
Health-Related Quality of Life among Artisanal Fisherwomen/Shellfish Gatherers: Lower than the General Population

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample and Area
2.2. Measures
2.3. Statistical Analyses
2.4. Ethical Aspects
3. Results
4. Discussion
4.1. Strengths and Limitations
4.2. Recommendations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Pena, G.L.; Freitas, M.C.S.; Cardim, A. Non-industrial labor, infernal conditions and repetitive strain injury: A case study in a shellfish-rearing community on Maré Island, State of Bahia, Brazil. Cien. Saúde Colet. 2011, 16, 3383–3392. [Google Scholar] [CrossRef] [PubMed]
- Gill, T.; Feinstein, A. A critical appraisal of the quality of quality-of-life measurements. JAMA 1994, 272, 619–626. [Google Scholar] [CrossRef] [PubMed]
- Kluthcovsky, A.C.G.C.; Magosso, A.M. Quality of life—Conceptual issues. Salus 2007, 1, 13–15. [Google Scholar]
- Diniz, P.D. Qualidade de Vida: Saúde e Trabalho (Quality of Life: Health and Work), 2nd ed.; Manole: Barueri, Brazil, 2013. [Google Scholar]
- Minayo, M.C.S.; Hartz, Z.M.A.; Buss, P.M. Quality of life and health: A necessary. Cien. Saúde Colet. 2000, 5, 7–18. [Google Scholar] [CrossRef]
- World Health Organization. The World Health Organization Quality of Life Assessment (WHOQOL): Position Paper from the World Health Organization. Soc. Sci. Med. 1995, 41, 403–409. [Google Scholar]
- Rodriguez-Romero, B.; Pita-Fernandez, S.; Díazby, S.P.; Chouza-Insua, M. Health-related quality of life in women working in the fishing industry measured through the Short-Form 36 questionnaire. Gac. Sanit. 2013, 27, 418–424. [Google Scholar] [PubMed]
- Ciconelli, R.M. Brazilian Portuguese version of the SF-36: A reliable and valid quality of life outcome measure. Res. Bras. Reumatolog. 1999, 39, 143–150. [Google Scholar]
- Ministério da Pesca e Aquicultura (MPA). Pesca Artesanal, 2012. Available online: http://www.mpa.gov.br/#pesca/pesca-artesanal (accessed on 7 March 2016).
- Instituto Brasileiro de Geografia e Estatística (IBGE). Basic Data, 2010. Available online: http://www.ibge.gov.br/cidadesat/painel/painel.php?codmun=292975# (accessed on 7 March 2016).
- Ministério da Pesca e Aquicultura (MPA). Boletim Estatístico da Pesca e Aquicultura, 2010. Available online: http://www.mpa.gov.br/files/docs/Boletim_MPA_2010_pub.pdf (accessed on 7 March 2016).
- Instituto Brasileiro de Geografia e Estatística (IBGE). Estimativas de População Para 1° de Julho de 2011. Available online: http://www.ibge.gov.br/home/estatistica/populacao/estimativa2011/tab_Municipios_TCU.pdf (accessed on 7 March 2016).
- Bandeira, F.P.S.; Brito, R.R.C. Comunidades pesqueiras na Baía de Todos os Santos: Aspectos históricos e etnoecológicos (Fishermen Communities in Todos os Santos Bay: Historical and Ethnoecological Aspects). In Baía de Todos os Santos: Aspectos Humanos; Caroso, C., Tavares, F., Pereira, C., Eds.; EDUFBA: Salvador, Brazil, 2011; pp. 291–326. [Google Scholar]
- Pena, P.; Martins, V. Sofrimento Negligenciado: Doenças do Trabalho em Marisqueiras e Pescadores Artesanais (Neglected Suffering: Occupational Disease in Shellfish Gatherers and Artisanal Fishermen); EDUFBA: Salvador, Brazil, 2014. [Google Scholar]
- Rios, A.O.; Rego, R.F.; Pena, P.G.L. Diseases in fishery workers. Rev. Baiana Saúde Públ. 2011, 35, 175–188. [Google Scholar]
- Fernandes, R.C.P. Some features of the cross-sectional study in occupational epidemiology. RSCdaUEFS 2002, 1, 44–49. [Google Scholar]
- Falcão, I.R.; Couto, M.C.B.M.; Lima, V.M.C.; Pena, P.G.L.; Andrade, L.L.; Müller, J.S.; Alves, I.B.; Viana, W.S.; Rêgo, R.C.F. Prevalence of neck and upper limb musculoskeletal disorders in artisan fisherwomen/shellfish gatherers in Saubara, Bahia, Brazil. Cien. Saúde Colet. 2015, 20, 2469–2480. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, R.C.P.; Assunção, A.A.; Silvany Neto, A.M.; Carvalho, F.M. Musculoskeletal disorders among workers in plastic manufaturing plants. Rev. Bras. Epidemiol. 2010, 13, 11–20. [Google Scholar] [CrossRef]
- Couto, M.C.B.M. Prevalência e Fatores Associados à Lombalgia em Pescadoras Artesanais/Marisqueiras de Saubara—BA (Prevalence and Associated Factors of Back Pain in Artisanal Fishermen and Shellfish Gatherers). Available online: http://www.sat.ufba.br/site/db/dissertacoes/28112014112914.pdf (accessed on 7 March 2016).
