
The Effects of Intensive Nutrition Education on Late Middle-Aged Adults with Type 2 Diabetes


 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Ethics Statement
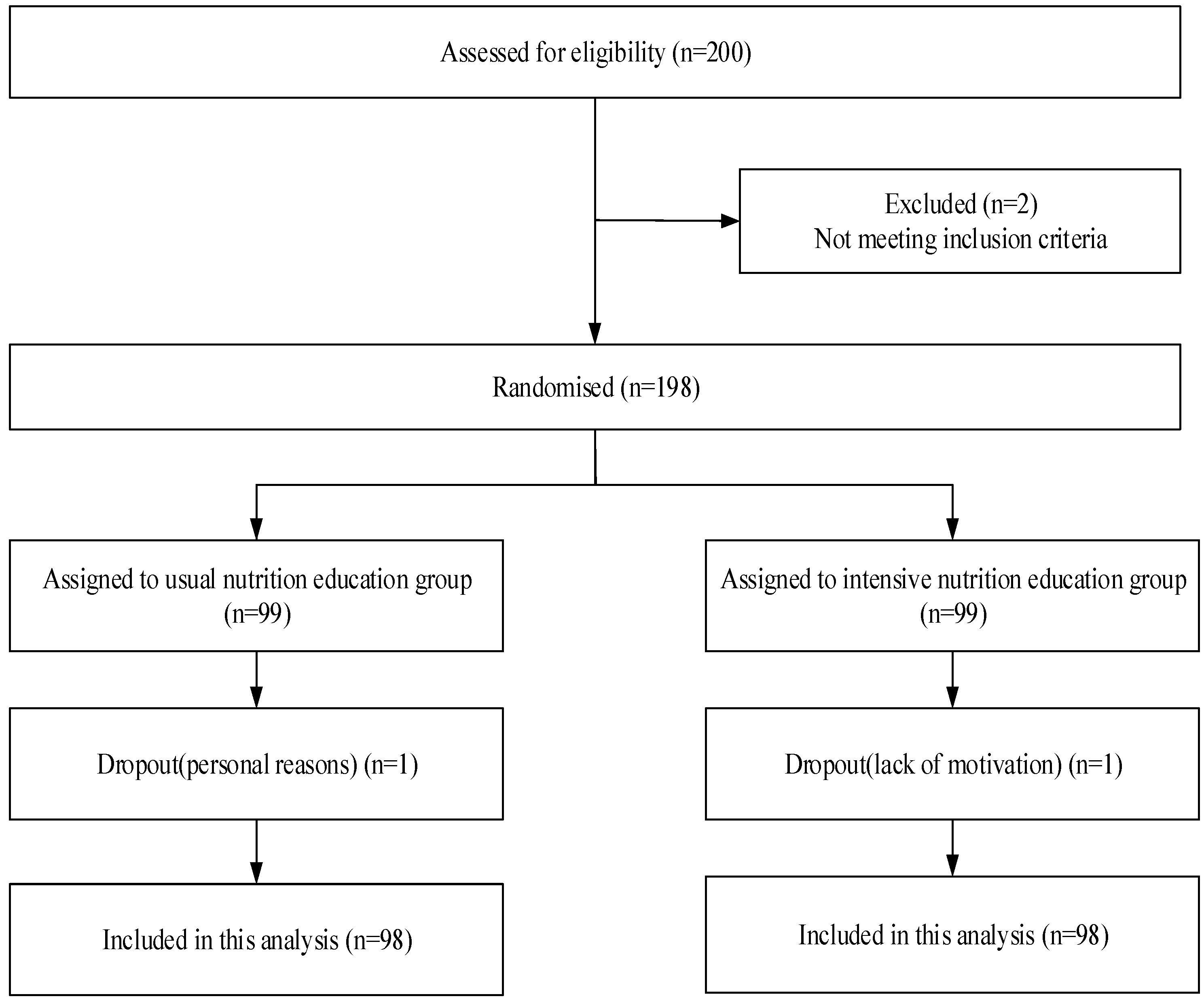
2.2. Study Design and Participants
2.3. Interventions
2.4. Data Collection
2.5. Statistics
3. Results
3.1. Basic Characteristics of the Study Population
3.2. Diabetes Knowledge, Behavioral, and Medication Outcomes
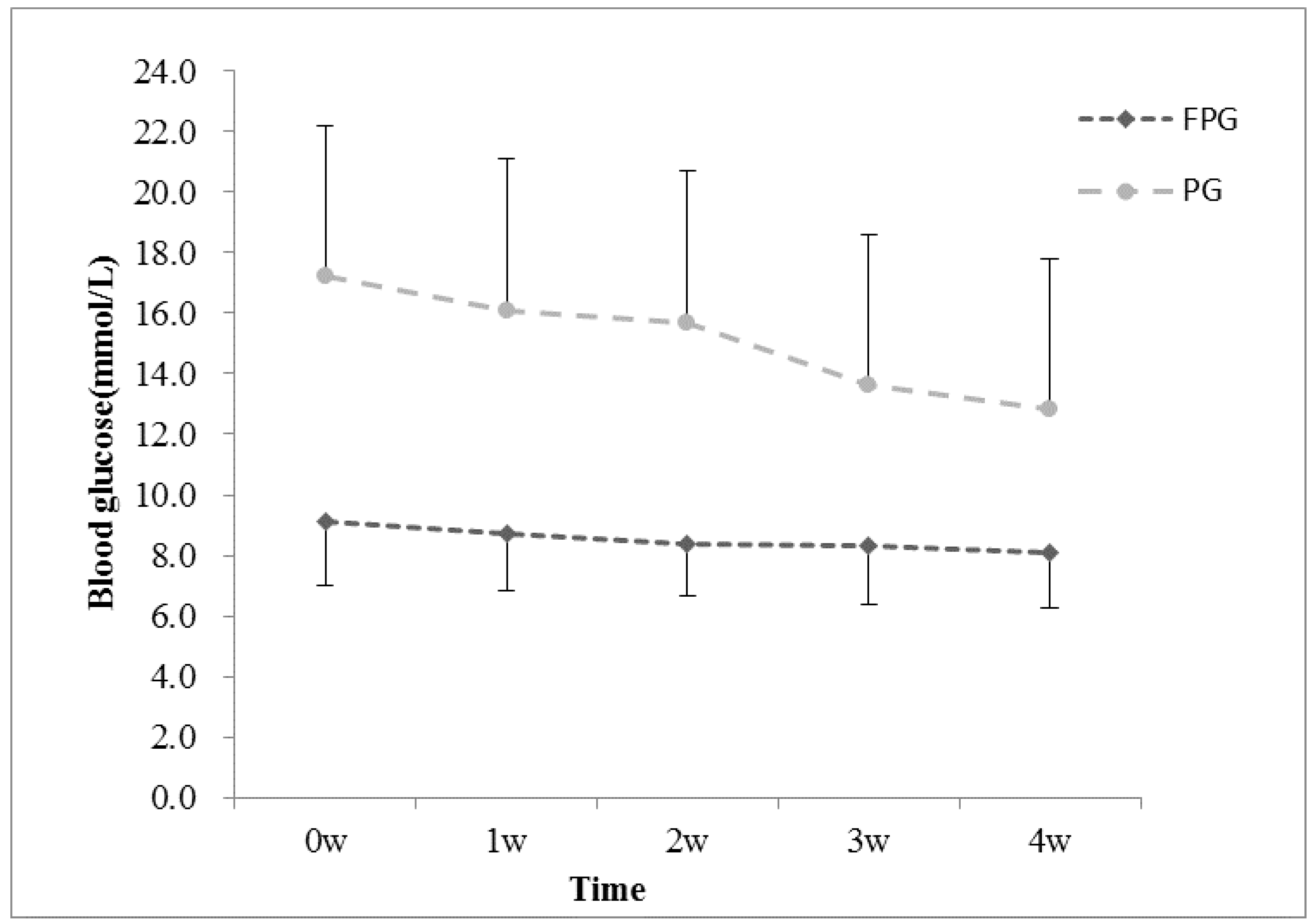
3.3. Fingertip Blood Glucose of INE Group
3.4. Weight, BMI, Blood Glucose, and Lipid Changes after Intervention
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Sarah, W.; Richard, S.; Gojka, R. Global Prevalence of Diabetes. Diabetes Care 2004, 27, 1047–1053. [Google Scholar]
- American Diabetes Association. Standards of Medical Care in Diabetes—2015 Abridged for Primary Care Providers. Clin. Diabetes 2015, 33, 97–111. [Google Scholar]
- Castro-Sánchez, A.E.; Ávila-Ortíz, M.N. Changing dietary habits in persons living with type 2 diabetes. J. Nutr. Educ. Behav. 2013, 45, 761–766. [Google Scholar] [CrossRef] [PubMed]
- Coppola, A.; Sasso, L.; Bagnasco, A.; Giustina, A.; Gazzaruso, C. The role of patient education in the prevention and management of type 2 diabetes: An overview. Endocrine 2015, 53, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Chapman-Novakofski, K.; Karduck, J. Improvement in knowledge, social cognitive theory variables, and movement through stages of change after a community-based diabetes education program. J. Am. Diet. Assoc. 2005, 105, 1613–1616. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.K.; Edwards, L.; Kissling, G.; Sanville, L. Nutrition education improves metabolic outcomes among older adults with diabetes mellitus: Results from a randomized controlled trial. Prev. Med. 2002, 34, 252–259. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Song, Z.; Ba, Y.; Zhu, L.; Wen, Y. Nutritional and eating education improves knowledge and practice of patients with type 2 diabetes concerning dietary intake and blood glucose control in an outlying city of China. Public Health Nutr. 2014, 17, 2351–2358. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Escamilla, R.; Hromi-Fiedler, A.; Vega-López, S.; Bermúdez-Millán, A.; Segura-Pérez, S. Impact of peer nutrition education on dietary behaviors and health outcomes among Latinos: A systematic literature review. J. Nutr. Educ. Behav. 2008, 40, 208–225. [Google Scholar] [CrossRef] [PubMed]
