
Shisha Smoking Practices, Use Reasons, Attitudes, Health Effects and Intentions to Quit among Shisha Smokers in Malaysia

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Respondents and Settings
2.2. Study Questionnaire
2.3. Data Analyses
2.4. Ethical Consideration
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Neergaard, J.; Singh, P.; Job, J.; Montgomery, S. Waterpipe smoking and nicotine exposure: A review of the current evidence. Nicotine Tob. Res. 2007, 9, 987–994. [Google Scholar] [CrossRef] [PubMed]
- Brockman, L.N.; Pumper, M.A.; Christakis, D.A.; Moreno, M.A. Hookah’s new popularity among U.S. college students: A pilot study of the characteristics of hookah smokers and their Facebook displays. BMJ Open 2012, 2, e001709. [Google Scholar] [CrossRef] [PubMed]
- Ramachandra, S.S.; Yaldrum, A. Shisha smoking: An emerging trend in Southeast Asian nations. J. Public Health Policy 2015, 36, 304–317. [Google Scholar] [CrossRef] [PubMed]
- Al-Naggar, R.A.; Bobryshev, Y.V. Shisha smoking and associated factors among medical students in Malaysia. Asian Pac. J. Cancer Prev. 2012, 13, 5627–5632. [Google Scholar] [CrossRef] [PubMed]
- Maziak, W.; Ward, K.D.; Eissenberg, T. Factors related to frequency of narghile (waterpipe) use: The first insights on tobacco dependence in narghile users. Drug Alcohol Depend. 2004, 76, 101–106. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Study Group on Tobacco Product Regulation (TOBREG) Geneva: Waterpipe Tobacco Smoking: Health Effects, Research Needs and Recommended Action by Regulators. 2005. Available online: http://www.who.int/tobacco/global_interaction/tobreg/Waterpipe%20recommendation_Final.pdf (accessed on 24 March 2016).
- Ward, K.D.; Eissenberg, T.; Rastam, S.; Asfar, T.; Mzayek, F.; Fouad, M.F.; Hammal, F.; Mock, J.; Maziak, W. The tobacco epidemic in Syria. Tob. Control 2006, 15, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.Y.; Curbow, B.; Stillman, F.A. Harm perception of nicotine products in college freshmen. Nicotine Tob. Res. 2007, 9, 977–982. [Google Scholar] [CrossRef] [PubMed]
- Primack, B.A.; Sidani, J.; Agarwal, A.A.; Shadel, W.G.; Donny, E.; Eissenberg, T.E. Prevalence of and associations with waterpipe tobacco smoking among U.S. university students. Ann. Behav. Med. 2008, 36, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Smith-Simone, S.; Maziak, W.; Ward, K.D.; Eissenberg, T. Waterpipe tobacco smoking: Knowledge, attitudes, beliefs, and behavior in two U.S. samples. Nicotine Tob. Res. 2008, 10, 393–398. [Google Scholar] [CrossRef] [PubMed]
