
Prenatal Exposure to Perfluoroalkyl Substances and Behavioral Development in Children

Abstract
:1. Introduction
2. Materials and Methods
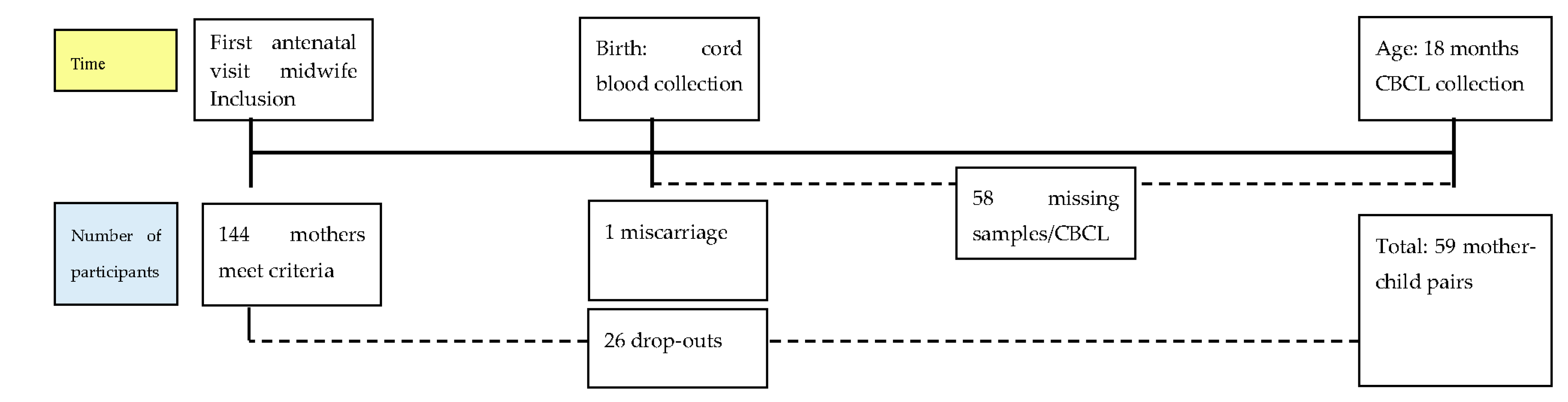
2.1. Linking Maternal Nutrition to Child Health (LINC) Cohort
2.2. Chemical Exposure
Behavioral Assessment
2.3. Covariates
2.4. Analysis
3. Results
3.1. Sample Characteristics
3.2. Exposure Levels
3.3. Associations between Perfluoroalkyl Substances (PFASs) and Behavioral Variables at 18 Months
3.3.1. Attention Deficit Hyperactivity Disorder (ADHD) Symptoms
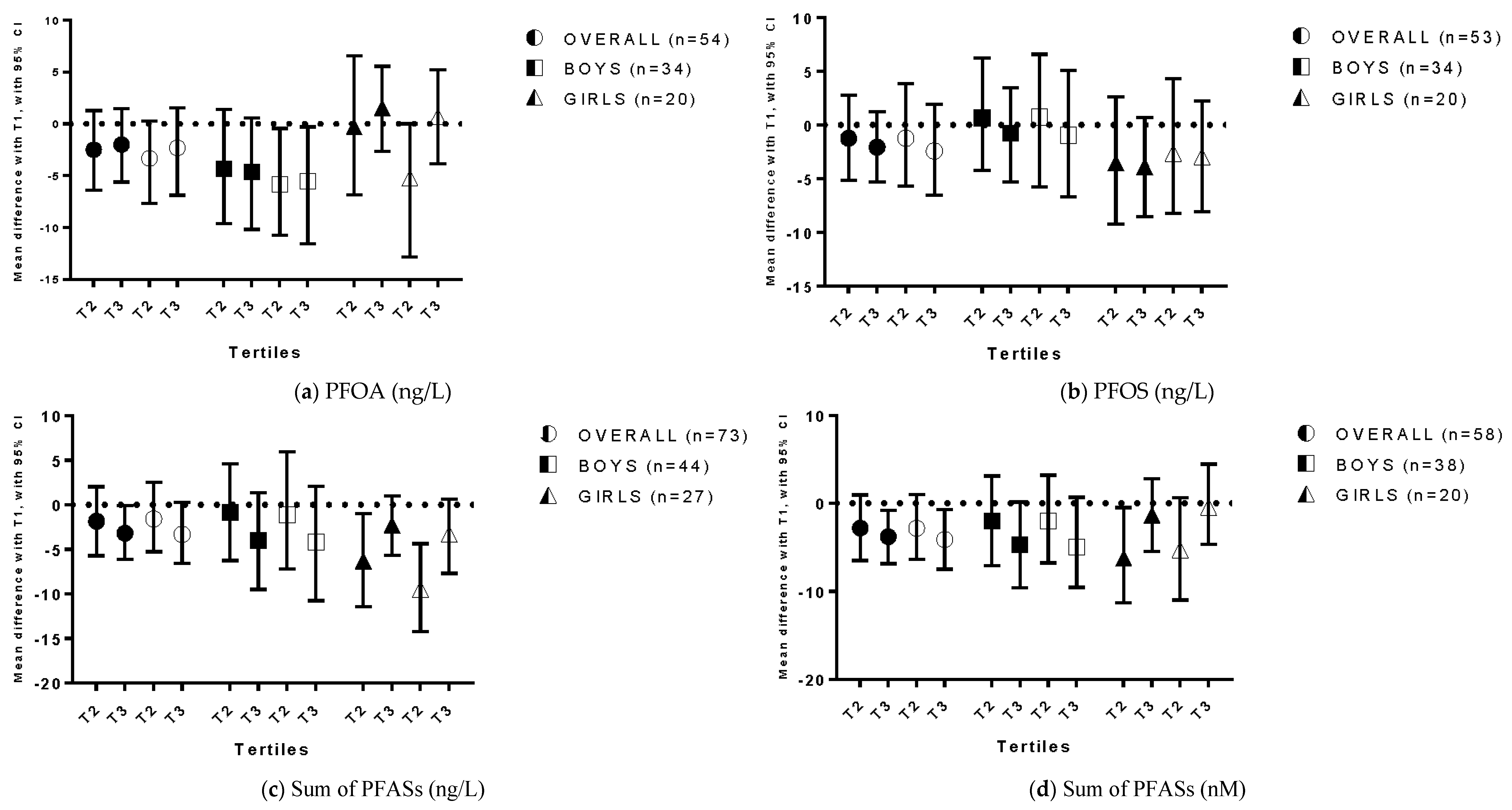
3.3.2. Externalizing Problems
3.4. Sensitivity Analyses
4. Discussion
5. Conclusions
Appendix

{kind=link}
{kind=link}
{kind=link}
| Compound | N | Matrix | Unit of Conc. | T1 | T2 | T3 | ||
|---|---|---|---|---|---|---|---|---|
| β (95% CI) | p-Value | β (95% CI) | p-Value | |||||
| PFOA | 200.0−640.0 | 640.1−1000.0 | 1000.1−2300.0 | |||||
| Crude model | 53 | CP | ng/L | Ref. | −0.18 (−1.56; 1.11) | 0.78 | −0.31 (−1.35; 0.79) | 0.55 |
| Adjusted model 1 | 53 | CP | ng/L | Ref. | −0.33 (−1.99; 1.20) | 0.70 | −0.24 (−1.65; 0.85) | 0.72 |
| PFOS | 570.0−1200.0 | 1200.1−1800.0 | 1800.1−3200.0 | |||||
| Crude model | 53 | CP | ng/L | Ref. | −0.27 (−1.58; 1.09) | 0.70 | −0.62 (−1.67; 0.41) | 0.26 |
| Adjusted model 2 | 53 | CP | ng/L | Ref. | −0.33 (−1.75; 1.17) | 0.66 | −0.87 (−2.06; 0.42) | 0.19 |
| Sum PFASs | 982.0−2517.8 | 2517.9−3337.7 | 3337.8−5969.0 | |||||
| Crude model | 53 | CP | ng/L | Ref. | −0.79 (−2.06; 0.49) | 0.23 | −0.81 (−1.82; 0.17) | 0.13 |
| Adjusted model 3 | 53 | CP | ng/L | Ref. | −0.72 (−1.96; 0.59) | 0.31 | −0.99 (−2.14; 0.18) | 0.11 |
| Sum PFASs (nM) | 2.08−5.36 | 5.37−7.21 | 7.22−13.12 | |||||
| Crude model | 59 | CP | nM | Ref. | −0.84 (−2.06; 0.43) | 0.20 | −0.53 (−1.58; 0.58) | 0.36 |
| Adjusted model 4 | 59 | CP | nM | Ref. | −0.84 (−2.05; 0.37) | 0.18 | −0.53 (−1.62; 0.59) | 0.33 |
| Compound | N | Matrix | Unit of Conc. | T1 | T2 | T3 | ||
|---|---|---|---|---|---|---|---|---|
| β (95% CI) | p-Value | β (95% CI) | p-Value | |||||
| PFOA | 200.0−640.0 | 640.1−1000.0 | 1000.1−2300.0 | |||||
| Crude model | 54 | CP | ng/L | Ref. | −2.50 (−6.39; 1.28) | 0.19 | −2.00 (−5.62; 1.46) | 0.28 |
| Adjusted model 1 | 54 | CP | ng/L | Ref. | −3.33 (−7.65; 0.29) | 0.12 | −2.30 (−6.88; 1.55) | 0.31 |
| PFOS | 570.0−1200.0 | 1200.1−1800.0 | 1800.1−3200.0 | |||||
| Crude model | 53 | CP | ng/L | Ref. | −1.24 (−5.15; 2.79) | 0.58 | −2.08 (−5.31; 1.22) | 0.22 |
| Adjusted model 2 | 53 | CP | ng/L | Ref. | −1.23 (−5.68; 3.85) | 0.62 | −2.43 (−6.55; 1.93) | 0.31 |
| Sum PFASs | 982.0−2517.8 | 2517.9−3337.7 | 3337.8−5969.0 | |||||
| Crude model | 56 | CP | ng/L | Ref. | −1.84 (−5.71; 2.04) | 0.33 | −3.19 (−6.10; −0.07) | 0.04 |
