A Geographical Analysis of Emergency Medical Service Calls and Extreme Heat in King County, WA, USA (2007–2012)

Abstract
:1. Introduction
2. Materials and Methods
2.1. Exposure Data and Assessment
2.2. EMS Data
2.3. Demographic and Environmental Data
2.4. Statistical Methods
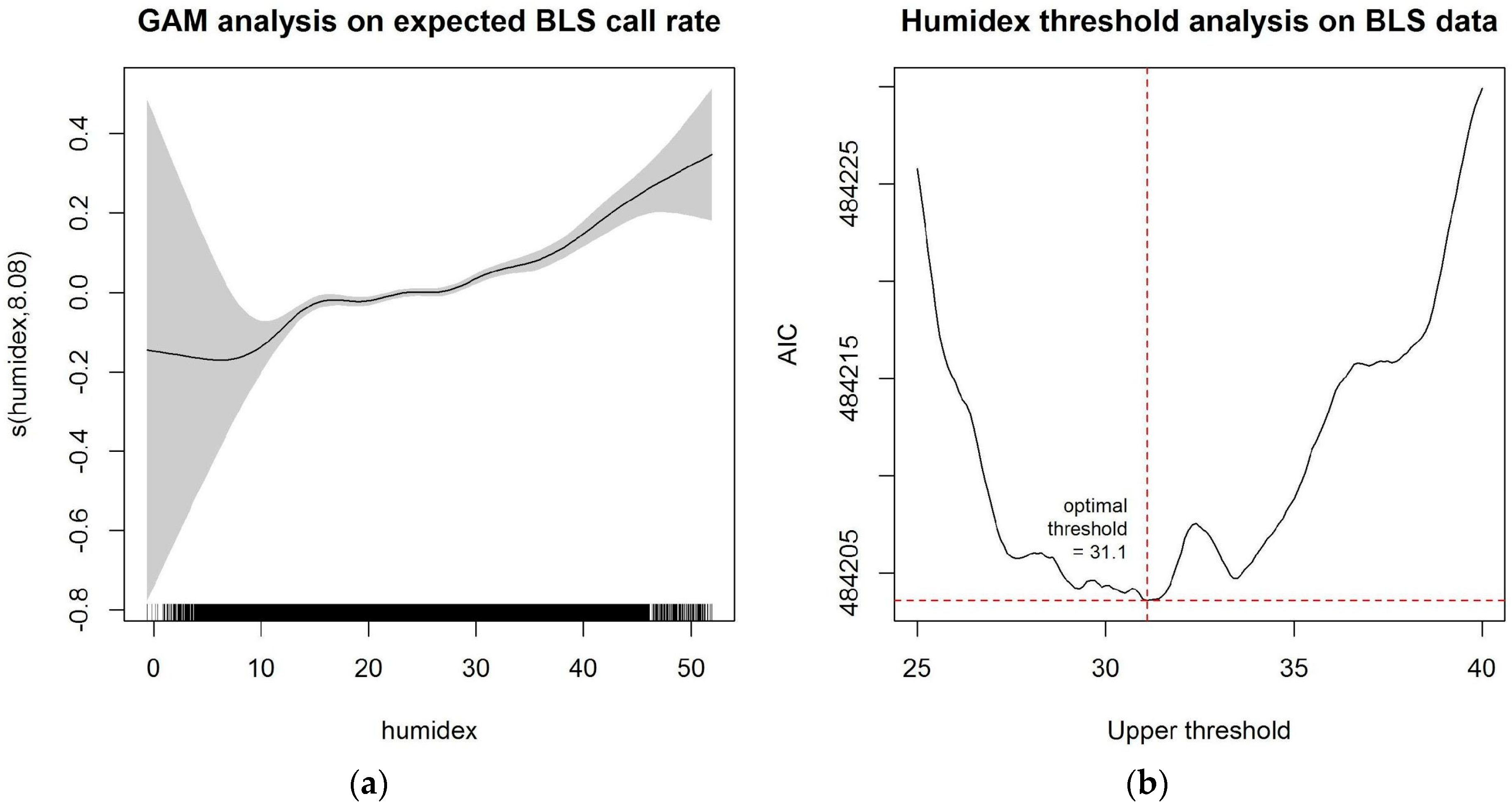
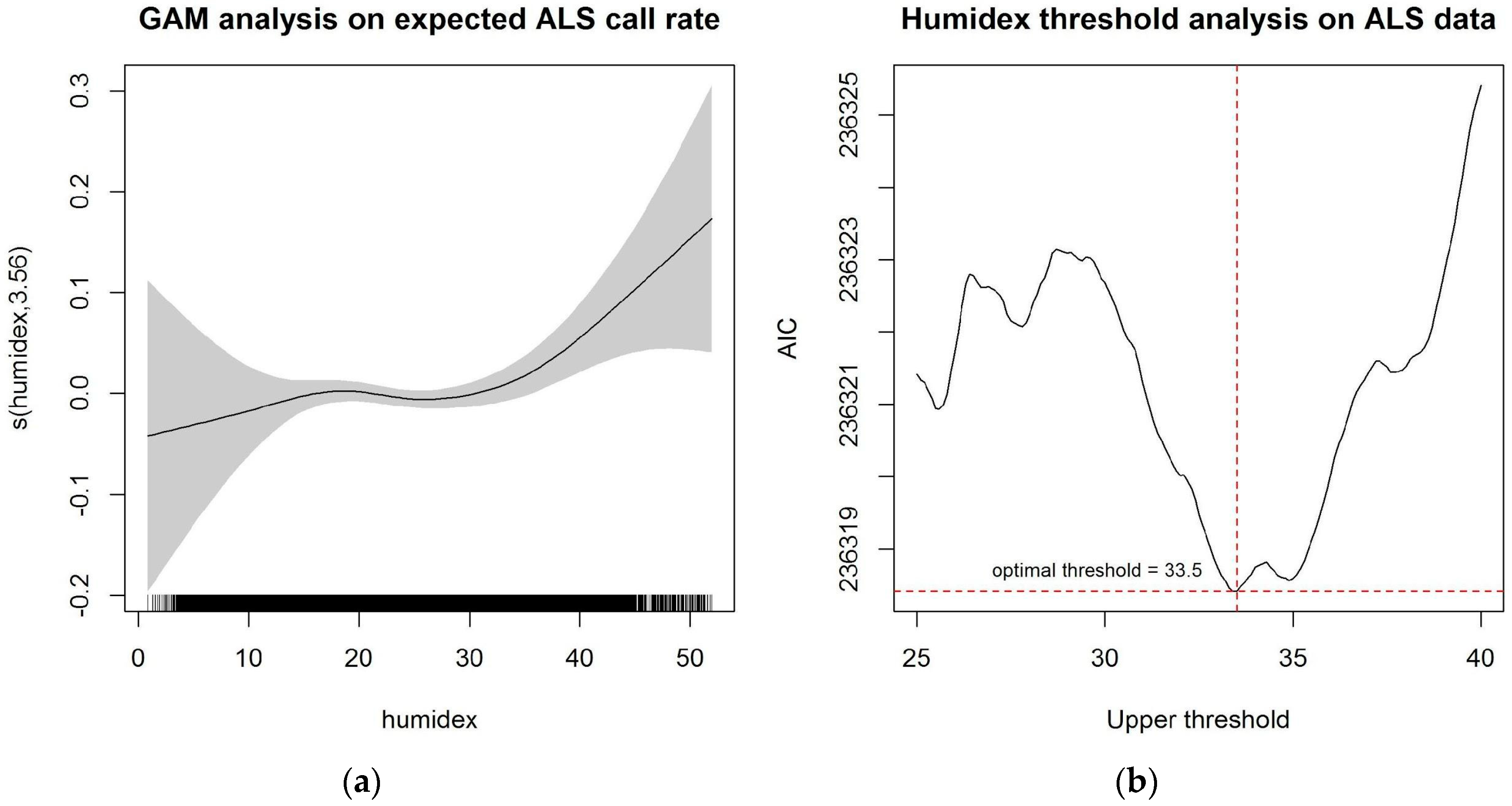
2.4.1. Temporal Analysis on Extreme Heat Thresholds
2.4.2. Association between Heat Exposure and EMS Call Rates
2.4.3. Effect Modification by Environmental and Demographic Characteristics