- Brunton, S.A. The changing shape of type 2 diabetes. Medscape J. Med. 2008, 10, 143. [Google Scholar] [PubMed]
- Garcia, A.A.; Villagomez, E.T.; Brown, S.A.; Kouzekanani, K.; Hanis, C.L. The Starr County Diabetes Education Study: Development of the Spanish-language diabetes knowledge questionnaire. Diabetes Care 2001, 24, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Yuan, C.; Lai, C.W.K.; Chan, L.W.C.; Chow, M.; Law, H.K.W.; Ying, M. The effect of diabetes self-management education on body weight, glycemic control, and other metabolic markers in patients with type 2 diabetes mellitus. J. Diabetes Res. 2014, 30, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Chrvala, C.A.; Sherr, D.; Lipman, R.D. Diabetes self-management education for adults with type 2 diabetes mellitus: A systematic review of the effect on glycemic control. Patient Educ. Couns. 2015, 99, 926–943. [Google Scholar] [CrossRef] [PubMed]
- Pani, L.N.; Nathan, D.M.; Grant, R.W. Clinical predictors of disease progression and medication initiation in untreated patients with type 2 diabetes and A1C less than 7%. Diabetes Care 2008, 31, 386–390. [Google Scholar] [CrossRef] [PubMed]
- Franz, M.J.; Boucher, J.L.; Rutten-Ramos, S.; VanWormer, J.J. Lifestyle weight-loss intervention outcomes in overweight and obese adults with type 2 diabetes: A systematic review and meta-analysis of randomized clinical trials. J. Acad. Nutr. Diet. 2015, 115, 1447–1463. [Google Scholar] [CrossRef] [PubMed]
- Osborn, C.Y.; Egede, L.E. Validation of an information-motivation-behavioral skills model of diabetes self-care (IMB-DSC). Patient Educ. Couns. 2010, 79, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Angel, S.; Frederiksen, K.N. Challenges in achieving patient participation: A review of how patient participation is addressed in empirical studies. Int. J. Nurs. Stud. 2015, 52, 1525–1538. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta, K.; Hajna, S.; Joseph, L.; Da, C.D.; Christopoulos, S.; Gougeon, R. Effects of meal preparation training on body weight, glycemia, and blood pressure: Results of a phase 2 trial in type 2 diabetes. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 125. [Google Scholar] [CrossRef] [PubMed]