- Kuorinka, I.; Forcier, L. Work Related Musculoskeletal Disorders (WMSDs): A Reference Book for Prevention; Taylor & Francis: London, UK, 1995. [Google Scholar]
- Bernard, B.P. Musculoskeletal Disorders and Workplace Factors: A Critical Review of Epidemiologic Evidence for Work Related Musculoskeltal Disorders of the Neck, Upper Extremity, and Low Back. Available online: http://www.cdc.gov/niosh/docs/97–141/#disclaimer (accessed on 7 March 2016).
- Cruz, L.N.; Fleck, M.P.; Oliveira, M.R.; Camey, S.A.; Hoffmann, J.F.; Bagattini, A.M.; Polanczyk, C.A. Health-related quality of life in Brazil: Normative data for the SF-36 in a general population sample in the south of the country. Cien. Saúde Colet. 2013, 18, 1911–1921. [Google Scholar] [CrossRef] [PubMed]
- SF-36: A Community for Measuring Health Outcomes Using SF Tools. Available online: http://www.sf-36.org (accessed on 7 March 2016).
- Laguardia, J.; Campos, M.R.; Travassos, C.; Najar, A.L.; Anjos, L.A.; Vasconcellos, M.M. Brazilian normative data for the Short Form 36 questionnaire, version 2. Rev. Bras. Epidemiol. 2014, 16, 889–897. [Google Scholar] [CrossRef]
- Buss, P.M. Health promotion and quality of life. Cien. Saúde Colet. 2000, 5, 163–177. [Google Scholar] [CrossRef]
- Oliveira, C.G.S. Avaliação das Condições de Saúde e Qualidade de Vida de Comunidade Pesqueira Sergipana (Assessment of Health Conditions and Quality of Life in the Fishermen Community of Sergipe). Available online: http://ppg.unit.br/psa/wp-content/uploads/sites/6/2013/07/Carla-de-Oliveira-AVALIA%C3%87%C3%83O-DAS-CONDI%C3%87%C3%95ES-DE-SA%C3%9ADE-E-QUALIDADE-DE-VIDA-DE-COMUNIDADE-PESQUEIRA-SERGIPANA.pdf (accessed on 7 March 2016).