| Adjusted model 3 | 56 | CP | ng/L | Ref. | −1.59 (−5.27; 2.50) | 0.45 | −3.31 (−6.55; 0.28) | 0.07 |
| Sum PFASs (nM) | 2.08−5.36 | 5.37−7.21 | 7.22−13.12 | |||||
| Crude model | 58 | CP | nM | Ref. | −2.82 (−6.50; 0.95) | 0.15 | −3.80 (−6.86; −0.79) | 0.03 |
| Adjusted model 4 | 58 | CP | nM | Ref. | −2.83 (−6.40; 0.99) | 0.14 | −4.11 (−7.49; −0.68) | 0.03 |
| Compound | Boys | Girls | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | T1 | T2 | T3 | N | T1 | T2 | T3 | |||||
| β (95% CI) | p-Value | β (95% CI) | p-Value | β (95% CI) | p-Value | β (95% CI) | p-Value | |||||
| PFOA | 200.0–670.0 | 670.1–1000.0 | 1000.1–2300.0 | 300.0–560.0 | 560.1–909.9 | 910.0–1700.0 | ||||||
| Crude model | 34 | Ref. | −0.64 (−2.40; 1.27) | 0.54 | −0.83 (−2.34; 0.75) | 0.32 | 19 | Ref. | 0.38 (−0.97; 1.71) | 0.59 | 0.38 (−1.41; 2.18) | 0.68 |
| Adj. model 1 | 34 | Ref. | −1.13 (−3.13; 0.79) | 0.27 | −1.06 (−2.82; 0.45) | 0.22 | 19 | Ref. | 0.31 (−2.44; 3.33) | 0.79 | 0.68 (−0.66; 2.11) | 0.31 |
| PFOS | 570.0–1300.0 | 1300.1–1800.0 | 1800.1–2900.0 | 570.0–906.7 | 906.8–1866.5 | 1866.6–3200.0 | ||||||
| Crude model | 34 | Ref. | −0.42 (−2.31; 1.41) | 0.62 | −0.75 (−2.21; 0.71) | 0.32 | 19 | Ref. | −0.13 (−1.50; 1.11) | 0.87 | −0.48 (−1.97; 1.20) | 0.56 |
| Adj. model 2 | 34 | Ref. | −0.55 (−2.84; 1.57) | 0.64 | −0.99 (−3.03; 0.92) | 0.35 | 19 | Ref. | 0.17 (−1.50; 1.67) | 0.85 | −0.73 (−2.36; 0.90) | 0.43 |
| Sum PFASs | 982.0–2665.9 | 2666.0–3337.8 | 3337.9–5969.0 | 1121.0–1894.9 | 1895.0–3618.2 | 3618.3–4622.0 | ||||||
| Crude model | 34 | Ref. | −1.04 (−2.81; 0.72) | 0.26 | −1.34 (−2.80; 0.10) | 0.07 | 20 | Ref. | −0.85 (−2.45; 0.80) | 0.33 | −0.10 (−1.38; 1.47) | 0.92 |
| Adj. model 3 | 34 | Ref. | −1.06 (−2.82; 0.73) | 0.65 | −1.33 (−3.00; 0.27) | 0.11 | 20 | Ref. | −0.85 (−2.50; 0.78) | 0.38 | −0.60 (−1.99; 0.83) | 0.43 |
| Sum PFASs (nM) | 2.08–5.80 | 5.81–7.21 | 7.22–13.12 | 2.44–4.15 | 4.16–7.76 | 7.77–9.99 | ||||||
| Crude model | 38 | Ref. | −1.04 (−2.53; 0.68) | 0.24 | −1.21 (−2.67; 0.46) | 0.13 | 20 | Ref. | −0.92 (−2.69; 0.56) | 0.30 | 0.33 (−1.30; 2.17) | 0.74 |
| Adj. model 4 | 38 | Ref. | −1.03 (−2.81; 0.73) | 0.23 | −1.32 (−2.86; 0.43) | 0.12 | 20 | Ref. | −1.10 (−2.84; 1.01) | 0.30 | 0.57 (−1.00; 2.55) | 0.57 |
| Compound | Boys | Girls | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | T1 | T2 | T3 | N | T1 | T2 | T3 | |||||
| β (95% CI) | p-Value | β (95% CI) | p-Value | β (95% CI) | p-Value | β (95% CI) | p-Value | |||||
| PFOA | 200.0–670.0 | 670.1–1000.0 | 1000.1–2300.0 | 300.0–560.0 | 560.1–909.9 | 910.0–1700.0 | ||||||
| Crude model | 34 | Ref. | −4.32 (−9.62; 1.42) | 0.13 | −4.61 (−10.18; 0.59) | 0.11 | 20 | Ref. | −0.31 (−6.87; 6.56) | 0.93 | 1.56 (−2.65; 5.55) | 0.47 |
| Adjusted model 1 | 34 | Ref. | −5.87 (−10.76;−0.43) | 0.05 | −5.54 (−11.57; −0.29) | 0.09 | 20 | Ref. | −5.24 (−12.82; 0.00) | 0.10 | 0.71 (−3.83; 5.21) | 0.74 |
