
Contributing Factors to Colorectal Cancer Screening among Chinese People: A Review of Quantitative Studies


Abstract
:1. Introduction
2. Methods
3. Results
3.1. Study Characteristics
3.2. Factors Associated with CRC Screening
3.2.1. Socio-Demographic Factors
3.2.2. Psychological Factors
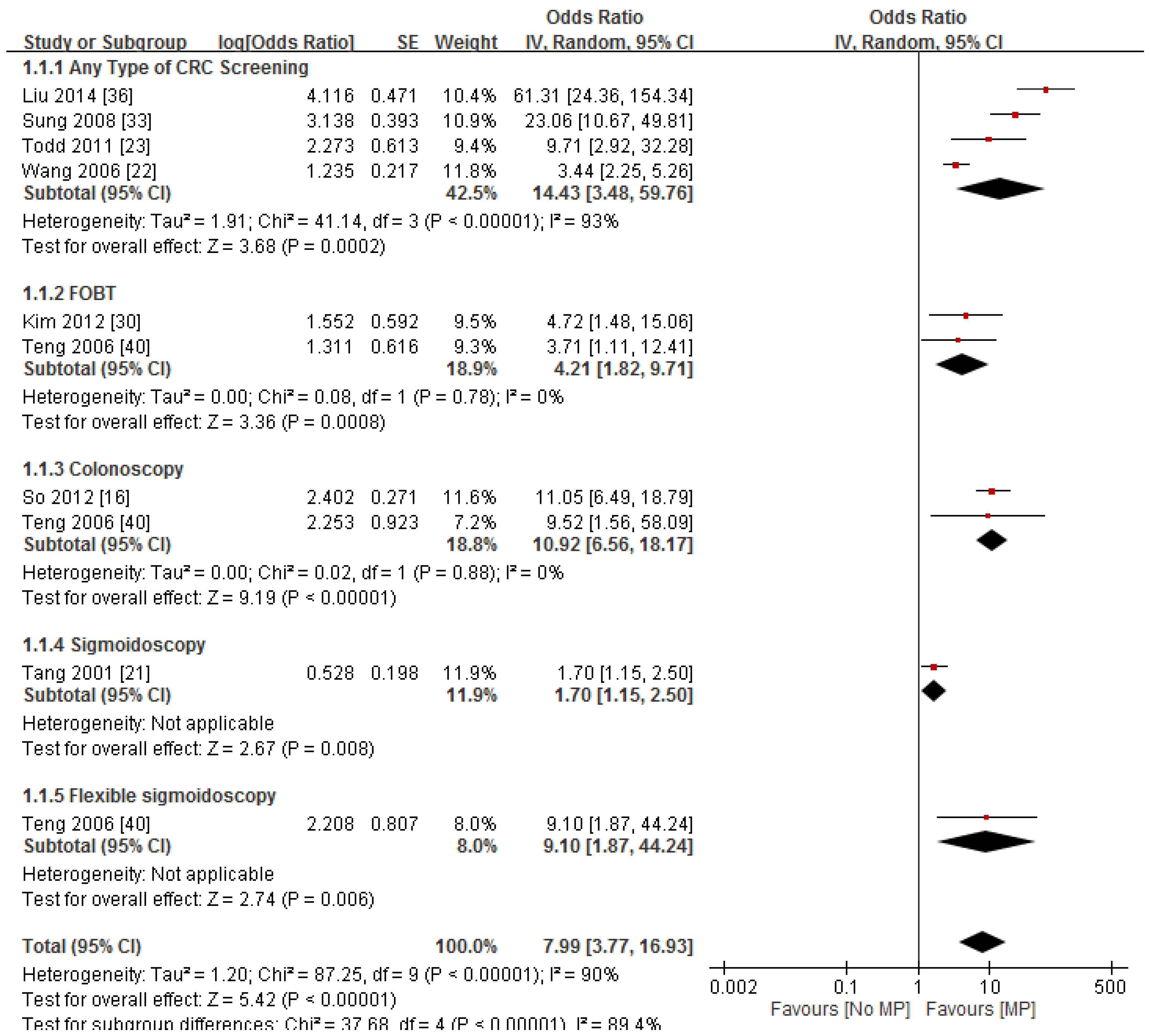
3.2.3. Contact with Medical Provider
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| Adj OR | Adjusted odds ratio |
| CRC | Colorectal cancer |
| FOBT | Fecal occult blood testing |
| FIT | Fecal immunochemical test |
| CS | Colonoscopy |
| FS | Flexible sigmoidoscopy |
| DRE | Digital rectal examination |
Appendix

{kind=link}
| First Author | Year | Country | Study Design | Sample Size | Method of Ascertainment | Selection Criteria of Participants | Effect Size | Variables Adjusted for in the Analysis | Quality Score |
|---|---|---|---|---|---|---|---|---|---|
| Todd et al. [27] | 2011 | Canada | Cross-sectional | 103 | Self-reported CRC screening: 75% | Women aged ≥50 years | No physician recommendation: Adj OR = 0.103 (95%CI = 0.031, 0.349); Cantonese as 19 language: Adj OR = 1.85 (95%CI = 0.055, 0.628); Self-efficacy: Adj OR = 3.613 (95%CI = 1.179, 11.070). | Years in Canada; Health literacy. | 5 |
| Cai et al. [29] * | 2009 | China | Case-control study | 463 | Data from registry of FOBT and CS | Adults aged 40–74 years | Knowledge | Age; Gender; Occupation; Gender by Occupation; Annual personal income. | 4 |
| Chen et al. [30] * | 2010 | China | Case-control study | 453 | Data from registry of compliance (FOBT and CS) | Adults aged 40–74 years | Understanding the purpose and method of the screening Value CRC screening Knowledge about CRC screening Screening can improve health | No multivariate analysis was done | 3 |
| Deng et al. [36] | 2011 | China | Cross-sectional | 1001 | Self-reported CRC screening in the past: 22.5% | Adults aged over 18 years excluding health care professionals | Age ≥ 40: Adj OR = 3.834 (95%CI = 2.657, 5.532) Health insurance : Adj OR = 1.996 (95%CI = 1.426, 2.794) Monthly household income ≥4000 RMB: Adj OR = 0.633 (95%CI = 0.467, 0.858) High knowledge level (low as reference): Adj OR = 5.299 (95%CI = 3.415, 8.223) | Gender; Educational level. | 5 |
| Hong [42] | 2012 | China | Cross-sectional | 1944 | Self-reported CS in the past: 24.5% | High CRC risk adults aged ≥ 40 years | Age ≥ 60: Adj OR = 0.682 (95%CI = 0.513, 0.916) Health insurance: Adj OR = 1.835 (95%CI = 1.207, 2.931) High knowledge (low as reference): Adj OR = 5.985 (95%CI = 3.471, 9.142) | Gender; Educational level; Monthly household income. | 5 |
| Liu [41] | 2014 | China | Cross-sectional | 600 | Self-reported CRC screening in the past: 22% | Adults aged 40–75 years | Logistical regression with psychological factors: Often have health checkup (never as reference): Adj OR = 2.938 (95%CI = 1.074, 8.038); Have regular health checkup (never as reference): Adj OR = 6.747 (95%CI = 2.484, 18.330) Exercise until reach the desirable pulse rate in sometime (never as reference): Adj OR = 3.447 (95%CI = 1.503, 7.907). Logistical regression with environmental factors: Discuss problems and worry with friends/family regularly (never as reference): Adj OR = 15.281 (95%CI = 1.788, 130.613); Received recommendation for CRC screening: Adj OR = 61.328 (95%CI = 24.341, 154.521). | For psychological factors: Report symptoms; Seeking health information via newspapers or TV; Ask if having difficulties in understanding health advice; Proactively seeking health advice; Attend health talk; Set exercise plan; Join physical exercise programs; Have physical exercise at least 3 times per week; Have training actively in daily life; Measure pulse during exercise; pay attention to nutrition information; release pressure; A balance between work and entertainment. For environmental factors: Spend time with close friends; satisfy the needs of close friends; Number of close friends who could provide help; Relationship with colleagues; Support from siblings; Support from other family members. | 6 |
