Few Sex Differences in Hospitalized Suicide Attempters Aged 70 and Above

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. Major and Minor Depression
2.4. Substance Abuse or Dependence
2.5. Dementia
2.6. Physical Disability
2.7. The Comprehensive Psychopathological Rating Scale (CPRS)
2.8. Geriatric Depression Scale (GDS)
2.9. Suicide Intent Scale (SIS)
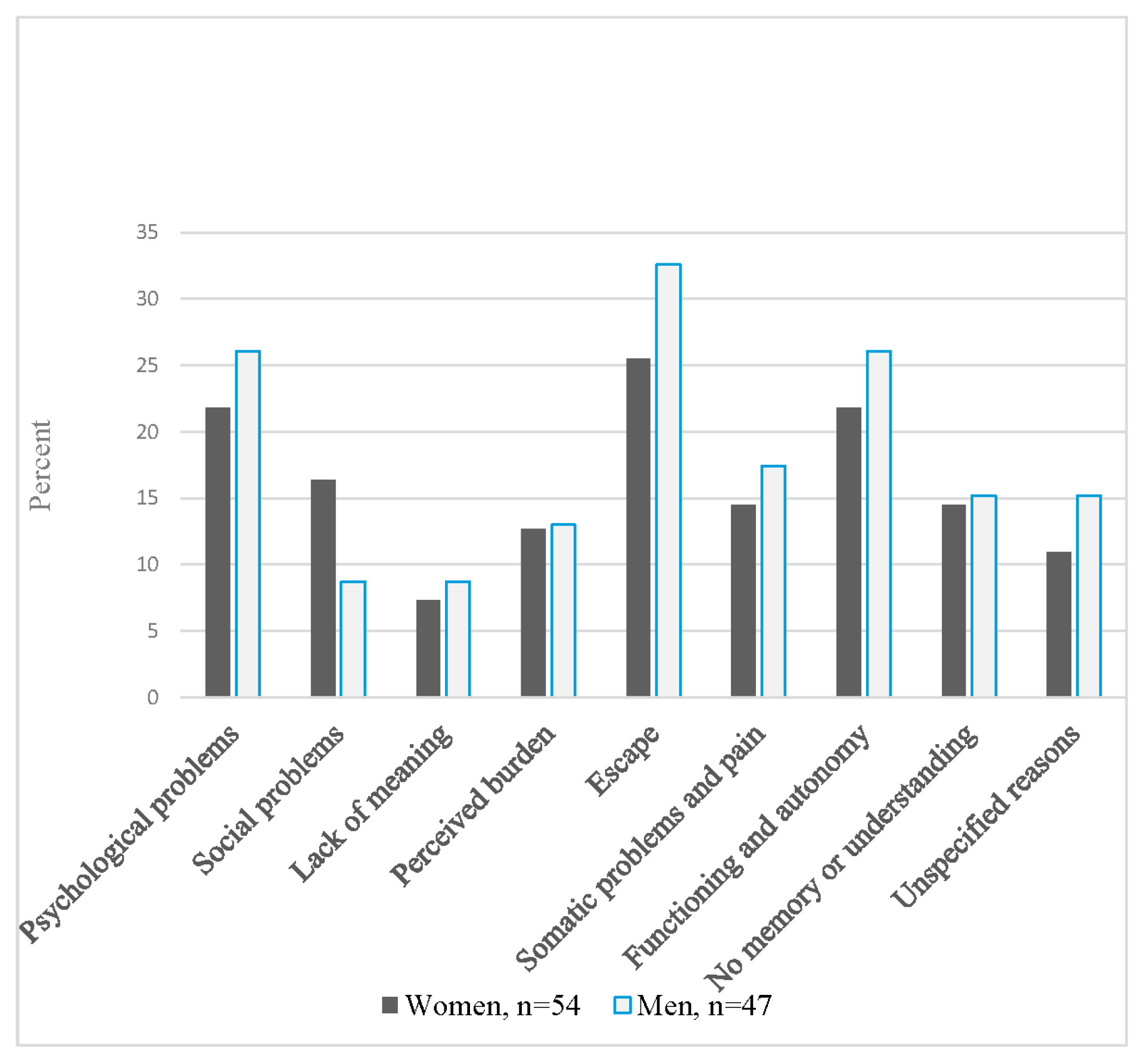
2.10. Reasons for Attempting Suicide
2.11. Ethics
2.12. Statistics
3. Results
4. Discussion
5. Methodological Considerations
6. Implications
7. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Lapierre, S.; Erlangsen, A.; Waern, M.; De Leo, D.; Oyama, H.; Scocco, P.; Quinett, P. A systematic review of elderly suicide prevention programs. Crisis 2011, 32, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Beautrais, A.L. Suicides and serious suicide attempts: Two populations or one? Psychol. Med. 2001, 31, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Arsenault-Lapierre, G.; Kim, C.; Turecki, G. Psychiatric diagnoses in 3275 suicides: A meta-analysis. BMC Psychiatry 2004, 4, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quan, H.; Arboleda-Flórez, J. Elderly suicide in Alberta: Difference by gender. Can. J. Psychiatry 1999, 44, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Oude Voshaar, R.C.; Veen, D.C.; Hunt, I.; Kapur, N. Suicide in late-life depression with and without comorbid anxiety disorders. Int. J. Geriatr. Psychiatry 2016, 31, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Schoevers, R.; Beekman, A.; Deeg, D.; Jonker, C.; Tilburg, W.V. Comorbidity and risk-patterns of depression, generalised anxiety disorder and mixed anxiety-depression in later life: Results from the AMSTEL study. Int. J. Geriatr. Psychiatry 2003, 18, 994–1001. [Google Scholar] [CrossRef] [PubMed]
- Préville, M.; Boyer, R.; Vasiliadis, H.-M.; Grenier, S.; Voyer, P.; Hudon, C.; Streiner, D.L.; Cairney, J.; Brassard, J. Study Scientific Committee of the ESA. One-year incidence of psychiatric disorders in Quebec’s older adult population. Can. J. Psychiatry 2010, 55, 449–457. [Google Scholar]