| PFOS | 570.0–1300.0 | 1300.1–1800.0 | 1800.1–2900.0 | 570.0–906.7 | 906.8–1866.5 | 1866.6–3200.0 | ||||||
| Crude model | 34 | Ref. | 0.65 (−4.27; 6.21) | 0.80 | −0.77 (−5.30; 3.45) | 0.74 | 20 | Ref. | −3.55 (−9.22; 2.59) | 0.26 | −3.89 (−8.57; 0.68) | 0.11 |
| Adjusted model 2 | 34 | Ref. | 0.72 (−5.77; 6.59) | 0.81 | −0.94 (−6.72; 5.12) | 0.74 | 20 | Ref. | −2.63 (−8.21; 4.33) | 0.44 | −2.98 (−8.08; 2.23) | 0.31 |
| Sum PFASs | 982.0–2665.9 | 2666.0–3337.8 | 3337.9–5969.0 | 1121.0–1894.9 | 1895.0–3618.2 | 3618.3–4622.0 | ||||||
| Crude model | 34 | Ref. | −0.84 (−6.27; 4.61) | 0.77 | −4.01 (−9.48; 1.38) | 0.16 | 20 | Ref. | −6.30 (−11.42; −0.99) | 0.03 | −2.30 (−5.65; 1.02) | 0.22 |
| Adj. model 3 | 34 | Ref. | −1.09 (−7.22; 5.95) | 0.74 | −4.20 (−10.73; 2.08) | 0.22 | 20 | Ref. | −9.50 (−14.21; −4.35) | 0.01 | −3.29 (−7.69; 0.66) | 0.13 |
| Sum PFASs (nM) | 2.08–5.80 | 5.81–7.21 | 7.22–13.12 | 2.44–4.15 | 4.16–7.76 | 7.77–9.99 | ||||||
| Crude model | 38 | Ref. | −2.05 (−7.07; 3.11) | 0.44 | −4.75 (−9.62; 0.13) | 0.07 | 20 | Ref. | −6.22 (−11.28; −0.50) | 0.03 | −1.37 (−5.50; 2.79) | 0.49 |
| Adj. model 4 | 38 | Ref. | −2.04 (−6.77; 3.21) | 0.42 | −4.93 (−9.56; 0.69) | 0.07 | 20 | Ref. | −5.29 (−11.00; 0.67) | 0.09 | −0.43 (−4.67; 4.47) | 0.85 |
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| ADHD | Attention Deficit Hyperactivity Disorder |
| CBCL 1.5–5 | Child Behavior Checklist 1.5–5 |
| LOQ | Limit of quantification |
| PFASs | Perfluoroalkyl substances |
| PFDA | Perfluoro-n-decanoic |
| PFHxS | Perfluorohexane sulfonate |
| PFHpS | Perfluoroheptane sulfonate |
| PFNA | Perfluorononanoic acid |
| PFOA | Perfluorooctanoic acid |
| PFOS | Perfluorooctanesulfonic acid |
| PFUnDA | Perfluoroundecanoic acid |
References
- Atladottir, H.O.; Gyllenberg, D.; Langridge, A.; Sandin, S.; Hansen, S.N.; Leonard, H.; Gissler, M.; Reichenberg, A.; Schendel, D.E.; Bourke, J.; et al. The increasing prevalence of reported diagnoses of childhood psychiatric disorders: A descriptive multinational comparison. Eur. Child Adolesc. Psychiatry 2015, 24, 173–183. [Google Scholar] [CrossRef] [PubMed]
- Holtmann, M.; Duketis, E.; Poustka, L.; Zepf, F.D.; Poustka, F.; Bölte, S. Bipolar disorder in children and adolescents in Germany: National trends in the rates of inpatients, 2000–2007. Bipolar. Disord. 2010, 12, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Meng, X.; D’Arcy, C.; Tempier, R. Long-term trend in pediatric antidepressant use, 1983–2007: A population-based study. Can. J. Psychiatry 2014, 59, 89–97. [Google Scholar] [PubMed]
- Centers for Disease Control and Prevention (CDC). Attention-Deficit/Hyperactivity Disorder (ADHD)—Data and Statistics; CDC: Atlanta, GA, USA, 2014.
