
Trauma Affecting Asian-Pacific Islanders in the San Francisco Bay Area



{kind=link}
Abstract
:1. Introduction
1.1. Background and Significance
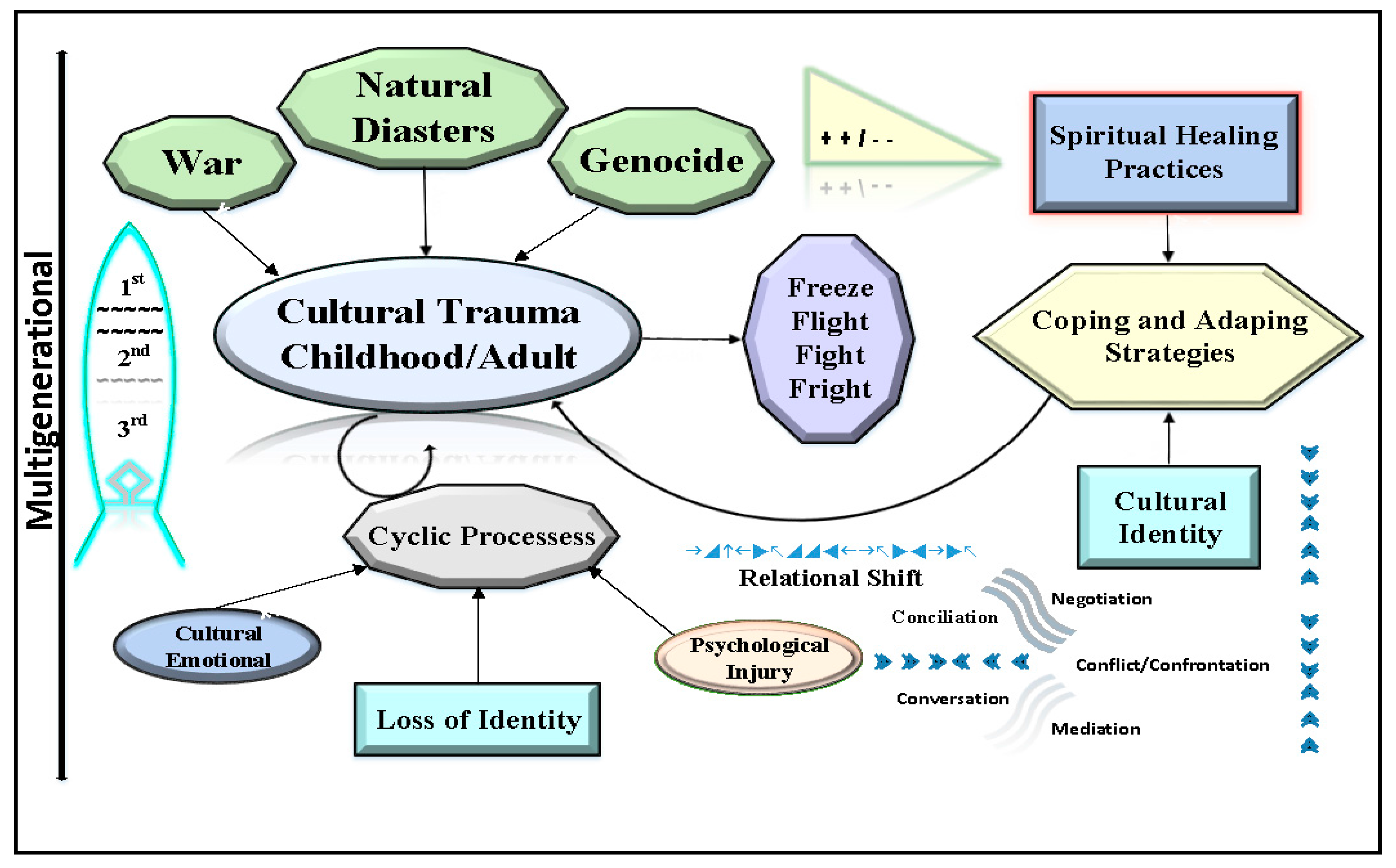
1.2. Conceptual Framework
1.3. Transgenerational and Complex Trauma (Complex Posttraumatic Stress Disorder)
1.4. Cultural Trauma
1.5. Evolutionary Perspective
1.6. Freeze, Flight, Fight, and Fright
1.7. Mental Health Problems and Treatment
2. Materials and Methods
2.1. Secondary Sources
2.2. Field Observations
2.3. Methodology
3. Results
3.1. Group Observations Overview
3.1.1. Group One
3.1.2. Group Two
3.1.3. Group Three
3.2. General Findings
3.2.1. Migration Experience
3.2.2. Western Modality, Treatments, and Side-Effects
3.2.3. Symptoms and Experiences Related to War
3.2.4. Daily Challenges and Barriers
3.2.5. Healing through Art
3.3. Secondary Findings
3.3.1. Client Demographic and Diagnoses
3.3.2. General Findings
Rates of PTSD and Diagnosis Complications
Trauma Manifestation and Perceived Psychological Control
Trauma, Stigma and Daily Challenges
3.4. Challenges of Western Modalities vs. Eastern Philosophies
3.5. Contrast with Other Immigrant/Refugee Groups
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Asian-Pacific Institute on Gender-Based Violence. Census Data & API Identities; Asian-Pacific Institute on Gender-Based Violence: Oakland, CA, USA, 2015. [Google Scholar]
- Yoshihama, M.; Dabby, C. Facts & Stats Report: Domestic Violence in Asian & Pacific Islander Homes; Asian & Pacific Islander Institute on Domestic Violence: San Francisco, CA, USA, 2014. [Google Scholar]
- U.S. Department of Health & Human Services. Reports of the Surgeon General, U.S. Public Health Service; U.S. Department of Health & Human Services: Washington, DC, USA, 2001.