- Kandela, P. Narghile smoking keeps Arabs in wonderland. Lancet 2000, 356, 1175. [Google Scholar] [CrossRef]
- Maziak, W.; Eissenberg, T.; Rastam, S.; Hammal, F.; Asfar, T.; Bachir, M.E.; Fouad, M.F.; Ward, K.D. Beliefs and attitudes related to narghile (waterpipe) smoking among university students in Syria. Ann. Epidemiol. 2004, 14, 646–654. [Google Scholar] [CrossRef] [PubMed]
- Chaouachi, K. Hookah (shisha, narghile) smoking and environmental tobacco smoke (ETS). A critical review of the relevant literature and the public health consequences. Int. J. Environ. Res. Public Health 2009, 6, 798–843. [Google Scholar] [CrossRef] [PubMed]
- Jukema, J.B.; Bagnasco, D.E.; Jukema, R.A. Waterpipe smoking: Not necessarily less hazardous than cigarette smoking. Neth. Heart J. 2014, 22, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Cobb, C.O.; Vansickel, A.R.; Blank, M.D.; Jentink, K.; Travers, M.J.; Eissenberg, T. Indoor air quality in Virginia waterpipe cafes. Tob. Control 2013, 22, 338–343. [Google Scholar] [CrossRef] [PubMed]
- Kadhum, M.; Sweidan, A.; Jaffery, A.E.; Al-Saadi, A.; Madden, B. A review of the health effects of smoking shisha. Clin. Med. 2015, 15, 263–266. [Google Scholar] [CrossRef] [PubMed]
- Chaouachi, K. A critique of the WHO TobReg’s “Advisory Note” report entitled: “Waterpipe tobacco smoking: Health effects, research needs and recommended actions by regulators”. J. Negat. Results Biomed. 2006, 5, 17. [Google Scholar] [CrossRef] [PubMed]
- Chandir, S.; Hussain, H.; Salahuddin, N.; Amir, M.; Ali, F.; Lotia, I.; Khan, A.J. Extrapulmonary tuberculosis: A retrospective review of 194 cases at a tertiary care hospital in Karachi, Pakistan. J. Pak. Med. Assoc. 2010, 60, 105–109. [Google Scholar] [PubMed]
- Tamim, H.; Terro, A.; Kassem, H.; Ghazi, A.; Khamis, T.A.; Hay, M.M.; Musharrafieh, U. Tobacco use by university students, Lebanon, 2001. Addiction 2003, 98, 933–939. [Google Scholar] [CrossRef] [PubMed]
- Aljarrah, K.; Ababneh, Z.Q.; Al-Delaimy, W.K. Perceptions of hookah smoking harmfulness: Predictors and characteristics among current hookah users. Tob. Induc. Dis. 2009, 5. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services. How Tobacco Smoke Causes Disease: The Biology and Behavioral Basis for Smoking-Attributable Disease. A Report of the Surgeon General. 2010. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK53017/pdf/Bookshelf_NBK53017.pdf (accessed on 14 March 2016). [Google Scholar]