- Skoog, I. Psychiatric disorders in the elderly. Can. J. Psychiatry 2011, 56, 387–397. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, J.; Östling, S.; Waern, M.; Karlsson, B.; Sigström, R.; Guo, X.; Skoog, I. The one-month prevalence of generalized anxiety disorder according to DSM-IV, DSM-V, and ICD-10 among nondemented 75-year-olds in Gothenburg, Sweden. Am. J. Geriatr. Psychiatry 2012, 20, 963–972. [Google Scholar] [CrossRef] [PubMed]
- Waern, M.; Rubenowitz, E.; Runeson, B.; Skoog, I.; Wilhelmson, K.; Allebeck, P. Burden of illness and suicide in elderly people: Case-control study. BMJ 2002, 324, 1355. [Google Scholar] [CrossRef] [PubMed]
- Clarke, L.H.; Korotchenko, A.; Bundon, A. “The calendar is just about up”: Older adults with multiple chronic conditions reflect on death and dying. Ageing Soc. 2012, 32, 1399–1417. [Google Scholar] [CrossRef] [PubMed]
- Winterrowd, E.; Canetto, S.S.; Benoit, K. Permissive beliefs and attitudes about older adult suicide: A suicide enabling script? Aging Ment. Health 2017, 21, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Cibis, A.; Mergl, R.; Bramesfeld, A.; Althaus, D.; Niklewski, G.; Schmidtke, A.; Hegerl, U. Preference of lethal methods is not the only cause for higher suicide rates in males. J. Affect. Disord. 2012, 136, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Mergl, R.; Koburger, N.; Heinrichs, K.; Székely, A.; Tóth, M.D.; Coyne, J.; Quintão, S.; Arensman, E.; Coffey, C.; Maxwell, M. What are reasons for the large gender differences in the lethality of suicidal acts? An epidemiological analysis in four European countries. PLoS ONE 2015, 10, e0129062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freeman, A.; Mergl, R.; Kohls, E.; Szekely, A.; Gusmao, R.; Arensman, E.; Koburger, N.; Hegerl, U.; Rummel-Kluge, C. A cross-national study on gender differences in suicide intent. BMC Psychiatry 2017, 17, 234. [Google Scholar] [CrossRef] [PubMed]
- Dombrovski, A.Y.; Szanto, K.; Duberstein, P.; Conner, K.R.; Houck, P.R.; Conwell, Y. Sex differences in correlates of suicide attempt lethality in late life. Am. J. Geriatr. Psychiatry 2008, 16, 905–913. [Google Scholar] [CrossRef] [PubMed]
