WHO Environmental Noise Guidelines for the European Region: A Systematic Review on Environmental Noise and Adverse Birth Outcomes

Abstract
:1. Introduction
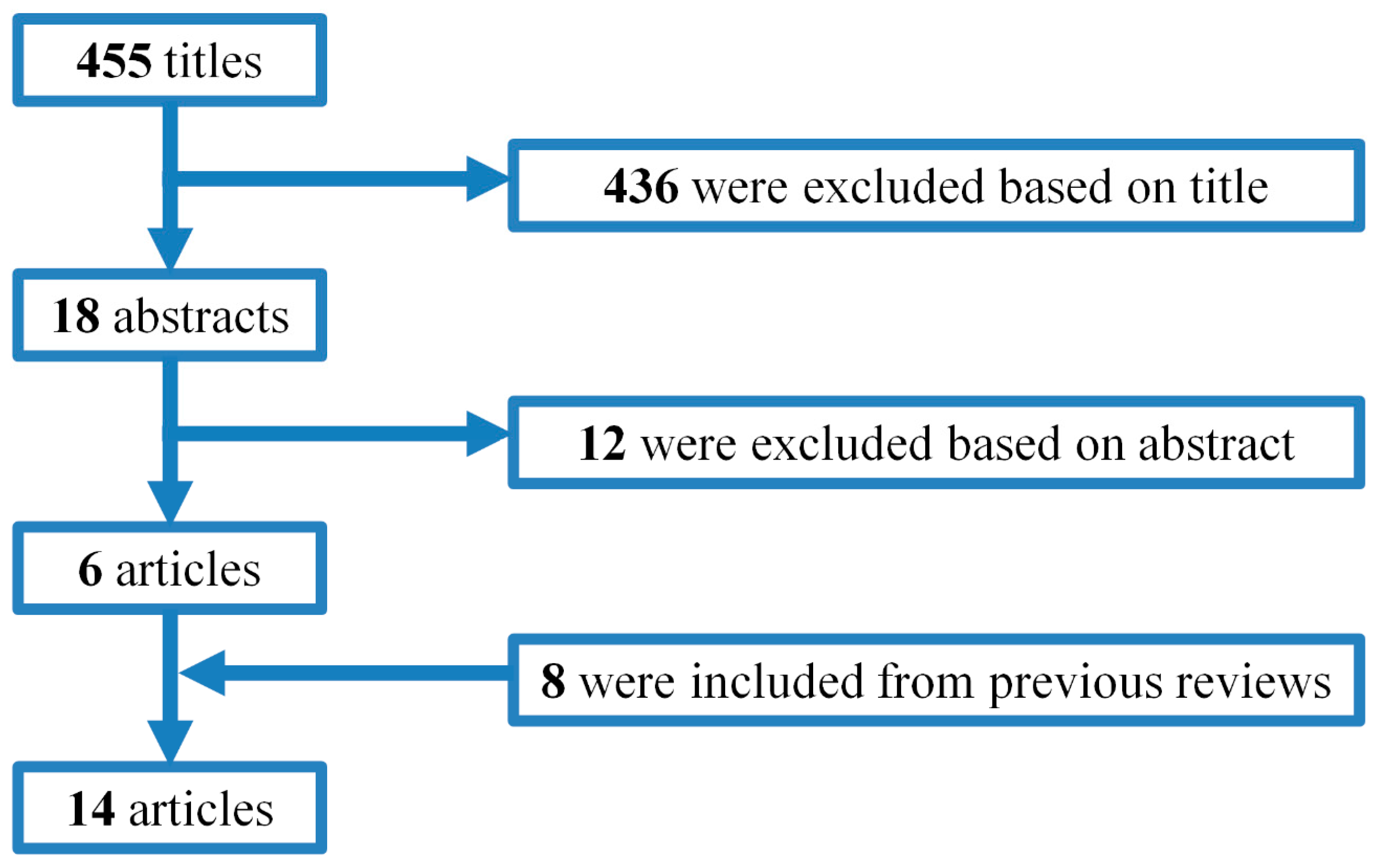
2. Methods
- Publication type (0 = not peer reviewed, 1 = peer reviewed article),
- Study design (1 = ecological, 2 = case control or cohort study, 3 = RCT, 0 = other),
- Noise exposure assessment (3 = objective assessment with noise measurements or noise calculations),
- Assessment of the birth outcomes (1 = subjective assessment by report of mother, 2 = objective e.g., from medical records),
- Confounding factors (0 = no confounding factors considered, 1 = confounding factors considered but some key confounders omitted, 3 = careful consideration of confounders),
- Statistics (0 = flaws in or inappropriate statistical testing or interpretation of statistical tests that may have affected results, 1 = appropriate statistical testing and interpretation of tests),
- Bias (0 = other study design or conduct issues that may have led to bias, 1 = no other serious study flaws).