- Roux, C.; Guillemin, F.; Boini, S.; Longuetaud, F.; Arnault, N.; Hercberg, S.; Briancon, S. Impact of musculoskeletal disorders on quality of life: An inception cohort study. Ann. Rheum. Dis. 2005, 64, 606–611. [Google Scholar] [CrossRef] [PubMed]
- Yeng, L.T.; Teixeira, M.J.; Romano, M.A.; Picarelli, H.; Settimi, M.M.; Greve, J.M.A. Musculoskeletal disorders Work Related. Rev. Med. 2001, 80, 422–442. [Google Scholar]

{kind=link}
| Domain | Questionnaire Items | Measures Evaluated | Measures |
|---|---|---|---|
| Physical Functioning | 3a, 3b, 3c, 3d, 3e, 3f, 3g, 3h, 3i, 3j | Assess the presence and extent of the restrictions imposed on physical capacity | Physical health |
| Physical Role Limitations | 4a, 4b, 4c, 4d | Assess physical aspects | |
| Bodily Pain | 7, 8 | Based on a question from the SF-20 questionnaire regarding pain intensity plus the interference of pain in daily activities | |
| General Health Perceptions | 1, 11a, 11b, 11c, 11d | Derived from the General Health Rating Index survey | |
| Vitality | 9a, 9e, 9g, 9l | Consider energy level and fatigue, derived from the Mental Health Inventory (MHI) questionnaire | Mental health |
| Social Functioning | 6, 10 | Assess the integration of the individual in social activities | |
| Emotional Role Limitations | 5a, 5b, 5c | Assess emotional wellbeing | |
| Mental health | 9e, 9d, 9f, 9h | Investigate the dimensions of anxiety, depression, changes in behavior or emotional imbalance and psychological wellbeing; Summary of 38 items from the Mental Health Assessment Questionnaire (MHI-38) |
| Sociodemographic Characteristics | n (209) | % |
|---|---|---|
| Age | ||
| 20–29 | 47 | 22 |
| 30–44 | 94 | 45 |
| 45–64 | 68 | 33 |
| Race | ||
| Black | 125 | 59.8 |
| Brown | 76 | 36.4 |
| White | 8 | 3.8 |
| Civil Status | ||
| Single | 56 | 26.8 |