- U.S. Department of Health and Human Services. The Health Consequences of Smoking—50 Years of Progress. A Report of the Surgeon General. 2014. Available online: http://www.surgeongeneral.gov/library/reports/50-years-of-progress/full-report.pdf (accessed on 18 March 2016). [Google Scholar]
- Combrink, A.; Irwin, N.; Laudin, G.; Naidoo, K.; Plagerson, S.; Mathee, A. High prevalence of hookah smoking among secondary school students in a disadvantaged community in Johannesburg. S. Afr. Med. J. 2010, 100, 297–299. [Google Scholar] [CrossRef] [PubMed]
- Anjum, Q.; Ahmed, F.; Ashfaq, T. Knowledge, attitude and perception of water pipe smoking (shisha) among adolescents aged 14–19 years. J. Pak. Med. Assoc. 2008, 58, 312–317. [Google Scholar] [PubMed]
- Jackson, D.; Aveyard, P. Waterpipe smoking in students: Prevalence, risk factors, symptoms of addiction, and smoke intake. Evidence from one British university. BMC Public Health 2008, 8, 174. [Google Scholar] [CrossRef] [PubMed]
- Al-Naggar, R.A.; Saghir, F.S. Water pipe (shisha) smoking and associated factors among Malaysian university students. Asian Pac. J. Cancer Prev. 2011, 12, 3041–3047. [Google Scholar] [PubMed]
- Barnett, T.E.; Smith, T.; He, Y.; Soule, E.K.; Curbow, B.A.; Tomar, S.L.; McCarty, C. Evidence of emerging hookah use among university students: A cross-sectional comparison between hookah and cigarette use. BMC Public Health 2013, 13, 302. [Google Scholar] [CrossRef] [PubMed]
- Kahr, M.K.; Padgett, S.; Shope, C.D.; Griffin, E.N.; Xie, S.S.; Gonzalez, P.J.; Levison, J.; Mastrobattista, J.; Abramovici, A.R.; Northrup, T.F.; et al. A qualitative assessment of the perceived risks of electronic cigarette and hookah use in pregnancy. BMC Public Health 2015, 15, 1273. [Google Scholar] [CrossRef] [PubMed]
- Milam, J.E. Perceived invulnerability and cigarette smoking among adolescents. Addict. Behav. 2000, 25, 71–80. [Google Scholar] [CrossRef]
- Moreira, M.T.; Smith, L.A.; Foxcroft, D. Social norms interventions to reduce alcohol misuse in university or college students. Cochrane Database Syst. Rev. 2009, 3, CD006748. [Google Scholar] [PubMed]
- Neighbors, C.; Jensen, M.; Tidwell, J.; Walter, T.; Fossos, N.; Lewis, M.A. Social-norms interventions for light and nondrinking students. Group Process. Intergroup Relat. 2011, 14, 651–669. [Google Scholar] [CrossRef]
- Karasek, D.; Ahern, J.; Galea, S. Social norms, collective efficacy, and smoking cessation in urban neighborhoods. Am. J. Public Health 2012, 102, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Aslam, H.M.; Saleem, S.; German, S.; Qureshi, W.A. Harmful effects of shisha: Literature review. Int. Arch. Med. 2014, 7. [Google Scholar] [CrossRef] [PubMed]