- Chien, I.C.; Lin, C.H.; Chou, Y.J.; Chou, P. Prevalence, incidence, and stimulant use of attention-deficit hyperactivity disorder in Taiwan, 1996–2005: A national population-based study. Soc. Psychiatry Psychiatr. Epidemiol. 2012, 47, 1885–1890. [Google Scholar] [CrossRef] [PubMed]
- Neggers, Y.H. Increasing prevalence, changes in diagnostic criteria, and nutritional risk factors for autism spectrum disorders. ISRN Nutr. 2014, 2014. [Google Scholar] [CrossRef] [PubMed]
- Sjowall, D.; Backman, A.; Thorell, L.B. Neuropsychological Heterogeneity in Preschool ADHD: Investigating the Interplay between Cognitive, Affective and Motivation-Based Forms of Regulation. J. Abnorm. Child Psychol. 2014, 43, 669–680. [Google Scholar] [CrossRef] [PubMed]
- Nigg, J.T.; Casey, B.J. An integrative theory of attention-deficit/ hyperactivity disorder based on the cognitive and affective neurosciences. Dev. Psychopathol. 2005, 17, 785–806. [Google Scholar] [CrossRef] [PubMed]
- Klahr, A.M.; Burt, S.A. Evaluation of the known behavioral heterogeneity in conduct disorder to improve its assessment and treatment. J. Child Psychol. Psychiatry 2014, 55, 1300–1310. [Google Scholar] [CrossRef] [PubMed]
- Kemf, E. Global Chemicals Outlook: Towards Sound Management of Chemicals; United Nations Environment Programme (UNEP): Nairobi, Kenya, 2013. [Google Scholar]
- Organisation for Economic Co-Operation and Development (OECD). Hazard Assessment of Perfluorooctane Sulfonate (PFOS) and Its Salts; OECD: Paris, France, 2002. [Google Scholar]
- US Environmental Protection Agency (EPA). Long-Chain Perfluorinated Chemicals (PFCs) Action Plan; EPA: Washington, DC, USA, 2009.
- Agency for Toxic Substances and Disease Registry (ATSDR). Draft Toxicological Profile for Perfluoroalkyls; ATSDR: Atlanta, GA, USA, 2015.
- European Commission. COMMISSION REGULATION (EU) No 757/2010 of 24 August 2010 amending Regulation (EC) No 850/2004 of the European Parliament and of the Council on persistent organic pollutants as regards Annexes I and III, in Official. J. Eur. Union 2010, 68, 234–241. [Google Scholar]
- US Environmental Protection Agency (EPA). Emerging Contaminants—Perfluorooctane Sulfonate (PFOS) and Perfluorooctanoic Acid (PFOA); EPA: Washington, DC, USA, 2014.
- D’Eon, J.C.; Mabury, S.A. Is indirect exposure a significant contributor to the burden of perfluorinated acids observed in humans? Environ. Sci. Technol. 2011, 45, 7974–7984. [Google Scholar] [CrossRef] [PubMed]
- Kato, K.; Wong, L.Y.; Jia, L.T.; Kuklenyik, Z.; Calafat, A.M. Trends in exposure to polyfluoroalkyl chemicals in the U.S. Population: 1999–2008. Environ. Sci. Technol. 2011, 45, 8037–8045. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.S.; Nørgaard-Pedersen, B.; Toft, G.; Hougaard, D.M.; Bonde, J.P.; Cohen, A.; Thulstrup, A.M.; Ivell, R.; Anand-Ivell, R.; Lindh, C.H.; et al. Phthalates and perfluorooctanesulfonic acid in human amniotic fluid: Temporal trends and timing of amniocentesis in pregnancy. Environ. Health Perspect. 2012, 120, 897–903. [Google Scholar] [CrossRef] [PubMed]
- Stein, C.R.; Wolff, M.S.; Calafat, A.M.; Kato, K.; Engel, S.M. Comparison of polyfluoroalkyl compound concentrations in maternal serum and amniotic fluid: A pilot study. Reprod. Toxicol. 2012, 34, 312–316. [Google Scholar] [CrossRef] [PubMed]
- Inoue, K.; Okada, F.; Ito, R.; Kato, S.; Sasaki, S.; Nakajima, S.; Uno, A.; Saijo, Y.; Sata, F.; Yoshimura, Y.; et al. Perfluorooctane sulfonate (PFOS) and related perfluorinated compounds in human maternal and cord blood samples: Assessment of PFOS exposure in a susceptible population during pregnancy. Environ. Health Perspect. 2004, 112, 1204–1207. [Google Scholar] [CrossRef] [PubMed]
- Midasch, O.; Drexler, H.; Hart, N.; Beckmann, M.W.; Angerer, J. Transplacental exposure of neonates to perfluorooctanesulfonate and perfluorooctanoate: A pilot study. Int. Arch. Occup. Environ. Health 2007, 80, 643–648. [Google Scholar] [CrossRef] [PubMed]
- Kuklenyik, Z.; Reich, J.A.; Tully, J.S.; Needham, L.L.; Calafat, A.M. Automated solid-phase extraction and measurement of perfluorinated organic acids and amides in human serum and milk. Environ. Sci. Technol. 2004, 38, 3698–3704. [Google Scholar] [CrossRef] [PubMed]
- So, M.K.; Yamashita, N.; Taniyasu, S.; Jiang, Q.; Giesy, J.P.; Chen, K.; Lam, P.K. Health risks in infants associated with exposure to perfluorinated compounds in human breast milk from Zhoushan, China. Environ. Sci. Technol. 2006, 40, 2924–2929. [Google Scholar] [CrossRef] [PubMed]
- Tao, L.; Kannan, K.; Wong, C.M.; Arcaro, K.F.; Butenhoff, J.L. Perfluorinated compounds in human milk from Massachusetts, USA. Environ. Sci. Technol. 2008, 42, 3096–3101. [Google Scholar] [CrossRef] [PubMed]