3. Results
3.1. Statistical Results
3.1.1. Temporal Analysis of Extreme Heat Thresholds
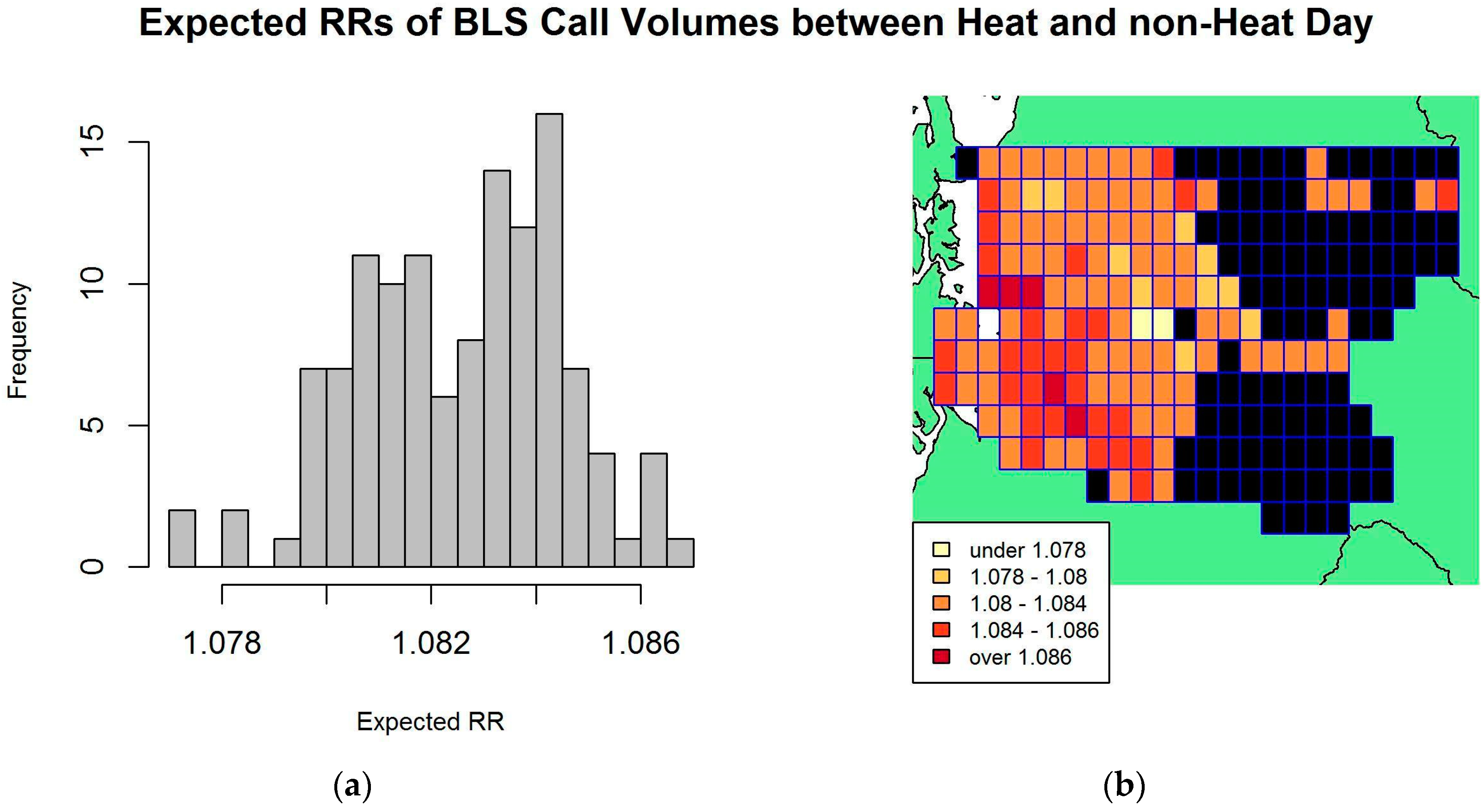
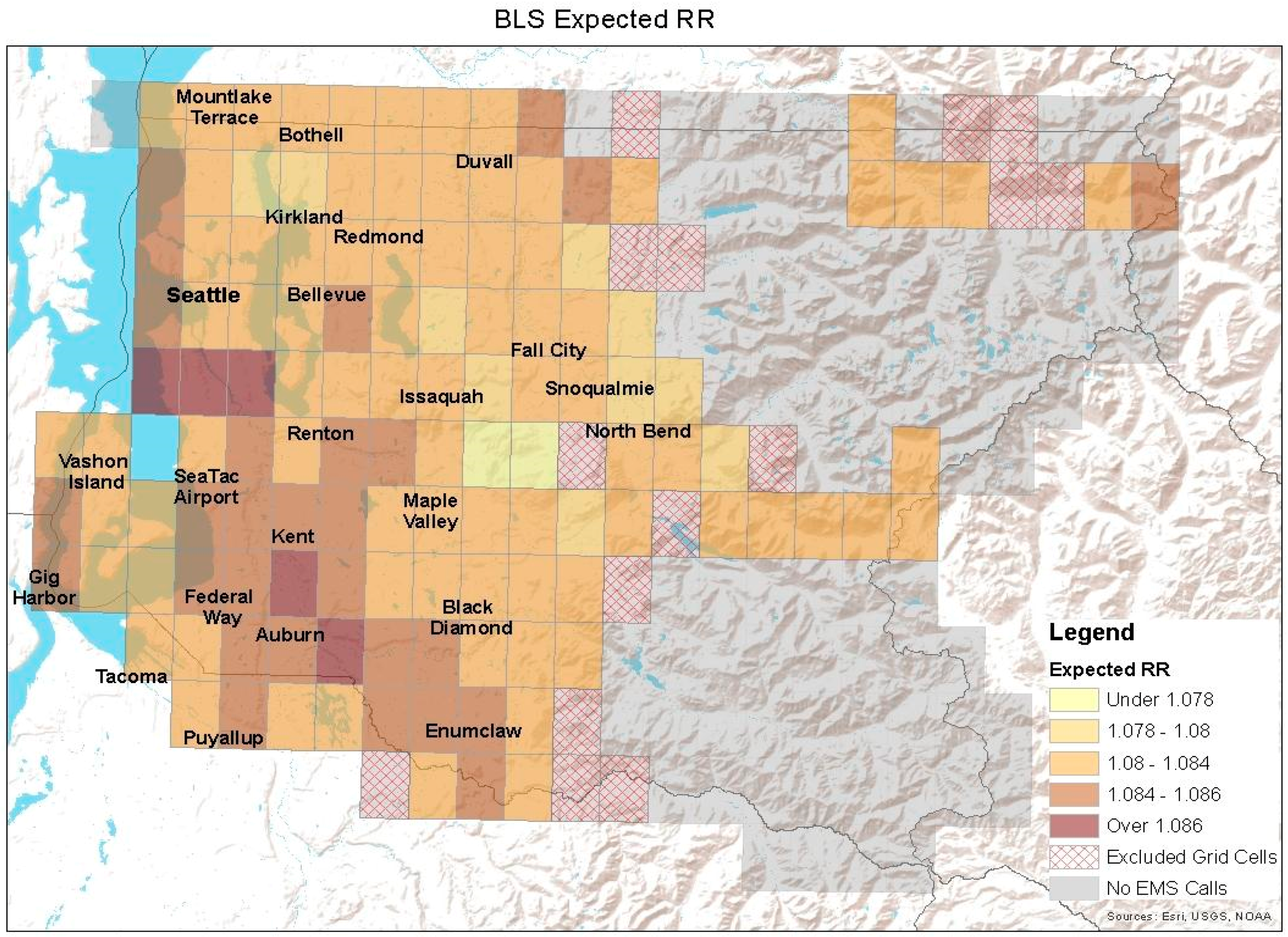
3.1.2. Association between Heat Exposure and EMS Call Counts
3.1.3. Effect Modifications by Environmental and Demographic Characteristics
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Estimated RR | 95% Confidence Interval | p Value |
|---|---|---|---|
| Heat day | 1.102 | (1.054, 1.151) | <0.001 |
| % Impervious surfaces | 1.011 | (0.998, 1.025) | 0.101 |
