Evaluation of a Brief Intervention for Promoting Mental Health among Employees in Social Enterprises: A Cluster Randomized Controlled Trial

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Intervention Description
2.1.1. Development of the Intervention
2.1.2. Specific Content of the Intervention
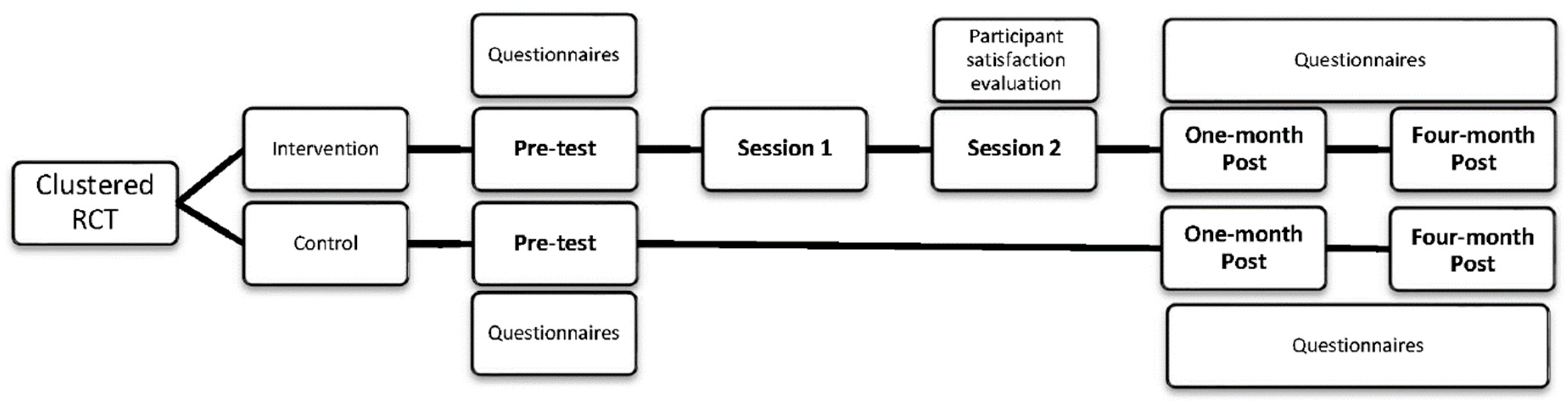
2.2. Study Design
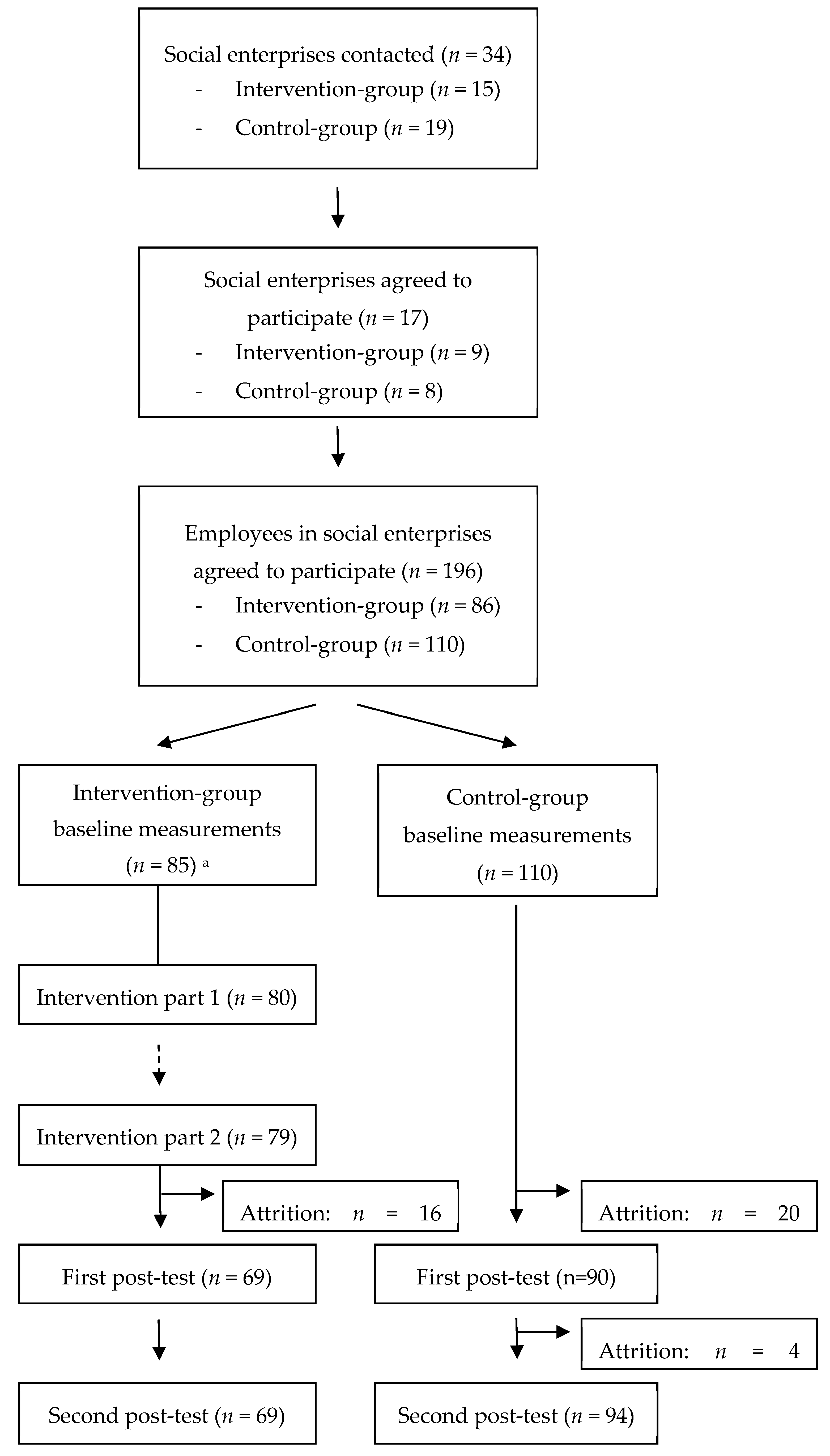
2.3. Sample Description and Attrition
2.4. Data Collection Procedures
2.5. Measures
2.5.1. Sociodemographics
2.5.2. Effectiveness Evaluation
Empowerment
Resilience
Palliative Behavior
Determinants of Coping Strategies
Quality of Life and Life Satisfaction
Participants’ Satisfaction with the Intervention
2.6. Data Analysis
3. Results
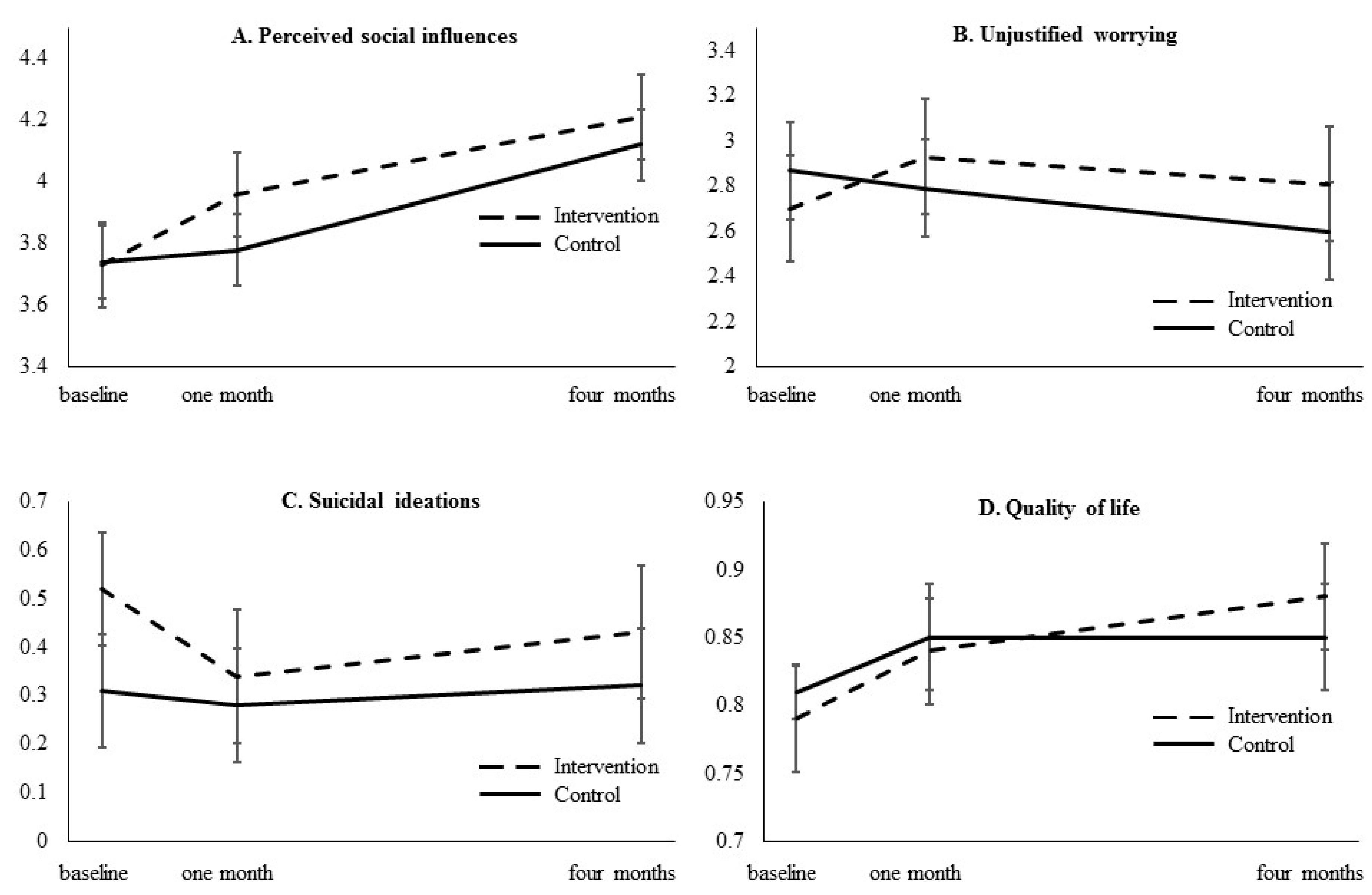
3.1. Effectiveness Evaluation
3.2. Participant Satisfaction with the Intervention
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kröger, H.; Pakpahan, E.; Hoffmann, R. What causes health inequality? A systematic review on the relative importance of social causation and health selection. Eur. J. Public Health 2015, 25, 951–960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mithen, J.; Aitken, Z.; Ziersch, A.; Kavanagh, A.M. Inequalities in social capital and health between people with and without disabilities. Soc. Sci. Med. 2015, 126, 26–35. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization and World Bank Group. World Report on Disability; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- Iezzoni, L. Public health goals for persons with disabilities: Looking ahead to 2020. Disabil. Health J. 2009, 2, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Van Schrojenstein Lantman-de Valk, H.M.; Walsh, P.N. Managing health problems in people with intellectual disabilities. BMJ 2008, 337, 1408–1412. [Google Scholar] [CrossRef] [PubMed]
- Kavanagh, A.; Aitken, Z.; Emerson, E.; Sahabandu, S.; Milner, A.; Bentley, R.; LaMontagne, A.D.; Pirkis, J.; Studdert, D. Inequalities in socio-economic characteristics and health and wellbeing of men with and without disabilities: A cross-sectional analysis of the baseline wave of the Australian Longitudinal. BMC Public Health 2016, 16 (Suppl. S3), 1042. [Google Scholar] [CrossRef]
- Hublet, A.; Maes, L.; De Bourdeaudhuij, I. Haalbaarheidsstudie Sociale Economie en Gezondheidspromotie (StEIGERs) [Feasibility Study Social Economy and Health Promotion]; Steunpunt Welzijn, Volksgezondheid en Gezin: Leuven, Belgium, 2013. [Google Scholar]
- Rimmer, J.H. Health promotion for people with disabilities: The emerging paradigm shift from disability prevention to prevention of secondary conditions. Phys. Ther. 1999, 79, 495–502. [Google Scholar] [PubMed]