| Married/Unmarried Couple/Living Together | 135 | 64.6 |
| Separated/Widow | 18 | 8.6 |
| Schooling | ||
| Up to 4 years | 48 | 23 |
| From 5 to 8 years | 94 | 45 |
| From 9 to 11 years | 67 | 32 |
| Health conditions | ||
| Overall musculoskeletal disorders | ||
| Yes | 198 | 94.7 |
| No | 11 | 5.3 |
| Diabetes | ||
| Yes | 14 | 6.7 |
| No | 195 | 93.3 |
| Hypertension | ||
| Yes | 57 | 27.3 |
| No | 152 | 72.7 |
| Arthritis | ||
| Yes | 22 | 10.5 |
| No | 187 | 89.5 |
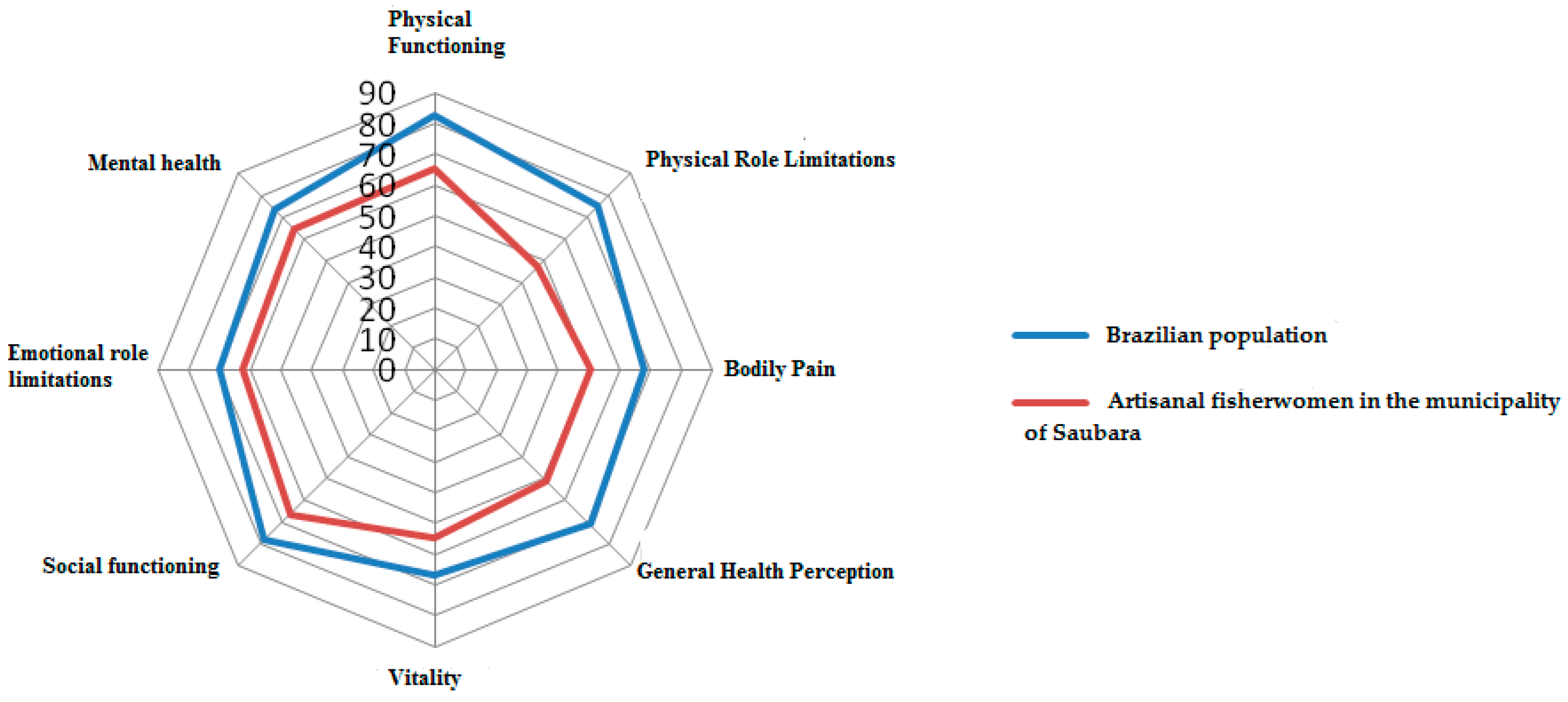
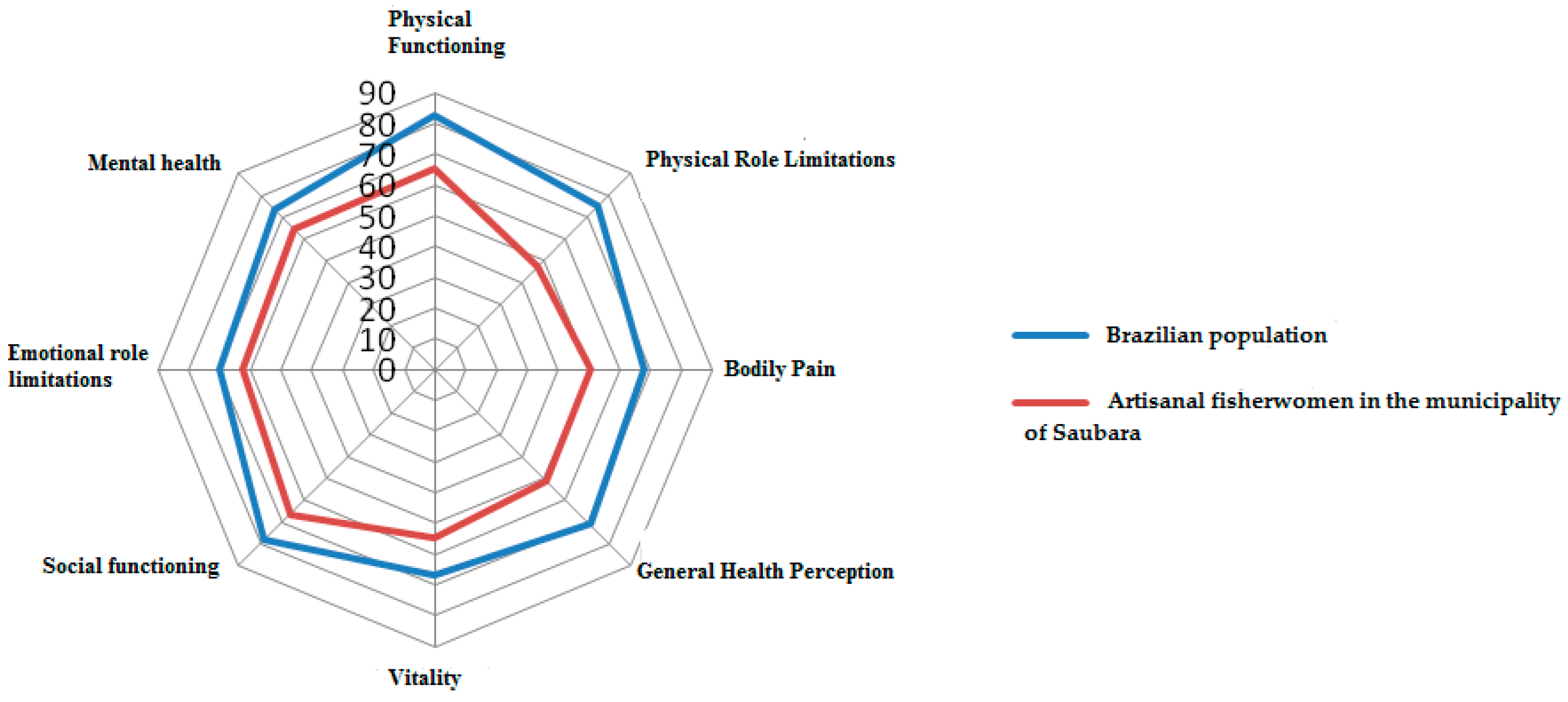
| Descriptive Statistics | PF 1 | PRL 2 | BP 3 | GHP 4 | Vitality 5 | SF 6 | ERL 7 | MH 8 |
|---|---|---|---|---|---|---|---|---|
| Mean | 65.7 | 47.3 | 50.44 | 51.2 | 54.5 | 66.4 | 62.4 | 64.8 |
| Standard Deviation | 24.9 | 40.8 | 25.3 | 21.8 | 22.9 | 30.5 | 42.9 | 23.5 |
| Median | 7.0 | 50.0 | 51.0 | 34.0 | 55.0 | 71.0 | 100.0 | 68.0 |
| Skewness a | −0.531 | 0.091 | 0.427 | −0.131 | −0.054 | −0.566 | −0.508 | −0.51 |
| Floor b | 0.96 | 33.0 | 2.4 | 1.4 | 0.5 | 4.8 | 26.3 | 0.96 |
| Ceiling c | 8.1 | 26.8 | 12.0 | 1.4 | 0.96 | 27.8 | 50.2 | 7.7 |
| Variables | Physical Functioning (PF) | Physical Role Limitations (PRL) | Bodily Pain (BP) | General Health Perception (GHP) | ||||||||
| Mean | SD | p-Value * | Mean | SD | p-Value * | Mean | SD | p-Value * | Mean | SD | p-Value * | |
| Age 1,7 | ||||||||||||
| 20 to 29 years a | 79.8 | 17.4 | 60.1 | 39.9 | 65.6 | 25.0 | 59.2 | 19.9 | ||||
| 30 to 44 years a | 70.1 | 21.6 | 0.000 | 51.6 | 40.8 | 0.000 | 47.2 | 23.0 | 0.000 | 52.3 | 21.6 | 0.001 |
| 45 or older b | 49.7 | 25.6 | 32.4 | 37.4 | 44.4 | 24.7 | 44.3 | 21.4 | ||||
| Schooling 1,7 | ||||||||||||
| Up to 4 years b | 51.04 | 26.8 | 33.9 | 37.4 | 42.9 | 24.3 | 47.3 | 21.4 | ||||
| 5 to 8 years a | 67.8 | 23.7 | 0.000 | 48.4 | 42.6 | 0.028 | 49.8 | 25.7 | 0.251 | 47.3 | 21.4 | 0.248 |
