1. Introduction
The increase in antibiotic resistance has been acknowledged as one of the top three greatest threats to global health in our time [
1]. In 2014, the World Health Organization (WHO) published a report on the global surveillance of antimicrobial resistance [
2]. Mapping of the availability of national surveillance data on antimicrobial resistance worldwide showed large gaps, particularly in Africa and South and South-East Asia, which is of great concern. Without such data, we will not know the scope of the problem, we will not know where to put our efforts and we will not be able to detect new trends and threats. In the Global Action Plan on Antimicrobial Resistance (GAP-AMR, with special emphasis on antibiotic resistance) adopted by the World Health Assembly in May 2015, one of the objectives is to strengthen the knowledge and evidence base through surveillance and research [
3]. As a response to the GAP-AMR, the WHO has launched an initiative called the Global Antimicrobial Resistance Surveillance System (GLASS) that aims to establish a global standardized approach to the collection of, analysis and sharing of data [
4]. Setting up a national surveillance system can be a challenge to many countries, particularly in countries where health systems are weak. In addition to the costs of running a laboratory of high standards, there is a need for skilled personnel and standardized methods that allow for comparisons of resistance proportions between countries.
Since a national surveillance system is lacking in India, there is a great need for long-term studies on the proportions and trends in antibiotic resistance. Several long-term studies from India have found high antibiotic resistance proportions, but most of these studies are single-site studies or cover shorter periods of time [
5,
6,
7,
8,
9,
10,
11]. Recently, a retrospective study over seven years from a private laboratory network in India concluded that there are high proportions of resistant bacterial strains among blood culture isolates from patients across India [
12].
High proportions of resistant Gram-negative bacterial strains are of great concern since there are few treatment options left, especially for the extended-spectrum cephalosporin and carbapenem-resistant E. coli and Klebsiella spp. strains. In this study, we have examined the trends in resistance to extended-spectrum cephalosporins and carbapenems among clinical E. coli and Klebsiella spp. isolates in the district of Nashik in Western India over an 11-year period (2004–2014).
4. Discussion
We have examined data on antibacterial susceptibility over an 11-year period among
E. coli and
Klebsiella spp. isolates from community- and hospital-acquired infections in the district of Nashik in Western India. High proportions of extended-spectrum cephalosporin and carbapenem non-susceptible isolates, as well as high proportions of ESBL-producing isolates were found for both
E. coli and
Klebsiella spp. In our data, we observed that the proportions of non-susceptible bacterial isolates did not show a steady increase or decrease over time. Rather, the proportions fluctuated over time. This has also been observed in other long-term studies of trends in antibiotic resistance [