- Etter, J.F. Electronic cigarettes: A survey of users. BMC Public Health 2010, 10, 231. [Google Scholar] [CrossRef] [PubMed]
- Grana, R.; Benowitz, N.; Glantz, S.A. E-cigarettes: A scientific review. Circulation 2014, 129, 1972–1986. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services. Youth and Tobacco. Preventing Tobacco Use among Young People. A Report of the Surgeon General. 1994. Available online: http://profiles.nlm.nih.gov/ps/access/NNBCLQ.pdf (accessed on 21 March 2016). [Google Scholar]
- Marques-Vidal, P.; Melich-Cerveira, J.; Paccaud, F.; Waeber, G.; Vollenweider, P.; Cornuz, J. Prevalence and factors associated with difficulty and intention to quit smoking in Switzerland. BMC Public Health 2011, 11, 227. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.A.; Unger, J.B.; Ritt-Olson, A.; Palmer, P.H.; Cen, S.Y.; Gallaher, P.; Chou, C.P. Smoking prevention for ethnically diverse adolescents: 2-year outcomes of a multicultural, school-based smoking prevention curriculum in Southern California. Prev. Med. 2005, 40, 842–852. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Fang, X.; Li, X.; Stanton, B.; Lin, D. Stay away from tobacco: A pilot trial of a school-based adolescent smoking prevention program in Beijing, China. Nicotine Tob. Res. 2006, 8, 227–237. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.H.; Wu, D.M.; Lai, H.R.; Chu, N.F. The impacts of a school-wide no smoking strategy and classroom-based smoking prevention curriculum on the smoking behavior of junior high school students. Addict. Behav. 2007, 32, 2099–2107. [Google Scholar] [CrossRef] [PubMed]
- Sun, P.; Miyano, J.; Rohrbach, L.A.; Dent, C.W.; Sussman, S. Short-term effects of Project EX-4: A classroom-based smoking prevention and cessation intervention program. Addict. Behav. 2007, 32, 342–350. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Details | n (%) |
|---|---|
| (A) Socio-demographic data | |
| Age group | |
| 20 and below | 66 (13.1) |
| 21–30 years old | 317 (63.0) |
| >30 years old | 120 (23.9) |
| Gender | |
| Male | 403 (80.1) |
| Female | 100 (19.9) |
| Marital status | |
| Single | 341 (67.8) |
| Married or previously married | 162 (32.2) |
| Ethnic | |
| Malay | 377 (75.0) |
| Chinese | 67 (13.3) |
| Indian | 32 (6.4) |
| Others | 27 (5.4) |
| Highest education attainment | |