- Prince, M.; Patel, V.; Saxena, S.; Maj, M.; Maselko, J.; Phillips, M.R.; Rahman, A. No health without mental health. Lancet 2007, 370, 859–877. [Google Scholar] [CrossRef]
- Friedli, L. Mental Health, Resilience and Inequalities; World Health organization Regional office for Europe: Copenhagen, Denmark, 2009. [Google Scholar]
- Naaldenberg, J.; Kuijken, N.; van Dooren, K.; de Valk, H.V.S.L. Topics, methods and challenges in health promotion for people with intellectual disabilities: A structured review of literature. Res. Dev. Disabil. 2013, 34, 4534–4545. [Google Scholar] [CrossRef] [PubMed]
- Ervin, D.A.; Hennen, B.; Merrick, J.; Morad, M. Healthcare for persons with intellectual and developmental disability in the community. Front. Public Health 2014, 2, 83. [Google Scholar] [CrossRef]
- Heller, T.; Fisher, D.; Marks, B.; Hsieh, K. Interventions to promote health: Crossing networks of intellectual and developmental disabilities and aging. Disabil. Health J. 2014, 7, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Rimmer, J.H.; Vanderbom, K.A.; Bandini, L.G.; Drum, C.E.; Luken, K.; Suarez-Balcazar, Y.; Graham, I.D. GRAIDs: A framework for closing the gap in the availability of health promotion programs and interventions for people with disabilities. Implement. Sci. 2014, 9, 100. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, A.; Moreno-Péral, P.; Zabaleta-del-Olmo, E.; Bellon, J.A.; Aranda-Regules, J.M.; Luciano, J.V.; Serrano-Blanco, A.; Rubio-Valera, M. Is there a case for mental health promotion in the primary care setting? A systematic review. Prev. Med. 2015, 76, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Lunsky, Y. The impact of stress and social support on the mental health of individuals with intellectual disabilities. Salud Publica Mex. 2008, 50, 51–53. [Google Scholar] [CrossRef]
- Arneson, H.; Ekberg, K. Evaluation of empowerment processes in a workplace health promotion intervention based on learning in Sweden. Health Promot. Int. 2005, 20, 351–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barry, M.M.; Clarke, A.M.; Jenkins, R.; Patel, V. A systematic review of the effectiveness of mental health promotion interventions for young people in low and middle income countries. BMC Public Health 2013, 13, 835. [Google Scholar] [CrossRef] [PubMed]
- Alegría, M.; Polo, A.; Gao, S.; Santana, L.; Rothstein, D.; Jimenez, A.; Hunter, M.L.; Mendieta, F.; Oddo, V.; Normand, S.L. Evaluation of a patient activation and empowerment intervention in mental health care. Med. Care 2008, 46, 247–256. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Ottawa Charter of Health Promotion; WHO: Geneva, Switzerland, 1986. [Google Scholar]
- Van Opstal, W.; Deraedt, E.; Gijselinckx, C. Monitoring Profile Shifts and Differences among WISEs in Flanders. Soc. Enterp. J. 2009, 5, 229–258. [Google Scholar] [CrossRef] [Green Version]
