residents’ health: Adding quality to quantity. J. Epidemiol. Commun. Health 2012, 66, e8. [Google Scholar] [CrossRef] [PubMed]
- Van Den Berg, A.E.; Custers, M.H. Gardening promotes neuroendocrine and affective restoration from stress. J. Health Psychol. 2011, 16, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, M.A.; Ramirez-Valles, J.; Zapert, K.M.; Maton, K.I. A longitudinal study of stress-buffering effects for urban African-American male adolescent problem behaviors and mental health. J. Commun. Psychol. 2000, 28, 17–33. [Google Scholar] [CrossRef]
- Van den Berg, A.E.; Maas, J.; Verheij, R.A.; Groenewegen, P.P. Green space as a buffer between stressful life events and health. Soc. Sci. Med. 2010, 70, 1203–1210. [Google Scholar] [CrossRef] [PubMed]
- Tarzia, V. European Common Indicators (ECI): Towards a Local Sustainability Profile; Final Project Report; Ambiente Italia Research Institute: Milan, Italy, 2003. [Google Scholar]
- Dinnie, E.; Brown, K.M.; Morris, S. Community, cooperation and conflict: Negotiating the social well-being benefits of urban greenspace experiences. Landsc. Urban Plan. 2013, 118, 103–111. [Google Scholar] [CrossRef]
- Macintyre, S.; Macdonald, L.; Ellaway, A. Lack of agreement between measured and self-reported distance from public green parks in Glasgow, Scotland. Int. J. Behav. Nutr. Phys. 2008, 5. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, S. The restorative benefits of nature—Toward an integrative framework. J. Environ. Psychol. 1995, 15, 169–182. [Google Scholar] [CrossRef]
- Ulrich, R.S.; Simons, R.F.; Losito, B.D.; Fiorito, E.; Miles, M.A.; Zelson, M. Stress recovery during exposure to natural and urban environments. J. Environ. Psychol. 1991, 11, 201–230. [Google Scholar] [CrossRef]
- Gilchrist, K.; Brown, C.; Montarzino, A. Workplace settings and wellbeing: Greenspace use and views contribute to employee wellbeing at pen-urban business sites. Landsc. Urban Plan. 2015, 138, 32–40. [Google Scholar] [CrossRef]
- Hallal, P.C.; Bauman, A.E.; Heath, G.W.; Kohl, H.W.; Lee, I.M.; Pratt, M. Physical activity: More of the same is not enough. Lancet 2012, 380, 190–191. [Google Scholar] [CrossRef]
- Nieminen, T.; Martelin, T.; Koskinen, S.; Aro, H.; Alanen, E.; Hyyppä, M. Social capital as a determinant of self-rated health and psychological well-being. Int. J. Public Health 2010, 55, 531–542. [Google Scholar] [CrossRef] [PubMed]
- Cornwell, E.Y.; Waite, L.J. Social disconnectedness, perceived isolation, and health among older adults. J. Health Soc. Behav. 2009, 50, 31–48. [Google Scholar] [CrossRef] [PubMed]
- Steptoe, A.; Shankar, A.; Demakakos, P.; Wardle, J. Social isolation, loneliness, and all-cause mortality in older men and women. Proc. Natl. Acad. Sci. USA 2013, 110, 5797–5801. [Google Scholar] [CrossRef] [PubMed]
- Mathis, A.; Rooks, R.; Kruger, D. Improving the neighborhood environment for urban older adults: Social Context and self-rated health. Int. J. Environ. Res. Public Health 2016, 13, 3. [Google Scholar] [CrossRef] [PubMed]
- Heinrichs, M.; Baumgartner, T.; Kirschbaum, C.; Ehlert, U. Social support and oxytocin interact to suppress cortisol and subjective responses to psychosocial stress. Biol. Psychiatry 2003, 54, 1389–1398. [Google Scholar] [CrossRef]
- Choenarom, C.; Williams, R.A.; Hagerty, B.M. The role of sense of belonging and social support on stress and depression in individuals with depression. Arch. Psychiatr. Nurs. 2005, 19, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Grobecker, P.A. A sense of belonging and perceived stress among baccalaureate nursing students in clinical placements. Nurse Educ. Today 2016, 36, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Bedimo-Rung, A.L.; Mowen, A.J.; Cohen, D.A. The significance of parks to physical activity and public health—A conceptual model. Am. J. Prev. Med. 2005, 28, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Lachowycz, K.; Jones, A.P. Does walking explain associations between access to greenspace and lower mortality? Soc. Sci. Med. 2014, 107, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Villeneuve, P.J.; Jerrett, M.; Su, G.J.; Burnett, R.T.; Chen, H.; Wheeler, A.J.; Goldberg, M.S. A cohort study relating urban green space with mortality in Ontario, Canada. Environ. Res. 2012, 115, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Pope, D.; Tisdall, R.; Middleton, J.; Verma, A.; van Ameijden, E.; Birt, C.; Bruce, N.G. Quality of and access to green space in relation to psychological distress: Results from a population-based cross-sectional study as part of the EURO-URHIS 2 project. Eur. J. Public Health 2015. [Google Scholar] [CrossRef] [PubMed]
- Maas, J.; van Dillen, S.M.E.; Verheij, R.A.; Groenewegen, P.P. Social contacts as a possible mechanism behind the relation between green space and health. Health Place 2009, 15, 586–595. [Google Scholar] [CrossRef] [PubMed]
- De Vries, S.; van Dillen, S.M.E.; Groenewegen, P.P.; Spreeuwenberg, P. Streetscape greenery and health: Stress, social cohesion and physical activity as mediators. Soc. Sci. Med. 2013, 94, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Hartig, T.; Mitchell, R.; de Vries, S.; Frumkin, H. Nature and health. Annu. Rev. Public Health 2014, 35, 207–228. [Google Scholar] [CrossRef] [PubMed]
- Madge, C. Public parks and the geography of fear. Tijdschr. Econ. Soc. Geogr. 1997, 88, 237–250. [Google Scholar] [CrossRef]
- Ward Thompson, C.; Aspinall, P.; Bell, S.; Findlay, C. “It gets you away from everyday life”: Local woodlands and community use—What makes a difference? Landsc. Res. 2005, 30, 109–146. [Google Scholar] [CrossRef]
- Sreetheran, M.; van den Bosch, C.C.K. A socio-ecological exploration of fear of crime in urban green spaces—A systematic review. Urban. For. Urban. Green. 2014, 13, 1–18. [Google Scholar] [CrossRef]
- Richardson, E.A.; Mitchell, R. Gender differences in. relationships between urban green space and health in the United Kingdom. Soc. Sci. Med. 2010, 71, 568–575. [Google Scholar] [CrossRef] [PubMed]
- Jiang, B.; Li, D.; Larsen, L.; Sullivan, W.C. A dose-response curve describing the relationship between urban tree cover density and self-reported stress recovery. Environ. Behav. 2014. [Google Scholar] [CrossRef]
- Carstairs, V.D.L.; Morris, R. Deprivation and Health in Scotland; Aberdeen University Press: Aberdeen, UK, 1991; p. 334. [Google Scholar]
- Miller, D.R.; Morrice, J.G. Contribution of Green and Open Space to Public Health and Wellbeing; James Hutton Institute: Aberdeen, UK, 2014. [Google Scholar]
- Mitchell, R.; Astell-Burt, T.; Richardson, E.A. A comparison of green space indicators for epidemiological research. J. Epidemiol. Commun. Health 2011, 65, 853–858. [Google Scholar] [CrossRef] [PubMed]
- CRESH. The Percentage Green Space Coverage Data for UK CAS Wards. Available online: https://cresh.org.uk/cresh-themes/green-spaces-and-health/ward-level-green-space-estimates/ (accessed on 19 April 2016).
- Scottish Neighbourhood Statistics. Scottish Index of Multiple Deprivation; The Scottish Government: Edinburgh, UK, 2009.
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Stewart-Brown, S.; Tennant, A.; Tennant, R.; Platt, S.; Parkinson, J.; Weich, S. Internal construct validity of the Warwick-Edinburgh Mental Well-being Scale (WEMWBS): A Rasch analysis using data from the Scottish Health Education Population Survey. Health Qual. Life Outcomes 2009, 7, 15. [Google Scholar] [CrossRef] [PubMed]
- Milton, K.; Bull, F.C.; Bauman, A. Reliability and validity testing of a single-item physical activity measure. Br. J. Sports Med. 2011, 45, 203–208. [Google Scholar] [CrossRef] [PubMed]
- The Scottish Government. Planning Advice Note 65: Planning and Open Space; The Scottish Government: Edinburgh, UK, 2008.