5,
22,
23,
24] and might reflect differences in the annual burden of infections, changes over time in the choice of empiric drugs for treatment of infections and changes in the study population.
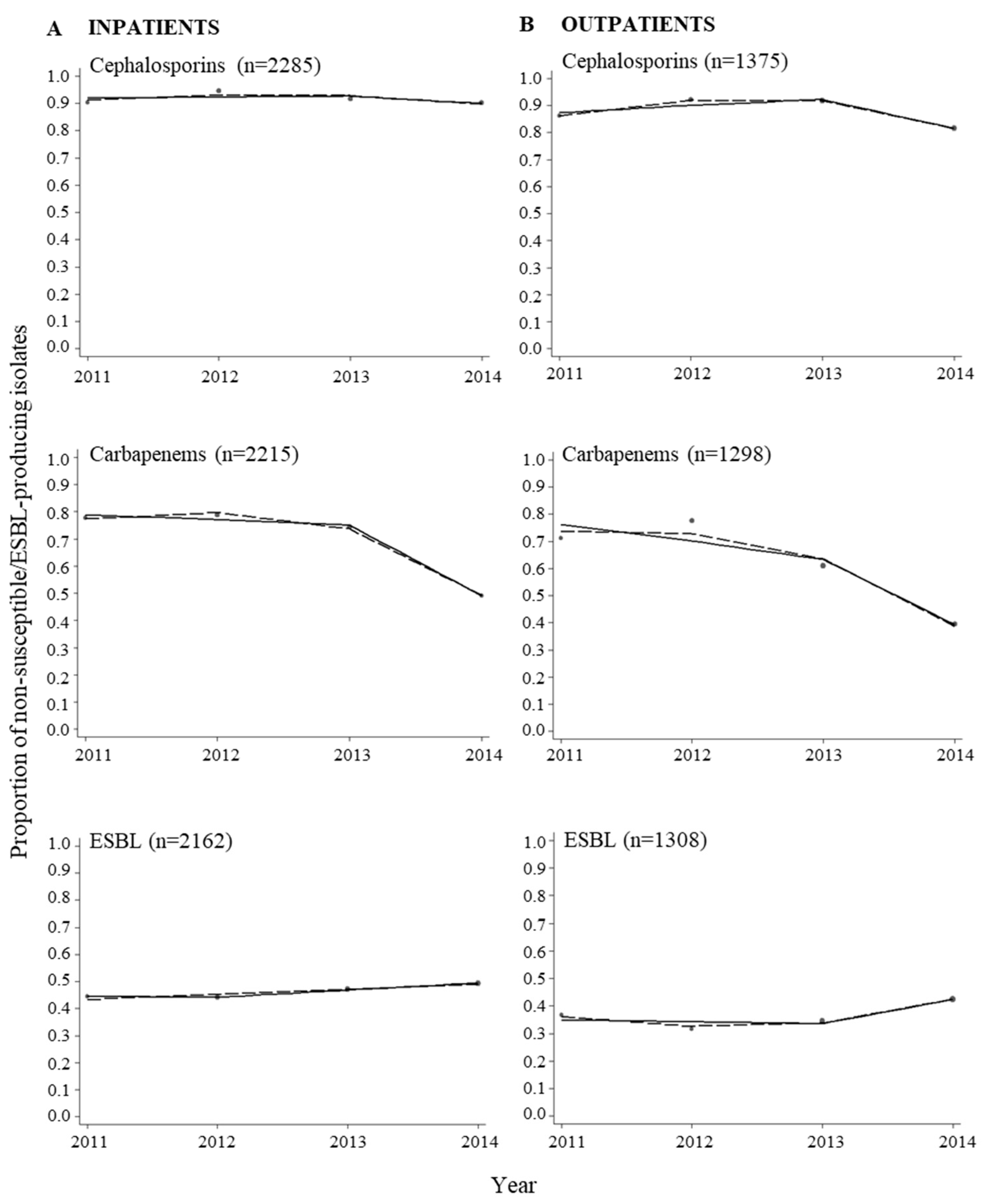
We found that the proportions of non-susceptible isolates were higher in inpatients compared to outpatients. Higher prevalence of resistance among bacterial isolates from inpatients compared to outpatients has also been found in other studies [
25,
26]. Higher prevalence of resistance was also found among bacterial isolates from males compared to females. The differences observed between males and females could be due to differences in exposure to bacterial pathogens and/or antibiotics. Differences in the proportions of non-susceptible isolates were also found when comparing urinary samples and all other specimen types for both
E. coli and
Klebsiella spp. Lower proportions of non-susceptible isolates from urinary samples might reflect that cephalosporins and carbapenems are not recommended as first line treatment of urinary tract infections. Despite lower proportions of non-susceptible isolates among urinary samples compared to other specimen types, the proportions are alarmingly high. Analysis of nitrofurantoin non-susceptible
E. coli isolates during the period 2004–2014 revealed that the non-susceptibility proportions ranged from 4.9–39.8% (data not shown). The lower prevalence of resistant
E. coli isolates observed for nitrofurantoin, one of the drugs recommended as first line treatment of urinary tract infections [
27], compared to cephalosporins and carbapenems might indicate irrational use of antibiotics to treat urinary tract infections.
To analyse the trends in proportions of non-susceptible isolates, we modelled calendar time using two different approaches, namely a multivariable regression spline model to flexibly model time without constraints and a piece-wise linear spline to summarize the overall change of non-susceptibility over time. Using these approaches, we were able to detect a point in time where a change in the proportions of non-susceptible isolates most probably occurred. In some cases, the MVRS approach indicated complicated trends with probably more than a single point of change in slope. For example, for ESBL-producing
E. coli and
Klebsiella spp. (
Figure 2), the year 2009 was chosen as the knot year (
Table 1) resulting in an increasing trend in ESBL-producing isolates before 2009 and a decreasing trend after 2009. From the graph showing the predicted proportions from the MVRS approach, an increasing trend was predicted up to the year 2009, followed by a decreasing trend to the year 2012 in
E. coli and 2012–2013 in
Klebsiella spp., and then an increasing trend from 2012 and 2013, respectively. It would be possible to choose more than one knot to detect more than one change in the trend, but we wanted to grasp the major changes and therefore chose to use one knot in our analyses.
