2. Subjects and Methods
2.1. Subjects
The subjects of the study were recruited from August to December of 2013. A cluster random sampling method was used in this survey. Seven representative communities were randomly selected from the suburban area of Beijing. The exclusion criteria were: an age below 18 years, a lack of mobility, communication disorders, pregnancy, severe cardiac, hepatic or kidney disease, or no experience with thyroid ultrasound. People who were or had been treated with medicines influencing thyroid function, such as amiodarone, iodine, lithium preparation, interferon, or hormones such as glucocorticoid and estrogen were also excluded. A total of 8233 individuals were initially included; however, 85% participated. Another 674 people were excluded according to the criteria. Finally, 6324 participants were included in the cross-sectional survey analysis. All subjects gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki. The study was approved by the ethics committee of the Chinese People’s Liberation Army (PLA) General Hospital (Project code 2011ZX09307-001-08).
2.2. Measurements
Initially, potential participants signed informed consent forms, and then assented to a questionnaire survey, a physical examination, and thyroid ultrasound. A thyroid nodule is a discrete lesion within the thyroid gland that is radiologically distinct from the surrounding thyroid parenchyma [
9]. Thyroid ultrasound was performed using LOGIQ e (GE Healthcare, Milwaukee, WI, USA) B ultrasonic wave, a high-frequency linear array 12L, and a 7–13-MHz probe.
Smoking habits, drinking, taste preferences, seafood intake, educational level, physical labor intensity, physical exercise intensity, and medical history were recorded in the questionnaire. As far as smoking was concerned, individuals were divided into current smokers (those who had been smoking at least one cigarette per day for over six months), former smokers, and non-smokers. For alcohol-drinking status, subjects were classified as current drinkers (those who had been taking alcohol at least once a week for over six months), former drinkers, and non-drinkers. Concerning the educational level, subjects were classified into six groups: those who had never gone to school, those who had gone to elementary school, those who had gone to middle school, those who had gone to high school/technical school/polytechnic school, those who had gone to junior college, and those who had gone to college and beyond. Taste preferences were divided into three groups of salt preference: salty, average, and less salty. Frequency of seafood intake was assessed in three groups: frequent (≥3 times/week), occasional (<3 times/week), and never. According to national physical labor intensity classification GB3869-1997, physical labor was assessed and placed into four groups of very light, light, moderate, and heavy physical labor. Based on the classification of American College of Sports Medicine, physical exercise intensity was grouped into mild (exercise heart rate <55% of maximum heart rate), moderate (exercise heart rate within 55%–69% of maximum heart rate), and high (exercise heart rate ≥70% of maximum heart rate).
2.3. Statistical Analysis
Data were recorded on the computer twice by two independent individuals who were responsible for logic and consistency checks. Statistical analyses were performed using SPSS version 16.0 (SPSS Inc., Chicago, IL, USA). Age-standardized prevalence was calculated by the direct method using data of the population distribution in China in 2010. Measurements were expressed as mean ± standard deviation (SD), and two groups were compared using t-test. Counts were represented by frequency or percentage, and the groups were compared using a chi-square test and a Cochran–Armitage trend test. Related factors were analyzed using logistic regression. Missing data were missing at random and were not included in the analysis. A p < 0.05 was considered statistically significant.
4. Discussion
In recent years, the prevalence of TNs significantly increased. This survey was conducted on individuals over 18 years of age from seven communities in Beijing. It showed that the overall prevalence of TNs in the population was 49.0%. According to the literature, the prevalence was 67% in North America [
10], 27% in Finland, 19% in Belgium, and 17% in Brazil [
11]. The differences may be due to age, gender, inheritance, living environment, eating habits, and iodine nutritional status, among others [
12,
13,
14].