3. Results
4. Aircraft Noise
4.1. Birth Weight and Preterm Birth
4.2. Congenital Malformations
5. Road Traffic Noise
Birth Weight and Preterm Birth
6. Discussion
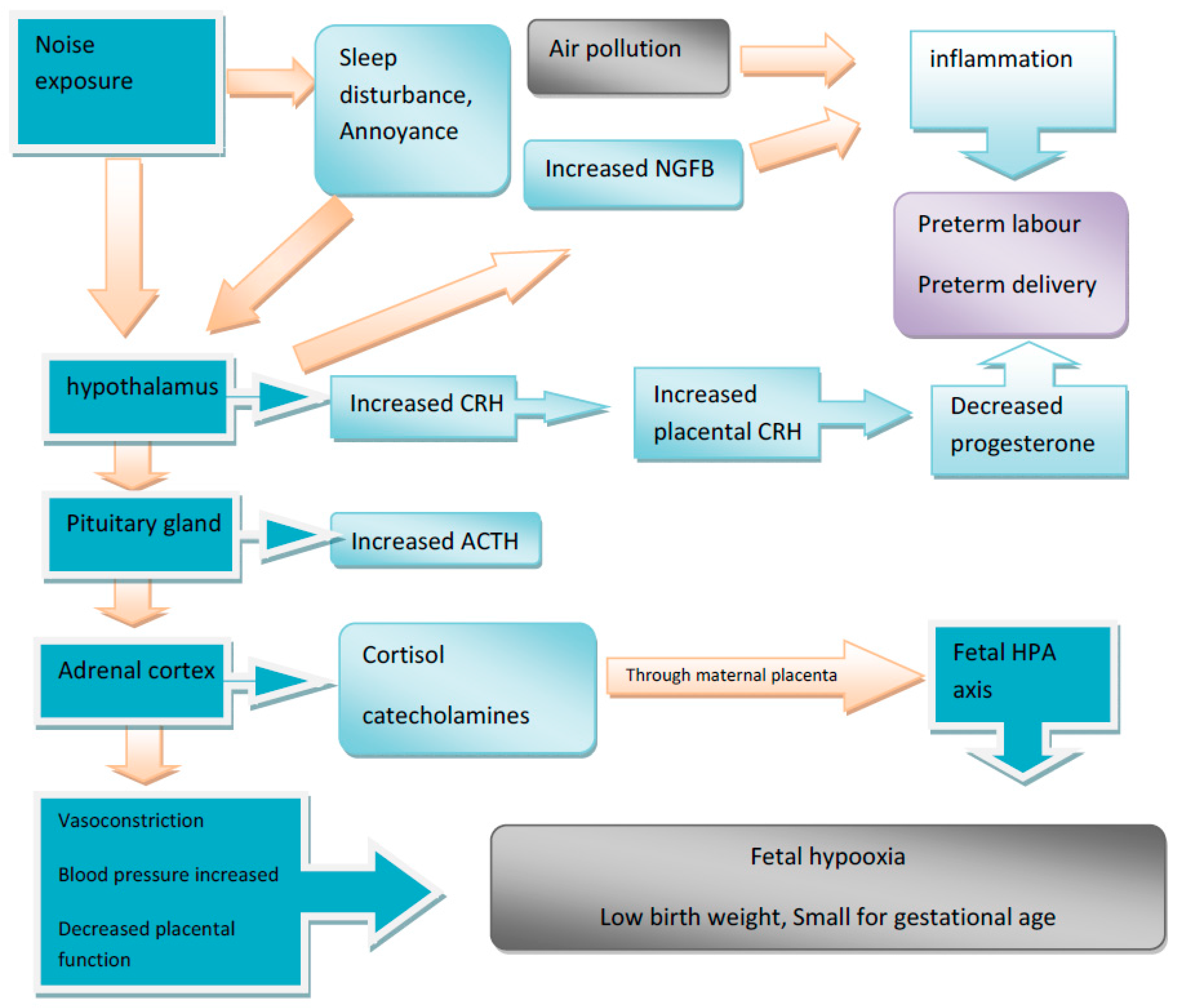
6.1. Biological Mechanism
6.2. Knowledge Gaps and Recommendations
7. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Basner, M.; Babisch, W.; Davis, A.; Brink, M.; Clark, C.; Janssen, S.; Stansfeld, S. Auditory and non-auditory effects of noise on health. Lancet 2014, 383, 1325–1332. [Google Scholar] [CrossRef]
- Hohmann, C.; Grabenhenrich, L.; de Kluizenaar, Y.; Tischer, C.; Heinrich, J.; Chen, C.-M.; Thijs, C.; Nieuwenhuijsen, M.; Keil, T. Health effects of chronic noise exposure in pregnancy and childhood: A systematic review initiated by ENRIECO. Int. J. Hyg. Environ. Health 2013, 216, 217–229. [Google Scholar] [CrossRef] [PubMed]
- Ristovska, G.; Laszlo, H.E.; Hansell, A.L. Reproductive Outcomes Associated with Noise Exposure—A Systematic Review of the Literature. Int. J. Environ. Res. Public Health 2014, 11, 7931–7952. [Google Scholar] [CrossRef] [PubMed]
- Dzhambov, A.M.; Dimitrova, D.D.; Dimitrakova, E.D. Noise exposure during pregnancy, birth outcomes and fetal development: Meta-analyses using quality effects model. Folia Med. 2014, 56, 204–214. [Google Scholar] [CrossRef]
- Johnson, C.D.; Jones, S.; Paranjothy, S. Reducing low birth weight: Prioritizing action to address modifiable risk factors. J. Public Health 2017, 39, 122–131. [Google Scholar] [CrossRef] [PubMed]
- McGowan, J.E.; Alderdice, F.A.; Holmes, V.A.; Johnston, L. Early childhood development of late-preterm infants: A systematic review. Pediatrics 2011, 127, 1111–1124. [Google Scholar] [CrossRef] [PubMed]
- Vadillo-Ortega, F.; Osornio-Vargas, A.; Buxton, M.A.; Sánchez, B.N.; Rojas-Bracho, L.; Viveros-Alcaráz, M.; Castillo-Castrejón, M.; Beltrán-Montoya, J.; Brown, D.G.; O’Neill, M.S. Air pollution, inflammation and preterm birth: A potential mechanistic link. Med. Hypotheses 2014, 82, 219–224. [Google Scholar] [CrossRef] [PubMed]
- WHO Regional Office for Europe. Health 2020: A European Policy Framework Supporting Action across Government and Society for Health and Well-Being. Malta 2012. Available online: http://www.euro.who.int/__data/assets/pdf_file/0009/169803/RC62wd09-Eng.pdf (accessed on 20 May 2016).
- Well, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle–Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 18 April 2013).
- Ando, Y.; Hattori, H. Statistical studies on the effects of intense noise during human fetal life. J. Sound Vib. 1973, 27, 101–110. [Google Scholar] [CrossRef]
- Schell, L.M. Environmental noise and human prenatal growth. Am. J. Phys. Anthropol. 1981, 56, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Knipschild, P.; Meijer, H.; Sallé, H. Aircraft noise and birthweight. Int. Arch. Occup. Environ. Health 1981, 48, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Matsui, T.; Matsuno, T.; Ashimine, K.; Miyakita, T.; Hiramatsu, K.; Yamamoto, T. Association between the rates of low birth-weight and/or preterm infants and aircraft noise exposure. Nihon Eiseigaku Zasshi 2003, 58, 385–394. [Google Scholar] [CrossRef] [PubMed]
- Jones, F.N.; Tauscher, J. Residence under an airport landing pattern as a factor in teratism. Arch. Environ. Health 1978, 33, 10–12. [Google Scholar] [CrossRef] [PubMed]