- BDO. POP in de Sociale Economie [POP in the Social Economy]. Available online: http://www.bdo.be/nl/special-advisory-services/management-advisory/hr-tools/pop-in-de-sociale-economie/ (accessed on 7 April 2012).
- Kuoppala, J.; Lamminpää, A.; Husman, P. Work health promotion, job well-being, and sickness absences: A systematic review and meta-analysis. J. Occup. Environ. Med. 2008, 50, 1216–1227. [Google Scholar] [CrossRef]
- Sun, J.; Buys, N.; Wang, X. Effectiveness of a Workplace-Based Intervention Program to Promote Mental Health among Employees in Privately Owned Enterprises in China. Popul. Health Manag. 2013, 16, 406–414. [Google Scholar] [CrossRef]
- Rees, C.S.; Breen, L.J.; Cusack, L.; Hegney, D. Understanding individual resilience in the workplace: The international collaboration of workforce resilience model. Front. Psychol. 2015, 6, 73. [Google Scholar] [CrossRef]
- Segal, S. The great integration debate: Part 2. Br. J. Learn. Disabil. 1993, 21, 109–111. [Google Scholar] [CrossRef]
- Goldgruber, J.; Ahrens, D. Effectiveness of workplace health promotion and primary prevention interventions: A review. J. Public Health 2010, 18, 75–88. [Google Scholar] [CrossRef]
- Hogan, S.E.; Evers, S.E. A nutritional rehabilitation program for persons with severe physical and developmental disabilities. J. Am. Diet. Assoc. 1997, 97, 162–166. [Google Scholar] [CrossRef]
- Messent, P.R.; Cooke, C.B.; Long, J. Primary and secondary barriers to physically active healthy lifestyles for adults with learning disabilities. Disabil. Rehabil. 1999, 21, 409–419. [Google Scholar] [CrossRef] [PubMed]
- Gable, S.L.; Haidt, J. What (and why) is positive psychology. Rev. Gen. Psychol. 2005, 9, 103–110. [Google Scholar] [CrossRef]
- Seligman, M.E.P.; Csikszentmihalyi, M. Positive psychology—An introduction. Am. Psychol. 2000, 55, 5–14. [Google Scholar] [CrossRef]
- Antonovsky, A. The salutogenic model as a theory to guide health promotion. Health Promot. Int. 1996, 11, 11–18. [Google Scholar] [CrossRef] [Green Version]
- Fletcher, D.; Sarkar, M. Psychological Resilience A Review and Critique of Definitions, Concepts, and Theory. Eur. Psychol. 2013, 18, 12–23. [Google Scholar] [CrossRef]
- Harrop, E.; Addis, S.; Elliott, E.; Williams, G. Resilience, Coping and Salutogenic Approaches to Maintaining and Generating Health: A Review; Cardiff Institute of Society, Health and Ethics: Cardiff, UK, 2006. [Google Scholar]
- Saxena, S.; Jané-LLopis, E.; Hosman, C. Prevention of mental and behavioural disorders: Implications for policy and practice. World Psychiatry 2006, 5, 5–14. [Google Scholar]
