1. Introduction
Studded tires wear the asphalt surface and contribute to particle matter (PM), specifically the coarse fraction PM
coarse between 2.5–10 microns in aerodynamic diameter (PM
2.5–10). Short-term exposure to PM attributed to mechanical wear has been associated with emergency room visits for asthma [
1] and increased mortality [
2]. Stronger effects of short-term exposure to coarse particles PM
2.5–10 were found on respiratory outcomes as asthma admissions compared to other endpoints [
3] and increased respiratory morbidity and mortality in relation to higher short-term PM
2.5–10 concentrations [
4]. However, the findings have been heterogeneous and stronger associations have been reported from arid regions [
3] and in European studies [
4].
Nitric oxide (NO) is a signalling molecule produced by epithelial cells in the airways. In airway inflammation the fraction of exhaled nitric oxide (FENO) is increased [
5]. Increased levels of FENO have also been shown to predict new-onset asthma in children [
6] and new-onset wheeze in adults [
7]. It has also been suggested to be a predictor for asthma in children with virus-induced wheeze [
8]. Taken together, these data indicate that FENO is a relevant biomarker to assess early sub-clinical inflammation, as elevated FENO levels are present before the onset of symptoms.
In northern Sweden, the exposure to coarse particles is unusually high during April and May when streets and highways are cleared from sand and particles produced by wintertime driving with studded tires and the sanding of roads from October, resulting in lots of wear particles which are present until the roads are cleaned in late spring. This is therefore an ideal time point to better elucidate the effect of coarse particles. We were especially interested in the effect of exposure in children, as they are potentially more vulnerable.
FENO has been used in children to assess the effects of traffic exposure in several studies; exposure to black carbon and PM
2.5 has been associated with increases in FENO in both healthy [
9,
10] and asthmatic subjects [
11]. In children, PM
2.5 was associated with elevated FENO in both healthy [
12] and allergic children [
13]. PM
10 from traffic as well as biomass burning has also been associated with increased FENO in healthy children [
14,
15] as well in a panel of urban- and suburban-dwelling children [
16], and with PM
coarse in asthmatic children [
17]; however, the study was smaller (
n = 58) and the setting radically different. A European study found associations between background exposure to PM
coarse and increased risk of pneumonia in children at ages two to three [
18], whereas no assocation was found with lung funtion in children in another study [
19]. The role of PM
coarse from studded tires on airway inflammation in healthy children has not been investigated.
The aim of this study was to investigate if there was an association between airway inflammation (FENO50) and PMcoarse in a northern Swedish town in healthy children.
2. Materials and Methods
2.1. Study Population
The study population was sampled from grades 4, 5 and 6 (age 11–12) in two different schools in Umeå, Västerbotten, Sweden. The study participants were recruited from classes which had schedules compatible with the clinical research staff’s. All eligible children were invited to participate through a letter to their parents, who gave informed consent for the participation. The study protocol was approved by the regional ethical review board (reference number: 2010-345-31M).
2.2. Exposure
The children’s air pollution exposure at school was estimated based on data from measuring stations located within 1500 m of the schools. PM10 and PM2.5 and ozone (O3) were measured at the Mården continuous measuring station using a TEOM instrument (Monitor Europe 9810, Casella Measurement, Bedford, UK) for PM. Coarse particles, PMcoarse, were defined as the fraction between PM2.5 from PM10 and calculated by subtracting PM2.5 from PM10. Nitrogen dioxide (NO2), nitrogen oxides (NOx), and nitrogen oxide (NO) was measured at Västra Esplanaden measuring station using a chemilluminiscence instrument (ML 9841 B, Teledyne Monitor Labs, Englewood, CO, USA). Temperature was measured at Umeå airport, approximately 5 km away from the schools, and provided as 30 minute means and recalculated into daily means when 75% of the data were available; otherwise, it was coded as missing. Pollen was measured as daily birch pollen using a Burkard trap at the roof the University Hospital. Pollen counts were recoded into categories from the daily value (0 = 0, 1–10 = 1, 11–100 = 2, 101–1000 = 3).