- Greenspace_Scotland. Urban Greenspace Mapping and Characterisation Handbook; Greenspace_Scotland: Stirling, UK, 2011. [Google Scholar]
- Ding, C.S. Using regression mixture analysis in educational research. Pract. Assess. Res. Eval. 2006, 11, 1. [Google Scholar]
- Magidson, J.; Vermunt, J.K. An extension of the CHAID tree-based segmentation algorithm to multiple dependent variables. In Classification: the Ubiquitous Challenge; Weihs, C., Gaul, W., Eds.; Springer: Heidelberg, Germany, 2005; pp. 176–183. [Google Scholar]
- Green, S.B.; Salkind, N.J. Using SPSS for Windows and Macintosh: Analyzing and Understanding Data, 5th ed.; Pearson/Prentice Hall: Upper Saddle River, NJ, USA, 2008; p. 459. [Google Scholar]
- Magidson, J. Correlated component regression: Re-thinking regression in the presence of near collinearity. In New Perspectives in Partial Least Squares and Related Methods; Abdi, H., Chin, W.W., Esposito Vinzi, V., Russolillo, G., Trinchera, L., Eds.; Springer New York: New York, NY, USA, 2013; pp. 65–78. [Google Scholar]
- Schmoll, C.; Khan, A.; Aspinall, P.; Goudie, C.; Koay, P.; Tendo, C.; Cameron, J.; Roe, J.; Deary, I.; Dhillon, B. New light for old eyes: Comparing melanopsin-mediated non-visual benefits of blue-light and UV-blocking intraocular lenses. Br. J. Ophthalmol. 2014, 98, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Aspinall, P.A.; Borooah, S.; Al Alouch, C.; Roe, J.; Laude, A.; Gupta, R.; Gupta, M.; Montarzino, A.; Dhillon, B. Gaze and pupil changes during navigation in age-related macular degeneration. Br. J. Ophthalmol. 2014, 98, 1393–1397. [Google Scholar] [CrossRef] [PubMed]
- Nathans, L.L.; Oswald, F.L.; Nimon, K. Interpreting multiple linear regression: A guidebook of variable importance. Pract. Assess. Res. Eval. 2012, 17, 1–19. [Google Scholar]
- Kenny, D.A. Mediation. Available online: http://davidakenny.net/cm/mediate.htm (accessed on 30 October 2015).
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef] [PubMed]
- Scottish Government. Scottish Index of Multiple Deprivation 2009: General Report; Scottish Government: Edinburgh, UK, 2009.
- Wood, C.J.; Pretty, J.; Griffin, M. A case-control study of the health and well-being benefits of allotment gardening. J. Public Health 2015. [Google Scholar] [CrossRef] [PubMed]
- Weller, R. The prodigal sun. New Sci. 2015, 226, 26–27. [Google Scholar] [CrossRef]
- Ulrich, R.S.; Zimring, C.; Zhu, X.M.; DuBose, J.; Seo, H.B.; Choi, Y.S.; Quan, X.B.; Joseph, A. A review of the research literature on evidence-based healthcare design. Herd-Health Env. Res. 2008, 1, 61–125. [Google Scholar] [CrossRef]
- Pearce, J. The ”blemish of place”: Stigma, geography and health inequalities. A commentary on Tabuchi, Fukuhara & Amp; Iso. Soc. Sci. Med. 2012, 75, 1921–1924. [Google Scholar] [PubMed]
- Gidlow, C.J.; Randall, J.; Gillman, J.; Smith, G.R.; Jones, M.V. Natural environments and chronic stress measured by hair cortisol. Landsc. Urban Plan. 2016, 148, 61–67. [Google Scholar] [CrossRef]
- Lengen, C.; Kistemann, T. Sense of place and place identity: Review of neuroscientific evidence. Health Place 2012, 18, 1162–1171. [Google Scholar] [CrossRef] [PubMed]
- Hillsdon, M.; Jones, A.; Coombes, E. Green Space Access, Green Space Use, Physical Activity and Overweight; Natural England Commissioned Reports; Natural England: Sheffield, UK, 2011.