- Steinmann, R.M. Mental Health Stress—State of the Art Report to Develop a National Strategy for the Prevention of Stress and the Promotion of Mental Health; Health Promotion Switzerland: Bern/Lausanne, Switzerland, 2006. [Google Scholar]
- World Health Organization. Prevention of Mental Disorders—Effective Interventions and Policy Options: Summary Report; WHO: Geneva, Switzerland, 2004. [Google Scholar]
- Portzky, M. VK+ en P3 Vragenlijst over Veerkracht en Palliatieve Activiteiten: Handleiding. [VK+ en P3 Questionnaire Resilience and Palliative Activities: Manual]; Hogrefe: Amsterdam, The Netherlands, 2015. [Google Scholar]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [Green Version]
- Campbell, M.; Piaggio, G.; Elbourne, D.; Altman, D.; CONSORT group. Consort 2010 statement: Extension to cluster randomised trials. BMJ 2012, 345, e5661. [Google Scholar] [CrossRef] [PubMed]
- Bartholomew, L.K.; Markham, C.M.; Ruiter, R.A.C.; Fernández, M.E.; Kok, G.; Parcel, G.S. Planning Health Promotion Programs: An Intervention Mapping Approach, 4th ed.; Jossey-Bass: San Francisco, CA, USA, 2016. [Google Scholar]
- De Vries, H.; Dijkstra, M.; Kuhlman, P. Self-efficacy the third factor besides attitude and subjective norm as a predictor of behavioural intention. Health Educ. Res. 1988, 3, 273–282. [Google Scholar] [CrossRef]
- Prochaska, J.O.; DiClemente, C.C. Stages of change in the modification of problem behaviors. In Progress in Behavior Modification; Hersen, M., Eisler, R.M., Miller, P.M., Eds.; Sycamore Press: Berkshire, UK, 1992; pp. 184–218. [Google Scholar]
- Boevink, W.; Kroon, H.; Giesen, F. Empowerment—Constructie en Validatie Van een Vragenlijst [Empowerment—Construction and Validation of a Questionnaire]; Trimbos-instituut: Utrecht, The Netherlands, 2009. [Google Scholar]
- Wagnild, G.M. The Resilience Response Scale; YouthREX: Toronto, ON, Canada, 2011. [Google Scholar]
- Hublet, A.; Mommen, J.; Maes, L.; De Bourdeaudhuij, I. Steigers—Screenen Voor een Betere Gezondheid: Ontwikkeling en Handleiding [Steigers—Screening for Better Health: Development and Manual]; Steunpunt Welzijn, Volksgezondheid en Gezin: Leuven, Belgium, 2014. [Google Scholar]
- Schreurs, P.J.; van de Willige, G.; Brosschot, J.F.; Tellegen, B.; Graus, G.M. Handleiding Utrechtse Coping Lijst UCL [Manual]; Swets & Zeitlinger: Lisse, The Netherlands, 1993. [Google Scholar]
- Hoekstra, H.A.; De Fruyt, F. NEO-PI-3 Persoonlijkheidsvragenlijst, Handleiding; Hogrefe Uitgevers: Amsterdam, The Netherlands, 2014. [Google Scholar]