- Stein, C.R.; Savitz, D.A.; Bellinger, D.C. Perfluorooctanoate exposure in a highly exposed community and parent and teacher reports of behaviour in 6–12-year-old children. Paediatr. Perinat. Epidemiol. 2014, 28, 146–156. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Li, J.; Liu, Y.; Chan, H.M.; Zhao, Y.; Cai, Z.; Wu, Y. Comparison on gestation and lactation exposure of perfluorinated compounds for newborns. Environ. Int. 2011, 37, 1206–1212. [Google Scholar] [CrossRef] [PubMed]
- Halldorsson, T.I.; Rytter, D.; Haug, L.S.; Bech, B.H.; Danielsen, I.; Becher, G.; Henriksen, T.B.; Olsen, S.F. Prenatal exposure to perfluorooctanoate and risk of overweight at 20 years of age: A prospective cohort study. Environ. Health Perspect. 2012, 120, 668–673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lv, Z.; Li, G.; Li, Y.; Ying, C.; Chen, J.; Chen, T.; Wei, J.; Lin, Y.; Jiang, Y.; Wang, Y.; et al. Glucose and lipid homeostasis in adult rat is impaired by early-life exposure to perfluorooctane sulfonate. Environ. Toxicol. 2013, 28, 532–542. [Google Scholar] [CrossRef] [PubMed]
- White, S.S.; Fenton, S.E.; Hines, E.P. Endocrine disrupting properties of perfluorooctanoic acid. J. Steroid Biochem. Mol. Biol. 2011, 127, 16–26. [Google Scholar] [CrossRef] [PubMed]
- Kirkley, A.G.; Sargis, R.M. Environmental endocrine disruption of energy metabolism and cardiovascular risk. Curr. Diab. Rep. 2014, 14, 494. [Google Scholar] [CrossRef] [PubMed]
- Taylor, K.W.; Hoffman, K.; Thayer, K.A.; Daniels, J.L. Polyfluoroalkyl chemicals and menopause among women 20–65 years of age (NHANES). Environ. Health Perspect. 2014, 122, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Knox, S.S.; Jackson, T.; Javins, B.; Frisbee, S.J.; Shankar, A.; Ducatman, A.M. Implications of early menopause in women exposed to perfluorocarbons. J. Clin. Endocrinol. Metab. 2011, 96, 1747–1753. [Google Scholar] [CrossRef] [PubMed]
- Harada, K.H.; Koizumi, A. Environmental and biological monitoring of persistent fluorinated compounds in Japan and their toxicities. Environ. Health Prev. Med. 2009, 14, 7–19. [Google Scholar] [CrossRef] [PubMed]
- Legler, J.; Fletcher, T.; Govarts, E.; Porta, M.; Blumberg, B.; Heindel, J.J.; Trasande, L. Obesity, diabetes, and associated costs of exposure to endocrine-disrupting chemicals in the European Union. J. Clin. Endocrinol. Metab. 2015, 100, 1278–1288. [Google Scholar] [CrossRef] [PubMed]
- Hauser, R.; Skakkebaek, N.E.; Hass, U.; Toppari, J.; Juul, A.; Andersson, A.M.; Kortenkamp, A.; Heindel, J.J.; Trasande, L. Male reproductive disorders, diseases, and costs of exposure to endocrine-disrupting chemicals in the European Union. J. Clin. Endocrinol. Metab. 2015, 100, 1267–1277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grindler, N.M.; Allsworth, J.E.; Macones, G.A.; Kannan, K.; Roehl, K.A.; Cooper, A.R. Persistent organic pollutants and early menopause in U.S. women. PLoS ONE 2015, 10, e0116057. [Google Scholar]
- Zawatski, W.; Lee, M.M. Male pubertal development: Are endocrine-disrupting compounds shifting the norms? J. Endocrinol. 2013, 218, R1–R12. [Google Scholar] [CrossRef] [PubMed]
- Zoeller, R.T.; Brown, T.R.; Doan, L.L.; Gore, A.C.; Skakkebaek, N.E.; Soto, A.M.; Woodruff, T.J.; Vom Saal, F.S. Endocrine-disrupting chemicals and public health protection: A statement of principles from The Endocrine Society. Endocrinology 2012, 153, 4097–4110. [Google Scholar] [CrossRef] [PubMed]
- DiVall, S.A. The influence of endocrine disruptors on growth and development of children. Curr. Opin. Endocrinol. Diabetes Obes. 2013, 20, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Onishchenko, N.; Fischer, C.; Wan Ibrahim, W.N.; Negri, S.; Spulber, S.; Cottica, D.; Ceccatelli, S. Prenatal exposure to PFOS or PFOA alters motor function in mice in a sex-related manner. Neurotox. Res. 2011, 19, 452–461. [Google Scholar] [CrossRef] [PubMed]
- Stein, C.R.; Savitz, D.A. Serum perfluorinated compound concentration and attention deficit/hyperactivity disorder in children 5–18 years of age. Environ. Health Perspect. 2011, 119, 1466–1471. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, K.; Webster, T.F.; Weisskopf, M.G.; Weinberg, J.; Vieira, V.M. Exposure to polyfluoroalkyl chemicals and attention deficit/hyperactivity disorder in U.S. children 12–15 years of age. Environ. Health Perspect. 2010, 118, 1762–1767. [Google Scholar] [CrossRef] [PubMed]
- Gump, B.B.; Wu, Q.; Dumas, A.K.; Kannan, K. Perfluorochemical (PFC) exposure in children: Associations with impaired response inhibition. Environ. Sci. Technol. 2011, 45, 8151–8159. [Google Scholar] [CrossRef] [PubMed]
- Campbell, S.B.; Shaw, D.S.; Gilliom, M. Early externalizing behavior problems: Toddlers and preschoolers at risk for later maladjustment. Dev. Psychopathol. 2000, 12, 467–488. [Google Scholar] [CrossRef] [PubMed]
- Eisenberg, N.; Cumberland, A.; Spinrad, T.L.; Fabes, R.A.; Shepard, S.A.; Reiser, M.; Murphy, B.C.; Losoya, S.H.; Guthrie, I.K. The relations of regulation and emotionality to children’s externalizing and internalizing problem behavior. Child Dev. 2001, 72, 1112–1134. [Google Scholar] [CrossRef] [PubMed]