| % Population ≥ 65 years old | 1.033 | (0.984, 1.085) | 0.184 |
| % Poverty | 1.066 | (1.029, 1.105) | <0.001 |
| Interaction between heat and % impervious surfaces | 0.999 | (0.998, 1.001) | 0.353 |
| Heat day | 1.097 | (0.992, 1.215) | 0.072 |
| % Impervious surfaces | 1.011 | (0.998, 1.025) | 0.102 |
| % Population ≥ 65 years old | 1.034 | (0.984, 1.085) | 0.187 |
| % Poverty | 1.064 | (1.029, 1.105) | <0.001 |
| Interaction between heat and % population ≥ 65 years old | 0.999 | (0.989, 1.008) | 0.752 |
| Heat day | 1.123 | (1.066, 1.182) | <0.001 |
| % Impervious surfaces | 1.011 | (0.998, 1.025) | 0.102 |
| % Population ≥ 65 years old | 1.033 | (0.985, 1.085) | 0.184 |
| % Poverty | 1.067 | (1.029, 1.106) | <0.001 |
| Interaction between heat and % poverty | 0.997 | (0.992, 1.001) | 0.144 |


References
- U.S. Global Change Research Program. The Impacts of Climate Change on Human Health in the United States: A Scientific Assessment. 2016. Available online: https://health2016.globalchange.gov/ (accessed on 31 July 2017).