- van Hout, B.; Janssen, M.F.; Feng, Y.; Kohlmann, T.; Busschbach, J.; Golicki, D.; Lloyd, A.; Scalone, L.; Kind, P.; Pickard, A.S. Interim scoring for the EQ-5D-5L: Mapping the EQ-5D-5L to EQ-5D-3L value sets. Value Health 2012, 15, 708–715. [Google Scholar] [CrossRef] [PubMed]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.F.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janssen, M.F.; Pickard, A.S.; Golicki, D.; Gudex, C.; Niewada, M.; Scalone, L.; Swinburn, P.; Busschbach, J. Measurement properties of the EQ-5D-5L compared to the EQ-5D-3L across eight patient groups: A multi-country study. Qual. Life Res. 2013, 22, 1717–1727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cantril, H. The Pattern of Human Concern; Rutgers University Press: New Brunswick, NJ, USA, 1965. [Google Scholar]
- Sterne, J.A.C.; Smith, G.D. Sifting the evidence—What’s wrong with significance tests? BMJ 2001, 322, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Szabo, M. The emotional experience associated with worrying: Anxiety, depression, or stress? Anxiety Stress Coping 2011, 24, 91–105. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Llanes, J.M.; Vos, F.; Guha-Sapir, D. Measuring psychological resilience to disasters: Are evidence-based indicators an achievable goal? Environ. Health 2013, 12, 115. [Google Scholar] [CrossRef] [PubMed]
- Coffeng, J.K.; Boot, C.R.; Duijts, S.F.; Twisk, J.W.; van Mechelen, W.; Hendriksen, I.J. Effectiveness of a Worksite Social & Physical Environment Intervention on Need for Recovery, Physical Activity and Relaxation; Results of a Randomized Controlled Trial. PLoS ONE 2014, 9, e114860. [Google Scholar]
- Polit, D.F.; Beck, C.T. Essentials of Nursing Research: Appraising Evidence for Nursing Practice; Wolters Kluwer: London, UK, 2010. [Google Scholar]
- Galea, S.; Tracy, M. Participation rates in epidemiological studies. Ann. Epidemiol. 2007, 17, 643–653. [Google Scholar] [CrossRef]
- Tengland, P.A. Empowerment: A goal or a means for health promotion? Med. Health Care Philos. 2007, 10, 197–207. [Google Scholar] [CrossRef] [PubMed]
- Hochwälder, J. The psychosocial work environment and burnout among Swedish registered and assistant nurses: The main, mediating, and moderating role of empowerment. Nurs. Health Sci. 2007, 9, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Burton, N.W.; Pakenham, K.I.; Brown, W.J. Feasibility and effectiveness of psychosocial resilience training: A pilot study of the READY program. Psychol. Health Med. 2010, 15, 266–277. [Google Scholar] [CrossRef] [PubMed]
- Kobau, R.; Seligman, M.E.; Peterson, C.; Diener, E.; Zack, M.M.; Chapman, D.; Thompson, W. Mental health promotion in public health: Perspectives and strategies from positive psychology. Am. J. Public Health 2011, 101, e1–e9. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Sharma, S.D.; Sharma, M. Mental health promotion: A narrative review of emerging trends. Curr. Opin. Psychiatry 2017, 30, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Martin, A.; Sanderson, K.; Cocker, F. Meta-analysis of the effects of health promotion intervention in the workplace on depression and anxiety symptoms. Scand. J. Work Environ. Health 2009, 35, 7–18. [Google Scholar] [CrossRef] [PubMed]