The years 2009, 2012, and 2013 were identified as the years where a change in the odds of bacterial isolates being non-susceptible or ESBL-producing most likely occurred (
Table 1). In the period following these years, decreasing trends in non-susceptible and ESBL-producing isolates were detected for both
E. coli and
Klebsiella spp. Since we did not have data on antibiotic consumption, neither from the individual patient nor at the aggregated level from the district of Nashik, we can only speculate about the reason for this observation. The WHO selected antimicrobial resistance as theme for World Health Day 2011 [
28], and in accordance to this activity directed towards physicians were conducted in the district of Nashik in order to promote rational use of antibiotics. This was done through the Indian Initiative of Management of Antibiotic Resistance (IIMAR) [
29]. IIMAR activities were continued further in the program of the Antibiotic Stewardship Network in India [
30] in 2013–2014 in the Nashik district. These activities were focusing on proper use of antibiotics, particularly prescription of last resort antibiotics, like carbapenems, to treat infections caused by Gram-negative bacteria (unpublished information). Many factors influence prescribing decisions, and raising awareness and knowledge among physicians have been shown to be important to improve the prescribing of antibiotics [
31,
32]. The decreasing trends in non-susceptible and ESBL-producing isolates observed in the last part of the study period might be attributed to these activities, and also to the increased focus on antibiotic resistance in general, both in India and the rest of the world [
2,
27,
33].
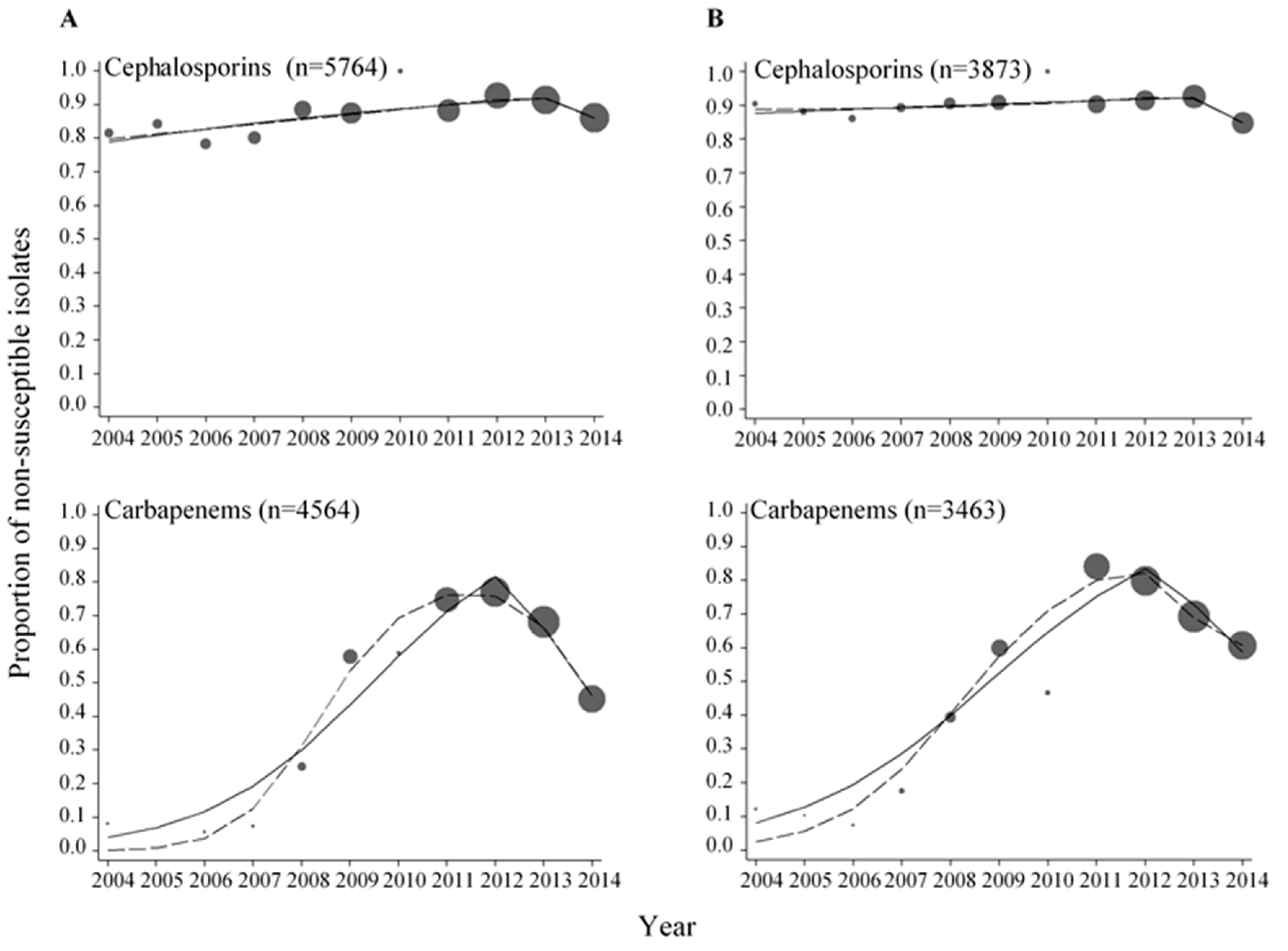
High proportions of extended-spectrum cephalosporin and carbapenem non-susceptible isolates were observed in this study. For the extended-spectrum cephalosporins, the proportions of non-susceptible
E. coli and
Klebsiella spp. isolates were above 78.4% and 84.9%, respectively, throughout the period 2004–2014. For the carbapenems, there were much more variations in the proportions of non-susceptible
E. coli and
Klebsiella spp. isolates. Most samples were collected from 2008 and onwards which reflects the increasing use of carbapenems in the recent years due to increased availability and reduced cost of these drugs (unpublished information). Similar proportions of extended-spectrum cephalosporin and carbapenem non-susceptible isolates have been reported in other studies from India [
10,
12,