- Roe, G.H.; Baker, M.B. Why is climate sensitivity so unpredictable? Science 2007, 318, 629–632. [Google Scholar] [CrossRef] [PubMed]
- Knutti, R.; Hegerl, G.C. The equilibrium sensitivity of the earth’s temperature to radiation changes. Nat. Geosci. 2008, 1, 735–742. [Google Scholar] [CrossRef]
- Sherwood, S.C.; Huber, M. An adaptability limit to climate change due to heat stress. PNAS 2010, 107, 9552–9555. [Google Scholar] [CrossRef] [PubMed]
- Busch Isaksen, T.; Fenske, R.; Hom, E.; Ren, Y.; Lyons, H.; Yost, M. Increased mortality associated with extreme-heat exposure in King County, Washington, 1980–2010. Int. J. Biometeorol. 2016, 60, 85–98. [Google Scholar] [CrossRef] [PubMed]
- Busch Isaksen, T.; Yost, M.; Hom, E.; Ren, Y.; Lyons, H.; Fenske, R. Increased hospital admissions associated with extreme-heat exposure in King County, Washington 1990–2010. Rev. Environ. Health 2015, 30, 51–64. [Google Scholar] [CrossRef]
- Medina-Ramon, M.; Zanobetti, A.; Cavanagh, D.P.; Schwartz, J. Extreme temperature and mortality: Assessing effect modification by personal characteristics and specific cause of death in a multi-city case-only analysis. Environ. Health Perspect. 2006, 114, 1331–1336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kue, R.C.; Dyer, K. The impact of heat waves on transport volumes in an urban emergency medical services system: A retrospective review. Prehosp. Disaster Med. 2013, 28, 610–615. [Google Scholar] [CrossRef] [PubMed]
- Golden, J.S.; Hartz, D.; Brazel, A.; Luber, G.; Phelan, P. A biometeorology study of climate and heat-related morbidity in Phoenix from 2001 to 2006. Int. J. Biometeorol. 2008, 52, 471–480. [Google Scholar] [CrossRef] [PubMed]
- Alessandrini, E.; Sajani, S.; Scotto, F.; Miglio, R.; Marchesi, S.; Lauriola, P. Emergency ambulance dispatches and apparent temperature: A time series analysis in Emilia-Romagna, Italy. Environ. Res. 2011, 111, 1192–1200. [Google Scholar] [CrossRef] [PubMed]
- Bassil, K.L.; Cole, D.C.; Moineddin, R.; Lou, W.; Craig, A.M.; Schwartz, B.; Rea, E. The relationship between temperature and ambulance response calls for heat-related illness in Toronto, Ontario, 2005. J. Epidemiol. Community Health 2011, 65, 829–831. [Google Scholar] [CrossRef] [PubMed]
- Dolney, T.J.; Sheridan, S.C. The relationship between extreme heat and ambulance response calls for the city of Toronto, Ontario, Canada. Environ. Res. 2006, 101, 94–103. [Google Scholar] [CrossRef] [PubMed]
- Calkins, M.M.; Isaksen, T.B.; Stubbs, B.A.; Yost, M.G.; Fenske, R.A. Impacts of extreme heat on emergency medical service calls in King County, Washington, 2007–2012: Relative risk and time series analyses of basic and advanced life support. Environ. Health 2016, 15, 13. [Google Scholar] [CrossRef] [PubMed]
- Buyantuyev, A.; Wu, J. Urban heat islands and landscape heterogeneity: linking spatiotemporal variations in surface temperatures to land-cover and socioeconomic patterns. Landsc. Ecol. 2010, 25, 17–33. [Google Scholar] [CrossRef]
- Yuan, F.; Bauer, M.E. Comparison of impervious surface area and normalized difference vegetation index as indicators of surface urban heat island effects in Landsat imagery. Remote Sens. Environ. 2007, 106, 375–386. [Google Scholar] [CrossRef]
- Carrega, P. A method for the reconstruction of mountain air temperatures with automatic cartographic applications. Theor. Appl. Climatol. 1995, 52, 69–84. [Google Scholar] [CrossRef]