- Czabala, C.; Charzynska, K.; Mroziak, B. Psychosocial interventions in workplace mental health promotion: An overwiew. Health Promot. Int. 2011, 26, 70–84. [Google Scholar] [CrossRef] [PubMed]
- Sheeran, P. Intention—Behavior Relations: A Conceptual and Empirical Review. Eur. Rev. Soc. Psychol. 2002, 12, 1–36. [Google Scholar] [CrossRef]
- Dilorio, C.K. Measurement in Health Behavior: Methods for Research and Evaluation; John Wiley & Sons: San Francisco, CA, USA, 2005. [Google Scholar]
- Van Woerkom, M.; Meyers, M.C. Effects of a strengths-based psychological climate on positive affect and job performance. Hum. Resour. Manag. 2015, 54, 81–103. [Google Scholar] [CrossRef]
- Anderson, P.; Jané-Llopis, E.; Hosman, C. Reducing the silent burden of impaired mental health. Health Promot. Int. 2011, 26, 4–9. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Intervention Group (n = 86) | Control Group (n = 108) | X2 | p |
|---|---|---|---|---|
| Gender (% women) | 56.5 | 52.8 | 0.26 | 0.61 |
| Age categories (%) | 0.26 | 0.97 | ||
| 20–30 years | 16.9 | 15.9 | ||
| 31–40 years | 21.7 | 24.3 | ||
| 41–50 years | 36.1 | 33.6 | ||
| 51–61 years | 25.3 | 26.2 | ||
| Age when ending school (% 18 years or older) | 78.8 | 70.5 | 1.71 | 0.19 |
| Educational level (%) | 1.18 | 0.56 | ||
| Secondary education for people with disabilities | 47.6 | 57.7 | ||
| Vocational or technical secondary education | 41.3 | 32.7 | ||
| General secondary or tertiary education | 11.1 | 9.6 | ||
| Birthplace (% other than Belgium) | 9.4 | 9.2 | 0.003 | 0.96 |
| Mother tongue (%) | 4.01 | 0.13 | ||
| Dutch | 81.2 | 86.2 | ||
| Dutch and other | 16.5 | 8.3 | ||
| Other | 2.4 | 5.5 |
| Outcome | Group | Baseline (M ± sd) | One Month (M ± sd) | Four Months (M ± sd) |
|---|---|---|---|---|
| Empowerment | Intervention | 3.8 ± 0.4 | 3.9 ± 0.4 | 4.0 ± 0.5 |
| Control | 3.8 ± 0.5 | 3.9 ± 0.5 | 4.0 ± 0.6 | |
| Resilience daily activities | Intervention | 3.5 ± 1.1 | 3.7 ± 1.2 | 3.9 ± 1.2 |
| Control | 3.2 ± 1.2 | 3.4 ± 1.1 | 3.5 ± 1.3 | |
| Duration mental recovery | Intervention | 2.6 ± 1.1 | 2.5 ± 1.2 | 2.8 ± 1.1 |
| Control | 2.3 ± 1.2 | 2.3 ± 1.1 | 2.3 ± 1.2 | |
| Optimism | Intervention | 3.7 ± 1.0 | 3.8 ± 0.9 | 4.2 ± 0.9 |
| Control | 3.8 ± 1.1 | 3.9 ± 1.0 | 4.0 ± 1.0 | |
| Unjustified worrying | Intervention | 2.7 ± 1.1 | 2.9 ± 1.1 | 2.8 ± 1.2 |
| Control | 2.9 ± 1.0 | 2.8 ± 1.0 | 2.6 ± 1.0 | |
| Destructive activities | Intervention | 0.7 ± 0.3 | 0.6 ± 0.3 | 0.7 ± 0.3 |
| Control | 0.7 ± 0.3 | 0.7 ± 0.2 | 0.7 ± 0.3 | |