- He, S. Asian American Mental Health Disparities and Cultural Psychiatry; Office for Research on Disparities and Global Mental Health, National Institute of Mental Health: Washington, DC, USA, 2015; p. 82. [Google Scholar]
- Cheng, A.W.; Chang, J.; O’Brien, J.; Budgazad, M.S.; Tsai, J. Model Minority Stereotype: Influence on Perceived Mental Health Needs of Asian Americans. J. Immigr. Minor. Health 2017, 19, 572–581. [Google Scholar] [CrossRef] [PubMed]
- Kwok, J. Factors that influence the diagnoses of Asian Americans in mental health: An exploration. Perspect. Psychiatr. Care 2013, 49, 288–292. [Google Scholar] [CrossRef] [PubMed]
- Kim, P.Y.; Lee, D. Internalized model minority myth, Asian values, and help-seeking attitudes among Asian American students. Cult. Divers. Ethn. Minor. Psychol. 2014, 20, 98–106. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, J. Trauma Trails, Recreating Song Lines: The Transgenerational Effects of Trauma in Indigenous Australia; Spinifex Press: North Melbourne, Australia, 2002. [Google Scholar]
- Chung, S.; Mikrogianakis, A.; Wales, P.W.; Dirks, P.; Shroff, M.; Singhal, A.; Grant, V.; Hancock, B.J.; Creery, D.; Atkinson, J.; et al. Trauma association of Canada Pediatric Subcommittee National Pediatric Cervical Spine Evaluation Pathway: Consensus guidelines. J. Trauma 2011, 70, 873–884. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, J.; Nelson, J.; Atkinson, C. Trauma, transgenerational transfer and effects on community wellbeing. In Working Together: Aboriginal and Torres Strait Islander Mental Health and Wellbeing Principles and Practice; Purdie, N., Dudgeon, P., Walker, R., Eds.; Australian Government Department of Health and Ageing: Canberra, Australia, 2010; pp. 135–144. [Google Scholar]
- Schwarz, E.D.; Perry, B.D. The post-traumatic response in children and adolescents. Psychiatr. Clin. N. Am. 1994, 17, 311–326. [Google Scholar]
- Courtois, C.A.; Ford, J.D. Defining and understanding complex trauma and complex traumatic stress disorders. In Treating Complex Traumatic Stress Disorders (Adults). Scientific Foundations and Therapeutic Models; Guilford Publications: New York, NY, USA, 2013. [Google Scholar]
- Ho, J. Community violence exposure of Southeast Asian American adolescents. J. Interpers. Violence 2008, 23, 136–146. [Google Scholar] [CrossRef] [PubMed]
- Ima, K.; Hohm, C.F. Child maltreatment among Asian and Pacific Islander refugees and immigrants: The San Diego case. J. Interpers. Violence 1991, 6, 267–285. [Google Scholar] [CrossRef]
- Han, M. Relationship Among Perceived Parental Trauma, Parental Attachment, and Sense of Coherence in Southeast Asian American College Students. J. Fam. Soc. Work 2006, 9, 25–45. [Google Scholar] [CrossRef]
- Ford, J.D.; Courtois, C.A. Complex PTSD, affect dysregulation, and borderline personality disorder. Borderline Pers. Disord. Emot. Dysregul. 2014, 1, 9. [Google Scholar] [CrossRef] [PubMed]
- Cloitre, M.; Garvert, D.W.; Brewin, C.R.; Bryant, R.A.; Maercker, A. Evidence for proposed ICD-11 PTSD and complex PTSD: A latent profile analysis. Eur. J. Psychotraumatol. 2013, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbara, W.K.Y. The Social and Cultural Context of Adaptive Aging among Southeast Asian Elders. In The Cultural Context of Aging Greenwood; Praeger: New York, NY, USA, 1997; pp. 293–303. [Google Scholar]
- Young-Eisendrath, P. What Suffering Teaches; American Psychological Association and Work Projects Administration: New York, NY, USA, 1998. [Google Scholar]
- Palinkas, L.A.; Pickwell, S.M. Acculturation as a risk factor for chronic disease among Cambodian refugees in the United States. Soc. Sci. Med. 1995, 40, 1643–1653. [Google Scholar] [CrossRef]
- Mouanoutoua, V.L.; Brown, L.G. Hopkins Symptom Checklist-25, Hmong version: A screening instrument for psychological distress. J. Pers. Assess. 1995, 64, 376–383. [Google Scholar] [CrossRef] [PubMed]
- Abueg, F.R.; Chun, K.M. Traumatization Stress among Asians and Asian Americans; American Psychological Association: Washington, DC, USA, 1996. [Google Scholar]
- 4 Flight from Indochina. Available online: http://www.unhcr.org/3ebf9bad0.pdf (accessed on 20 August 2017).
