Prevalence of Chlamydia trachomatis Infection and Its Association with Sexual Behaviour and Alcohol Use in the Population Living in Separated and Segregated Roma Settlements in Eastern Slovakia

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
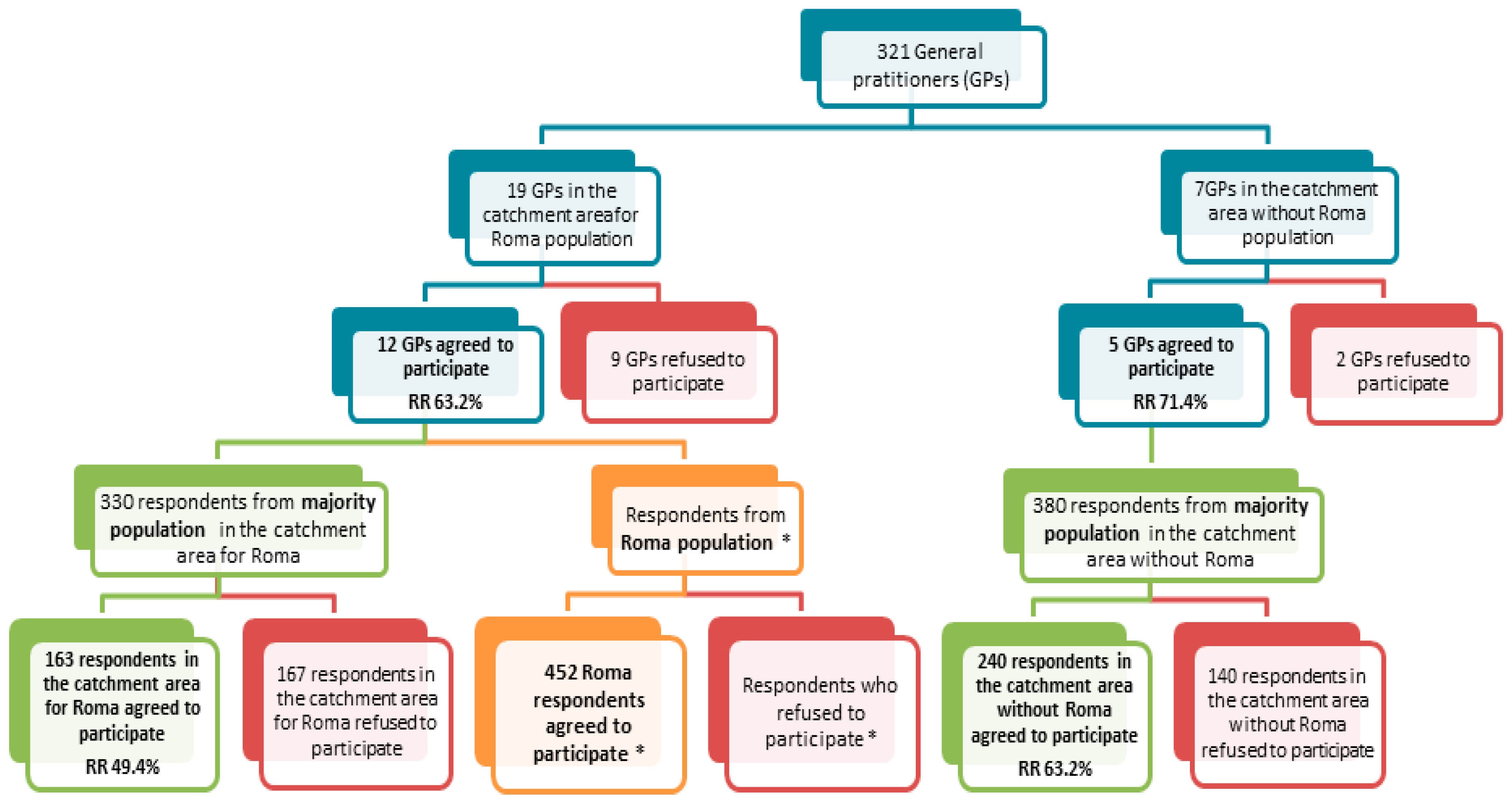
2.1. Study Population
2.2. Questionnaire
2.3. Urine Samples Measurements
2.4. Statistical Analysis
3. Results
3.1. Basic Characteristics of Sample
3.2. Sexual and Drinking Behaviour
3.3. Occurence of Chlamydia Trachomatis Infection
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Mušinka, A.; Škobla, D.; Hurrle, J.; Matlovičová, K.; Kling, J. An Atlas of Roma Communities in Slovakia 2013 (Atlas Rómskych Komunít Na SLOVENSKU 2013); UNDP: Bratislava, Slovakia, 2014; ISBN 978-80-89263-18-9. (In Slovak) [Google Scholar]
- Szeghy, P.; Popper, M. Analysis of the Situation in Slovakia. In Health and the Roma Community, Analysis of the Situation in Europe. Bulgaria, Czech Republic, Greece, Portugal, Romania, Slovakia, Spain; Fundación Secretariado Gitano: Madrid, Spain, 2009; pp. 153–163. [Google Scholar]
- European Union. Roma Health Report. Health Status of the Roma Population. Data Collection in the Member States of the European Union. 2014. Available online: https://ec.europa.eu/health//sites/health/files/social_determinants/docs/2014_roma_health_report_en.pdf (accessed on 15 October 2016).