- Wiktorsson, S.; Runeson, B.; Skoog, I.; Östling, S.; Waern, M. Attempted suicide in the elderly: Characteristics of suicide attempters 70 years and older and a general population comparison group. Am. J. Geriatr. Psychiatry 2010, 18, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.; Davis, J.R.; Frederick, C.J.; Perlin, S.; Pokorny, A.D.; Schulman, R.E.; Seiden, R.H.; Wittlin, B.J. Classification and Nomenclature. Suicide Prevention in the Seventies; Resnick, H.L.P., Hatorne, B.C., Eds.; U.S. Government Printing Office: Washington, DC, USA, 1972.
- Folstein, M.F.; Robins, L.N.; Helzer, J.E. The mini-mental state examination. Arch. Gen. Psychiatry 1983, 40, 812. [Google Scholar] [CrossRef] [PubMed]
- Skoog, I. Psychiatric epidemiology of old age: The H70 study—The NAPE lecture 2003. Acta Psychiatr. Scand. 2004, 109, 4–18. [Google Scholar] [CrossRef] [PubMed]
- Asberg, M.; Montgomery, S.A.; Perris, C.; Schalling, D.; Sedvall, G. A comprehensive psychopathological rating scale. Acta Psychiatr. Scand. Suppl. 1978, 57, 5–27. [Google Scholar] [CrossRef]
- American Psychiatric Association (APA). Diagnostic and Statistical Manual of Mental Disorders (DSM-IV), 4th ed.; American Psychiatric Association: Washington, DC, USA, 1993. [Google Scholar]
- Skoog, I.; Nilsson, L.; Palmertz, B.; Andreasson, L.A.; Svanborg, A. A population-based study of dementia in 85-year-olds. N. Engl. J. Med. 1993, 328, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Morin, J.; Wiktorsson, S.; Marlow, T.; Olesen, P.J.; Skoog, I.; Waern, M. Alcohol use disorder in elderly suicide attempters: A comparison study. Am. J. Geriatr. Psychiatry 2013, 21, 196–203. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association (APA). Diagnostic and Statistical Manual of Mental Disorders, Revised (DSM-III-R); American Psychiatric Association: Washington, DC, USA, 1987. [Google Scholar]
- World Health Organisation (WHO). Healt Topics—Disabilities. Available online: http://www.who.int/topics/disabilities/en/ (accessed on 17 October 2017).