| Suicidal ideations | Intervention | 0.5 ± 0.7 | 0.3 ± 0.4 | 0.4 ± 0.6 |
| Control | 0.3 ± 0.6 | 0.3 ± 0.5 | 0.3 ± 0.5 | |
| Attitude | Intervention | 3.9 ± 0.5 | 4.0 ± 0.5 | 4.2 ± 0.6 |
| Control | 3.9 ± 0.5 | 3.9 ± 0.5 | 4.1 ± 0.6 | |
| Self-efficacy | Intervention | 3.2 ± 0.7 | 3.2 ± 0.8 | 3.6 ± 0.9 |
| Control | 3.4 ± 0.7 | 3.5 ± 0.7 | 3.7 ± 0.9 | |
| Perceived social support | Intervention | 3.7 ± 0.5 | 4.0 ± 0.6 | 4.2 ± 0.7 |
| Control | 3.7 ± 0.6 | 3.7 ± 0.6 | 4.1 ± 0.6 | |
| Quality of life | Intervention | 0.79 ± 0.17 | 0.84 ± 0.15 | 0.88 ± 0.13 |
| Control | 0.81 ± 0.15 | 0.85 ± 0.15 | 0.85 ± 0.16 | |
| Life satisfaction (physical health) | Intervention | 66.9 ± 20.6 | 69.2 ± 20.9 | 72.0 ± 18.8 |
| Control | 67.1 ± 19.6 | 73.3 ± 19.1 | 74.7 ± 19.7 | |
| Life satisfaction (mental health) | Intervention | 7.4 ± 2.5 | 7.8 ± 2.5 | 7.2 ± 2.5 |
| Control | 7.7 ± 2.6 | 7.8 ± 2.6 | 7.7 ± 2.4 |
| Outcomes | ICC | Intercept | Group (ref. = Control) | Time 1 (One Month) | Time 2 (Four Months) | Group * Time 1 | Group * Time 2 | % Variance Explained a | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| b (SE) | b (SE) | p | b (SE) | p | b (SE) | p | b (SE) | p | b (SE) | p | |||
| Empowerment | 0.04 | 3.86 (0.06) | −0.04 (0.09) | 0.65 | 0.11 (0.05) | 0.03 | 0.22 (0.05) | <0.001 | −0.02 (0.08) | 0.75 | 0.01 (0.08) | 0.87 | 2.10 |
| Resilience daily activities | 0.01 | 3.17 (0.11) | 0.32 (0.17) | 0.06 | 0.18 (0.13) | 0.16 | 0.33 (0.13) | 0.01 | −0.01 (0.17) | 0.97 | 0.11 (0.20) | 0.58 | 4.00 |
| Duration mental recovery | 0.08 | 2.32 (0.15) | 0.30 (0.22) | 0.17 | −0.06 (0.12) | 0.61 | 0.02 (0.12) | 0.86 | −0.08 (0.18) | 0.66 | 0.10 (0.18) | 0.58 | 1.77 |
| Optimism | 0.00 | 3.75 (0.09) | −0.06 (0.14) | 0.65 | 0.09 (0.11) | 0.44 | 0.23 (0.11) | 0.04 | −0.01 (0.17) | 0.94 | 0.26 (0.18) | 0.14 | 1.81 |
| Unjustified worrying | 0.00 | 2.87 (0.11) | −0.17 (0.16) | 0.30 | −0.09 (0.11) | 0.44 | −0.27 (0.11) | 0.01 | 0.31 (0.17) | 0.07 | 0.38 (0.17) | 0.03 | 0.00 |
| Destructive activities | 0.00 | 0.72 (0.03) | −0.01 (0.04) | 0.77 | −0.004 (0.03) | 0.88 | −0.04 (0.03) | 0.10 | −0.06 (0.04) | 0.11 | 0.002 (0.04) | 0.96 | 0.00 |
| Suicidal ideations | 0.02 | 0.31 (0.06) | 0.21 (0.09) | 0.01 | −0.03 (0.05) | 0.56 | 0.01 (0.05) | 0.90 | −0.15 (0.08) | 0.05 | −0.09 (0.08) | 0.24 | 1.71 |
| Attitude | 0.01 | 3.87 (0.06) | 0.05 (0.09) | 0.59 | 0.08 (0.06) | 0.20 | 0.23 (0.06) | <0.001 | 0.01 (0.09) | 0.95 | 0.05 (0.09) | 0.59 | 1.00 |
| Self−efficacy | 0.17 | 3.42 (0.13) | −0.26 (0.19) | 0.16 | 0.13 (0.08) | 0.12 | 0.29 (0.08) | 0.001 | −0.09 (0.13) | 0.47 | 0.13 (0.13) | 0.31 | 4.42 |
| Perceived social support | 0.00 | 3.74 (0.06) | −0.01 (0.09) | 0.93 | 0.04 (0.07) | 0.59 | 0.38 (0.07) | <0.001 | 0.19 (0.10) | 0.06 | 0.10 (0.10) | 0.36 | 3.40 |