- Madarasová Gecková, A.; Babinská, I.; Bobáková, D.; Dankulincová Veselská, Z.; Bosáková, L.; Kolarčik, P.; Jarčuška, P.; Pella, D.; Halánová, M.; HepaMeta Team. Socioeconomic characteristics of the population living in Roma settlements and association with health and health-related behaviour. Cent. Eur. J. Public Health 2014, 22, 57–64. [Google Scholar]
- Molinuevo, D.; Koomen, M.; Fóty, K. Living Conditions of the Roma: Substandard Housing and Health; European Foundation for the Improvement of Living and Working Conditions: Dublin, Ireland, 2012; Available online: http://observatorio-lisboa.eapn.pt/ficheiro/Living-conditions-of-the-Roma_Substandard-housing-and-health.pdf (accessed on 10 May 2017).
- Janevic, T.; Jankovic, J.; Bradley, E. Socioeconomic position, gender, and inequalities in self-rated health between Roma and non-Roma in Serbia. Int. J. Public Health 2012, 57, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Voko, Z.; Csepe, P.; Nemeth, R.; Kosa, K.; Kosa, Z.; Szeles, G.; Adany, R. Does socioeconomic status fully mediate the effect of ethnicity on the health of Roma people in Hungary? J. Epidemiol. Community Health 2009, 63, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, N.S.; Derecho, N.R. Health and the Roma Community, Analysis of the Situation in Europe, Bulgaria, Czech Republic, Greece, Portugal, Romania, Slovakia, Spain, 1st ed.; Fundación Secretariado Gitano: Madrid, Spain, 2009; pp. 7–175. [Google Scholar]
- Jarcuska, P.; Bobakova, D.; Uhrin, J.; Bobak, L.; Babinska, I.; Kolarcik, P.; Veselska, Z.; Madarasová Gecková, A.; HEPA-META Team. Are barriers in accessing health services in the Roma population associated with worse health status among Roma? Int. J. Public Health 2013, 58, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Masseria, C.; Mladovsky, P.; Hernández-Quevedo, C. The socio-economic determinants of the health status of Roma in comparison with non-Roma in Bulgaria, Hungary and Romania. Eur. J. Public Health 2010, 20, 549–554. [Google Scholar] [CrossRef] [PubMed]
- Peters, J.A.; Parry, G.D.; Van Cleemput, P.; Moore, J.; Cooper, C.L.; Walters, S.J. Health and use of health services: A comparison between Gypsies and Travellers and other ethnic groups. Ethn. Health 2009, 14, 359–377. [Google Scholar] [CrossRef] [PubMed]
- Colombini, M.; Rechel, B.; Mayhew, S.H. Access of Roma to sexual and reproductive health services: Qualitative findings from Albania, Bulgaria and Macedonia. Glob. Public Health 2012, 7, 522–553. [Google Scholar] [CrossRef] [PubMed]
- Babinská, I.; Madarasová Gecková, A.; Jarčuška, P.; Pella, D.; Mareková, M.; Štefková, G.; Dankulincová Veselská, Z.; HepaMeta Team. Does the Population Living in Roma Settlements Differ in Physical Activity, Smoking and Alcohol Consumption from the Majority Population in Slovakia? Cent. Eur. J. Public Health 2014, 22, 22–27. [Google Scholar]
- Kenyon, C.; Buyze, J.; Colebunders, R. Classification of incidence and prevalence of certain sexually transmitted infections by world regions. Int. J. Infect. Dis. 2014, 18, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Chan, P.A.; Robinette, A.; Montgomery, M.; Almonte, A.; Cu-Uvin, S.; Lonks, J.R.; Chapin, K.C.; Kojic, E.M.; Hardy, E.J. Extragenital Infections Caused by Chlamydia trachomatis and Neisseria gonorrhoeae: A Review of the Literature. Infect. Dis. Obstet. Gynecol. 2016. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.; Cheng, V.Y.; Kwong, N.S. Neonatal haemorrhagic conjunctivitis: A specific sign of chlamydial infection. Hong Kong Med. J. 2006, 12, 27–32. [Google Scholar] [PubMed]