- Laing, B.; Weng, Q. Multiscale analysis of Census-based land surface temperature variations and determinants in Indianapolis, United States. J. Urban Plan. Dev. 2008, 134, 129–139. [Google Scholar] [CrossRef]
- Svensson, M.; Eliasson, I.; Holmer, B. A GIS-based empirical model to simulate air temperature variations in the Göteborg urban area during the night. Clim. Res. 2002, 22, 215–226. [Google Scholar] [CrossRef]
- Tveito, O.E.; Førland, E.J. Mapping temperatures in Norway: Applying terrain information, geostatistics and GIS. Nor. Geogr. Tidsskr. 1999, 53, 202–212. [Google Scholar] [CrossRef]
- Weng, Q.; Yang, S. Managing the adverse thermal effects of urban development in a densely populated Chinese city. J. Environ. Manage. 2004, 70, 145–156. [Google Scholar] [CrossRef] [PubMed]
- Weng, Q.; Lu, D.; Liang, B. Urban surface biophysical descriptors and land surface temperature variations. Photogramm. Eng. Remote Sens. 2006, 72, 1275–1286. [Google Scholar] [CrossRef]
- Huang, G.; Zhou, W.; Cadenasso, M.L. Is everyone hot in the city? Spatial pattern of land surface temperatures, land cover, and neighborhood socioeconomic characteristics in Baltimore, MD. J. Environ. Manage. 2011, 92, 1753–1759. [Google Scholar] [CrossRef] [PubMed]
- Jenerette, G.D.; Harlan, S.L.; Stefanov, W.L.; Martin, C.A. Ecosystem services and urban heat riskscape moderation: Water, green spaces and social inequality in Phoenix, USA. Ecol. Appl. 2011, 21, 2637–2651. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.P.; Wilson, J.S. The socio-spatial dynamics of extreme urban heat events: The case of heat-related deaths in Philadelphia. Appl. Geogr. 2009, 29, 419–434. [Google Scholar] [CrossRef]
- Zhang, K.; Oxwald, E.M.; Brown, D.G.; Brines, S.J.; Gronlund, C.J.; White-Newsome, J.L.; Rood, R.B.; O’Neill, M.S. Geospatial exploration of spatial variation of summertime temperatures in the Detroit metropolitan region. Environ. Res. 2011, 111, 1046–1053. [Google Scholar] [CrossRef] [PubMed]
- Kestens, Y.; Brand, A.; Fournier, M.; Goudreau, S.; Kosatsky, T.; Maloley, M.; Smargiassi, A. Modelling the variation of land surface temperature as determinant of risk of heat-related health events. Int. J. Health Geogr. 2011, 10, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Harlan, S.L.; Brazel, A.J.; Prashad, L.; Stefanov, W.L.; Larsen, L. Neighborhood microclimates and vulnerability to heat stress. Soc. Sci. Med. 2006, 63, 2847–2863. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.P.; Stanforth, A.; Lulla, V.; Luber, G. Developing an applied extreme heat vulnerability index utilizing socioeconomic and environmental data. Appl. Geogr. 2012, 35, 23–31. [Google Scholar] [CrossRef]
- Eliasson, I.; Svensson, M.K. Spatial air temperature variations and urban land use—A statistical approach. Meteorol. Appl. 2003, 10, 135–143. [Google Scholar] [CrossRef]
- Center for Disease Control (CDC). About Extreme Heat. 2017. Available online: https://www.cdc.gov/disasters/extremeheat/heat_guide.html (accessed on 31 July 2017).
- Congressional Black Caucus Foundation (CBCF). African Americans and Climate Change: An Unequal Burden. 2004. Available online: http://sustainablecommunitydevelopmentgroup.org/wordpress/wp-content/uploads/2013/06/African-Americans-Climate-Report-l.pdf (accessed on 31 July 2017).
- International Federation of Red Cross (IFRC). India: Heat Wave. 2003. Available online: http://www.ifrc.org/docs/appeals/rpts03/indiaheatwave03a1.pdf (accessed on 6 June 2013).