| Secondary and below | 173 (34.4) |
| Tertiary (university level) | 330 (65.6) |
| Occupation | |
| Professional & Managerial | 79 (15.7) |
| Skilled/Non-skilled worker | 226 (44.9) |
| Student | 148 (29.4) |
| Retiree | 8 (1.6) |
| Unemployed | 42 (8.3) |
| Monthly income | |
| ≤RM1000 | 169 (33.6) |
| RM1000–2000 | 120 (23.9) |
| RM2001–3000 | 124 (24.7) |
| >RM3000 | 90 (17.9) |
| (B) Shisha smoking practices | |
| Shisha Smoking status | |
| Non-regular smoker | 412 (81.9) |
| Regular smoker | 91 (18.1) |
| Duration of smoking | |
| 6 months and below | 236 (46.9) |
| >6 months to 12 months | 98 (19.5) |
| >12 months | 169 (33.6) |
| Frequency of shisha smoking in a week | |
| Once in a week or less | 302 (60.4) |
| 2–3 times a week | 201 (40.0) |
| Details | n (%) | Total Detrimental Health Effects | Binary Logistic Regression for Total Adverse Health Effects 3–9 vs. 0–2 | ||
|---|---|---|---|---|---|
| Shisha smoking practices | 0–2 | 3–9 | p-Value | OR (95% CI) | |
| (n = 282) | (n = 221) | ||||
| Shisha Smoking status | |||||
| Non-regular smoker | 412 (81.9) | 246 (59.7) | 166 (40.3) | 0.001 | Reference |
| Regular smoker | 91 (18.1) | 36 (39.6) | 55 (60.5) | 2.264 (1.424–3.601) ** | |
| Duration of smoking | |||||
| 6 months and below | 236 (46.9) | 134 (56.8) | 102 (43.2) | ||
| >6 months to 12 months | 98 (19.5) | 57 (58.2) | 41 (41.8) | 0.755 | |
| >12 months | 169 (33.6) | 91 (53.8) | 78 (46.2) | ||
| Frequency of shisha smoking in a week | |||||
| Once a week or less | 302 (60.4) | 168 (55.3) | 134 (44.4) | 0.855 | |
| 2–3 times | 201 (40.0) | 114 (56.7) | 87 (43.3) | ||
| Details | n (%) | Intention to Quit Smoking Shisha | Multiple Logistic Regression for Yes vs. No | ||
|---|---|---|---|---|---|
| (A) Socio-demographic | Yes (n = 290) | No (n = 213) | p-Value | Adjusted OR (95% CI) | |
| Age group | |||||
| 20 and below | 66 (13.1) | 46 (69.7) | 20 (30.3) | 0.058 | |
| 21–30 years old | 317 (63.0) | 172 (54.3) | 145 (45.7) | ||
| >30 years old | 120 (23.9) | 72 (60.0) | 48 (40.0) | ||
| Gender | |||||
| Male | 403 (80.1) | 249 (61.8) | 154 (38.2) | <0.001 | 1.483 (0.822–2.673) |
| Female | 100 (19.9) | 41 (41.0) | 59 (59.0) | Reference | |
| Marital status | |||||
| Single | 341 (67.8) | 202 (59.2) | 139 (40.8) | 0.334 | |
| Married or previously married | 162 (32.2) | 88 (54.3) | 74 (45.7) | ||
| Ethnic | |||||
| Malay | 377 (75.0) | 242 (64.2) | 135 (35.8) | <0.001 | 2.242 (0.828–6.069) |
| Chinese | 67 (13.3) | 21 (31.3) | 46 (68.7) | 0.653 (0.216–1.977) | |