- Edmonds, L.D.; Layde, P.M.; Erickson, J.D. Airport noise and teratogenesis. Arch. Environ. Health 1979, 34, 243–247. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.N.; Chen, L.J.; Lai, J.S.; Ko, G.N.; Shen, C.Y.; Chang, P.Y. Prospective study of noise exposure during pregnancy on birth weight. Am. J. Epidemiol. 1996, 143, 792–796. [Google Scholar] [CrossRef] [PubMed]
- Gehring, U.; Tamburic, L.; Sbihi, H.; Davies, H.W.; Brauer, M. Impact of noise and air pollution on pregnancy outcomes. Epidemiology 2014, 25, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Dadvand, P.; Ostro, B.; Figueras, F.; Foraster, M.; Basagaña, X.; Valentín, A.; Martinez, D.; Beelen, R.; Cirach, M.; Hoek, G.; et al. Residential Proximity to Major Roads and Term Low Birth Weight: The Roles of Air Pollution, Heat, Noise, and Road-adjacent Trees. Epidemiology 2014, 25, 518–525. [Google Scholar] [CrossRef] [PubMed]
- Hystad, P.; Davies, H.W.; Frank, L.; Van Loon, J.; Gehring, U.; Tamburic, L.; Brauer, M. Residential greenness and birth outcomes: Evaluating the influence of spatially correlated built-environment factors. Environ. Health Perspect. 2014, 122, 1095–1102. [Google Scholar] [CrossRef] [PubMed]
- Hjortebjerg, D.; Andersen, A.M.N.; Ketzel, M.; Pedersen, M.; Raaschou-Nielsen, O.; Sørensen, M. Associations between maternal exposure to air pollution and traffic noise and newborn’s size at birth: A cohort study. Environ. Int. 2016, 95, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Arroyo, V.; Díaz, J.; Ortiz, C.; Carmona, R.; Sáez, M.; Linares, C. Short term effect of air pollution, noise and heat waves on preterm births in Madrid (Spain). Environ. Res. 2016, 145, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Arroyo, V.; Díaz, J.; Carmona, R.; Ortiz, C.; Linares, C. Impact of air pollution and temperature on adverse birth outcomes: Madrid, 2001–2009. Environ. Pollut. 2016, 218, 1154–1161. [Google Scholar] [CrossRef] [PubMed]
- Díaz, J.; Arroyo, V.; Ortiz, C.; Carmona, R.; Linares, C. Effect of Environmental Factors on Low Weight in Non-Premature Births: A Time Series Analysis. PLoS ONE 2016, 11, e0164741. [Google Scholar]
- Goines, L.; Hagler, L. Noise pollution: A modem plague. South Med. J. 2007, 100, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Hepper, P.G.; Shahidullah, S. Noise and the Foetus: A Critical Review of the Literature. Available online: http://www.hse.gov.uk/research/crr_pdf/1994/crr94063.pdf (accessed on 20 November 2012).
- Nakamura, K.; Sheps, S.; Arck, P.C. Stress and reproductive failure: Past notions, present insights and future directions. J. Assist. Reprod. Genet. 2008, 25, 47–62. [Google Scholar] [CrossRef] [PubMed]
- Ising, H.; Kruppa, B. Health effects caused by noise: Evidence in the literature from the past 25 years. Noise Health 2004, 6, 5–13. [Google Scholar] [PubMed]
- Andersson, K.; Lindvall, T. Health Effects of Community Noise; Evaluation of the Nordic Project on “The health Effects of Community Noise”; Nordic Council of Ministers: Copenhagen, Denmark, 1988. [Google Scholar]
- Spreng, M. Central nervous system activation by noise. Noise Health 2000, 7, 49–57. [Google Scholar]
- Babisch, W. The noise/stress concept, risk assessment and research needs. Noise Health 2002, 4, 1–11. [Google Scholar] [PubMed]