- Liu, J. Childhood externalizing behavior: Theory and implications. J. Child Adolesc. Psychiatr. Nurs. 2004, 17, 93–103. [Google Scholar] [CrossRef] [PubMed]
- Hinshaw, S.P. On the distinction between attentional deficits/hyperactivity and conduct problems/aggression in child psychopathology. Psychol. Bull. 1987, 101, 443–463. [Google Scholar] [CrossRef] [PubMed]
- De Cock, M.; de Boer, M.R.; Lamoree, M.; Legler, J.; van de Bor, M. First year growth in relation to prenatal exposure to endocrine disruptors—A Dutch prospective cohort study. Int. J. Environ. Res. Public Health 2014, 11, 7001–7021. [Google Scholar] [CrossRef] [PubMed]
- De Cock, M.; de Boer, M.R.; Lamoree, M.; Legler, J.; van de Bor, M. Prenatal exposure to endocrine disrupting chemicals in relation to thyroid hormone levels in infants—A Dutch prospective cohort study. Environ. Health 2014, 13, 106. [Google Scholar] [CrossRef] [PubMed]
- Achenbach, T.M.; Rescorla, L.A. Manual for the ASEBA Preschool Forms and Profiles; University of Vermont Department of Psychiatry: Burlington, VT, USA, 2000. [Google Scholar]
- Linnet, K.M.; Dalsgaard, S.; Obel, C.; Wisborg, K.; Henriksen, T.B.; Rodriguez, A.; Kotimaa, A.; Moilanen, I.; Thomsen, P.H.; Olsen, J.; et al. Maternal lifestyle factors in pregnancy risk of attention deficit hyperactivity disorder and associated behaviors: Review of the current evidence. Am. J. Psychiatry 2003, 160, 1028–1040. [Google Scholar] [CrossRef] [PubMed]
- Mick, E.; Biederman, J.; Faraone, S.V.; Sayer, J.; Kleinman, S. Case-control study of attention-deficit hyperactivity disorder and maternal smoking, alcohol use, and drug use during pregnancy. J. Am. Acad. Child Adolesc. Psychiatry 2002, 41, 378–385. [Google Scholar] [CrossRef] [PubMed]
- Silva, D.; Colvin, L.; Hagemann, E.; Bower, C. Environmental risk factors by gender associated with attention-deficit/hyperactivity disorder. Pediatrics 2014, 133, e14–e22. [Google Scholar] [CrossRef] [PubMed]
- Piper, B.J.; Corbett, S.M. Executive function profile in the offspring of women that smoked during pregnancy. Nicotine Tob. Res. 2012, 14, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Bada, H.S.; Bann, C.M.; Whitaker, T.M.; Bauer, C.R.; Shankaran, S.; Lagasse, L.; Lester, B.M.; Hammond, J.; Higgins, R. Protective factors can mitigate behavior problems after prenatal cocaine and other drug exposures. Pediatrics 2012, 130, e1479–e1488. [Google Scholar] [CrossRef] [PubMed]
- Han, J.Y.; Kwon, H.J.; Ha, M.; Paik, K.C.; Lim, M.H.; Gyu Lee, S.; Yoo, S.J.; Kim, E.J. The effects of prenatal exposure to alcohol and environmental tobacco smoke on risk for ADHD: A large population-based study. Psychiatry Res. 2015, 225, 164–168. [Google Scholar] [CrossRef] [PubMed]
- De Coster, S.; van Larebeke, N. Endocrine-disrupting chemicals: Associated disorders and mechanisms of action. J. Environ. Public Health 2012, 2012, 713696. [Google Scholar] [CrossRef] [PubMed]
- Puth, M.T.; Neuhauser, M.; Ruxton, G.D. On the variety of methods for calculating confidence intervals by bootstrapping. J. Anim. Ecol. 2015, 84, 892–897. [Google Scholar] [CrossRef] [PubMed]
- Strom, M.; Hansen, S.; Olsen, S.F.; Haug, L.S.; Rantakokko, P.; Kiviranta, H.; Halldorsson, T.I. Persistent organic pollutants measured in maternal serum and offspring neurodevelopmental outcomes—A prospective study with long-term follow-up. Environ. Int. 2014, 68, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Govarts, E.; Nieuwenhuijsen, M.; Schoeters, G.; Ballester, F.; Bloemen, K.; de Boer, M.; Chevrier, C.; Eggesbø, M.; Guxens, M.; Krämer, U.; et al. Birth weight and prenatal exposure to polychlorinated biphenyls (PCBs) and dichlorodiphenyldichloroethylene (DDE): A meta-analysis within 12 European Birth Cohorts. Environ. Health Perspect. 2012, 120, 162–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.J.; Kim, M.K.; Bae, J.; Yang, J.H. Concentrations of perfluoroalkyl compounds in maternal and umbilical cord sera and birth outcomes in Korea. Chemosphere 2013, 90, 1603–1609. [Google Scholar] [CrossRef] [PubMed]
- Manzano-Salgado, C.B.; Casas, M.; Lopez-Espinosa, M.J.; Ballester, F.; Basterrechea, M.; Grimalt, J.O.; Jiménez, A.M.; Kraus, T.; Schettgen, T.; Sunyer, J.; et al. Transfer of perfluoroalkyl substances from mother to fetus in a Spanish birth cohort. Environ. Res. 2015, 142, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Liew, Z.; Ritz, B.; von Ehrenstein, O.S.; Bech, B.H.; Nohr, E.A.; Fei, C.; Bossi, R.; Henriksen, T.B.; Bonefeld-Jørgensen, E.C.; Olsen, J. Attention deficit/hyperactivity disorder and childhood autism in association with prenatal exposure to perfluoroalkyl substances: A nested case-control study in the Danish National Birth Cohort. Environ. Health Perspect. 2015, 123, 367–373. [Google Scholar] [CrossRef] [PubMed]
- Ode, A.; Källén, K.; Gustafsson, P.; Rylander, L.; Jönsson, B.A.; Olofsson, P.; Ivarsson, S.A.; Lindh, C.H.; Rignell-Hydbom, A. Fetal exposure to perfluorinated compounds and attention deficit hyperactivity disorder in childhood. PLoS ONE 2014, 9, e95891. [Google Scholar] [CrossRef] [PubMed]