2.3. FENO Measurements
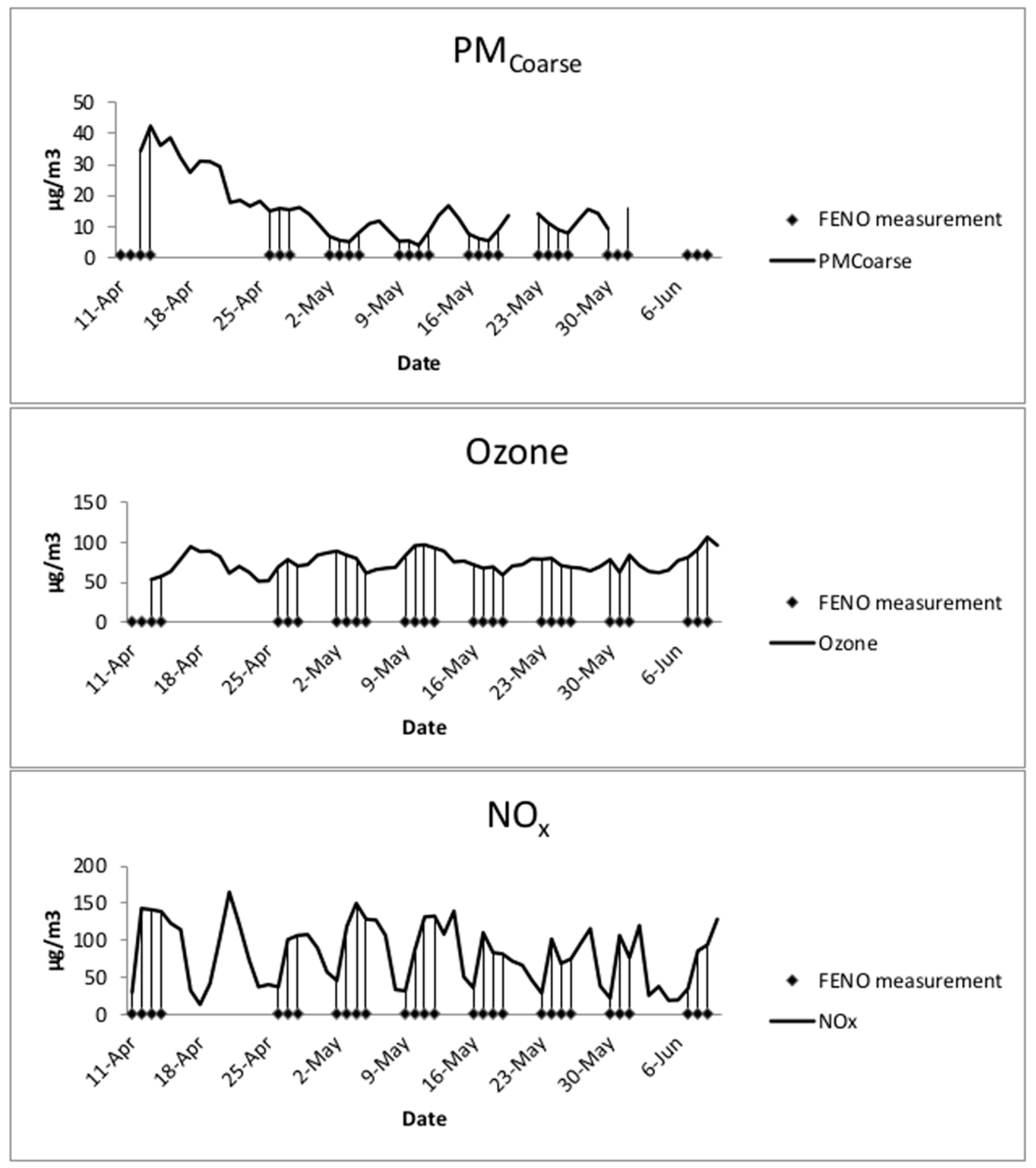
FENO measurements were performed on each participant twice each week during spring 2011 (11 April to 6 June) if the child was present and did not have respiratory symptoms.
Fraction of exhaled nitric oxide was measured at the flow rate 50 mL/s (FENO50) using Niox Mino (Aerocrine AB, Solna, Sweden). One measurement was performed at each occasion, according to the manufacturer’s instructions. The parents of the participants answered questionnaires about respiratory health, use of asthma medication, and rhinitis (allergies to furred animals and pollen). At each measuring occasion, children were asked about cold symptoms. If possible the measurements were performed at the same hour on each occasion.
If the FENO value was less than 5 ppb (n = 32), i.e., the lower limit of the measurement device, it was set to 2.5 ppb. As FENO is skewed to the right, log transformed values were used in the model, the estimate was then log-transformed back after the modelling.