- Sack, W.H.; Him, C.; Dickason, D. Twelve-year follow-up study of Khmer youths who suffered massive war trauma as children. J. Am. Acad. Child Adolesc. Psychiatry 1999, 38, 1173–1179. [Google Scholar] [CrossRef] [PubMed]
- Sack, W.H.; Clarke, G.N.; Seeley, J. Posttraumatic stress disorder across two generations of Cambodian refugees. J. Am. Acad. Child Adolesc. Psychiatry 1995, 34, 1160–1166. [Google Scholar] [CrossRef] [PubMed]
- Savin, D.; Sack, W.H.; Clarke, G.N.; Meas, N.; Richart, I. The Khmer Adolescent Project: III. A study of trauma from Thailand’s Site II refugee camp. J. Am. Acad. Child Adolesc. Psychiatry 1996, 35, 384–391. [Google Scholar] [CrossRef] [PubMed]
- Southeast Asia Resource Action Center. Southeast Asia Resource Action Center: Annual Report; Southeast Asia Resource Action Center: Washington, DC, USA, 2015. [Google Scholar]
- Sepic, M. Brought as Kids, Possibly Deported as Adults, Several Cambodians await Federal Action; MPRNEWS: Saint Paul, MN, USA, 2016. [Google Scholar]
- Ohman, A.; Mineka, S. Fears, phobias, and preparedness: Toward an evolved module of fear and fear learning. Psychol. Rev. 2001, 108, 483–522. [Google Scholar] [CrossRef] [PubMed]
- Keane, T.M.; Marshall, A.D.; Taft, C.T. Posttraumatic stress disorder: Etiology, epidemiology, and treatment outcome. Annu. Rev. Clin. Psychol. 2006, 2, 161–197. [Google Scholar] [CrossRef] [PubMed]
- Marks, I.; Tobena, A. Learning and unlearning fear: A clinical and evolutionary perspective. Neurosci. Biobehav. Rev. 1990, 14, 365–384. [Google Scholar] [CrossRef]
- Nesse, R.M. Evolutionary explanations of emotions. Hum. Nat. 1990, 1, 261–289. [Google Scholar] [CrossRef] [PubMed]
- Cantor, C. Evolution and Posttraumatic Stress: Disorders of Vigilance and Defence; Routledge: New York, NY, USA, 2005. [Google Scholar]
- Bracha, H.S.; Ralston, T.C.; Matsukawa, J.M.; Williams, A.E.; Bracha, A.S. Does “fight or flight” need updating? Psychosomatics 2004, 45, 448–449. [Google Scholar] [CrossRef] [PubMed]
- Galliano, G.; Noble, L.; Travis, L.; Puechl, C. Victim Reactions during Rape/Sexual Assault. J. Interpers. Violence 1993, 8, 109–114. [Google Scholar] [CrossRef]
- Bados, A.; Toribio, L.; Garcia-Grau, E. Traumatic events and tonic immobility. Span. J. Psychol. 2008, 11, 516–521. [Google Scholar] [CrossRef] [PubMed]
- Lerner, J.S.; Keltner, D. Fear, anger, and risk. J. Pers. Soc. Psychol. 2001, 81, 146–159. [Google Scholar] [CrossRef] [PubMed]
- Sylvers, P.; Lilienfeld, S.O.; LaPrairie, J.L. Differences between trait fear and trait anxiety: Implications for psychopathology. Clin. Psychol. Rev. 2011, 31, 122–137. [Google Scholar] [CrossRef] [PubMed]
- Nicassio, P.M. The Psychosocial Adjustment of the Southeast Asian Refugee An Overview of Empirical Findings and Theoretical Models. J. Cross-Cult. Psychol. 1985, 16, 153–173. [Google Scholar] [CrossRef]
- Schwerdtfeger, K.L.; Goff, B.S. Intergenerational transmission of trauma: Exploring mother-infant prenatal attachment. J. Trauma. Stress 2007, 20, 39–51. [Google Scholar] [CrossRef] [PubMed]
- Stewart, D.W.; Shamdasani, P.N.; Rook, D.W. Focus Groups: Theory and Practice; Sage: Thousand Oaks, CA, USA, 2007. [Google Scholar]
- Seymour, J. Combined qualitative and quantitative research designs. Curr. Opin. Support. Palliat. Care 2012, 6, 514–524. [Google Scholar] [CrossRef] [PubMed]
- Post-Traumatic Stress Disorder among Adults. Available online: https://www.nimh.nih.gov/health/statistics/prevalence/post-traumatic-stress-disorder-among-adults.shtml (accessed on 28 August 2017).