| Leung et al. [24] | 2012 | Hong Kong | Cross-sectional | 1533 | Self-reported of FOBT/endoscopy in the past 2 years: 10.8% | Women aged ≥ 60 years Long-term care service applicants | Cognitive impairment: Adj OR = 0.81 (95%CI = 0.66, 0.99) | Number of chronic diseases | 6 |
| Leung et al. [40] * | 2014 | Hong Kong | Scale validation | 219 | Self-reported CRC screening in the past: 24.4% | Adults ≥ 60 years | Severity-fear Severity-life impact Psychological barriers Knowledge barriers | No multivariate analysis was done. | 4 |
| So et al. [20] | 2012 | Hong Kong | Cross-sectional | 2004 | Self-reported ever CS: 19% Self-reported ever FOBT: 12% | Random sample 50–75 years | For CS: Male: Adj OR = 1.58 (95%CI = 1.19, 2.10) Family history of cancer: Adj OR = 1.43 (95%CI = 1.05, 1.95) Had serious disease/cancer: Adj OR = 2.62 (95%CI = 1.79, 3.83) Poor perceived health status: Adj OR = 1.38 (95%CI = 1.02, 1.86) Perceived visiting a doctor regularly is good for health: Adj OR = 2.42 (95%CI = 1.81, 3.24) Health care professional recommendation: Adj OR = 11.04 (95%CI = 6.49, 18.77) For FOBT: Had serious disease/cancer: Adj OR = 1.50 (95%CI = 1.04, 2.10) Ex-smoker (non-smoker as reference): Adj OR = 1.45 (95%CI = 1.05, 2.02) Perceived visiting a doctor regularly is good for health: Adj OR = 1.96 (95%CI = 2.49) Taking dietary supplement is good for health: Adj OR = 1.54 (95%CI = 1.18, 2.01) Use of complementary medicine: Adj OR = 1.54 (95%CI = 1.18, 2.01) | For CS: Age; Health status; Smoking status; Perceived maintaining a healthy diet is good for health; Perceived visiting a Chinese herbalist regularly is good for health; Perceived taking dietary supplements is good for health. For FOBT: Educational level; Family history of cancer; Health status; Perceived health status; Perceived doing exercise is good for health; Perceived maintaining a healthy diet is good for health; Perceived visiting a Chinese herbalist regularly is good for health. | 4 |
| Sung et al. [37] | 2008 | Hong Kong | Cross-sectional | 1004 | Self-reported CRC screening uptake in the past: 9.9% | Random sample of Adults aged 30–65 years | Middle knowledge of CRC symptoms level (low as reference): Adj OR = 3.33 (95%CI = 1.22, 9.11) High knowledge of CRC risk factors level (low as reference): Adj OR = 2.61 (95%CI = 1.18, 5.88) Middle perceived severity of CRC level (low as reference): Adj OR = 0.28 (95%CI = 0.13, 0.65) Middle health/psychological barriers level (low as reference): Adj OR = 0.42 (95%CI = 0.21, 0.85) High access barrier level (low as reference): Adj OR = 0.22 (95%CI = 0.06, 0.85) Health insurance: Adj OR = 2.06 (95%CI = 1.01, 4.19) Physician recommendation: Adj OR = 23.05 (95%CI = 10.66, 51.80) | All variables are significant in the multivariate analysis. | 5 |
| Wong et al. [28] | 2013 | Hong Kong | Cohort | 5700 | Compliance of annual FIT checked by returned specimens: Year 1: 95.1% Year 2: 79.9% Year 3: 66.2% Year 4: 68.4% | Previous self-referred screeners aged 50–70 years | Female: Adj OR = 1.27 (95%CI = 1.11, 1.45) Age 55–59 (50-54 as reference): Adj OR = 0.82 (95%CI = 0.70, 0.95) Age 65–70 (50-54 as reference): Adj OR = 1.54 (95%CI = 1.26, 1.89) Non-smoking: Adj OR = 1.84 (95%CI = 1.43, 2.37) Family history of bowl cancer 1st degree relative: Adj OR = 0.74 (95%CI = 0.61, 0.89) 2nd degree relative: Adj OR = 0.78 (95%CI = 0.65, 0.94) | Monthly household income; Educational level; Marital status; Occupation; Self-perceived health status; Self-perceived risk. | 6 |
| Ng et al. [38] | 2007 | Singapore | Cross-sectional | 557 | Self-reported FOBT in the past: 26.5% | Random sample of adults aged ≥ 50 years | Had other screening: Adj OR = 3.47 (95%CI = 1.75, 6.91) Influenced by family/friend: Adj OR = 2.14 (95%CI = 1.02, 4.49) Knowledge: Adj OR = 1.03 (95%CI = 1.01, 1.04) Severity: Adj OR = 0.97 (95%CI = 0.96, 0.99) | Age; Education; Perceived barriers; Perceived benefits. | 5 |