2.4. Statistical Methods
Cumulative means of pollution exposure 24, 48 and 72 h prior to the FENO measurement were calculated and used in the model. Same-day temperature and pollen counts were included in the model. In the statistical analysis, MLR (multiple linear regression) was used to examine personal covariates related to FENO as a first step. If the p-value was <0.25 for a variable, it was included in the initial models. Then the personal covariates of interest, sex, allergy, pollen, day of week and meteorological variables, were included in the linear mixed models, together with the pollutants, to examine if the pollutants had any effect on FENO. Subjects were included as a random effect to account for personal differences, and all other variables were included as fixed effects.
First each pollutant’s effect on FENO was examined individually in single-pollutant models. Since PM mass and nitrogen oxides (reflecting vehicle exhaust) were represented by several variables, the multi-pollutant models were constructed for each pairwise combination of PM2.5 and PMcoarse and NO, NO2 and NOx which were included in the multi-pollutant models with O3. Each pollutant’s effect on FENO was examined with exposure windows of 24, 48 and 72 h. If a covariate changed any pollutants’ effect on FENO by more than 10% or lowered Akaike’s information criteria (AIC) it was considered to be an effect modifier and was included in the model. Model selection was based on minimizing AIC.
Sensitivity analysis of sex, allergy status and background residential exposure by quartile of modeled annual mean NOx exposure at each participant’s home address was performed.
The results are reported as change FENO (ppb) per interquartile range (IQR) of the pollutants with a 95% confidence interval (CI). All statistical analysis was performed using PASW 18 (SPSS, Chicago, IL, USA).
4. Discussion
In this panel study of repeated FENO measurements in 95 schoolchildren over two months, we found significant within-individual increases of FENO after exposure to PMcoarse during the previous 24 h and NO2 during the previous 72 h in models adjusted for other pollutants. Exposure to O3, on the other hand, was associated with decreased FENO levels after adjusting for other pollutants. The results indicate that PMcoarse, derived mainly from mechanical wear, can induce sub-clinical airway inflammation in healthy children, and it would appear that exposure 24 h before the clinical examination is most relevant. This could be due to very low background levels of PM, so even moderate exposure levels affect FENO in the study group.
FENO is mainly associated with T-helper cell type 2 (Th2) driven airway inflammation, where an increase in airway eosinophils is a major characteristic even if the association between FENO and eosinophils is not very strong [
20,
21]. It seems likely that eosinophils in induced sputum and FENO reflect parallel processes in the inflamed airways. Traffic exposure, on the other hand, is merely inducing neutrophilic inflammation [
22]. Nevertheless, FENO has been shown to be elevated in children with asthma living close to major roads [
23], as well as after ozone exposure [
24,
25], and hence seems a biomarker of interest. In the current study, children with colds were excluded; nevertheless, the maximum FENO value was 71 ppb, but FENO has high variability.
PM
coarse is a general problem in cities in northern Sweden where sand and studded tires are used to increase driving safety on icy roads. The entire road network is an important source of PM
coarse in winter and spring, especially during periods of dry and windy weather where the European 24 h air quality guideline values are exceeded in the central part of Umeå, the current study setting [
26]. However, regional background levels of PM are very low, which is why small absolute concentration changes present as large relative changes. Newly and locally generated particles thus become a larger fraction of PM in urban settings where most central monitors are located. Previous reports of health effects from coarse PM in urban settings could be due to variation in regional background PM (e.g., desert dust) which is reflected in concentrations measured at a single monitor rather than variation from nearby local sources, e.g., a construction site.
A possible limitation of the current study is assigning exposure from a single, central monitor which limits the available outcome. The monitors are located near the schools, but the children’s residence may not be very close and other daytime activities may modify the children’s daily exposure. However, assigning PM
coarse exposure from a single, central monitor is considered to be representative for large urban areas, especially in studies of temporal variation [
27]. Several studies have determined that there is a high correlation between personal exposure in children and exposure from central monitors in children and that classroom PM
10 exposure was highly correlated with these metrics [
28], and similar trends have been found for smaller particles in studies of the relationship between ambient and classroom measures [
29].
For NO2, which increases during stagnation and cold temperatures, the cumulative 72 h exposure in models adjusted for PMcoarse and O3 yielded a higher effect estimate than at shorter lags.