- Abbott, P.A.; Davison, J.E.; Moore, L.F.; Rubinstein, R. Effective Nutrition Education for Aboriginal Australians: Lessons from a Diabetes Cooking Course. J. Nutr. Educ. Behav. 2012, 44, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Wolf, A.M.; Conaway, M.R.; Crowther, J.Q.; Hazen, K.Y.; Nadler, J.; Oneida, B.; Bovbjerg, V.E.; Improving Control with Activity and Nutrition (ICAN) Study. Translating lifestyle intervention to practice in obese patients with type 2 diabetes: Improving Control with Activity and Nutrition (ICAN) study. Diabetes Care 2004, 27, 1570–1576. [Google Scholar] [CrossRef] [PubMed]
- Kontogianni, M.D.; Liatis, S.; Grammatikou, S.; Perrea, D.; Katsilambros, N.; Makrilakis, K. Changes in dietary habits and their association with metabolic markers after a non-intensive, community-based lifestyle intervention to prevent type 2 diabetes, in Greece. The DEPLAN study. Diabetes Res. Clin. Pract. 2012, 95, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Goldhaber-Fiebert, J.D.; Goldhaber-Fiebert, S.N.; Tristan, M.L.; Nathan, D.M. Randomized controlled community-based nutrition and exercise intervention improves glycemia and cardiovascular risk factors in type 2 diabetic patients in rural Costa Rica. Diabetes Care 2003, 26, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Luo, X.; Liu, T.; Yuan, X.; Ge, S.; Yang, J.; Li, C.; Sun, W. Factors Influencing Self-Management in Chinese Adults with Type 2 Diabetes: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2015, 12, 11304–11327. [Google Scholar] [CrossRef] [PubMed]
- Levy, M.D.; Loy, L.; Zatz, L.Y. Policy approach to nutrition and physical activity education in health care professional training. Am. J. Clin. Nutr. 2014, 99, 1194S–1201S. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Contents | |
|---|---|
| Knowledge of diabetes | Diagnosis of type 2 diabetes mellitus |
| Symptoms of type 2 diabetes mellitus | |
| Main causes of type 2 diabetes mellitus | |
| Complications of type 2 diabetes mellitus | |
| Diabetes medication | The importance of taking medications |
| Different types of diabetic medications | |
| The proper methods of taking diabetic medication | |
| Blood glucose monitoring | The importance of regular blood glucose monitoring |
| The optimal target range for blood glucose control | |
| Methods of self-monitoring of blood glucose | |
| Techniques of handling abnormal blood glucose | |