| Chou et al. [33] | 2007 | Taiwan | interventional | 1252 | FS screening at the site: 77.8% | Self-referred adults aged 21–87 years | For incompletion of FS screening: Female: Adj OR = 2.06 (95%CI = 1.56, 2.73) Age ≥ 60: Adj OR = 1.68 (95%CI = 1.26, 2.23) BMI < 25: Adj OR = 1.41 (95%CI = 1.05, 1.89) History of constipation: Adj OR = 2.43 (95%CI = 1.04, 5.69) Inadequate bowel preparation: Adj OR = 1.66 (95%CI = 1.21, 2.16) | All variables are significant in the multivariate analysis. | 6 |
| Kim et al. [34] | 2012 | USA | Interventional | 113 | FOBT test after educational session | Adults aged ≥ 50 years | Having primary-care physician: Adj OR = 4.72 (95%CI = 1.48, 15.11) | Years in US, Age; Gender. | 5 |
| Ma et al. [43] | 2012 | USA | Cross-sectional | 311 | Self-reported compliance to CRC screening: 34.7% | Random sample of adults aged ≥ 50 years | For non-screening: Knowledge barriers: Adj OR = 3.3 (95%CI = 1.51, 7.23) Language barriers: Adj OR = 2.98 (95%CI = 1.2, 7.4) Time barriers: Adj OR = 4.68 (95%CI = 1.21, 18.11) | Psychological barrier; Insurance. | 7 |
| Sun et al. [39] | 2004 | USA | Cross-sectional | 203 | Self-reported FOBT in the past 12 month: 15.8% Self-reported FOBT plus SC in the past: 22.2% Self-reported FOBT or SC in the past: 37.9% | Adults aged ≥ 50 years | For ever screener vs non-screener: Years of residency: Adj OR = 0.545 (95%CI = 0.042, 0.045) Worry/fear: Adj OR = 0.658 (95%CI = 0.549, 0.788) Susceptibility: Adj OR = 1.502 (95%CI = 1.309, 1.724) For FOBT plus SC: Education year: Adj OR = 1.580 (95%CI = 1.015, 2.459) Worry/fear: Adj OR = 0.727 (95%CI = 0.629, 0.868) Susceptibility: Adj OR = 1.264 (95%CI = 1.127, 1.418) | For ever screener vs non-screener: Education; Family history of CRC; Self-efficacy; Social influence; Efficacy of screening; Intention. For FOBT plus SC: Years of residency in US, Self-efficacy; Social influence; Efficacy of screening; Intention. | 6 |
| Tang et al. [25] | 2001 | USA | Cross-sectional | 100 | Self-reported FOBT in the past: 25% Self-reported Sigmoidoscopy in the past: 31%: | Women aged ≥ 60 years | For FOBT: Acculturation: Adj OR = 5.54 (95%CI = 1.85, 16.60) For Sigmoidoscopy: Acculturation: Adj OR = 8.70 (95%CI = 2.07, 36.55) Lack of physician recommendation: Adj OR = 0.59 (95%CI = 0.40, 0.89) | For FOBT: No other variable was controlled in the multivariate analysis. For Sigmoidoscopy: Income; modesty; use of Eastern medicine. | 4 |
| Teng et al. [44] | 2006 | USA | Cross-sectional | 206 | Self-reported FOBT in the past: 65.0% Self-reported FS in the past: 54.0% Self-reported CS in the past: 49.2% | Adults aged ≥ 18 years | For FOBT: Physician recommendation: Adj OR = 3.71 (95%CI = 1.11, 12.46) For FS: Physician recommendation: Adj OR = 9.10 (95%CI = 1.87, 44.21) For CS: Physician recommendation: Adj OR = 9.52 (95%CI = 1.56, 58.82) | For FOBT: Acculturation; Risk perception. For FS: Acculturation; Risk perception. For CS: Acculturation; Risk perception. | 6 |
| Tu et al. [32] | 2006 | USA | Interventional | 210 | Medical record of FOBT: 48.5% | Adults aged ≥ 50 years | No significant factors other than the intervention | Age; Gender; Language; Insurance; Prior FOBT. | 7 |
| Wang et al. [26] | 2006 | USA | Cross-sectional | 433 | Self-reported CRC screening according to US guideline: 57% | Women aged ≥50 years | Physician recommendation: Adj OR = 3.44 (95%CI = 2.25, 5.28) Symptoms: Adj OR = 1.74 (95%CI = 1.10, 2.73) Thoughts about getting CRC: Adj OR = 2.79 (95%CI = 1.63, 4.77) Cultural views: Adj OR = 0.97 (95%CI = 0.95, 0.99) | All variables are significant in the multivariate analysis. | 6 |
| Yip et al. [31] | 2006 | USA | Cross-sectional | 383 | Medical record of CRC screening : 40% | Adults aged 50–78 years | No significant factor | Age; Gender; Insurance status; Language. | 6 |
| Yu et al. [35] | 2001 | USA | Cross-sectional | 664 | Self-reported DRE in the past: 14.1% Self-reported FOBT in the past: 8.5% | Random sample of adults aged 40–69 years | For DRE: Education ≥ 12 years: Adj OR = 2.38 (95%CI = 1.47, 3.84) For FOBT: Age < 55: Adj OR = 0.46 (95%CI = 0.29, 0.72) | For DRE: Age; Gender; Usual source of care; Cancer warning signs; Length of residency in US. For FOBT: Gender; Education; Usual source of care; Cancer warning signs; Length of residence in US. | 6 |