- Braun, J.M.; Kalkbrenner, A.E.; Just, A.C.; Yolton, K.; Calafat, A.M.; Sjödin, A.; Hauser, R.; Webster, G.M.; Chen, A.; Lanphear, B.P. Gestational exposure to endocrine-disrupting chemicals and reciprocal social, repetitive, and stereotypic behaviors in 4- and 5-year-old children: The HOME study. Environ. Health Perspect. 2014, 122, 513–520. [Google Scholar] [CrossRef] [PubMed]
- Fei, C.; Olsen, J. Prenatal exposure to perfluorinated chemicals and behavioral or coordination problems at age 7 years. Environ. Health Perspect. 2011, 119, 573–578. [Google Scholar] [CrossRef] [PubMed]
- Fei, C.; McLaughlin, J.K.; Lipworth, L.; Olsen, J. Prenatal exposure to perfluorooctanoate (PFOA) and perfluorooctanesulfonate (PFOS) and maternally reported developmental milestones in infancy. Environ. Health Perspect. 2008, 116, 1391–1395. [Google Scholar] [CrossRef] [PubMed]
- Stein, C.R.; Savitz, D.A.; Bellinger, D.C. Perfluorooctanoate and neuropsychological outcomes in children. Epidemiology 2013, 24, 590–599. [Google Scholar] [CrossRef] [PubMed]
- Power, M.C.; Webster, T.F.; Baccarelli, A.A.; Weisskopf, M.G. Cross-sectional association between polyfluoroalkyl chemicals and cognitive limitation in the National Health and Nutrition Examination Survey. Neuroepidemiology 2013, 40, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Ankley, G.T.; Bennett, R.S.; Erickson, R.J.; Hoff, D.J.; Hornung, M.W.; Johnson, R.D.; Mount, D.R.; Nichols, J.W.; Russom, C.L.; Schmieder, P.K.; et al. Adverse outcome pathways: A conceptual framework to support ecotoxicology research and risk assessment. Environ. Toxicol. Chem. 2010, 29, 730–741. [Google Scholar] [CrossRef] [PubMed]
- Vanden Heuvel, J.P.; Thompson, J.T.; Frame, S.R.; Gillies, P.J. Differential activation of nuclear receptors by perfluorinated fatty acid analogs and natural fatty acids: A comparison of human, mouse, and rat peroxisome proliferator-activated receptor-alpha, -beta, and -gamma, liver X receptor-beta, and retinoid X receptor-alpha. Toxicol. Sci. 2006, 92, 476–489. [Google Scholar] [PubMed]
- Kapadia, R.; Yi, J.H.; Vemuganti, R. Mechanisms of anti-inflammatory and neuroprotective actions of PPAR-gamma agonists. Front. Biosci. 2008, 13, 1813–1826. [Google Scholar] [CrossRef] [PubMed]
- Tureyen, K.; Kapadia, R.; Bowen, K.K.; Satriotomo, I.; Liang, J.; Feinstein, D.L.; Vemuganti, R. Peroxisome proliferator-activated receptor-gamma agonists induce neuroprotection following transient focal ischemia in normotensive, normoglycemic as well as hypertensive and type-2 diabetic rodents. J. Neurochem. 2007, 101, 41–56. [Google Scholar] [CrossRef] [PubMed]
- Collino, M.; Aragno, M.; Mastrocola, R.; Benetti, E.; Gallicchio, M.; Dianzani, C.; Danni, O.; Thiemermann, C.; Fantozzi, R. Oxidative stress and inflammatory response evoked by transient cerebral ischemia/reperfusion: Effects of the PPAR-alpha agonist WY14643. Free Radic. Biol. Med. 2006, 41, 579–589. [Google Scholar] [CrossRef] [PubMed]
- Grandjean, P.; Andersen, E.W.; Budtz-Jørgensen, E.; Nielsen, F.; Mølbak, K.; Weihe, P.; Heilmann, C. Serum vaccine antibody concentrations in children exposed to perfluorinated compounds. JAMA 2012, 307, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Steenland, K.; Fletcher, T.; Savitz, D.A. Epidemiologic evidence on the health effects of perfluorooctanoic acid (PFOA). Environ. Health Perspect. 2010, 118, 1100–1108. [Google Scholar] [CrossRef] [PubMed]
- Corsini, E.; Avogadro, A.; Galbiati, V.; dell’Agli, M.; Marinovich, M.; Galli, C.L.; Germolec, D.R. In vitro evaluation of the immunotoxic potential of perfluorinated compounds (PFCs). Toxicol. Appl. Pharmacol. 2011, 250, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Wang, I.J.; Hsieh, W.S.; Chen, C.Y.; Fletcher, T.; Lien, G.W.; Chiang, H.L.; Chiang, C.F.; Wu, T.N.; Chen, P.C. The effect of prenatal perfluorinated chemicals exposures on pediatric atopy. Environ. Res. 2011, 111, 785–791. [Google Scholar] [CrossRef] [PubMed]
- Weiss, B. Same sex, no sex, and unaware sex in neurotoxicology. Neurotoxicology 2011, 32, 509–517. [Google Scholar] [CrossRef] [PubMed]
- Sagiv, S.K.; Thurston, S.W.; Bellinger, D.C.; Altshul, L.M.; Korrick, S.A. Neuropsychological measures of attention and impulse control among 8-year-old children exposed prenatally to organochlorines. Environ. Health Perspect. 2012, 120, 904–909. [Google Scholar] [CrossRef] [PubMed]
- Vested, A.; Ramlau-Hansen, C.H.; Olsen, S.F.; Bonde, J.P.; Kristensen, S.L.; Halldorsson, T.I.; Becher, G.; Haug, L.S.; Ernst, E.H.; Toft, G. Associations of in utero exposure to perfluorinated alkyl acids with human semen quality and reproductive hormones in adult men. Environ. Health Perspect. 2013, 121, 453–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lau, C.; Anitole, K.; Hodes, C.; Lai, D.; Pfahles-Hutchens, A.; Seed, J. Perfluoroalkyl acids: A review of monitoring and toxicological findings. Toxicol. Sci. 2007, 99, 366–394. [Google Scholar] [CrossRef] [PubMed]