- Lachowycz, K.; Jones, A.P.; Page, A.S.; Wheeler, B.W.; Cooper, A.R. What can global positioning systems tell us about the contribution of different types of urban greenspace to children’s physical activity? Health Place 2012, 18, 586–594. [Google Scholar] [CrossRef] [PubMed]
- Marengoni, A.; Angleman, S.; Melis, R.; Mangialasche, F.; Karp, A.; Garmen, A.; Meinow, B.; Fratiglioni, L. Aging with multimorbidity: A systematic review of the literature. Ageing Res. Rev. 2011, 10, 430–439. [Google Scholar] [CrossRef] [PubMed]
- De Vries, S.; Verheij, R.A.; Groenewegen, P.P.; Spreeuwenberg, P. Natural environments—Healthy environments? An exploratory analysis of the relationship between greenspace and health. Environ. Plan. A 2003, 35, 1717–1731. [Google Scholar] [CrossRef]
- Broekhuizen, K.; de Vries, S.; Pierik, F. Healthy Aging in a Green Living Environment: A Systematic Review of the Literature; TNO Leiden: Leiden, The Netherlands, 2013. [Google Scholar]
- Grazuleviciene, R.; Danileviciute, A.; Dedele, A.; Vencloviene, J.; Andrusaityte, S.; Uzdanaviciute, I.; Nieuwenhuijsen, M.J. Surrounding greenness, proximity to city parks and pregnancy outcomes in Kaunas Cohort Study. Int. J. Hyg. Environ. Health 2015, 218, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Dzhambov, A.M.; Dimitrova, D.D.; Dimitrakova, E.D. Association between residential greenness and birth weight: Systematic review and meta-analysis. Urban For. Urban Green. 2014, 13, 621–629. [Google Scholar] [CrossRef]
- Dadvand, P.; Villanueva, C.M.; Font-Ribera, L.; Martinez, D.; Basagana, X.; Belmonte, J.; Vrijheid, M.; Grazuleviciene, R.; Kogevinas, M.; Nieuwenhuijsen, M.J. Risks and benefits of green spaces for children: A cross-sectional study of associations with sedentary behavior, obesity, asthma, and allergy. Environ. Health Perspect. 2014, 122, 1329–1335. [Google Scholar] [CrossRef] [PubMed]
- Dadvand, P.; Nieuwenhuijsen, M.J.; Esnaola, M.; Forns, J.; Basagana, X.; Alvarez-Pedrerol, M.; Rivas, I.; Lopez-Vicente, M.; De Castro Pascual, M.; Su, J.; et al. Green spaces and cognitive development in primary schoolchildren. Proc. Natl. Acad. Sci. USA 2015, 112, 7937–7942. [Google Scholar] [CrossRef] [PubMed]
- Miles, R.; Coutts, C.; Mohamadi, A. Neighborhood urban form, social environment, and depression. J. Urban Health Bull. N. Y. Acad. Med. 2012, 89, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Executive, S. Scottish Neighbourhood Statistics Guide; Scottish Executive Publications: Edinburgh, UK, 2005. [Google Scholar]
- Openshaw, S. The Modifiable Areal Unit Problem; Geobooks: Norwich, UK, 1984. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total Sample (N = 406) | Community 1 (N = 101) | Community 2 (N = 100) | Community 3 (N = 99) | Community 4 (N = 106) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| % | Mean (SD) | % | Mean (SD) | % | Mean (SD) | % | Mean (SD) | % | Mean (SD) | |
| Age: | 44 (17.1) | 44 (17.0) | 42 (16.3) | 45 (18.6) | 45 (16.5) | |||||
| 16–34 | 34.6 | 33.7 | 37.0 | 33.7 | 34.0 | |||||
| 35–54 | 36.3 | 34.7 | 41.0 | 32.7 | 36.8 | |||||
| 55–64 | 11.6 | 13.9 | 8.0 | 14.3 | 10.4 | |||||
| 65+ | 17.5 | 17.8 | 14.0 | 19.4 | 18.9 | |||||
| Sex (% male) | 45.3 | 47.5 | 44.0 | 42.4 | 47.2 | |||||
| Education level (%tertiary+) | 14.5 | 4.0 | 10.0 | 28.3 | 16.2 | |||||
| Carstairs Index | 6.5 (2.4) | 6.9 (1.0) | 8.07 (2.5) | 3.7 (0.0) | 5.6 (2.6) | |||||
| Relationship Status: | ||||||||||
| Single | 36.1 | 25.0 | 41.0 | 44.4 | 34.3 | |||||
| Married | 26.2 | 27.0 | 21.0 | 30.3 | 26.7 | |||||
| Partnered/cohabiting | 17.5 | 22.0 | 20.0 | 7.1 | 21.0 | |||||
| Divorced/separated/widowed | 20.2 | 26.0 | 18.0 | 18.2 | 18.1 | |||||
| Employment status: (% working full-time) | 24.6 | 16.8 | 20.0 | 21.2 | 39.6 | |||||
| Children in the household (%yes) | 39.5 | 46.9 | 38.9 | 44.6 | 28.3 | |||||
| Private car access (% yes) | 39.1 | 23.9 | 27.3 | 55.7 | 48.5 | |||||
| Health/Wellbeing | ||||||||||
| Stress (PSS score) | 15.4 (6.0) | 20.0 (1.9) | 14.3 (6.4) | 13.2 (6.8) | 14.0 (5.2) | |||||
| General health (score) | 3.9 (1.0) | 3.49 (0.7) | 4.01 (1.1) | 3.85 (1.0) | 4.25 (0.8) | |||||