References
- World Health Organization. Cancer: Fact Sheet. 2013. Available online: http://www.who.int/mediacentre/factsheets/fs297/en/ (accessed on 1 March 2015).
- Pignone, M.; Saha, S.; Hoerger, T.; Mandelblatt, J. Cost-effectiveness analyses of colorectal cancer screening: A systematic review for the U.S. Preventive Services Task Force. Ann. Intern. Med. 2002, 137, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Walsh, J.; Terdiman, J. Colorectal cancer screening: Scientific review. J. Am. Med. Assoc. 2003, 289, 1288–1296. [Google Scholar] [CrossRef]
- Edwards, B.K.; Ward, E.; Kohler, B.A.; Eheman, C.; Zauber, A.G.; Anderson, R.N.; Jemal, A.; Schymura, M.J.; Lansdorp-Vogelaar, I.; Seeff, L.C.; et al. Annual report to the nation on the status of cancer, 1975–2006, featuring colorectal cancer trends and impact of interventions (risk factors, screening, and treatment) to reduce future rates. Cancer 2010, 116, 544–573. [Google Scholar] [CrossRef] [PubMed]
- Sung, J.J.Y.; Lau, J.Y.W.; Goh, K.L.; Leung, W.K.; Asia Pacific Working Group on Colorectal Cancer. Increasing incidence of colorectal cancer in Asia: Implications for screening. Lancet Oncol. 2005, 6, 871–876. [Google Scholar] [CrossRef]
- Ng, S.C.; Wong, S.H. Colorectal cancer screening in Asia. Br. Med. Bull. 2013, 105, 29–42. [Google Scholar] [CrossRef] [PubMed]
- Koo, J.H.; Leong, R.W.L.; Ching, J.; Yeoh, K.-G.; Wu, D.-C.; Murdani, A.; Cai, Q.; Chiu, H.-M.; Chong, V.H.; Rerknimitr, R.; et al. Knowledge of, attitudes toward, and barriers to participation of colorectal cancer screening tests in the Asia-Pacific region: A multicenter study. Gastrointest Endosc. 2012, 76, 126–135. [Google Scholar] [CrossRef] [PubMed]
- American Cancer Society. Colorectal Cancer Facts & Figures 2014–2016. 2014. Available online: http://www.cancer.org/acs/groups/content/documents/document/acspc-042280.pdf (accessed on 20 April 2015).
- Kiviniemi, M.T.; Bennett, A.; Zaiter, M.; Marshall, J.R. Individual-level factors in colorectal cancer screening: A review of the literature on the relation of individual-level health behavior constructs and screening behavior. Psychooncology 2011, 20, 1023–1033. [Google Scholar] [CrossRef] [PubMed]
- Power, E.; Miles, A.; von Wagner, C.; Robb, K.; Wardle, J. Uptake of colorectal cancer screening: System, provider and individual factors and strategies to improve participation. Future Oncol. 2009, 5, 1371–1388. [Google Scholar] [CrossRef] [PubMed]
- Gimeno García, A.Z. Factors influencing colorectal cancer screening participation. Gastroenterol. Res. Pract. 2012, 2012, 8. [Google Scholar] [CrossRef] [PubMed]
- Guessous, I.; Dash, C.; Lapin, P.; Doroshenk, M.; Smith, R.A.; Klabunde, C.N. Colorectal cancer screening barriers and facilitators in older persons. Prev. Med. 2010, 50, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Hwang, H. Colorectal cancer screening among Asian Americans. Asian Pac. J. Cancer Prev. 2013, 14, 4025–4032. [Google Scholar] [CrossRef] [PubMed]
- Sung, J.J.Y.; Ng, S.C.; Chan, F.K.L.; Chiu, H.M.; Kim, H.S.; Matsuda, T.; Ng, S.S.M.; Lau, J.Y.W.; Zheng, S.; Adler, S.; et al. An updated Asia Pacific consensus recommendations on colorectal cancer screening. Gut 2015, 64, 121–132. [Google Scholar] [CrossRef] [PubMed]
- Department of Health, the Hong Kong Special Region of Administration. CRC Screening Pilot Programme. 2016. Available online: http://www.colonscreen.gov.hk/en/colorectal-cancer-screening-pilot-program/about-the-colorectal-cancer-screening-pilot-program.html (accessed on 30 April 2016). [Google Scholar]
- Kang, L.N.; Qiao, R.L. Cancer screening and prevention in China. Cancer Control 2014, 8, 131–133. [Google Scholar]
- Taiwanese Bureau of Health Promotion. Cancer Control and Prevention. Available online: http://www.hpa.gov.tw/BHPNet/English/ClassPrint.aspx?No=201401280006.html (accessed on 12 May 2016).