| Healthy diet | Balanced diet for type 2 diabetics |
| Appropriate caloric intake for type 2 diabetics | |
| Diet combination and cooking method for type 2 diabetics | |
| The importance of eating vegetables, fruits and whole grains | |
| Healthy lifestyle | The importance of regular exercise for type 2 diabetics |
| The appropriate exercise for type 2 diabetics | |
| Taking suitable exercises according to personal fitness level | |
| Giving up bad habits and maintaining healthy behaviors |
| Characteristic | Intervention Assignment | p-Value | |
|---|---|---|---|
| UNE (n = 98) | INE (n = 98) | ||
| Male | 52 (53.1) | 47 (48.0) | 0.48 |
| Age (years) | 58.3 (4.1) | 59.1 (4.6) | 0.23 |
| Duration of diabetes (years) | 6.5 (5.4) | 6.8 (4.8) | 0.63 |
| Diabetes medication use | |||
| No diabetes medication | 16 (16.3) | 14 (14.3) | 0.96 |
| Oral medication only | 48 (49.0) | 49 (50.0) | |
| Insulin only | 17 (17.3) | 16 (16.3) | |
| Oral medication and insulin | 17 (17.3) | 19 (19.4) | |
| Education | |||
| Illiteracy | 7 (7.1) | 2 (2.0) | 0.24 |
| Primary school | 9 (9.2) | 9 (9.2) | |
| Middle school | 25 (25.5) | 31 (31.6) | |
| High school | 29 (29.6) | 36 (36.7) | |
| College | 28 (28.6) | 20 (20.4) | |
| Height (cm) | 164.5 (7.1) | 163.9 (8.1) | 0.56 |
| Weight (kg) | 68.3 (10.0) | 69.1 (11.5) | 0.64 |
| BMI (kg/m2) | 25.1 (1.8) | 25.7 (3.7) | 0.26 |
| Variable | UNE (n = 98) | INE (n = 98) | p-Value * | ||
|---|---|---|---|---|---|
| Baseline | 30-Day | Baseline | 30-Day | ||
| Diabetes Knowledge Questionnaire, mean(SD) | |||||
| Total score | 53.6 (18.2) | 61.8 (19.5) | 56.4 (16.4) | 84.5 (12.8) | <0.001 |
| Daily dietary intake | |||||
| Energy intake (kcal) | 2486 (307) | 2458 (396) | 2452 (253) | 2112 (274) | <0.001 |
| Protein(% of energy intake) | 19% | 19% | 17% | 18% | 0.043 |
| Carbohydrate (% of energy intake) | 43% | 44% | 46% | 60% | |
| Fat (% of energy intake) | 38% | 37% | 37% | 22% | |
| Fiber (g) | 19 (6) | 22 (5) | 21 (4) | 31 (6) | <0.001 |
| Exercise | |||||
| MVPA (min per day) | 23.3 (20.4) | 23.6 (18.2) | 26.7 (21.3) | 46.8 (14.6) | <0.001 |
| Sedentary time (hours per day) | 5.6 (2.4) | 6.1 (4.4) | 5.8 (3.2) | 4.5 (3.8) | 0.007 |
| 30-min MVPA per day, no. (% patients) | 31 (31.6) | 37 (37.8) | 28 (28.6) | 58 (59.2) | 0.003 |
| Glucose-lowering treatment, no. (% patients) | |||||
| Decrease | 2 (2.1) | 5 (5.1) | 0.199 | ||