| 9 years or more a | 73.06 | 21.0 | 55.2 | 38.8 | 56.7 | 24.2 | 54.1 | 22.0 | ||||
| Overall MSDs 2 | ||||||||||||
| No | 84.6 | 15.7 | 0.006 | 81.8 | 31.8 | 0.004 | 79.9 | 26.1 | 0.000 | 63.0 | 16.9 | 0.067 |
| Yes | 64.6 | 25.0 | 45.3 | 40.5 | 48.8 | 24.3 | 50.6 | 21.9 | ||||
| Diabetes 3,6 | ||||||||||||
| No | 65.8 | 25.2 | 0.270 | 47.1 | 40.8 | 0.960 | 50.8 | 25.8 | 0.657 | 51.4 | 21.8 | 0.604 |
| Yes | 58.2 | 26.6 | 48.2 | 43.3 | 45.4 | 18.4 | 48.5 | 21.8 | ||||
| Hypertension 4,6 | ||||||||||||
| No | 68.1 | 24.6 | 0.000 | 51.9 | 40.4 | 0.006 | 53.5 | 25.7 | 0.005 | 54.8 | 21 | 0.000 |
| Yes | 55.6 | 25.8 | 34.7 | 39.7 | 42.3 | 22.5 | 41.7 | 21 | ||||
| Arthritis 5,6 | ||||||||||||
| No | 67.7 | 24.8 | 0.000 | 49.2 | 41.2 | 0.024 | 51.9 | 25.1 | 0.012 | 52.3 | 21.5 | 0.060 |
| Yes | 45.7 | 22.3 | 30.7 | 33.6 | 37.6 | 23.9 | 42.6 | 22.4 | ||||
| Variables | Vitality | Social Functioning (SF) | Emotional Role Limitations (ERL) | Mental Health (MH) | ||||||||
| Mean | SD | p-Value * | Mean | SD | p-Value * | Mean | SD | p-Value * | Mean | SD | p-Value * | |
| Age 1,7 | ||||||||||||
| 20 to 29 years a | 56.8 | 22.9 | 72.7 | 24.7 | 74.5 | 39.0 | 65.5 | 20.6 | ||||
| 30 to 44 years a | 55.6 | 21.8 | 0.470 | 68.2 | 30.0 | 0.126 | 64.5 | 42.0 | 0.012 | 67.4 | 23.5 | 0.193 |
| 45 or older b | 51.5 | 24.3 | 59.7 | 33.7 | 50.1 | 44.0 | 60.8 | 25.0 | ||||
| Schooling 1,7 | ||||||||||||
| Up to 4 years b | 47.3 | 21.4 | 59.3 | 34.4 | 63.2 | 42.0 | 59.5 | 25.0 | ||||
| 5 to 8 years a | 51.1 | 21.7 | 0.138 | 69.8 | 30.6 | 0.188 | 55.7 | 44.0 | 0.072 | 66.7 | 24.0 | 0.223 |
| 9 years or more a | 54.2 | 22.0 | 66.9 | 26.7 | 71.1 | 41.0 | 66.2 | 21.0 | ||||
| Overall MSDs 2 | ||||||||||||
| No | 64.6 | 19.3 | 0.133 | 87.0 | 19.6 | 0.016 | 81.8 | 41.0 | 0.081 | 81.8 | 40.5 | 0.081 |