- Health Promotion Board, Singapore Government. Colorectal Cancer. 2016. Available online: http://www.hpb.gov.sg/HOPPortal/dandc-article/598 (accessed on 30 April 2016). [Google Scholar]
- Johannesen, M.; LoGiudice, D. Elder abuse: A systematic review of risk factors in community-dwelling elders. Age Ageing 2013, 42, 292–298. [Google Scholar] [CrossRef] [PubMed]
- So, W.K.W.; Choi, K.C.; Chan, D.N.S.; Shiu, A.T.Y.; Ho, S.S.M.; Chan, H.Y.L.; Lam, W.W.T.; Cheng, K.K.F.; Goggins, W.; Chan, C.W.H. Colorectal cancer screening behaviour and associated factors among Chinese aged 50 and above in Hong Kong—A population-based survey. Eur. J. Oncol. Nurs. 2012, 16, 413–418. [Google Scholar] [CrossRef] [PubMed]
- So, W.K.W.; Choi, K.C.; Chan, D.N.S.; Chan, C.W.H.; Shiu, A.T.Y.; Ho, S.S.M.; Chan, H.Y.L.; Lam, W.W.T.; Cheng, K.K.F.; Goggins, W.B. Colorectal cancer testing and associated factors among older Chinese adults. Prev. Med. 2012, 54, 104–105. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.C.; Chan, H.Y.L.; Chan, D.N.S.; Lam, W.W.T.; Chan, C.W.H.; Ho, S.S.M.; Cheng, K.K.F.; Goggins, W.B.; Shiu, A.T.Y.; So, W.K.W. The mediating role of health professionals’ recommendation in the uptake of colorectal cancer testing among older Chinese adults. Int. J. Nurs. Pract. 2014, 20, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.C.; So, W.K.W.; Chan, D.N.S.; Shiu, A.T.Y.; Ho, S.S.M.; Chan, H.Y.L.; Lam, W.W.T.; Cheng, K.K.F.; Goggins, W.B.; Chan, C.W.H. Gender differences in the use of colorectal cancer tests among older Chinese adults. Eur. J. Oncol. Nurs. 2013, 17, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Leung, D.Y.P.; Leung, A.Y.M.; Chi, I. Breast and colorectal cancer screening and associated correlates among Chinese older women. Asian Pac. J. Cancer Prev. 2012, 13, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Tang, T.S.; Solomon, L.J.; McCracken, L.M. Barriers to fecal occult blood testing and sigmoidoscopy among older Chinese-American women. Cancer Pract. 2001, 9, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.H.Y.; Liang, W.; Chen, M.Y.; Cullen, J.; Feng, S.; Yi, B.; Schwartz, M.D.; Mandelblatt, J.S. The influence of culture and cancer worry on colon cancer screening among older Chinese-American women. Ethn. Dis. 2006, 16, 404–411. [Google Scholar] [PubMed]
- Todd, L.; Harvey, E.; Hoffman-Goetz, L. Predicting breast and colon cancer screening among English-as-a-second-language older Chinese immigrant women to Canada. J. Cancer Educ. 2011, 26, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.C.S.; Ching, J.Y.L.; Lam, T.Y.T.; Luk, A.K.C.; Hirai, H.W.; Griffiths, S.M.; Chan, F.K.L.; Sung, J.J.Y. Prospective cohort study of compliance with faecal immunochemical tests for colorectal cancer screening in Hong Kong. Prev. Med. 2013, 57, 227–231. [Google Scholar] [CrossRef] [PubMed]
- Cai, S.R.; Zhang, S.Z.; Zhu, H.H.; Zheng, S. Barriers to colorectal cancer screening: A case-control study. World J. Gastroenterol. 2009, 15, 2531–2536. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.G.; Zhang, T.; Wu, Y.; Huang, J. Case comparison study of the compliance influencing factors for colorectal cancer screening among residents in urban communities. Chin. J. Hosp. Admin. 2010, 26, 311–314. [Google Scholar]
- Yip, M.P.; Tu, S.P.; Chun, A.; Yasui, Y.; Taylor, V.M. Participation in colorectal cancer screening among Chinese Americans. Asian Pac. J. Cancer Prev. 2006, 7, 645–650. [Google Scholar] [PubMed]
- Tu, S.P.; Taylor, V.; Yasui, Y.; Chun, A.; Yip, M.P.; Acorda, E.; Li, L.; Bastani, R. Promoting culturally appropriate colorectal cancer screening through a health educator. Cancer 2006, 107, 959–966. [Google Scholar] [CrossRef] [PubMed]
- Chou, M.Y.; Hsu, P.I.; Chou, S.L.; Chou, Y.M.; Wang, F.W.; Hsueh, K.C.; Chen, L.K.; Hwang, S.J.; Tu, M.S. Factors related to incomplete flexible sigmoidoscopy among adult Chinese in Taiwan. J. Chin. Med. Assoc. 2007, 70, 361–366. [Google Scholar] [CrossRef]
- Kim, K.; Chapman, C.; Vallina, H. Colorectal cancer screening among Chinese American immigrants. J. Immigr. Minor. Health 2012, 14, 898–901. [Google Scholar] [CrossRef] [PubMed]
- Yu, E.S.H.; Kim, K.K.; Chen, E.H.; Brintnall, R.A.; Liu, W.T. Colorectal cancer screening among Chinese Americans. J. Psychosoc. Oncol. 2001, 19, 97–112. [Google Scholar] [CrossRef]