| Indian | 32 (6.4) | 14 (43.8) | 18 (56.2) | 1.323 (0.366–4.782) | |
| Others | 27 (5.4) | 13 (48.1) | 14 (51.9) | Reference | |
| Highest educational attainment | |||||
| Secondary and below | 173 (34.4) | 113 (65.3) | 60 (34.7) | 0.013 | 0.988 (0.549–1.815) |
| Tertiary (University level) | 330 (65.6) | 177 (53.6) | 153 (46.4) | Reference | |
| Occupation | |||||
| Professional & Managerial | 79 (15.7) | 44 (55.7) | 35 (44.3) | <0.001 | |
| Skilled/Non-skilled worker | 226 (44.9) | 154 (68.1) | 72 (31.9) | 0.937 (0.343–2.560) | |
| Student | 148 (29.4) | 68 (45.9) | 80 (54.1) | 1.240 (0.506–3.038) | |
| Retiree | 8 (1.6) | 4 (50.0) | 4 (50.0) | 1.191 (0.419–3.386) | |
| Unemployed | 42 (8.3) | 20 (47.6) | 22 (52.4) | 1.036 (0.174–6.177) | |
| Monthly income | |||||
| ≤RM1000 | 169 (33.6) | 78 (46.2) | 91 (53.8) | 0.010 | 0.509 (0.211–1.224) |
| RM1000–2000 | 120 (23.9) | 79 (65.8) | 41 (34.2) | 0.812 (0.361–1.825) | |
| RM2001–3000 | 124 (24.7) | 83 (66.9) | 41 (33.1) | 1.095 (0.534–2.246) | |
| >RM3000 | 90 (17.9) | 50 (55.6) | 40 (44.4) | Reference | |
| (B) Shisha smoking practices | |||||
| Shisha Smoking status | |||||
| Non-regular smoker | 412 (81.9) | 252 (61.2) | 160 (38.8) | 0.001 | 0.963 (0.506–1.832) |
| Regular smoker | 91 (18.1) | 38 (41.8) | 53 (58.2) | Reference | |
| Duration of smoking | |||||
| 6 months and below | 236 (46.9) | 167 (70.8) | 69 (29.2) | <0.001 | 2.601 (1.475–4.584) ** |
| >6 months to 12 months | 98 (19.5) | 59 (60.2) | 39 (39.8) | 3.212 (1.651–6.248) ** | |
| >12 months | 169 (33.6) | 64 (37.9) | 105 (62.1) | Reference | |
| Frequency of shisha smoking in a week | |||||
| Once | 302 (60.4) | 200 (66.2) | 102 (33.8) | <0.001 | 1.569 (0.929–2.650) |
| 2 times and above | 201 (40.0) | 90 (44.8) | 111 (55.2) | Reference | |
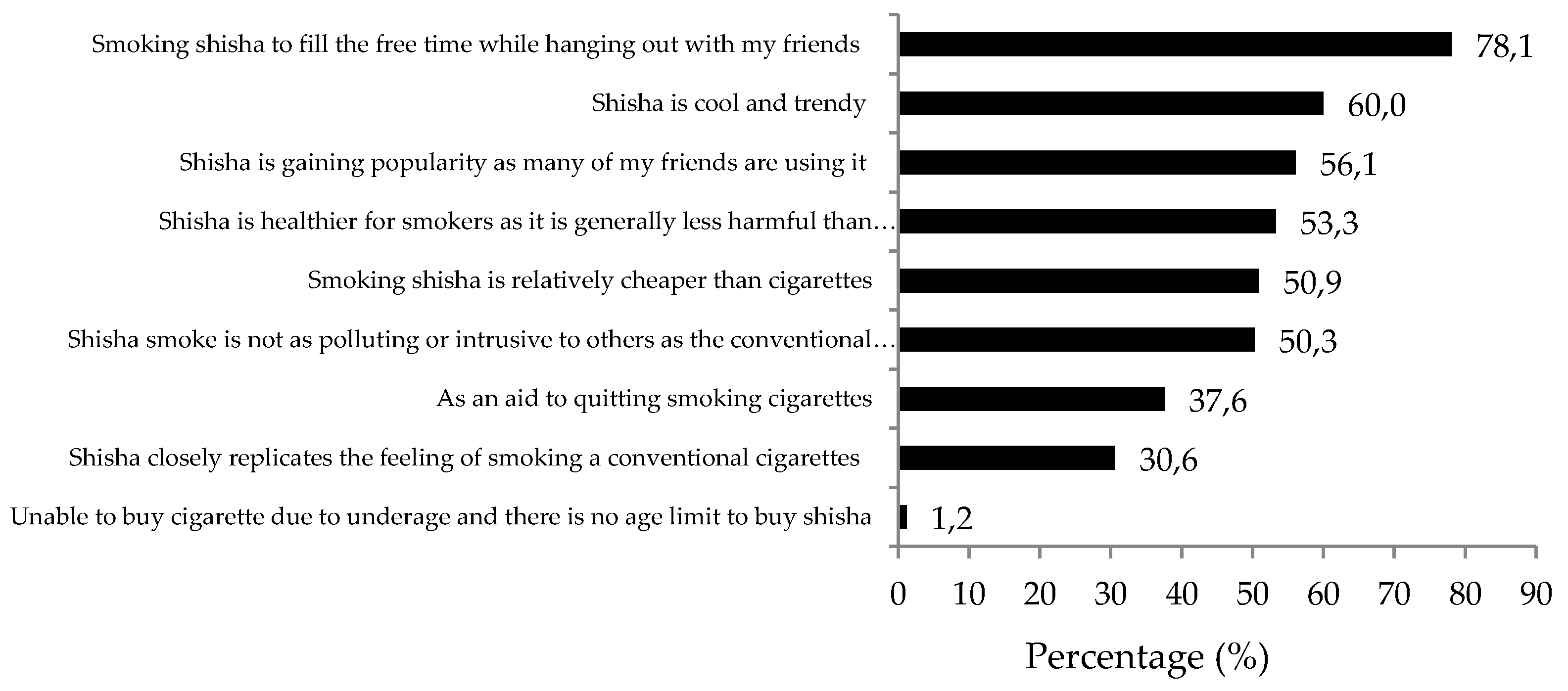
| (C) Reasons for using shisha | |||||
| Shisha is healthier for smokers as it is generally less harmful than conventional tobacco cigarettes | |||||
| Yes | 268 (53.3) | 107 (39.9) | 161 (60.1) | <0.001 | 0.384 (0.232–0.635) *** |
| No | 235 (46.7) | 183 (77.9) | 52 (22.1) | Reference | |
| Shisha smoke is not as polluting or intrusive to others as the conventional tobacco cigarette | |||||
| Yes | 253 (50.3) | 113 (44.7) | 140 (55.3) | <0.001 | 0.521 (0.317–0.858) * |
| No | 250 (49.7) | 177 (70.8) | 73 (29.2) | Reference | |
| Shisha closely replicates the feeling of smoking a conventional tobacco cigarette | |||||
| Yes | 154 (30.6) | 74 (48.1) | 80 (51.9) | 0.004 | 0.840 (0.498–1.416) |