- Darville, T. Chlamydia trachomatis infections in neonates and young children. Semin. Pediatr. Infect. Dis. 2005, 16, 235–244. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, K.T.; Marcus, J.L.; Nieri, G.; Philip, S.S.; Klausner, J.D. Rectal Gonorrhea and Chlamydia Reinfection Is Associated with Increased Risk of HIV Seroconversion. J. Acquir. Immune Defic. Syndr. 2010, 53, 537–543. [Google Scholar] [CrossRef] [PubMed]
- Fleming, D.T.; Wasserheit, J.N. From epidemiological synergy to public health policy and practice: The contribution of other sexually transmitted diseases to sexual transmission of HIV infection. Sex. Transm. Infect. 1999, 75, 3–17. [Google Scholar] [CrossRef] [PubMed]
- Carter, J.D.; Inman, R.D. Chlamydia-induced reactive arthritis: Hidden in plain sight? Best Pract. Res. Clin. Rheumatol. 2011, 25, 359–374. [Google Scholar] [CrossRef] [PubMed]
- Zeidler, H.; Kuipers, J.; Köhler, L. Chlamydia-induced arthritis. Curr. Opin. Rheumatol. 2004, 16, 380–392. [Google Scholar] [CrossRef] [PubMed]
- Falasinnu, T.; Gilbert, M.; Salway, T.H.; Gustafson, P.; Ogilvie, G.; Shoveller, J. Predictors identifying those at increased risk for STDs: A theory-guided review of empirical literature and clinical guidelines. Int. J. STD AIDS 2015, 26, 839–851. [Google Scholar] [CrossRef] [PubMed]
- Nelson, H.D.; Helfand, M. Screening for chlamydial infection. Am. J. Prev. Med. 2001, 20, 95–107. [Google Scholar] [CrossRef]
- Novak, M.; Novak, D. Risk factors for Chlamydia trachomatis infection among users of an internet-based testing service in Sweden. Sex. Reprod. Healthc. 2013, 4, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Klovstad, H.; Grjibovski, A.; Aavitsland, P. Population based study of genital Chlamydia trachomatis prevalence and associated factors in Norway: A cross sectional study. BMC Infect. Dis. 2012, 12, 150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harling, G.; Subramanian, S.V.; Bärnighausen, T.; Kawachi, I. Socioeconomic disparities in Sexually Transmitted Infections among young adults in the United States: Examining the interaction between income and race/ethnicity. Sex. Transm. Dis. 2013, 40, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Matser, A.; Luu, N.; Geskus, R.; Heijman, T.; Heiligenberg, M.; van Veen, M.; van der Loeff, S.M. Higher Chlamydia trachomatis Prevalence in Ethnic Minorities Does Not Always Reflect Higher Sexual Risk Behaviour. PLoS ONE 2013, 8, e67287. [Google Scholar] [CrossRef] [PubMed]
- James, A.B.; Geisler, W.M. Predictors of high chlamydia and gonorrhea positivity rates among men in the southern United States. J. Natl. Med. Assoc. 2012, 104, 20–27. [Google Scholar] [CrossRef]
- Hogben, M.; Leichliter, J.S. Social Determinants and Sexually Transmitted Disease Disparities. Sex. Transm. Dis. 2008, 35, S13–S18. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2014; U.S. Department of Health and Human Services: Atlanta, GA, USA, 2015. Available online: http://www.cdc.gov/std/stats (accessed on 8 August 2017).