- Deng, S.X.; Gao, J.; An, W.; Yin, J.; Cai, Q.C.; Yang, H.; Li, Z.S. Colorectal cancer screening behavior and willingness: An outpatient survey in China. World J. Gastroenterol. 2011, 17, 3133–3139. [Google Scholar] [PubMed]
- Sung, J.J.Y.; Choi, S.Y.P.; Chan, F.K.L.; Ching, J.Y.L.; Lau, J.T.F.; Griffiths, S. Obstacles to colorectal cancer screening in Chinese: A study based on the health belief model. Am. J. Gastroenterol. 2008, 103, 974–981. [Google Scholar] [CrossRef] [PubMed]
- Ng, E.S.; Tan, C.H.; Teo, D.C.; Seah, C.Y.; Phua, K.H. Knowledge and perceptions regarding colorectal cancer screening among Chinese—A community-based survey in Singapore. Prev. Med. 2007, 45, 332–335. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.Y.; Basch, C.E.; Wolf, R.L.; Li, X.J. Factors associated with colorectal cancer screening among Chinese-Americans. Prev. Med. 2004, 39, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Leung, D.Y.P.; Wong, E.M.L.; Chan, C.W.H. Psychometric properties of a Chinese version of the Colorectal Cancer Perceptions Scale in a sample of older Chinese people. Cancer Nurs. 2014, 37, E53–E60. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z. The Status and Analysis of Influential Factors of Colorectal Cancer Screening among Community Residents in Shenyang. Ph.D. Thesis, China Medical University, Liaoning, China, March 2014. Available online: http://e.wanfangdata.com.hk/zh-TW/d/Thesis_Y2599947.aspx (accessed on 1 March 2015). [Google Scholar]
- Hong, S.Y. A Study on Strategy and Adherence to the Colonoscopic Screening for Colorectal Cancer. Ph.D. Thesis, The Second Military Medical University, Shanghai, China, May 2012. Available online: http://cdmd.cnki.com.cn/Article/CDMD-90024-1012404604.htm (accessed on 1 March 2015). [Google Scholar]
- Ma, G.X.; Wang, M.Q.; Toubbeh, J.; Tan, Y.; Shive, S.; Wu, D. Factors associated with colorectal cancer screening among Cambodians, Vietnamese, Koreans and Chinese living in the United States. N. Am. J. Med. Sci. (Boston) 2012, 5, 1–8. [Google Scholar] [CrossRef]
- Teng, E.J.; Friedman, L.C.; Green, C.E. Determinants of colorectal cancer screening behavior among Chinese Americans. Psychooncology 2006, 15, 374–381. [Google Scholar] [CrossRef] [PubMed]
- Green, P.M.; Kelly, B.A. Colorectal cancer knowledge, perceptions, and behaviors in African Americans. Cancer Nurs. 2004, 27, 206–215. [Google Scholar] [CrossRef] [PubMed]
- Von Wagner, C.; Good, A.; Whitaker, L.; Wardle, J. Psychosocial determinants of socioeconomic inequalities in cancer screening participation: A conceptual framework. Epidemiol. Rev. 2011, 33, 135–147. [Google Scholar] [CrossRef] [PubMed]
- Leung, D.Y.P.; Wong, E.M.L.; Chan, C.W.H. Determinants of participation in colorectal cancer screening among community-dwelling Chinese older people: Testing a comprehensive model using a descriptive correlational study. Eur. J. Oncol. Nurs. 2016, 21, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Carney, P.A.; Lee-Lin, F.; Mongoue-Tchokote, S.; Mori, M.; Leung, H.; Lau, C.; Le, T.D.; Lieberman, D.A. Improving colorectal cancer screening in Asian Americans: Results of a randomized intervention study. Cancer 2014, 120, 1702–1712. [Google Scholar] [CrossRef] [PubMed]
- Strecher, V.; Champion, V.; Rosenstock, I. The health belief model and health behavior. In Handbook of Health Behavior Research I: Personal and Social Determinations; Gochman, D.S., Ed.; Plenum Press: New York, NY, USA, 1997; pp. 71–91. [Google Scholar]
- Becker, M.H. The Health Belief Model and personal health behavior. Health Educ. Monogr. 1974, 2, 324–508. [Google Scholar] [CrossRef]
- Janz, N.K.; Becker, M.H. The Health Belief Model: A decade later. Health Educ. Q. 1984, 11, 1–47. [Google Scholar] [CrossRef] [PubMed]
- Rosenstock, I.M. Why people use health services. Milbank Mem. Fund. Q. 1966, 44, 94–127. [Google Scholar] [CrossRef] [PubMed]
- Peters, G.J.Y.; Ruiter, R.A.C.; Kok, G. Threatening communication: A critical re-analysis and a revised meta-analytic test of fear appeal theory. Health Psychol. Rev. 2013, 7 (Suppl. 1), S8–S31. [Google Scholar] [CrossRef] [PubMed]
- Choe, J.H.; Tu, S.P.; Lim, J.M.; Burke, N.J.; Acorda, E.; Taylor, V.M. “Heat in their intestine”: Colorectal cancer prevention beliefs among older Chinese Americans. Ethn. Dis. 2006, 16, 248–254. [Google Scholar] [PubMed]