34]. The high proportions of inpatients (or only inpatients) in the study populations can explain the high proportions of resistance observed in these studies. A study on the proportions of resistance in bacteria isolated from urine in individuals in the community in Northern India revealed low proportions for extended-spectrum cephalosporins, and no resistance towards carbapenems [
35].
The proportions of extended-spectrum cephalosporin and carbapenem non-susceptible isolates found in this study are alarmingly high. In Europe, where most countries have national surveillance systems, the population-weighted mean resistance percentages in 2014 were 12% for extended-spectrum cephalosporins and <0.1% for carbapenems among invasive
E. coli isolates. Among invasive
Klebsiella spp. isolates the percentages were 28% and 7.3%, respectively [
36]. Like in India there are variations in the proportions of resistance reported by various regions of Europe, with highest resistance proportions reported from southern and south-eastern Europe.
Of particular concern are the high proportions of ESBL-producing isolates found both in
E. coli and
Klebsiella spp. High proportions of ESBL-producing bacteria and a rapid increase in recent years have also been observed in other studies from India [
5,
6,
7,
37,
38]. The high proportions found are worrisome since there are few treatment options left to treat infections caused by these bacteria, particularly if there is also resistance to carbapenems.
Strengths and Limitations
The data analysed in this study are unique, since longitudinal surveillance data from India are scarce. The data were collected over an 11-year period and analysed at the same laboratory. Although there could be changes in staff and laboratory practices over time, the fact that the same laboratory performed all antibacterial susceptibility testing minimizes the risk for bias due to methodological issues. The availability of data on type of patient made it possible to distinguish between inpatients and outpatients in the period 2011–2014. The use of regression splines instead of using the overall linear trend allowed for more robust analysis of the trends in non-susceptibility over time. A limitation to our study is that a large proportion of the data was collected during the second half of the study period, making the estimates for the first half of the period less robust compared to estimates from the second half of the study period. No patient identifiers were available in the data set meaning that the number of patients included in the study was not known.

 ,
, 


{kind=link}
{kind=link}
{kind=link}
{kind=link}