- Hobel, C.; Culhaney, J. Role of psychosocial and nutritional stress on poor pregnancy outcome. J. Nutr. 2003, 133, 1709–1715. [Google Scholar]
- De Weerth, C.; Buitelaar, J.K. Physiological stress reactivity in human pregnancy—A review. Neurosci. Biobehav. Rev. 2005, 29, 295–312. [Google Scholar] [CrossRef] [PubMed]
- Gerhardt, K.J. Prenatal and perinatal risks of hearing loss. Semin. Perinatol. 1990, 14, 299–304. [Google Scholar] [PubMed]
- Tometten, M.; Blois, S.; Kuhlmei, A.; Stretz, A.; Klapp, B.F.; Arck, P.C. Nerve growth factor translates stress response and subsequent murine abortion via adhesion molecule-dependent pathways. Biol. Reprod. 2006, 74, 674–683. [Google Scholar] [CrossRef] [PubMed]
- Vrijheid, M.; Slama, R.; Robinson, O.; Chatzi, L.; Coen, M.; van den Hazel, P.; Thomsen, C.; Wright, J.; Athersuch, T.J.; Avellana, N.; et al. The Human Early-Life Exposome (HELIX): Project rationale and design. Environ. Health Perspect. 2014, 122, 535–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Population: general population in settings (hospitals, residences, public venues, educational facilities) | Studies including members of the general population Studies including specific segments of the population particularly at risk, such as pregnant women and newborns Studies including participants exposed to environmental noise; participants exposed to environmental and occupational combined; participants exposed to environmental noise and other environmental factors | Does not meet inclusion criteria Studies including participants exposed to noise in occupational settings not relevant with combined exposure to environmental noise |
| Exposure: exposure to high levels of environmental noise from various noise sources | Noise exposure levels either measured or calculated and expressed in decibel values. noise levels were representative for the exposure assessment of the study participants (for most observational studies, this would be the dwelling location or home) Calculated levels for transportation noise (road, rail, air) based on traffic data reflecting the use of roads, railway lines and in- and outbound flight routes at airports | Does not meet inclusion criteria Studies using hearing loss or defective hearing as a proxy for (previous) noise exposure Surveys with subjective noise exposure assessment, on the basis of subjective ratings |
| Comparator: no noise exposure or lower levels of noise exposure | Study have comparator group (corresponding to no exposure or lower level exposure) | Does not meet inclusion criteria |
| Confounding: adjusted for confounding factors | No inclusion criteria applied; however, for each study, we will assess which possible confounders have been taken into account | No exclusion criteria applied |
| Outcome: assessment of outcome | Data about outcomes taken from medical records or interview using a known scale or validated assessment method Self-reported data about outcome taken from questionnaire | Does not meet inclusion criteria |
| Author, Year | Country | Study Design | Sample Size | Exposure Assessment | Outcome | Confounding Factors | Potential for Bias | Effect Size | Quality Score |
|---|---|---|---|---|---|---|---|---|---|
| Preterm birth and Birth weight | |||||||||