| Quality of life | 0.00 | 0.81 (0.01) | −0.03 (0.02) | 0.23 | 0.04 (0.01) | 0.01 | 0.04 (0.01) | 0.01 | 0.01 (0.02) | 0.53 | 0.05 (0.02) | 0.02 | 1.91 |
| Life satisfaction (physical) | 0.00 | 67.14 (1.88) | −0.20 (2.86) | 0.95 | 7.08 (2.03) | 0.001 | 7.88 (2.01) | <0.001 | −4.63 (3.11) | 0.14 | −1.80 (3.13) | 0.57 | 1.40 |
| Life satisfaction (mental) | 0.00 | 7.73 (0.24) | −0.30 (0.36) | 0.40 | 0.02 (0.30) | 0.94 | −0.02 (0.30) | 0.96 | 0.37 (0.46) | 0.42 | −0.12 (0.46) | 0.79 | 0.00 |
| Questions | Percentages | ||
|---|---|---|---|
| (Strongly) Agree | I Don’t Know | (Strongly) Disagree | |
| I found the assignment about burden useful (n = 77) 1 | 94.8 | 3.9 | 1.3 |
| Through session 1, I have more understanding about my own burden (n = 77) | 88.3 | 3.9 | 2.6 |
| I found the assignment about resilience useful (n = 75) | 94.7 | 4.0 | 1.3 |
| Through session 1, I have more understanding about my own resilience (n = 76) | 90.8 | 6.6 | 2.6 |
| I found the proposed actions useful (n = 77) | 97.4 | 1.3 | 1.3 |
| I understand the four colors (n = 77) | 100.0 | 0.0 | 0.0 |
| The proposed actions give good ideas about my life (n = 76) | 93.4 | 1.3 | 5.2 |
| I am motivated to perform the actions (n = 77) | 88.3 | 6.5 | 5.2 |
| The sessions caused a good feeling (n = 77) | 89.6 | 10.4 | 0.0 |
| I felt understood by the teacher (n = 77) | 93.5 | 5.2 | 1.3 |
| The teacher gave a clear explanation of the assignments (n = 77) | 100.0 | 0.0 | 0.0 |
| I felt good in the group (n = 77) | 98.7 | 1.3 | 0.0 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deforche, B.; Mommen, J.; Hublet, A.; De Roover, W.; Huys, N.; Clays, E.; Maes, L.; De Bourdeaudhuij, I.; Van Cauwenberg, J. Evaluation of a Brief Intervention for Promoting Mental Health among Employees in Social Enterprises: A Cluster Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2018, 15, 2107. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15102107
Deforche B, Mommen J, Hublet A, De Roover W, Huys N, Clays E, Maes L, De Bourdeaudhuij I, Van Cauwenberg J. Evaluation of a Brief Intervention for Promoting Mental Health among Employees in Social Enterprises: A Cluster Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2018; 15(10):2107. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15102107
Chicago/Turabian StyleDeforche, Benedicte, Jasmine Mommen, Anne Hublet, Winnie De Roover, Nele Huys, Els Clays, Lea Maes, Ilse De Bourdeaudhuij, and Jelle Van Cauwenberg. 2018. "Evaluation of a Brief Intervention for Promoting Mental Health among Employees in Social Enterprises: A Cluster Randomized Controlled Trial" International Journal of Environmental Research and Public Health 15, no. 10: 2107. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15102107