- Ghumman, U.; Horney, J. Characterizing the Impact of Extreme Heat on Mortality, Karachi, Pakistan. Prehosp. Disaster Med. 2016, 31, 263–266. [Google Scholar] [CrossRef] [PubMed]
- Klinenberg, E. Heat Wave: A Social Autopsy of Disaster in Chicago; The University of Chicago Press: Chicago, IL, USA, 2002; ISBN 978-0226443225. [Google Scholar]
- Semenza, J.C.; Rubin, C.H.; Falter, K.H.; Selanikio, J.D.; Flanders, W.D.; Howe, H.L.; Wilhelm, J.L. Heat-related deaths during the July 1995 heat wave in Chicago. N. Engl. J. Med. 1996, 335, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.S.; Peng, F.; Zou, B.; Shi, W.Z.; Wilson, G.J. Spatially Analyzing the Inequity of the Hong Kong Urban Heat Island by Socio-Demographic Characteristics. Int. J. Environ. Res. Public Health 2016, 13, 317. [Google Scholar] [CrossRef] [PubMed]
- Kilbourne, E.M. Heat-related illness: Current status of prevention efforts. Am. J. Prev. Med. 2002, 22, 328–329. [Google Scholar] [CrossRef]
- Naughton, M.P.; Henderson, A.; Mirabelli, M.C.; Kaiser, R.; Wilhelm, J.L.; Kieszak, S.M.; McGeehin, M.A. Heat-related mortality during a 1999 heat wave in Chicago. Am. J. Prev. Med. 2002, 22, 221–227. [Google Scholar] [CrossRef]
- Rogot, E.; Sorlie, P.D.; Backlund, E. Air conditioning and mortality in hot weather. Am. J. Epidemiol. 1992, 136, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Kolpak, P.; Wang, L. Exploring the social and neighborhood predictors of diabetes: A comparison between Toronto and Chicago. Prim. Health Care Res. Dev. 2017, 18, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Curriero, F.C.; Heiner, K.S.; Samet, J.M.; Zeger, S.L.; Strug, L.; Patz, J.A. Temperature and mortality in 11 cities of the eastern United States. Am. J. Epidemiol. 2002, 155, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Reid, C.E.; O’Neil, M.S.; Gronlund, C.J.; Brines, S.J.; Brown, D.G.; Diez-Roux, A.V.; Schwartz, J. Mapping community determinants of heat vulnerability. Environ. Health Perspect. 2009, 117, 1730–1736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maurer, E.P.; Wood, A.W.; Adam, J.C.; Lettenmaier, D.P.; Nijssen, B. A long-term hydrologically based data set of land surface fluxes and states for the conterminous United States. J. Clim. 2002, 15, 3237–3325. [Google Scholar] [CrossRef]
- Santee, W.R.; Wallace, R.F. Use of Humidex to set Thermal Work Limits for Emergency Workers in Protective Clothing. Ind. Health 2011, 49, 95–106. [Google Scholar]
- Public Health-Seattle King County (PHSKC) Division of Emergency Medical Service. 2012 Annual Report to the King County Council. Available online: http://www.kingcounty.gov/depts/health/emergency-medical-services/~/media/depts/health/emergency-medical-services/documents/reports/2012-Annual-Report.ashx (accessed on 31 July 2017).
- U.S. Census Bureau. Age Groups and Sex: 2010. 2010. Available online: https://factfinder.census.gov/faces/nav/jsf/pages/index.xhtml (accessed on 31 July 2017).
- U.S. Census Bureau. 2010 Poverty Status in the Past 12 Months by Sex and Age. 2010. Available online: https://factfinder.census.gov/faces/nav/jsf/pages/index.xhtml (accessed on 31 July 2017).
- Department of Ecology. Western Washington Land Cover Change. 2016. Available online: http://www.ecy.wa.gov/services/gis/data/imageryBaseMapsEarthCover/landcover/landcover.htm (accessed on 26 July 2017).
- Akaike, H. Prediction and Entropy. In Selected Papers of Hirotugu Akaike; Springer: New York, NY, USA, 1985; pp. 387–410. [Google Scholar]
- Hastie, T.J.; Tibshirani, R.J. Generalized Additive Models; CRC Press: Boca Raton, FL, USA, 1990; ISBN 9780412343902. [Google Scholar]
- McCullagh, P.; Nelder, J.A. Generalized Linear Models; CRC Press: Boca Raton, FL, USA, 1989; ISBN 978-0412317606. [Google Scholar]
- Liang, K.; Zeger, S. Longitudinal Data Analysis Using Generalized Linear Models. Biometrika 1986, 73, 13–22. [Google Scholar] [CrossRef]
- Moran, P.A. Notes on Continuous Stochastic Phenomena. Biometrika 1950, 37, 17–23. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. The R Project for Statistical Computing. 2017. Available online: https://www.R-project.org/ (accessed on 31 July 2017).