| Ando and Hattori, 1973 [10] | Japan | Case-control study | 713 | Objective assessment, aircraft noise, ECPNL (dB) | LBW (<2500 g) | Gender, maternal age, occupation, parity | High | Higher rate of LBW in noisy area above 75 dBA | 8 |
| Knipschild et al., 1981 [11] | Netherlands | Case-control study | 1840 | Objective assessment, aircraft noise, 3 subgroups Ldn < 65 dBA, Ldn 65–70 dBA, Ldn > 70 dBA | LBW | Gender, parental income | High | 18% LBW in low noise exposed group, 24% LBW in high noise exposed group, 29% in noise exposed above 70 dBA Dose response relationship between aircraft noise and LBW | 8 |
| Schell, 1981 [12] | USA | Cross-sectional study | 115 | Objective assessment, aircraft noise, SEL = 75–100 dBA | Birth weight Gestational length | Maternal age, obstetric history, parental weight and height, education, smoking, family income | High | r = −0.04, p = 0.76 males r = −0.22, p = 0.014 females r = −0.18, p = 0.16 males r = −0.38, p = 0.008 females | 11 |
| Matsui et al., 2003 [13] | Japan | Survey | 160,460 births | Objective assessment, aircraft noise, WECPNL (dB) Control group <75 dBA Exposed subgroups 75–80 dBA, 81–85 dBA, >85 dBA | LBW (<2500 g) Preterm birth (<37 weeks) | Gender, maternal age, socio-economic status, live birth order No adjustment for smoking | High | OR = 1.32 (95% CI 1.18–1.48), p = 0.0001 in the highest level of exposure compared to control group OR = 1.25 (95% CI 1.1–1.4), p = 0.0018 in the highest level of exposure compared to control group | 10 |
| Congenital malformations | |||||||||
| Jones and Tauscher, 1978 [14] | USA | Ecological study | 225146 births 2105 defects | Above vs. below >90 dBA | Birth defects | Information not provided | High | 1185 vs. 737 per 100,000 births p < 0.02 | 8 |
| Edmonds et al., 1979 [15] | USA | Survey | 1745 birth defects | Objective assessment, aircraft noise, high noise level exposure above 65 dBA Ldn | 17 categories of birth defects | Socioeconomic status, race | High | Non significant differences in rates of birth defects in exposed and non-exposed groups | 10 |
| Author, Year | Country | Study Design | Sample Size | Exposure Assessment | Outcome | Confounding Factors | Potential for Bias | Effect Size | Quality Score |
|---|---|---|---|---|---|---|---|---|---|
| Wu et al., 1996 [16] | Taiwan | Prospective study | 200 | Objective and subjective assessment, Leq 24 h of traffic and total noise | LBW | Maternal age, weight gain, gender and gestational age, socioeconomic status | Low | Non-significant correlation between traffic noise exposure and LBW (p = 0.17) | 13 |
| Gehring et al., 2014 [17] | Canada | Retrospective study of birth records population-based cohort study | 68,238 births | Objective, all transportation and road traffic noise modeling | Preterm birth Term LBW Small for gestational age | Gender, ethnicity, parity, family income, education, smoking, air pollution | Low | All road traffic noise (per 6 dB(A) increase OR = 1.02 (95% CI 0.98–1.06) OR = 1.11 (95% CI 1.03–1.19) OR = 1.09 (95% CI 1.06–1.12) | 13 |
| Dadvand et al. 2014 [18] | Spain | Retrospective study of birth records population-based cohort study | 6438 | Objective, traffic noise modeling | Term LBW | Gender, ethnicity, marital status season of conception, parity, education, smoking, BMI, alcohol consumption, air pollution, temperature | Low | RR = 1.03 (95% CI 0.84–1.27) per 6.7 dB(A) | 13 |