| Increase | 9 (9.1) | 4 (4.1) | |||
| No change | 87 (88.8) | 89 (90.8) | |||
| Measure | UNE (n = 98) | INE (n = 98) | p-Value ‡ | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | 30-Day | Change | p-Value † | Baseline | 30-Day | Change | p-Value † | ||
| Weight (kg) | 68.3 (10.0) | 68.2 (10.2) | −0.1 (1.0) | 0.226 | 69.1 (11.5) | 68.3 (10.6) | −0.8 (2.9) | 0.012 | 0.625 |
| BMI (kg/m2) | 25.1 (1.8) | 25.0 (1.9) | −0.1 (0.4) | 0.169 | 25.7 (3.7) | 25.3 (3.4) | −0.3 (1.1) | 0.020 | 0.631 |
| FPG (mmol/L) | 9.3 (0.5) | 9.2 (0.5) | −0.0 (0.2) | 0.673 | 9.4 (3.1) | 8.3 (2.8) | −1.1 (2.4) | <0.001 | <0.001 |
| PG (mmol/L) | 18.5 (2.4) | 18.1 (2.3) | −0.4 (0.9) | <0.001 | 17.9 (5.6) | 15.6 (4.7) | −2.3 (3.9) | <0.001 | <0.001 |
| HbA1c (%) | 7.9 (0.4) | 8.0 (0.5) | 0.1 (0.4) | 0.224 | 7.9 (0.4) | 7.3 (0.9) | −0.6 (0.9) | <0.001 | <0.001 |
| TG (mmol/L) | 1.6 (0.5) | 1.6 (0.6) | 0.02 (0.2) | 0.305 | 1.8 (0.9) | 1.6 (0.9) | −0.2 (0.9) | 0.008 | 0.252 |
| TC (mmol/L) | 5.3 (1.1) | 5.2 (1.1) | −0.1 (0.2) | <0.001 | 5.1 (0.9) | 5.0 (1.0) | −0.1 (0.6) | 0.013 | 0.330 |
| HDL-c (mmol/L) | 1.3 (0.3) | 1.3 (0.2) | −0.1 (0.1) | <0.001 | 1.3 (0.2) | 1.3 (0.3) | 0.1 (0.1) | <0.001 | 0.616 |
| LDL-c (mmol/L) | 2.9 (0.5) | 2.9 (0.5) | 0.0 (0.1) | 0.986 | 3.0 (0.7) | 3.0 (0.8) | 0.0 (0.7) | 0.935 | 0.870 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Y.; Xu, M.; Fan, R.; Ma, X.; Gu, J.; Cai, X.; Liu, R.; Chen, Q.; Ren, J.; Mao, R.; et al. The Effects of Intensive Nutrition Education on Late Middle-Aged Adults with Type 2 Diabetes. Int. J. Environ. Res. Public Health 2016, 13, 897. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13090897
Li Y, Xu M, Fan R, Ma X, Gu J, Cai X, Liu R, Chen Q, Ren J, Mao R, et al. The Effects of Intensive Nutrition Education on Late Middle-Aged Adults with Type 2 Diabetes. International Journal of Environmental Research and Public Health. 2016; 13(9):897. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13090897
Chicago/Turabian StyleLi, Ye, Meihong Xu, Rui Fan, Xiaotao Ma, Jiaojiao Gu, Xiaxia Cai, Rui Liu, Qihe Chen, Jinwei Ren, Ruixue Mao, and et al. 2016. "The Effects of Intensive Nutrition Education on Late Middle-Aged Adults with Type 2 Diabetes" International Journal of Environmental Research and Public Health 13, no. 9: 897. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph13090897