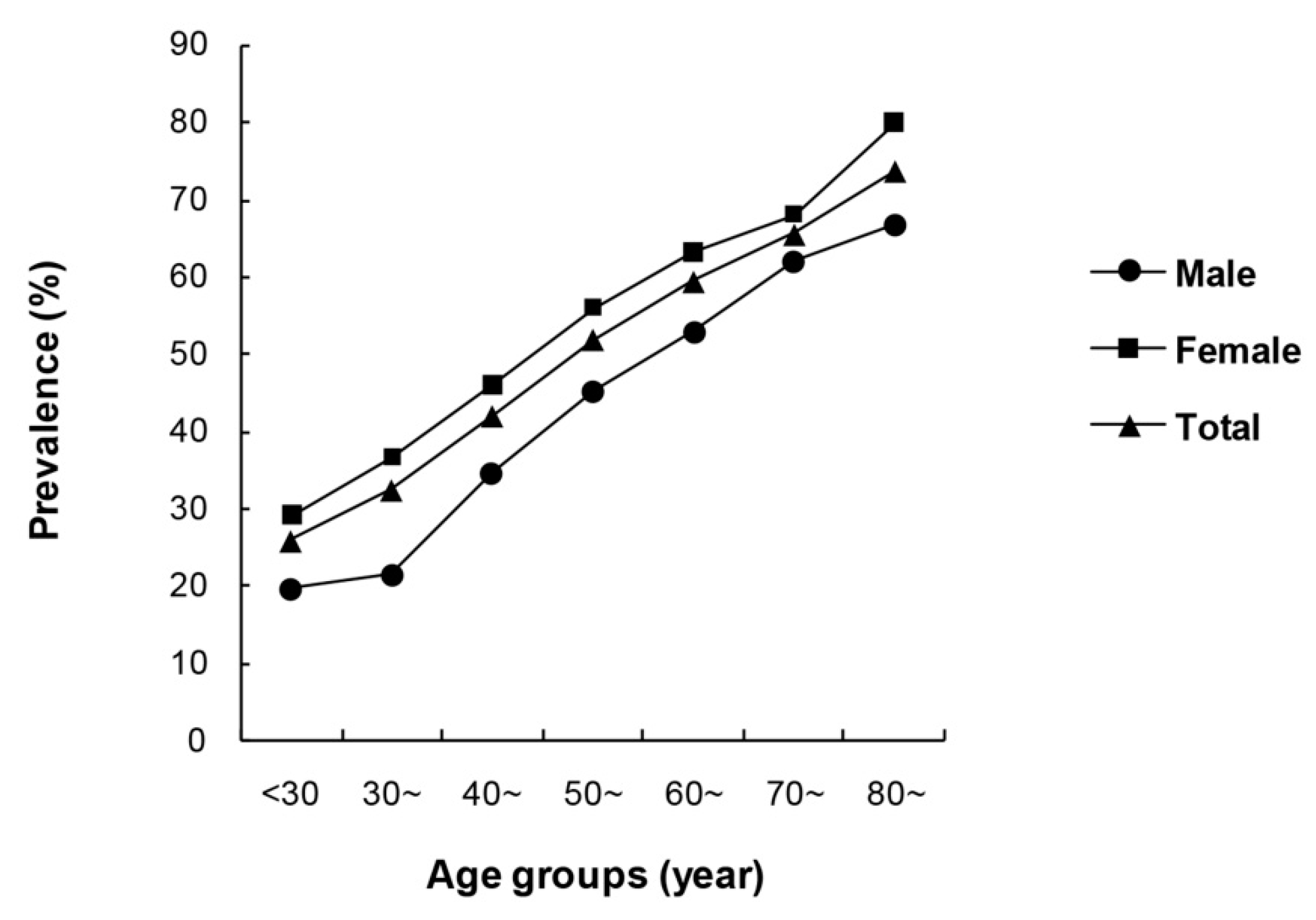
This survey showed that the prevalence of TNs increased significantly with age, which is consistent with previous studies [
15,
16,
17]. The prevalence among Japanese women over 40 years of age was 35.3%, and increased with age [
18]. In another iodine-deficient area, solitary nodule prevalence remained stable independent of age, while the prevalence of multiple nodules increased with age [
19,
20]. The prevalence of TNs increased with age, which is likely to be due to degenerative changes occurring in the thyroid.
The prevalence of TNs was 52.5% in females, which was significantly higher, compared to the 42.7% for males. Logistic regression proved that the female sex was an independent risk factor for the development of TNs. Previous reports have also revealed that women were more likely to suffer from TNs than men [
21,
22]. Clinical studies have shown that the prevalence in pregnant and fertile women was much higher [
23,
24], suggesting that gender differences might be due to the combined effect of estrogen and progesterone. Since estrogen has an effect on the thyroid gland and stimulates thyrotropin (TSH) generation [
25,
26], and both normal and neoplastic thyroid tissues have estrogen receptor expression [
27], it can be deduced that estrogen plays a possible role in the growth of thyroid cells and nodule formation. It was demonstrated in
in vitro studies that 17β-estradiol may stimulate the growth of normal thyroid cells [
28] and that thyroid follicular cells contained functional estrogen receptors [
29]. Moreover, a previous study illustrated that estrogen could stimulate the growth of benign and malignant thyroid cells by activating the mitogen-activated protein kinase pathway [
30]. However, Ceresini
et al. [
31] reported that the administration of estrogen for one year did not affect thyroid volume or the number and volume of thyroid nodules in postmenopausal women. Kim
et al. [
32] also reported that uterine fibroids were independently associated with the occurrence of TNs, although the study was more focused on premenopausal women. However, systemic estradiol levels had an inverse correlation with the incidence of TNs. This study hypothesized that, similar to uterine fibroids [
33], the thyroid might have intracrine or paracrine estrogen responsiveness and
in-situ estrogen synthesis [
34,
35]. The internal mechanisms of gender difference associated with TNs need to be further investigated.