| Hystadt et al., 2014 [19] | Canada | Retrospective study of birth records population-based cohort study | 64,705 births | Objective, all transportation and road traffic noise modeling | Preterm birth Small for gestational age | Gender, ethnicity, parity, family income, education, smoking, air pollution | Low | All road traffic noise (per 6 dB(A) increase OR = 1.02 (95% CI 0.98–1.06) OR = 1.09 (95% CI 1.06–1.12) | 13 |
| Hjortebjerg et al. (2016) [20] | Denmark | Cohort study | 75,166 live-born singletons born at term | Calculation method for road and railway traffic noise at the residential address | Term birth weight, | Gestational age sex. maternal age at conception, pre-pregnancy BMI, maternal height, parity, season of conception, educational level, disposable income, smoking and alcohol consumption, air pollution. | low | OR: 1.07 (95% CI: 0.94; 1.21) per 10 dB) No associations after full adjustment | 13 |
| Arroyo et al. (2016a) [21] | Spain | Ecological time series study | 298,705 births | Objective noise measurements from 26 monitoring stations in Madrid Mean Leqd = 64.6 dB(A) Mean Leqn = 59.4 dB(A) | LBW Premature birth | Not considered, air pollution and temperature are controlled variables | high | Transportation noise Leqd (3rd tr) RR = 1.01 (95% CI 1.00–1.02) Leqd (2nd tr) RR = 1.04 (95% CI 1.03–1.05) Leqd (1st tr) RR = 1.03 (95% CI 1.02–1.04) Leqd (2nd tr) RR=1.03 (95%CI 1.02–1.03) Leqn (3rd tr) RR = 1.02 (95%CI 1.01–1.02) | 10 |
| Arroyo et al. (2016b) [22] | Spain | Ecological time series study | 298,705 births | Objective noise measurements from 26 monitoring stations in Madrid Mean Leqd = 64.6 dB(A) Mean Leqn = 59.4 dB(A) | Very Preterm births (30- < 37 weeks) Extremely preterm births (<30 weeks) | Not considered, air pollution and temperature are controlled variables | high | Transportation noise Leqd (Lag 0) RR = 1.07 (95% CI 1.04–1.10) Leqd (Lag 0) RR = 1.28 (95% CI 1.21–1.36) | 10 |
| Diaz et al. (2016) [23] | Spain | Ecological time series study | 298,705 births | Measured noise levels from monitoring stations | LBW in non-premature births Very LBW Extremely LBW | Not considered, air pollution and temperature are controlled variables | low | All noise RR = 1.09 (95% CI 0.99–1.19) (p < 0.1). | 10 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nieuwenhuijsen, M.J.; Ristovska, G.; Dadvand, P. WHO Environmental Noise Guidelines for the European Region: A Systematic Review on Environmental Noise and Adverse Birth Outcomes. Int. J. Environ. Res. Public Health 2017, 14, 1252. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph14101252
Nieuwenhuijsen MJ, Ristovska G, Dadvand P. WHO Environmental Noise Guidelines for the European Region: A Systematic Review on Environmental Noise and Adverse Birth Outcomes. International Journal of Environmental Research and Public Health. 2017; 14(10):1252. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph14101252
Chicago/Turabian StyleNieuwenhuijsen, Mark J., Gordana Ristovska, and Payam Dadvand. 2017. "WHO Environmental Noise Guidelines for the European Region: A Systematic Review on Environmental Noise and Adverse Birth Outcomes" International Journal of Environmental Research and Public Health 14, no. 10: 1252. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph14101252