- Jun, J.; Oh, K.M. Asian and Hispanic Americans’ cancer fatalism and colon cancer screening. Am. J. Health Behav. 2013, 37, 145–154. [Google Scholar] [CrossRef] [PubMed]

| Study | Type of CRC Screening | Significant Factors of Screening |
|---|---|---|
| Cai et al. [29] 1 | Data from registry of FOBT and CS | Knowledge |
| Chen et al. [30] 1 | Data from registry of compliance (FOBT and CS) | Understanding the purpose and method of the screening |
| Value CRC screening | ||
| Knowledge about CRC screening | ||
| Screening can improve health | ||
| Chou et al. [33] | FS screening at the site | For not completing of FS screening: |
| Female: Adj OR = 2.06 (95%CI = 1.56, 2.73) | ||
| Age ≥ 60: Adj OR = 1.68 (95%CI = 1.26, 2.23) | ||
| BMI < 25: Adj OR = 1.41 (95%CI = 1.05, 1.89) | ||
| History of constipation: Adj OR = 2.43 (95%CI = 1.04, 5.69) | ||
| Inadequate bowel preparation: Adj OR = 1.66 (95%CI = 1.21, 2.16) | ||
| Deng et al. [36] | Self-reported CRC screening in the past | Age ≥ 40: Adj OR = 3.834 (95%CI = 2.657, 5.532) |
| Health insurance : Adj OR = 1.996 ((5% CI = 1.426, 2.794) | ||
| Monthly household income ≥ 4000 RMB: Adj OR = 0.633 (95%CI = 0.467, 0.858) | ||
| High knowledge level (low as reference): Adj OR = 5.299 (95%CI = 3.415, 8.223) | ||
| Hong [42] | Self-reported CS in the past | Age ≥ 60: Adj OR = 0.682 (95%CI = 0.513, 0.916) |
| Health insurance: Adj OR = 1.835 (95%CI = 1.207, 2.931) | ||
| High knowledge (low as reference): Adj OR = 5.985 (95%CI = 3.471, 9.142) | ||
| Kim et al. [34] | FOBT test after educational session | Having primary-care physician: Adj OR = 4.72 (95%CI = 1.48, 15.11) |
| Leung et al. [24] | Self-reported of FOBT/endoscopy in the past two years | Cognitive impairment: Adj OR = 0.81 (95%CI = 0.66, 0.99) |
| Leung et al. [40] 1 | Self-reported CRC screening in the past | Severity–fear |
| Severity–life impact | ||
| Psychological barriers | ||
| Knowledge barriers | ||
| Liu [41] | Self-reported CRC screening in the past | Logistical regression with psychological factors: |
| Often have health check-up (never as reference): Adj OR = 2.938 (95%CI = 1.074, 8.038); | ||
| Have regular health check-up (never as reference): Adj OR = 6.747 (95%CI = 2.484, 18.330) | ||
| Exercise until reach the desirable pulse rate in sometime (never as reference): Adj OR = 3.447 (95%CI = 1.503, 7.907). | ||
| Logistical regression with environmental factors: | ||
| Discuss problems and worry with friends/family regularly (never as reference): Adj OR = 15.281 (95%CI = 1.788, 130.613); | ||
| Received recommendation for CRC screening: Adj OR = 61.328 (95%CI = 24.341, 154.521). | ||
| Ma et al. [43] | Self-reported compliance with CRC screening | For non-screening: |
| Knowledge barriers: Adj OR = 3.3 (95%CI = 1.51, 7.23) | ||
| Language barriers: Adj OR = 2.98 (95%CI = 1.2, 7.4) | ||
| Time barriers: Adj OR = 4.68 (95%CI = 1.21, 18.11) | ||
| Ng et al. [38] | Self-reported FOBT in the past | Had other screening: Adj OR = 3.47 (95%CI = 1.75, 6.91) |
| Influenced by family/friends: Adj OR = 2.14 (95%CI = 1.02, 4.49) | ||
| Knowledge: Adj OR = 1.03 (95%CI = 1.01, 1.04) | ||
| Severity: Adj OR = 0.97 (95%CI = 0.96, 0.99) | ||
| So et al. [20] | Self-reported ever CS; Self-reported ever FOBT | For CS: |
| Male: Adj OR = 1.58 (95%CI = 1.19, 2.10) | ||
| Family history of cancer: Adj OR = 1.43 (95%CI = 1.05, 1.95) | ||
| Had serious disease/cancer: Adj OR = 2.62 (95%CI = 1.79, 3.83) | ||
| Poor perceived health status: Adj OR = 1.38 (95%CI = 1.02, 1.86) | ||
| Perceived visiting a doctor regularly is good for health: Adj OR = 2.42 (95%CI = 1.81, 3.24) | ||
| Healthcare professional recommendation: Adj OR = 11.04 (95%CI = 6.49, 18.77) | ||
| For FOBT: | ||
| Had serious disease/cancer: Adj OR = 1.50 (95%CI = 1.04, 2.10) | ||
| Ex-smoker (non-smoker as reference): Adj OR = 1.45 (95%CI = 1.05, 2.02) | ||
| Perceived visiting a doctor regularly is good for health: Adj OR = 1.96 (95%CI = 2.49) | ||
| Perceived taking dietary supplement is good for health: Adj OR = 1.54 (95%CI = 1.18, 2.01) | ||
| Use of complementary medicine: Adj OR = 1.54 (95%CI = 1.18, 2.01) | ||
| Sun et al. [39] | Self-reported FOBT in the past 12 months; Self-reported FOBT plus SC in the past; Self-reported FOBT or SC in the past | For ever screener vs. non-screener: |