In our study, a current smoking habit was demonstrated to be an independent lifestyle risk factor for thyroid nodules by logistic regression (OR = 1.246 (1.046–1.483)). Some previous studies have reported higher goiter prevalence and higher thyroid volumes among smokers compared to non-smokers [
36,
37]. Meanwhile, differing results were also published [
38]. A discrepancy might be explained by differences in iodine status, as the association seems to be stronger in iodine-deficient areas [
39]. Less research has focused on the association between TNs and smoking habits. We found a positive association of smoking with TNs in seven communities in Beijing, which is consistent with previous findings [
40,
41]. Several pathological mechanisms for the effect of smoking on thyroid morphology and function have been suggested. Thiocyanate, a degradation product of cyanide in tobacco smoke, is the major mediator of the goitrogenic effect of tobacco smoke. Thiocyanate acting as a competitive inhibitor inhibits iodine uptake and organification. It probably increases the prevalence of TNs and goiter by mimicking iodine deficiency. Smoking also stimulates thyroid hormone turnover, increases iodine demands and relative iodine deficiency, inhibits peripheral deiodinase activity, and has a direct effect on the pituitary. However, a Denmark study [
42] reported that smoking was associated with an increased prevalence of thyroid multinodularity (OR = 1.9 (1.4–2.5)), but not with an increased prevalence of solitary thyroid nodules. The association with multinodularity was also not statistically significant following salt iodization [
43]. Karatoprak
et al. [
44] observed that smoking had no effect on TN formation in iodine-sufficient regions like Istanbul. Furthermore, well-designed studies taking the amount and duration of smoking into account should be conducted to fully elucidate this relationship. Interestingly, we found no difference in the occurrence of TNs between drinkers and non-drinkers. A cross-sectional population study [
45] found that a lower prevalence of a solitary nodule was associated with increased levels of alcohol consumption. Confirmatory studies are required.
The logistic regression analysis showed that BMI was another independent risk factor for TNs. A study from Korea [
4] also reported that a higher BMI was associated with a higher frequency of TNs in women. Another study [
5] showed that a greater prevalence of nodules in obese male subjects. The precise mechanisms were not entirely clear. The main hypothesis is that the association between obesity and TNs is by means of insulin resistance (IR). In a previous report by Rezzonico
et al. [
46], patients with IR have a higher risk of formation of TNs. Higher circulating levels of insulin might cause increased thyroid proliferation. Another hypothesis is some humoral or hormonal mediators like leptin from adipose tissue stimulate the hypothalamus-pituitary-thyroid axis [
6]. Further studies are necessary to illuminate the association between obesity and TNs.
Our results showed that an increased frequency of seafood consumption was associated with a decreased prevalence of TNs. However, the logistic regression analysis did not show an independent association between the frequency of seafood intake and prevalence of TNs. A similar trend was evident in a study conducted in Belgium [
47], which reported that TN prevalence in Wallonia was higher than that in Flanders, while the consumption of seafood was significantly lower in Wallonia than in Flanders. The author believed that the longer distance of Wallonia to the sea than Flanders resulted in the lower iodine content of the local food. The difference in iodine content was the most plausible explanation for the difference in thyroid nodular prevalence. Our regression analysis proved that the frequency of seafood consumption was not an independent factor in the development of TNs. However, it may be affected by iodine intake, living habits, and other confounding factors. Further evaluation of the iodine nutritional status of the participants could help clarify the argument. Concerning the relationship between iodine nutritional status and TNs, Szabolcs
et al. [
48] showed that in three elderly Hungarian groups with deficient, adequate, and excessive iodine intake levels who underwent ultrasound TN detection, the prevalence rates were 20.2%, 16.2%, and 3.3%, respectively. Prevalence rates increased with a decreased iodine intake. On the contrary, Hu
et al. [
49] reported that the prevalence of TNs in deficient, adequate, and excessive iodine areas were 12.6%, 10.2%, and 10.8%, respectively, with no significant difference. Follow-up studies need to be conducted in order to fully reveal the relationship between iodine intake and the prevalence of TNs.
Univariate analysis showed that, with decreasing physical labor and physical exercise intensities, the prevalence of TNs increased. A significant negative correlation was observed in both instances as shown by the trend test. Leng
et al. [
50] reported that the prevalence of TNs in men who did not exercise or exercised rarely was significantly higher. In women, no such correlation was observed. We showed by multi-factor correction that labor and exercise were not independent factors in the development of TNs. However, these results indicate that other metabolic factors associated with labor and exercise may be relevant to the development of TNs.
Furthermore, we showed that the prevalence of TNs decreased with as education level increased; however, regression analysis showed this was not an independent factor. This may in part be attributed to the younger population often having higher education levels, the difference in smoking habits, and the methods of using iodinated salt. Knudsen
et al. [
51] also reported that the higher the education level, the smaller the thyroid volume, and the lower the prevalence of multiple nodules. On the other hand, the associations diminished markedly if an adjustment was made for smoking habits, alcohol consumption, and iodine intake.
Our study includes a large sample size for the prevalence of TNs in North China, and we have conducted a comprehensive analysis on the relationship between the prevalence of TNs and multiple lifestyle factors. The present study also has several limitations. First, there was no dose-response analysis between the amount and timing of both smoking and TN prevalence. Second, we did not assess the iodine nutritional status. A follow-up study that takes these factors into account is needed in the future.




{kind=link}