- Song, S.J.; Subica, A.; Kaplan, C.; Tol, W.; de Jong, J. Predicting the Mental Health and Functioning of Torture Survivors. J. Nerv. Ment. Dis. 2017. [Google Scholar] [CrossRef] [PubMed]
- Amnesty International Canada. Australia: Appalling Abuse, Neglect of Refugees on Nauru; Human Rights Watch: Sydney, Australia, 2016. [Google Scholar]
- Refugee Council of Australia. Australia’s Response to a World in Crisis; Refugee Council of Australia: Sydney, Australia, 2016. [Google Scholar]
- Sudhinaraset, M.; Ling, I.; To, T.M.; Melo, J.; Quach, T. Dreams deferred: Contextualizing the health and psychosocial needs of undocumented Asian and Pacific Islander young adults in Northern California. Soc. Sci. Med. 2017, 184, 144–152. [Google Scholar] [CrossRef] [PubMed]
- Wong, E.C.; Marshall, G.N.; Schell, T.L.; Berthold, S.M.; Hambarsoomians, K. Characterizing the Mental Health Care of U.S. Cambodian Refugees. Psychiatr. Serv. 2015, 66, 980–984. [Google Scholar] [CrossRef] [PubMed]
- Thikeo, M.; Florin, P.; Ng, C. Help Seeking Attitudes Among Cambodian and Laotian Refugees: Implications for Public Mental Health Approaches. J. Immigr. Minor. Health 2015, 17, 1679–1686. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.; Moeschberger, M.; Chen, M.S., Jr.; Kunn, P.; Wewers, M.E.; Guthrie, R. An acculturation scale for Southeast Asians. Soc. Psychiatry Psychiatr. Epidemiol. 1993, 28, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Casella, A. The Refugees from Vietnam: Rethinking the Issue; Sage: Thousand Oaks, CA, USA, 1989; pp. 160–174. [Google Scholar]
- Barry, W. The Refused: The Agony of the Indochina Refugees; Simon & Schuster: New York, NY, USA, 1981. [Google Scholar]
- Haing, N. A Cambodian Odyssey; MacMillan: New York, NY, USA, 1987. [Google Scholar]
- Hinton, A. Genocide, categorical certainty, and the truth: Questions from the Khmer Rouge Tribunal. J. Anal. Psychol. 2011, 56, 390–396. [Google Scholar] [CrossRef] [PubMed]
- Leary, W.M. CIA Air Operations in Laos, 1955–1974. Supporting the “Secret War”; CIA Public Affairs: Washington, DC, USA, 2008.

© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bith-Melander, P.; Chowdhury, N.; Jindal, C.; Efird, J.T. Trauma Affecting Asian-Pacific Islanders in the San Francisco Bay Area. Int. J. Environ. Res. Public Health 2017, 14, 1053. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph14091053
Bith-Melander P, Chowdhury N, Jindal C, Efird JT. Trauma Affecting Asian-Pacific Islanders in the San Francisco Bay Area. International Journal of Environmental Research and Public Health. 2017; 14(9):1053. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph14091053
Chicago/Turabian StyleBith-Melander, Pollie, Nagia Chowdhury, Charulata Jindal, and Jimmy T. Efird. 2017. "Trauma Affecting Asian-Pacific Islanders in the San Francisco Bay Area" International Journal of Environmental Research and Public Health 14, no. 9: 1053. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph14091053