- Miller, M.D.; Paradis, C.F.; Houck, P.R.; Mazumdar, S.; Stack, J.A.; Rifai, A.H.; Mulsant, B.; Reynolds, C.F. Rating chronic medical illness burden in geropsychiatric practice and research: Application of the Cumulative Illness Rating Scale. Psychiatry Res. 1992, 41, 237–248. [Google Scholar] [CrossRef]
- Wiktorsson, S.; Berg, A.I.; Wilhelmson, K.; Fässberg, M.M.; Van Orden, K.; Duberstein, P.; Waern, M. Assessing the role of physical illness in young old and older old suicide attempters. Int. J. Geriatr. Psychiatry 2016, 31, 771–774. [Google Scholar] [CrossRef] [PubMed]
- Van der Laan, N.C.; Schimmel, A.; Heeren, T.J. The applicability and the inter-rater reliability of the comprehensive psychopathological rating scale in an elderly clinical population. Int. J. Geriatr. Psychiatry 2005, 20, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, S.A.; Asberg, M. A new depression scale designed to be sensitive to change. Br. J. Psychiatry 1979, 134, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Tyrer, P.; Owen, R.T.; Cicchetti, D.V. The brief scale for anxiety: A subdivision of the comprehensive psychopathological rating scale. J. Neurol. Neurosurg. Psychiatry 1984, 47, 970–975. [Google Scholar] [CrossRef] [PubMed]
- Yesavage, J.A.; Brink, T.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and validation of a geriatric depression screening scale: A preliminary report. J. Psychiatr. Res. 1982, 17, 37–49. [Google Scholar] [CrossRef]
- Gottfries, G.G.; Noltorp, S.; Norgaard, N. Experience with a Swedish version of the geriatric depression scale in primary care centres. Int. J. Geriatr. Psychiatry 1997, 12, 1029–1034. [Google Scholar] [CrossRef]
- Beck, A.T.; Resnik, H.L.P.; Lettieri, D.J. The Prediction of Suicide. Development of Suicidal Scale; Charles Press: Bowie, MD, USA, 1974; pp. 45–56. [Google Scholar]
- Niméus, A.; én, M.; Träskman-Bendz, L. High suicidal intent scores indicate future suicide. Arch. Suicide Res. 2002, 6, 211–219. [Google Scholar] [CrossRef]
- Van Orden, K.A.; Wiktorsson, S.; Duberstein, P.; Berg, A.I.; Fassberg, M.M.; Waern, M. Reasons for attempted suicide in later life. Am. J. Geriatr. Psychiatry 2015, 23, 536–544. [Google Scholar] [CrossRef] [PubMed]
- Conwell, Y.; Rotenberg, M.; Caine, E.D. Completed suicide at age 50 and over. J. Am. Geriatr. Soc. 1990, 38, 640–644. [Google Scholar] [CrossRef] [PubMed]
- Neugarten, B.L.; Gutmann, D.L. Age-Sex Roles and Personality in Middle Age: A Thematic Apperception Study; University of Chicago Press: Chicago, IL, USA, 1968; pp. 58–71. [Google Scholar]
- Fässberg, M.M.; Cheung, G.; Canetto, S.S.; Erlangsen, A.; Lapierre, S.; Lindner, R.; Draper, B.; Gallo, J.J.; Wong, C.; Wu, J. A systematic review of physical illness, functional disability, and suicidal behaviour among older adults. Aging Ment. Health 2016, 20, 166–194. [Google Scholar] [CrossRef] [PubMed]
- Fassberg, M.M.; Ostling, S.; Braam, A.W.; Backman, K.; Copeland, J.R.; Fichter, M.; Kivela, S.L.; Lawlor, B.A.; Lobo, A.; Magnusson, H.; et al. Functional disability and death wishes in older Europeans: Results from the EURODEP concerted action. Soc. Psychiatry Psychiatr. Epidemiol. 2014, 49, 1475–1482. [Google Scholar] [CrossRef] [PubMed]
- Bamonti, P.M.; Price, E.C.; Fiske, A. Depressive symptoms and suicide risk in older adults: Value placed on autonomy as a moderator for men but not women. Suicide Life Threat. Behav. 2014, 44, 188–199. [Google Scholar] [CrossRef] [PubMed]