| Years of residency: Adj OR = 0.545 (95%CI = 0.042, 0.045) | ||
| Worry/fear: Adj OR = 0.658 (95%CI = 0.549, 0.788) | ||
| Susceptibility: Adj OR = 1.502 (95%CI = 1.309, 1.724) | ||
| For FOBT plus SC: | ||
| Education year: Adj OR = 1.580 (95%CI = 1.015, 2.459) | ||
| Worry/fear: Adj OR = 0.727 (95%CI = 0.629, 0.868) | ||
| Susceptibility: Adj OR = 1.264 (95%CI = 1.127, 1.418) | ||
| Sung et al. [37] | Self-reported CRC screening uptake in the past | Middle knowledge of CRC symptoms level (low as reference): Adj OR = 3.33 (95%CI = 1.22, 9.11) |
| High knowledge of CRC risk factors level (low as reference): Adj OR = 2.61 (95%CI = 1.18, 5.88) | ||
| Middle perceived severity of CRC level (low as reference): Adj OR = 0.28 (95%CI = 0.13, 0.65) | ||
| Middle health/psychological barriers level (low as reference): Adj OR = 0.42 (95%CI = 0.21, 0.85) | ||
| High access barrier level (low as reference): Adj OR = 0.22 (95%CI = 0.06, 0.85) | ||
| Health insurance: Adj OR = 2.06 (95%CI = 1.01, 4.19) | ||
| Physician recommendation: Adj OR = 23.05 (95%CI = 10.66, 51.80) | ||
| Tang et al. [25] | Self-reported FOBT in the past; Self-reported sigmoidoscopy in the past | For FOBT: |
| Acculturation: Adj OR = 5.54 (95%CI = 1.85, 16.60) | ||
| For sigmoidoscopy: | ||
| Acculturation: Adj OR = 8.70 (95%CI = 2.07, 36.55) | ||
| Lack of physician recommendation: Adj OR = 0.59 (95%CI = 0.40, 0.89) | ||
| Teng et al. [44] | Self-reported FOBT in the past; Self-reported FS in the past; Self-reported CS in the past | For FOBT: |
| Physician recommendation: Adj OR = 3.71 (95%CI = 1.11, 12.46) | ||
| For FS: | ||
| Physician recommendation: Adj OR = 9.10 (95%CI = 1.87, 44.21) | ||
| For CS: | ||
| Physician recommendation: Adj OR = 9.52 (95%CI = 1.56, 58.82) | ||
| Todd et al. [27] | Self-reported CRC screening | No physician recommendation: Adj OR = 0.103 (95%CI = 0.031, 0.349) |
| Cantonese as 1st language: Adj OR = 1.85 (95%CI = 0.055, 0.628) | ||
| Self-efficacy: Adj OR = 3.613 (95%CI = 1.179, 11.070) | ||
| Tu et al. [32] | Medical record of FOBT: 48.5% | No significant factors other than the intervention |
| Wang et al. [26] | Self-reported CRC screening according to US guideline | Physician recommendation: Adj OR = 3.44 (95%CI = 2.25, 5.28) |
| Symptoms: Adj OR = 1.74 (95%CI = 1.10, 2.73) | ||
| Thoughts about getting CRC: Adj OR = 2.79 (95%CI = 1.63, 4.77) | ||
| Cultural views: Adj OR = 0.97 (95%CI = 0.95, 0.99) | ||
| Wong et al. [28] | Compliance of annual FIT checked by returned specimens | Female: Adj OR = 1.27 (95%CI = 1.11, 1.45) |
| Age 55–59 (50–54 as reference): Adj OR = 0.82 (95%CI = 0.70, 0.95) | ||
| Age 65–70 (50–54 as reference): Adj OR = 1.54 (95%CI = 1.26, 1.89) | ||
| Non-smoking: Adj OR = 1.84 (95%CI = 1.43, 2.37) | ||
| Family history of bowel cancer | ||
| 1st degree relative: Adj OR = 0.74 (95%CI = 0.61, 0.89) | ||
| 2nd degree relative: Adj OR = 0.78 (95%CI = 0.65, 0.94) | ||
| Yip et al. [31] | Medical record of CRC screening | No significant factor |
| Yu et al. [35] | Self-reported DRE in the past; Self-reported FOBT in the past | For DRE: |
| Education ≥ 12 years: Adj OR = 2.38 (95%CI = 1.47, 3.84) | ||
| For FOBT: | ||
| Age < 55: Adj OR = 0.46 (95%CI = 0.29, 0.72) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leung, D.Y.P.; Chow, K.M.; Lo, S.W.S.; So, W.K.W.; Chan, C.W.H. Contributing Factors to Colorectal Cancer Screening among Chinese People: A Review of Quantitative Studies. Int. J. Environ. Res. Public Health 2016, 13, 506. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13050506
Leung DYP, Chow KM, Lo SWS, So WKW, Chan CWH. Contributing Factors to Colorectal Cancer Screening among Chinese People: A Review of Quantitative Studies. International Journal of Environmental Research and Public Health. 2016; 13(5):506. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13050506
Chicago/Turabian StyleLeung, Doris Y. P., Ka Ming Chow, Sally W. S. Lo, Winnie K. W. So, and Carmen W. H. Chan. 2016. "Contributing Factors to Colorectal Cancer Screening among Chinese People: A Review of Quantitative Studies" International Journal of Environmental Research and Public Health 13, no. 5: 506. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13050506