Twenty-four-hour O
3 levels were associated with reduced FENO in the multi-pollutant models. O
3 levels correlated with levels of PM
2.5 and temperature, but no other pollutants. O
3 levels in this region are positively correlated with temperature. During stagnation O
3 levels fall as nitrogen species build up. This happens especially in places where NOx levels are dominated by local sources due to a high NO/NO
2 ratio from NO from local exhaust emissions. Higher O
3 levels could indicate lower levels of exhaust components that are not measured such as ultrafine particles and aldehydes. This result is in contrast with results from other studies in settings with shorter exposure windows and higher O
3 levels [
24]; however, the exposure time window was different and O
3 levels were lower in the current study. In previous studies FENO levels were positively associated with mean O
3 levels of the previous eight hours in healthy children [
24,
25], and with those of the previous day in asthmatics [
30]. Other epidemiological studies in adults have found associations between five-day cumulative O
3 exposure levels and increased inflammation in the distal airways (FENO
270), but at shorter lags, the association was not significant [
31]. However, our effect estimates are similar to those reported in asthmatic children [
32], where same-day and two-day average O
3 levels were associated with significant decreases in FENO
50. Other studies found no association between O
3 and FENO
50 in healthy children [
12], and chamber studies of healthy adults also found no association with exposure to O
3 [
33]. A possible explanatory factor for this unexpected protective effect of O
3 could be related to behaviour, as O
3 levels tend to be higher during meteorological conditions with little wind, sun and relative warmth which could prompt people to spend more time outdoors and be physically active. Physical exercise was associated with lower FENO in adults even in settings with high exposure to traffic-related air pollutants [
34]. The present study has a strong advantage to assess the effects as the study design, where both exposure and FENO were measured over a two-month period, allowing for effect estimates based on within-individual variation independent of variation between different schools or class rooms.
Most previous studies were cross-sectional or cohort studies which evaluated the effects of chronic exposures. The exceptions are the studies of children in summer camps [
24,
25] where repeated FENO measurements were associated with eight-hour O
3 means. Sarnat and colleagues [
17] measured FENO in a panel of school children for 16 weeks and found that particle matter from traffic and other sources, rather than NO
2, was associated with FENO. Greenwald and colleagues [
35] measured FENO in a panel of elementary school students were measured weekly for 13 weeks to estimate the effects of exposure to diesel truck traffic, but no association was found in healthy children. Koenig and colleagues [
36] measured children for 10 days while monitoring indoor and outdoor PM
2.5. Steerenberg and colleagues [
16] measured FENO and several other biomarkers in children in an urban school and a suburban school weekly and found associations with black smoke, PM
10, NO, and NO
2.
PM
coarse originating from biomass has been associated with same-day increased FENO in children [
15] but the effect estimates were lower than for the current study. However, in a study of same-day PM
10, NO
2 and black smoke [
37], much higher effect estimates were found for PM
10 than in the current study. Barraza-Villarreal and colleagues [
11] reported that eight-hour exposure to PM
2.5, NO
2 and O
3 was associated with increased FENO in healthy subjects by 1.16 ppb per IQR (17.5 µg/m
3) PM
2.5. However, the study set in Mexico City experienced much higher levels of PM
2.5 and NO
2 , and lower levels of O
3. Other studies found no association between exhaled NO in healthy children and two-week NO
2 or 48 h PM
2.5 and elemental carbon measured at the school [
38].
Long-term exposure to PM
coarse at the residence was not associated with FENO in 9–11 year-old children [
39]. In a study of oxidative stress and airway inflammation in children, black carbon (BC) from combustion sources was associated with same-day measures of oxidative stress whereas 24 h and weekly exposure was associated with airway inflammation measured by FENO [
9], so our observation could be due to the involvement of different mechanisms.
Finally, other factors affect FENO levels, e.g., gene-environment interactions, which have been described for the association between FENO
50 and fine PM
2.5 [
40]. Among atopic rather than non-atopic children, associations between FENO and exposure to pollen [
13] and PM
2.5 have been found [
10,
11]. In our study, allergies were not a significant predictor of FENO and did not improve the model fit, and were thus discarded from the models. However, the current study setting had low levels of pollution, and the pollen levels were unusually low during the study period with a maximum 24 h mean concentration of 117 grains per m
3.
As the few asthmatic children in the recruited population were all treated with anti-inflammatory medication that may attenuate FENO response [
35], these children were excluded from the study population. Some children with rhinitis were, however, included, and we lack the information about the daily use of nasal steroids, but this seems unlikely to confound the results as we studied the effects of short-term fluctuations in air pollution.The lack of information about daily use of medication against rhinitis is not likely to be a confounding problem as we study short-term effects of fluctuations in air pollution.
Participation was dependent on parental consent, but it is unlikely that this would influence the result as all analysed children were healthy. Also, we lack information on time spent outdoors and physical exercise which could depend on weather conditions and influence both outdoor and indoor exposure, which could also affect FENO levels.




{kind=link}