- Fenton, K.A.; Mercer, C.H.; McManus, S.; Erens, B.; Wellings, K.; Macdowall, W.; Byron, C.L.; Copas, A.J.; Nanchahal, K.; Field, J.; et al. Ethnic variations in sexual behavior in Great Britain and risk of sexually transmitted infections: A probability survey. Lancet 2005, 365, 1246–1255. [Google Scholar] [CrossRef]
- Naimi, T.S.; Lipscomb, L.E.; Brewer, R.D.; Gilbert, B.C. Binge Drinking in the Preconception Period and the Risk of Unintended Pregnancy: Implications for Women and Their Children. Pediatrics 2003, 111, 1136–1141. [Google Scholar] [PubMed]
- Standerwic, K.; Davies, C.; Tucker, L.; Sheron, N. Binge drinking, sexual behaviour and sexually transmitted infection in the UK. Int. J. STD AIDS 2007, 18, 810–813. [Google Scholar] [CrossRef] [PubMed]
- Hutton, H.E.; McCaul, M.E.; Santora, P.B.; Erbelding, E.J. The Relationship between Recent Alcohol Use and Sexual Behaviors: Gender Differences among STD Clinic Patients. Alcohol. Clin. Exp. Res. 2008, 32, 2008–2015. [Google Scholar] [PubMed]
- Stulhofer, A.; Bacak, V.; Ajdukovic, D.; Graham, C. Understanding the association between condom use at first and most recent sexual intercourse: An assessment of normative, calculative, and habitual explanation. Soc. Sci. Med. 2010. [Google Scholar] [CrossRef] [PubMed]
- Zembe, Y.Z.; Townsend, L.; Thorson, A.; Ekström, A.M. Predictors of Inconsistent Condom Use among a Hard to Reach Population of Young Women with Multiple Sexual Partners in Peri-Urban South Africa. PLoS ONE 2012, 7, e51998. [Google Scholar] [CrossRef] [PubMed]
- Tarkang, E.E. Condom Use and Number of Sexual Partners among Secondary School Female Students in an Urban City of Cameroon. Rwanda J. Health Sci. 2013, 2, 30–33. [Google Scholar] [CrossRef]
- Ashenhurst, J.R.; Wilhite, E.R.; Harden, K.P.; Fromme, K. Number of Sexual Partners and Relationship Status Are Associated with Unprotected Sex across Emerging Adulthood. Arch. Sex. Behav. 2016. [Google Scholar] [CrossRef] [PubMed]
- Public Health Authority of the Slovak Republic (PHA SR). ANNUAL REPORT of Regional Public Health Authorities in Slovakia for the Year 2016. 2017. Available online: http://www.uvzsr.sk/docs/vs/vyrocna_sprava_SR_2016.pdf (accessed on 7 June 2017). (In Slovak).