- Sakuma, N.; Ura, C.; Miyamae, F.; Inagaki, H.; Ito, K.; Niikawa, H.; Ijuin, M.; Okamura, T.; Sugiyama, M.; Awata, S. Distribution of mini-mental state examination scores among urban community-dwelling older adults in Japan. Int. J. Geriatr. Psychiatry 2017, 32, 718–725. [Google Scholar] [CrossRef] [PubMed]
- Wiktorsson, S.; Olsson, P.; Waern, M. Medically serious and non-serious suicide attempts in persons aged 70 and above. Geriatrics 2016, 1, 23. [Google Scholar] [CrossRef]
- Hunt, K.; Sweeting, H.; Keoghan, M.; Platt, S. Sex, gender role orientation, gender role attitudes and suicidal thoughts in three generations. Soc. Psychiatry Psychiatr. Epidemiol. 2006, 41, 641–647. [Google Scholar] [CrossRef] [PubMed]
- West, C.; Zimmerman, D.H. Doing gender. Gender Soc. 1987, 1, 125–151. [Google Scholar] [CrossRef]
- Wood, W.; Eagly, A.H. 2 biosocial construction of sex differences and similarities in behavior. Adv. Exp. Soc. Psychol. 2012, 46, 55–123. [Google Scholar]
- Innamorati, M.; Tamburello, A.; Lester, D.; Amore, M.; Girardi, P.; Tatarelli, R.; Pompili, M. Inequalities in suicide rates in the European Union’s elderly: Trends and impact of macro-socioeconomic factors between 1980 and 2006. Can. J. Psychiatry 2010, 55, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Carter, M.W.; Reymann, M.R. ED use by older adults attempting suicide. Am. J. Emerg. Med. 2014, 32, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Hedna, K.; Sundell, K.A.; Hamidi, A.; Skoog, I.; Gustavsson, S.; Waern, M. Antidepressants and suicidal behaviour in late life: A prospective population-based study of use patterns in new users aged 75 and above. Eur. J. Clin. Pharmacol. 2018, 74, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Oslin, D.W.; Pettinati, H.; Volpicelli, J.R. Alcoholism treatment adherence: Older age predicts better adherence and drinking outcomes. Am. J. Geriatr. Psychiatry 2002, 10, 740–747. [Google Scholar] [CrossRef] [PubMed]
- Sen, A. The Idea of Justice; Harvard University Press: Cambridge, MA, USA, 2011. [Google Scholar]


{kind=link}
| Characteristics | Women n = 56 | Men n = 47 | Test Results a,b | ||
|---|---|---|---|---|---|
| n | (%) | n | (%) | p-Value | |
| Sociodemographics | |||||
| Married/cohabiting | 15 | (26.8) | 18 | (38.3) | 0.289 |
| Living alone | 41 | (73.2) | 29 | (61.7) | 0.289 |
| Living in an institution | 4 | (7.1) | 2 | (4.3) | 0.686 |
| Education, only mandatory | 31 | (55.4) | 27 | (57.4) | 0.845 |
| Clinical Characteristics | |||||
| Major depression | 38 | (67.9) | 30 | (63.8) | 0.682 |
| Minor depression | 13 | (23.2) | 14 | (29.8) | 0.504 |
| Alcohol/substance use disorder c | 8 | (14.3) | 21 | (44.7) | 0.001 |
| Dementia | 4 | (7.1) | 4 | (8.5) | 1.000 |
| Hopelessness | 36 | (67.9) | 19 | (43.8) | 0.023 |
| Psychiatric treatment c | 34 | (60.7) | 27 | (57.4) | 0.841 |
| Current antidepressant prescription | 36 | (64.3) | 26 | (55.3) | 0.421 |
| Previous suicide attempt | 23 | (41.1) | 14 | (29.8) | 0.303 |
| Violent method at index attempt d | 16 | (28.6) | 13 | (27.7) | 1.000 |
| Any serious physical disability e | 34 | (60.7) | 25 | (53.2) | 0.549 |
| CPRS-Symptoms | Women n = 56 | Men n = 47 | Test Results b | ||
|---|---|---|---|---|---|
| n | (%) | n | (%) | p-Value | |
| Depressive Symptoms | |||||