- Akbari, H. Energy Saving Potentials and Air Quality Benefits of Urban Heat Island Mitigation. 2005. Available online: http://www.actrees.org/files/Research/Energy%20Savings%20of%20Urban%20Heat%20Island%20Mitigation.PDF (accessed on 31 July 2017).




| Variable | BLS Call | ALS Call |
|---|---|---|
| Total number of calls—raw data | 441,119 | 121,794 |
| Total number of calls included in statistical analysis | 434,853 | 120,638 |
| Number of grid cells included in statistical analysis | 124 | 116 |
| Average number of local heat days per grid cell 1 | 109.08 | 60.44 |
| Average number of local non-heat days per grid cell 1 | 808.90 | 857.60 |
| Average (observed) number of calls per heat day per grid cell (SD) | 4.16 (7.51) | 1.24 (2.16) |
| Average (observed) number of calls per non-heat day per grid cell (SD) | 3.78 (6.77) | 1.13 (1.99) |
| Variable | Estimated RR | 95% Confidence Interval | p Value |
|---|---|---|---|
| Heat day | 1.080 | (1.060, 1.099) | <0.001 |
| % Impervious surfaces | 1.011 | (0.998, 1.025) | 0.102 |
| % Population ≥ 65 years old | 1.033 | (0.984, 1.085) | 0.185 |
| % Poverty | 1.066 | (1.029, 1.105) | <0.001 |
| Variable | Estimated RR | 95% Confidence Interval | p Value |
|---|---|---|---|
| Heat day | 1.067 | (1.035, 1.100) | <0.001 |
| % Impervious surfaces | 1.015 | (1.001, 1.029) | 0.039 |
| % Population ≥ 65 years old | 1.057 | (1.017, 1.098) | 0.005 |
| % Poverty | 1.041 | (1.008, 1.076) | 0.016 |
| Variable | Estimated RR | 95% Confidence Interval | p Value |
|---|---|---|---|
| Heat day | 1.190 | (1.093, 1.295) | <0.001 |
| % Impervious surfaces | 1.015 | (1.001, 1.029) | 0.037 |
| % Population ≥ 65 years old | 1.057 | (1.017, 1.098) | 0.005 |
| % Poverty | 1.041 | (1.008, 1.076) | 0.016 |
| Interaction between heat and % impervious surfaces | 0.997 | (0.994, 0.999) | 0.007 |
| Heat day | 1.006 | (0.855, 1.184) | 0.941 |
| % Impervious surfaces | 1.015 | (1.001, 1.029) | 0.039 |
| % Population ≥ 65 years old | 1.056 | (1.016, 1.098) | 0.005 |
| % Poverty | 1.041 | (1.008, 1.076) | 0.016 |
| Interaction between heat and % population ≥ 65 years old | 1.005 | (0.992, 1.019) | 0.446 |
| Heat day | 1.225 | (1.130, 1.327) | <0.001 |
| % Impervious surfaces | 1.015 | (1.001, 1.029) | 0.038 |
| % Population ≥ 65 years old | 1.057 | (1.017, 1.098) | 0.005 |
| % Poverty | 1.042 | (1.008, 1.077) | 0.014 |
| Interaction between heat and % poverty | 0.988 | (0.981, 0.994) | <0.001 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
DeVine, A.C.; Vu, P.T.; Yost, M.G.; Seto, E.Y.W.; Busch Isaksen, T.M. A Geographical Analysis of Emergency Medical Service Calls and Extreme Heat in King County, WA, USA (2007–2012). Int. J. Environ. Res. Public Health 2017, 14, 937. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph14080937
DeVine AC, Vu PT, Yost MG, Seto EYW, Busch Isaksen TM. A Geographical Analysis of Emergency Medical Service Calls and Extreme Heat in King County, WA, USA (2007–2012). International Journal of Environmental Research and Public Health. 2017; 14(8):937. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph14080937
Chicago/Turabian StyleDeVine, Aubrey C., Phuong T. Vu, Michael G. Yost, Edmund Y. W. Seto, and Tania M. Busch Isaksen. 2017. "A Geographical Analysis of Emergency Medical Service Calls and Extreme Heat in King County, WA, USA (2007–2012)" International Journal of Environmental Research and Public Health 14, no. 8: 937. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph14080937