- Madarasová Gecková, A.; Jarčuška, P.; Mareková, M.; Pella, D.; Siegfried, L.; Jarčuška, P.; Halánová, M.; HepaMeta Team. HepaMeta—Prevalence of hepatitis B/C and metabolic syndrome in population living in separated and segregated Roma settlements: A methodology used in a cross-sectional population-based study using community based approach. Cent. Eur. J. Public Health 2014, 22, 6–11. [Google Scholar]
- Tourangeau, R.; Smith, T.W. Asking sensitive questions: The impact of data collection mode, question format, and question context. Public Opin. Q. 1996, 60, 275–304. [Google Scholar] [CrossRef]
- Prättälä, R.; Helakorpi, S.; Sipilä, N.; Sippola, R.; Sääksjärvi, K. (Eds.) Social Determinants of Health Behaviours, Finbalt Health Monitor 1998–2008; Juvenes Print: Tampere, Finland, 2011; pp. 401–404. ISBN 978-952-245-485-0. [Google Scholar]
- Helasoja, V.; Lahelma, E.; Prättälä, R.; Petkeviciene, J.; Pudule, I.; Tekkel, M. The sociodemographic patterning of drinking and binge drinking in Estonia, Latvia, Lithuania and Finland, 1994–2002. BMC Public Health 2007, 7, 241. [Google Scholar] [CrossRef] [PubMed]
- Petrov, P. How reproductive behavior of Roma in Bulgaria is influenced by the age at which sexual life and marital life start. Meditsinski Pregled Sestrinsko Delo/Med. Rev. Inf. Nurs. Staff 2009, 41, 12–16. [Google Scholar]
- Sedlecky, K.; Rašević, M. Challenges in sexual and reproductive health of Roma people who live in settlements in Serbia. Eur. J. Contracept. Reprod. Health Care 2015, 20, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Šprocha, B. Reproduction of the Roma Population in Slovakia and Prognosis of Population Development (Reprodukcia Rómskeho Obyvateľstva na Slovensku a Prognóza Jeho Populačného Vývoja); The Institute for Forecasting of the Slovak Academy of Sciences. Infostat—Demographic Research Centre. OF PRINT JH: Bratislava, Slovakia, 2014; pp. 35–91. ISBN 978-80-89037-38-4. (In Slovak) [Google Scholar]
- Djonic, D.; Djuric, M.; Bassioni-Stamenic, F.; McFarland, W.; Knezevic, T.; Nikolic, S.; Zivkovic, V.; Vallabhaneni, S. HIV-related risk behaviors among Roma youth in Serbia: Results of two community-based surveys. J. Adolesc. Health 2013, 52, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Filadelfiová, J.; Mesochoritisová, A. Research on Sexual and Reproductive Behavior in Roma Communities in Slovakia (Výskum Sexuálneho a Reprodukčného Správania v Rómskych Komunitách na Slovensku); Association of Roma in Slovakia: Banska Bystrica, Slovakia, 2005. [Google Scholar]
- Amirkhanian, Y.A.; Kelly, J.A.; Kabakchieva, E.; Antonova, R.; Vassileva, S.; DiFranceisco, W.J.; McAuliffe, T.L.; Vassilev, B.; Petrova, E.; Khoursineb, R.A. High-risk sexual behavior, HIV/STD prevalence, and risk predictors in the social networks of young Roma (Gypsy) men in Bulgaria. J. Immigr. Minor. Health 2013, 15, 172–181. [Google Scholar] [CrossRef] [PubMed]
- Kabakchieva, E.; Vassileva, S.; Kelly, J.A.; Amirkhanian, Y.A.; DiFranceisco, W.J.; McAuliffe, T.L.; Antonova, R.; Mihaylova, M.; Vassilev, B.; Khouesine, R.A.; et al. HIV risk behavior patterns, predictors, and sexually transmitted disease prevalence in the social networks of young Roma (Gypsy) men in Sofia, Bulgaria. Sex. Trans. Dis. 2006, 33, 485–490. [Google Scholar] [CrossRef] [PubMed]
- Kabakchieva, E.; Amirkhanian, Y.A.; Kelly, J.A.; McAuliffe, T.L.; Vassileva, S. High levels of sexual HIV/STD risk behaviour among Roma (Gypsy) men in Bulgaria: Patterns and predictors of risk in a representative community sample. Int. J. STD AIDS 2002, 13, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.A.; Amirkhanian, Y.A.; Kabakchieva, E.; Csepe, P.; Seal, D.W.; Antonova, R.; Mihaylov, A.; Gyukits, G. Gender roles and HIV sexual risk vulnerability of Roma (Gypsy) men and women in Bulgaria and Hungary: An ethnographic study. AIDS Care 2004, 16, 231–245. [Google Scholar] [CrossRef] [PubMed]