| No | 349 (69.4) | 216 (61.9) | 133 (38.1) | Reference | |
| Unable to buy tobacco cigarettes due to being under age and there are no age limits on buying shisha | |||||
| Yes | 155 (30.8) | 104 (67.1) | 51 (32.9) | 0.005 | 2.217 (1.340–3.669) ** |
| No | 382 (69.2) | 186 (53.4) | 162 (46.6) | Reference | |
| Shisha is cool and trendy | |||||
| Yes | 302 (60.0) | 149 (49.3) | 153 (50.7) | <0.001 | 0.405 (0.244–0.672) *** |
| No | 201 (40.0) | 141 (70.1) | 60 (32.7) | Reference | |
| Shisha is gaining popularity and many of my friends are using it | |||||
| Yes | 282 (56.1) | 130 (46.1) | 152 (53.9) | <0.001 | 0.653 (0.395–1.078) |
| No | 221 (43.9) | 160 (72.4) | 61 (27.6) | Reference | |
| Smoking shisha is relatively cheaper than smoking tobacco cigarettes | |||||
| Yes | 256 (50.9) | 123 (48.0) | 133 (52.0) | <0.001 | 0.483 (0.297–0.784) ** |
| No | 247 (49.1) | 167 (67.6) | 80 (32.4) | Reference | |
| Smoke shisha to fill free time while hanging out with my friends. | |||||
| Yes | 393 (78.1) | 225 (57.3) | 168 (42.7) | 0.745 | |
| No | 110 (21.9) | 65 (59.1) | 45 (40.9) | ||
| As an aid to quitting smoking tobacco cigarettes | |||||
| Yes | 189 (37.6) | 99 (52.4) | 90 (47.6) | 0.077 | |
| No | 314 (62.4) | 191 (60.8) | 123 (39.2) | ||
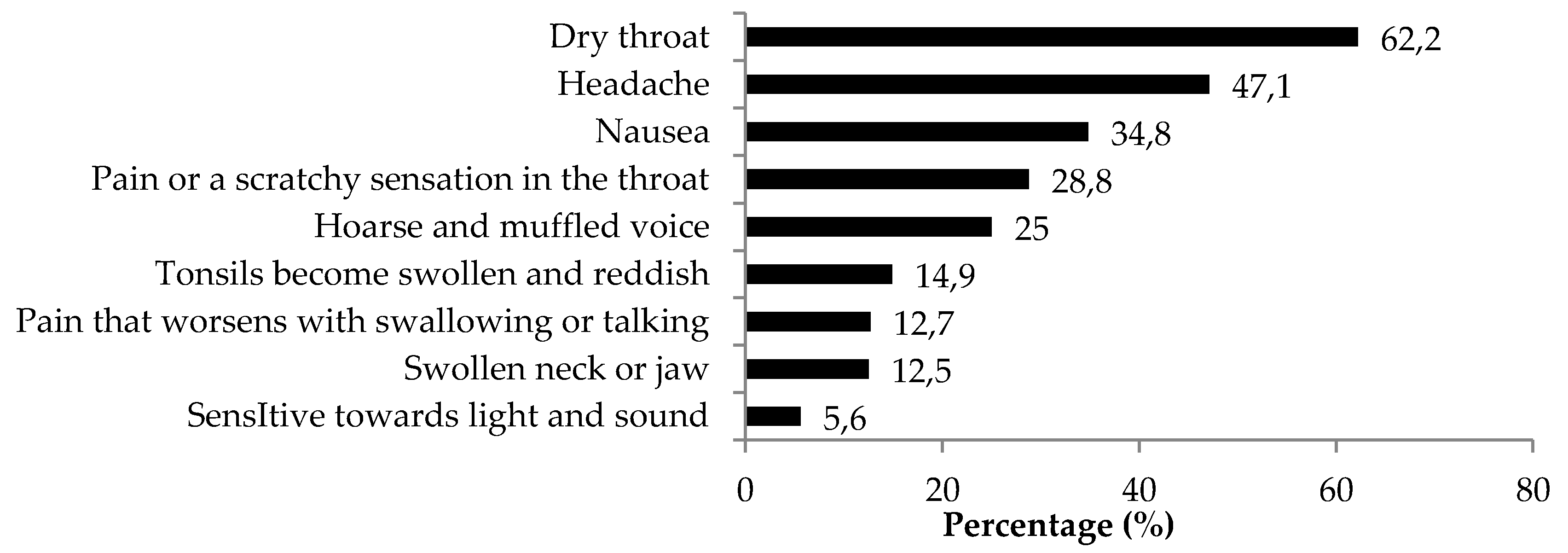
| (D) Symptoms experienced by shisha smokers | |||||
| 0–2 | 282 (56.1) | 170 (60.3) | 112 (39.7) | 0.203 | |
| 3–9 | 221 (43.9) | 120 (54.3) | 101 (45.7) | ||
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wong, L.P.; Alias, H.; Aghamohammadi, N.; Aghazadeh, S.; Hoe, V.C.W. Shisha Smoking Practices, Use Reasons, Attitudes, Health Effects and Intentions to Quit among Shisha Smokers in Malaysia. Int. J. Environ. Res. Public Health 2016, 13, 726. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13070726
Wong LP, Alias H, Aghamohammadi N, Aghazadeh S, Hoe VCW. Shisha Smoking Practices, Use Reasons, Attitudes, Health Effects and Intentions to Quit among Shisha Smokers in Malaysia. International Journal of Environmental Research and Public Health. 2016; 13(7):726. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13070726
Chicago/Turabian StyleWong, Li Ping, Haridah Alias, Nasrin Aghamohammadi, Sima Aghazadeh, and Victor Chee Wai Hoe. 2016. "Shisha Smoking Practices, Use Reasons, Attitudes, Health Effects and Intentions to Quit among Shisha Smokers in Malaysia" International Journal of Environmental Research and Public Health 13, no. 7: 726. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13070726