| Physical activity (days/month) | 10.3 (10.1) | 3.0 (5.8) | 12.7 (10.3) | 10.0 (9.8) | 15.5 (9.4) | |||||
| Social wellbeing | ||||||||||
| Place belonging (score) | 3.9 (0.9) | 3.5 (0.8) | 4.1 (1.0) | 4.1 (0.9) | 4.0 (0.5) | |||||
| Social isolation (score) | 2.5 (0.6) | 2.3 (0.6) | 2.7 (0.6) | 2.5 (0.8) | 2.6 (0.5) | |||||
| Neighbourhood trust (score) | 2.9 (1.0) | 3.0 (0.7) | 2.8 (1.2) | 3.0 (1.1) | 2.8 (0.8) | |||||
| Green space measures | ||||||||||
| % green space area (objective measure) | 56.8 (12.3) | 61.0 (7.8) | 53.5 (6.7) | 65.8 (6.7) | 49.5 (15.2) | |||||
| % participants who have a garden or allotment | 49.1 | 72.3 | 30.0 | 64.6 | 30.5 | |||||
| % participants with view (green space or hill) | 30.6 | 47.5 | 10.0 | 42.4 | 22.9 | |||||
| % participants visiting green space (at least once a week or more) in winter | 57.9 | 53.0 | 66.3 | 68.0 | 44.4 | |||||
| Predictors | Community 1 (Mean PSS Score 20) | Communities 2, 3 and 4 (Mean PSS Score 13.8) | Direction of Relationship between Variables Lower Stress Is Associated with: |
|---|---|---|---|
| Individual characteristics | - | Employment (1) a,(6) b | Bring in full-time employment |
| - | Car access (4) a,(5) b | Having access to a car a | |
| - | Age (3) b | Older age | |
| - | Children < 16 in household (4) b | No children in the household | |
| - | Sex (9) b | Being male | |
| Area-level deprivation | - | Carstairs Index score (7) b | Higher area-level deprivation |
| Social wellbeing | - | Social isolation (3) a | Not often lacking companionship |
| - | Place belonging (2) a | Greater belonging to the neighbourhood/local area | |
| Green space measures | - | Objective measure of % green space area (1) b | Greater% green space area |
| Garden or allotment (1) | Garden or allotment (2) b | Having a garden or allotment |
| Predictors | Community 1 (Mean Health Score 3.49) | Community 3 (Mean Health Score 3.85) | Communities 2 and 4 (Mean Health Score 4.13) | Direction of Relationship between Variables Better Health is Associated with: |
|---|---|---|---|---|
| Individual characteristics | Education level (3) | Higher education level | ||
| Age (5) | Age (2) | Younger age | ||
| Children <16 in household (6) | Children in the household | |||
| Relationship status (8) | Relationship status (3) | Being single | ||
| Employment (10) | Being in full-time employment | |||
| Area-level deprivation | Carstairs Index score (7) | Lower area-level deprivation | ||
| Physical activity levels (days/month) | Physical activity level (1) | Physical activity level (1) | More days of 30 min or more moderate to vigorous physical activity per month | |
| Social wellbeing | Social isolation (2) | Not often lacking companionship | ||
| Place belonging (4) | Greater belonging to the neighbourhood/local area | |||
| Green space measures | View of green space or hills (9) | View of green space or hills from the home | ||
| Winter green space visits (1) | Visiting green space in winter more often (at least once/month) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ward Thompson, C.; Aspinall, P.; Roe, J.; Robertson, L.; Miller, D. Mitigating Stress and Supporting Health in Deprived Urban Communities: The Importance of Green Space and the Social Environment. Int. J. Environ. Res. Public Health 2016, 13, 440. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13040440
Ward Thompson C, Aspinall P, Roe J, Robertson L, Miller D. Mitigating Stress and Supporting Health in Deprived Urban Communities: The Importance of Green Space and the Social Environment. International Journal of Environmental Research and Public Health. 2016; 13(4):440. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13040440
Chicago/Turabian StyleWard Thompson, Catharine, Peter Aspinall, Jenny Roe, Lynette Robertson, and David Miller. 2016. "Mitigating Stress and Supporting Health in Deprived Urban Communities: The Importance of Green Space and the Social Environment" International Journal of Environmental Research and Public Health 13, no. 4: 440. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13040440