- Seegal, R.F.; Marek, K.L.; Seibyl, J.P.; Jennings, D.L.; Molho, E.S.; Higgins, D.S.; Factor, S.A.; Fitzgerald, E.F.; Hills, E.A.; Korrick, S.A. Occupational exposure to PCBs reduces striatal dopamine transporter densities only in women: A beta-CIT imaging study. Neurobiol. Dis. 2010, 38, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Vahter, M.; Akesson, A.; Lidén, C.; Ceccatelli, S.; Berglund, M. Gender differences in the disposition and toxicity of metals. Environ. Res. 2007, 104, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Skovgaard, A.M.; Houmann, T.; Landorph, S.L.; Christiansen, E. Assessment and classification of psychopathology in epidemiological research of children 0–3 years of age: A review of the literature. Eur. Child Adolesc. Psychiatry 2004, 13, 337–346. [Google Scholar] [CrossRef] [PubMed]
- Melzer, D.; Rice, N.; Depledge, M.H.; Henley, W.E.; Galloway, T.S. Association between serum perfluorooctanoic acid (PFOA) and thyroid disease in the U.S. National Health and Nutrition Examination Survey. Environ. Health Perspect. 2010, 118, 686–692. [Google Scholar] [CrossRef] [PubMed]
- Calafat, A.M.; Kuklenyik, Z.; Reidy, J.A.; Caudill, S.P.; Tully, J.S.; Needham, L.L. Serum Concentrations of 11 Polyfluoroalkyl Compounds in the U.S. Population: Data from the National Health and Nutrition Examination Survey (NHANES) 1999–2000. Environ. Sci. Technol. 2007, 41, 2237–2242. [Google Scholar] [PubMed]
- Calafat, A.M.; Wong, L.Y.; Kuklenyik, Z.; Reidy, J.A.; Needham, L.L. Polyfluoroalkyl chemicals in the U.S. population: Data from the National Health and Nutrition Examination Survey (NHANES) 2003–2004 and comparisons with NHANES 1999–2000. Environ. Health Perspect. 2007, 115, 1596–1602. [Google Scholar] [CrossRef] [PubMed]



| Compound | N | Unit of Conc. | Mean (SD) | Median | Range | LOQ | <LOQ (%) |
|---|---|---|---|---|---|---|---|
| PFOA | 59 | ng/L | 905.6 (437.1) | 870.0 | 200–2300 | 50–140 | 0 |
| 59 | nM | 2.19 (1.06) | 2.10 | 0.48–5.55 | 0.12–0.34 | 0 | |
| PFOS | 59 | ng/L | 1583.6 (648.3) | 1600.0 | 570–3200 | 44–140 | 0 |
| 59 | nM | 3.17 (1.30) | 3.21 | 1.14–6.41 | 0.09–0.28 | 0 | |
| PFHxS | 59 | ng/L | 140.0 (69.2) | 145.0 | 36.0–260.0 | 47–100 | 1 |
| 59 | nM | 0.41 (0.19) | 0.38 | 0.06–1.00 | 0.09–0.25 | 1 | |
| PFHpS | 59 | ng/L | 35.6 (21.3) | 32.0 | 5.10–120.0 | 3.7–8.2 | 0 |
| 59 | nM | 0.08 (0.05) | 0.07 | 0.01–0.27 | 0.09–0.02 | 0 | |
| PFNA | 59 | ng/L | 140.0 (61.8) | 140.0 | 60.0–440.0 | 19–42 | 0 |
| 59 | nM | 0.32 (0.13) | 0.30 | 0.13–0.95 | 0.03–0.09 | 0 | |
| PFDA | 59 | ng/L | 52.2 (20.9) | 46.0 | 23.0–130.0 | 11–28 | 0 |
| 59 | nM | 0.10 (0.04) | 0.09 | 0.04–0.25 | 0.02–0.05 | 0 | |
| PFUnDA | 59 | ng/L | 32.05 (11.9) | 27.5 | 22.0–67.0 | 130–290 | 1 |
| 59 | nM | 0.03 (0.02) | 0.02 | 0.01–0.12 | 0.03–0.07 | 1 | |
| Sum PFASs | 59 | ng/L | 2907.0 (1051.5) | 2907.0 | 982–5969 | 165–404 | 0 |
| 59 | nM | 6.30 (2.29) | 6.24 | 2.08–13.12 | 0.37–1.01 | 0 |
| Characteristic | Whole Sample (N = 57–59) | Boys (N = 34–38) | Girls (N = 20–21) | |||
|---|---|---|---|---|---|---|
| Range | Range | Range | ||||
| Gestational age in weeks (mean, SD) | 40.0 (1.1) | 36.6–42.0 | 39.9 (1.2) | 37.2–41.6 | 40.1 (1.1) | 36.6–42.0 |
| Age mother in years (mean, SD) | 31.3 (3.8) | 23.0–40.0 | 30.9 (3.8) | 24.0–40.0 | 32.1 (3.6) | 23.0–36.0 |
| Educational level (high, %) | 43 (74.1) | - | 29 (78.4) | - | 14 (66.7) | - |
| Smoking pregnancy (yes, %) | 3 (5.3) | - | 2 (5.6) | - | 1 (4.8) | - |
| Alcohol use pregnancy (yes, %) | 6 (10.3) | - | 4 (10.5) | - | 2 (10.0) | - |
| Illicit drug use pregnancy (yes, %) | 0 (0) | - | 0 (0.0) | - | 0 (0.0) | - |
| Family history ADHD (yes, %) | 8 (14.3) | - | 6 (16.7) | - | 2 (10.0) | - |
| ADHD score (mean, SD) | 3.6 (1.9) | 0–8 | 3.3 (1.8) | 0–7 | 3.6 (1.5) | 1–7 |
| Externalizing behavior score (mean, SD) | 9.7 (5.7) | 1–24 | 9.2 (6.0) | 1–22 | 9.6 (4.7) | 1–19 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quaak, I.; De Cock, M.; De Boer, M.; Lamoree, M.; Leonards, P.; Van de Bor, M. Prenatal Exposure to Perfluoroalkyl Substances and Behavioral Development in Children. Int. J. Environ. Res. Public Health 2016, 13, 511. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13050511
Quaak I, De Cock M, De Boer M, Lamoree M, Leonards P, Van de Bor M. Prenatal Exposure to Perfluoroalkyl Substances and Behavioral Development in Children. International Journal of Environmental Research and Public Health. 2016; 13(5):511. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13050511
Chicago/Turabian StyleQuaak, Ilona, Marijke De Cock, Michiel De Boer, Marja Lamoree, Pim Leonards, and Margot Van de Bor. 2016. "Prenatal Exposure to Perfluoroalkyl Substances and Behavioral Development in Children" International Journal of Environmental Research and Public Health 13, no. 5: 511. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13050511