| Yes | 53.9 | 22.9 | 65.3 | 30.6 | 61.3 | 43.0 | 64.2 | 23.8 | ||||
| Diabetes 3,6 | ||||||||||||
| No | 54.5 | 22.9 | 0.916 | 66.5 | 30.5 | 0.957 | 62.9 | 43.0 | 0.490 | 64.6 | 23.5 | 0.685 |
| Yes | 54.3 | 22.3 | 66.4 | 31.9 | 54.8 | 46.0 | 66.9 | 23.6 | ||||
| Hypertension 4,6 | ||||||||||||
| No | 55.9 | 22.8 | 0.152 | 68.6 | 28.7 | 0.180 | 65.8 | 42.0 | 0.061 | 66.9 | 23.0 | 0.025 |
| Yes | 50.8 | 22.8 | 60.7 | 34.5 | 53.2 | 44.0 | 59.0 | 23.7 | ||||
| Arthritis 5,6 | ||||||||||||
| No | 55.7 | 22.6 | 0.030 | 68.9 | 29.3 | 0.001 | 65.4 | 42.0 | 0.003 | 65.0 | 23.5 | 0.635 |
| Yes | 44.6 | 23.2 | 44.9 | 32.2 | 36.3 | 41.0 | 62.9 | 23.7 | ||||
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Müller, J.D.S.; Falcão, I.R.; Couto, M.C.B.M.; Viana, W.D.S.; Alves, I.B.; Viola, D.N.; Woods, C.G.; Rêgo, R.F. Health-Related Quality of Life among Artisanal Fisherwomen/Shellfish Gatherers: Lower than the General Population. Int. J. Environ. Res. Public Health 2016, 13, 466. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13050466
Müller JDS, Falcão IR, Couto MCBM, Viana WDS, Alves IB, Viola DN, Woods CG, Rêgo RF. Health-Related Quality of Life among Artisanal Fisherwomen/Shellfish Gatherers: Lower than the General Population. International Journal of Environmental Research and Public Health. 2016; 13(5):466. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13050466
Chicago/Turabian StyleMüller, Juliana Dos Santos, Ila Rocha Falcão, Maria Carolina Barreto Moreira Couto, Wendel Da Silva Viana, Ivone Batista Alves, Denise Nunes Viola, Courtney Georgette Woods, and Rita Franco Rêgo. 2016. "Health-Related Quality of Life among Artisanal Fisherwomen/Shellfish Gatherers: Lower than the General Population" International Journal of Environmental Research and Public Health 13, no. 5: 466. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13050466