- Sipetic, S.; Ilic, D.; Marinkovic, J.; Vlajinac, H.; Bjegovic, V.; Cucic, V.; Laaser, U. HIV/AIDS risk behaviours among Roma and non-Roma sex workers in Belgrade (Serbia). Coll. Antropol. 2012, 36, 1197–1203. [Google Scholar] [PubMed]
- Marston, C.; King, E. Factors that shape young people’s sexual behaviour: A systematic review. Lancet 2006, 368, 1581–1586. [Google Scholar] [CrossRef]
- Khadr, S.N.; Jones, K.G.; Mann, S.; Hale, D.R.; Johnson, A.M.; Viner, R.M.; Mercer, C.H.; Wellings, K. Investigating the relationship between substance use and sexual behaviour in young people in Britain: Findings from a national probability survey. BMJ Open 2016, 6, e011961. [Google Scholar] [CrossRef] [PubMed]
- Tobin, K.E.; Yang, C.; King, K.; Latkin, C.A.; Curriero, F.C. Associations Between Drug and Alcohol Use Patterns and Sexual Risk in a Sample of African American Men Who Have Sex with Men. AIDS Behav. 2016, 20, 590–599. [Google Scholar] [CrossRef] [PubMed]
- Phillips-Howard, P.A.; Bellis, M.A.; Briant, L.B.; Jones, H.; Downing, J.; Kelly, I.E.; Bird, T.; Cook, P.A. Wellbeing, alcohol use and sexual activity in young teenagers: Findings from a cross-sectional survey in school children in North West England. Subst. Abuse Treat. Prev. Policy 2010, 10, 27. [Google Scholar] [CrossRef] [PubMed]
- Strote, J.; Lee, J.E.; Weschler, H. Increasing MDMA use among college students: Results of a national survey. J. Adolesc. Health 2002, 30, 64–72. [Google Scholar] [CrossRef]
- Cooper, M.L. Alcohol use and risky sexual behavior among college students and youth: Evaluating the evidence. J. Stud. Alcohol Suppl. 2002, 14, 101–117. [Google Scholar] [CrossRef]
- Velicko, I.; Ploner, A.; Sparén, P.; Marions, L.; Herrmann, B.; Kühlmann-Berenzon, S. Sexual and testing behaviour associated with Chlamydia trachomatis infection: A cohort study in an STI clinic in Sweden. BMJ Open 2016, 6, e011312. [Google Scholar] [CrossRef] [PubMed]
- Aicken, C.R.; Nardone, A.; Mercer, C.H. Alcohol misuse, sexual risk behaviour and adverse sexual health outcomes: Evidence from Britain’s national probability sexual behaviour surveys. J. Public Health 2011, 33, 262–271. [Google Scholar] [CrossRef] [PubMed]
- Kiene, S.M.; Barta, W.D.; Tennen, H.; Armeli, S. Alcohol, helping young adults to have unprotected sex with casual partners: Findings from a daily diary study of alcohol use and sexual behavior. J. Adolesc. Health 2009, 44, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Hensel, D.J.; Stupiansky, N.W.; Orr, D.P.; Fortenberry, J.D. Event-level marijuana use, alcohol use, and condom use among adolescent women. Sex. Transm. Dis. 2011, 38, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Leigh, B.C.; Vanslyke, J.G.; Hoppe, M.J.; Rainey, D.T.; Morrison, D.M.; Gillmore, M.R. Drinking and condom use: Results from an events-based daily diary. AIDS Behav. 2008, 12, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Balogová, L.; Jarčuška, P.; Pilátová, M.; Vološinová, D. Infection of Chlamydia trachomatis in chosen group of population. Intern. Med. 2009, 9, 19. [Google Scholar]
- Kacena, K.A.; Dohnal, K.; Benesova, V.; Grivna, M.; Deliopolu, J.; Trýzna, R.; Horák, J.; Gaydos, C.A.; Quinn, T.C. Chlamydia, gonorrhea, and HIV-1 prevalence among five populations of women in the Czech and Slovak Republics. Sex. Transm. Dis. 2001, 28, 356–362. [Google Scholar] [CrossRef] [PubMed]
- Andreassen, T.; Weiderpass, E.; Nicula, F.; Suteu, O. Controversies about cervical cancer screening: A qualitative study of Roma women’s (non)participation in cervical cancer screening in Romania. Soc. Sci. Med. 2017, 183, 485. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Roma | Non-Roma | p-Value | |