| Sadness (reported) | 47 | (83.9) | 43 | (93.5) | 0.217 |
| Sadness (observed) | 49 | (87.5) | 41 | (87.2) | 1.000 |
| Inability to feel | 44 | (80.0) | 37 | (80.4) | 1.000 |
| Pessimistic thoughts | 33 | (60.0) | 30 | (63.8) | 0.838 |
| Hostile feelings | 11 | (20.4) | 10 | (22.4) | 1.000 |
| Suicidal thoughts | 49 | (89.1) | 41 | (89.1) | 1.000 |
| Anxiety Symptoms | |||||
| Inner tension | 28 | (51.9) | 18 | (40.0) | 0.312 |
| Worrying over trifles | 32 | (59.3) | 22 | (48.9) | 0.319 |
| Autonomic disturbances | 12 | (22.2) | 5 | (11.1) | 0.185 |
| Muscular tension (reported) | 27 | (49.1) | 14 | (31.1) | 0.102 |
| Cognitive Symptoms | |||||
| Failing memory | 36 | (65.5) | 26 | (57.8) | 0.535 |
| Fatiguability | 43 | (78.2) | 32 | (71.1) | 0.489 |
| Indecision | 25 | (45.5) | 14 | (31.1) | 0.156 |
| Lassitude | 41 | (75.9) | 32 | (71.1) | 0.650 |
| Concentration difficulties | 27 | (50.0) | 25 | (55.6) | 0.687 |
| Somatic Symptoms | |||||
| Aches and pain | 29 | (53.7) | 23 | (51.1) | 0.842 |
| Reduced sleep | 22 | (40.7) | 17 | (37.8) | 0.838 |
| Reduced appetite | 26 | (47.3) | 21 | (45.7) | 1.000 |
| Number of Symptoms by Group | |||||
| Women | Men | Test Results c | |||
| Median | Median | Z-value | p-value | ||
| Depressive symptoms | 5 | 5 | −0.585 | 0.559 | |
| Anxiety symptoms | 2 | 1 | −1.673 | 0.094 | |
| Cognitive symptoms | 1 | 1 | −1.009 | 0.313 | |
| Somatic symptoms | 0 | 0 | −0.375 | 0.708 | |
| Rating Scales | Women n = 56 | Men n = 47 | Test Results a,b | |||||
|---|---|---|---|---|---|---|---|---|
| Mean SD | Mean SD | t | df | p-Value | Cohen’s d | |||
| Montgomery-Asberg Depression Rating Scale (MADRS) | 26.6 | 11.3 | 26.4 | 11.4 | −0.08 | 95 | 0.939 | 0.02 |
| Geriatric Depression Scale (GDS) | 10.1 | 4.5 | 9.3 | 5.0 | −0.76 | 95 | 0.448 | 0.17 |
| Brief Scale for Anxiety (BSA) | 10.2 | 6.1 | 8.4 | 5.0 | −1.56 | 96 | 0.122 | 0.32 |
| Mini Mental State Examination (MMSE) | 24.8 | 3.8 | 26.5 | 2.7 | 2.48 | 95 | 0.015 | −0.52 |
| Suicide Intent Scale (SIS) | ||||||||
| Women | Men | Test Results c | ||||||
| Median | Median | Z-value | p-value | |||||
| SIS total score | 17 | 17 | −0.521 | 0.602 | ||||
| SIS objective score | 5.5 | 6 | −0.585 | 0.559 | ||||
| SIS subjective score | 11 | 11 | −0.167 | 0.867 | ||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wiktorsson, S.; Rydberg Sterner, T.; Mellqvist Fässberg, M.; Skoog, I.; Ingeborg Berg, A.; Duberstein, P.; Van Orden, K.; Waern, M. Few Sex Differences in Hospitalized Suicide Attempters Aged 70 and Above. Int. J. Environ. Res. Public Health 2018, 15, 141. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15010141
Wiktorsson S, Rydberg Sterner T, Mellqvist Fässberg M, Skoog I, Ingeborg Berg A, Duberstein P, Van Orden K, Waern M. Few Sex Differences in Hospitalized Suicide Attempters Aged 70 and Above. International Journal of Environmental Research and Public Health. 2018; 15(1):141. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15010141
Chicago/Turabian StyleWiktorsson, Stefan, Therese Rydberg Sterner, Madeleine Mellqvist Fässberg, Ingmar Skoog, Anne Ingeborg Berg, Paul Duberstein, Kimberly Van Orden, and Margda Waern. 2018. "Few Sex Differences in Hospitalized Suicide Attempters Aged 70 and Above" International Journal of Environmental Research and Public Health 15, no. 1: 141. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15010141