|---|---|---|---|
| n = 452 | n = 403 | ||
| Age, mean (SD) | 34.7 (9.14) | 33.5 (7.4) | <0.05 a |
| Gender, n (%) | |||
| Women | 293 (64.8) | 218 (54.1) | <0.01 b |
| Men | 159 (35.2) | 185 (45.9) | |
| Highest education, n (%) | |||
| Higher | 10 (2.3) | 300 (76.3) | <0.001 b |
| Apprenticeship | 73 (16.5) | 84 (21.4) | |
| Elementary | 360 (81.3) | 9 (2.3) | |
| Unemployment, n (%) | 396 (89.6) | 102 (26.4) | <0.001 b |
| Number of children in household, mean (SD) | 3.8 (3.72) | 1.2 (1.48) | <0.001 a |
| Roma n (%) | Non-Roma 1 n (%) | OR (CI) | |
|---|---|---|---|
| Living with a partner in the present | |||
| Yes | 374 (82.7) | 263 (65.3) | 2.48 (1.77–3.47) *** |
| Age at first sexual intercourse | |||
| 15 years or less | 126 (27.9) | 18 (4.5) | 7.71 (4.59–12.94) *** |
| Number of sexual partners | |||
| 5 or more partners | 52 (11.5) | 83 (20.6) | 0.45 (0.31–0.66) *** |
| Condom use | |||
| Inconsistent use | 422 (93.4) | 314 (77.9) | 3.56 (1.99–6.36) *** |
| Reasons for condom use | |||
| Protection against unwanted pregnancy | 103 (22.8) | 177 (43.9) | 0.37 (0.28–0.50) *** |
| Protection against infectious diseases | 40 (8.8) | 88 (21.8) | 0.34 (0.23–0.52) *** |
| Sexual intercourse for money or reward | |||
| Yes | 13 (2.9) | 8 (2.0) | 1.37 (0.56–3.34) n.s. |
| Drinking behaviour | |||
| 6 or more doses of alcohol on one occasion once a month or more | 75 (16.6) | 64 (15.6) | 1.06 (0.74–1.54) n.s. |
| Drinking Behaviour (Six or More Doses of Alcohol on One Occasion) | |||
|---|---|---|---|
| Less Than Once a Month 1 n (%) | Once a Month or More n (%) | OR (CI) | |
| ROMA | |||
| Number of sexual partners | |||
| Five or more partners | 26 (7.1) | 26 (34.7) | 6.99 (3.73–13.09) *** |
| Condom use | |||
| Inconsistent use | 347 (94.8) | 69 (92) | 0.67 (0.21–2.14) n.s. |
| NON-ROMA | |||
| Number of sexual partners | |||
| Five or more partners | 54 (16.7) | 29 (45.3) | 4.27 (2.35–7.78) *** |
| Condom use | |||
| Inconsistent use | 256 (79) | 55 (85.9) | 1.77 (0.70–4.49) n.s. |
| Roma N = 422 | Non-Roma N = 335 | p-Value a | |
|---|---|---|---|
| Men, n (%) | 3 (2.0) | 4 (2.4) | 0.778 |
| Women, n (%) | 13 (4.8) | 5 (2.9) | 0.330 |
| ∑ | 16 (3.8) | 9 (2.7) | 0.398 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Babinská, I.; Halánová, M.; Kalinová, Z.; Čechová, L.; Čisláková, L.; Madarasová Gecková, A. Prevalence of Chlamydia trachomatis Infection and Its Association with Sexual Behaviour and Alcohol Use in the Population Living in Separated and Segregated Roma Settlements in Eastern Slovakia. Int. J. Environ. Res. Public Health 2017, 14, 1579. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph14121579
Babinská I, Halánová M, Kalinová Z, Čechová L, Čisláková L, Madarasová Gecková A. Prevalence of Chlamydia trachomatis Infection and Its Association with Sexual Behaviour and Alcohol Use in the Population Living in Separated and Segregated Roma Settlements in Eastern Slovakia. International Journal of Environmental Research and Public Health. 2017; 14(12):1579. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph14121579
Chicago/Turabian StyleBabinská, Ingrid, Monika Halánová, Zuzana Kalinová, Lenka Čechová, Lýdia Čisláková, and Andrea Madarasová Gecková. 2017. "Prevalence of Chlamydia trachomatis Infection and Its Association with Sexual Behaviour and Alcohol Use in the Population Living in Separated and Segregated Roma Settlements in Eastern Slovakia" International Journal of Environmental Research and Public Health 14, no. 12: 1579. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph14121579