Short Telomere Length as a Biomarker Risk of Lung Cancer Development Induced by High Radon Levels: A Pilot Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
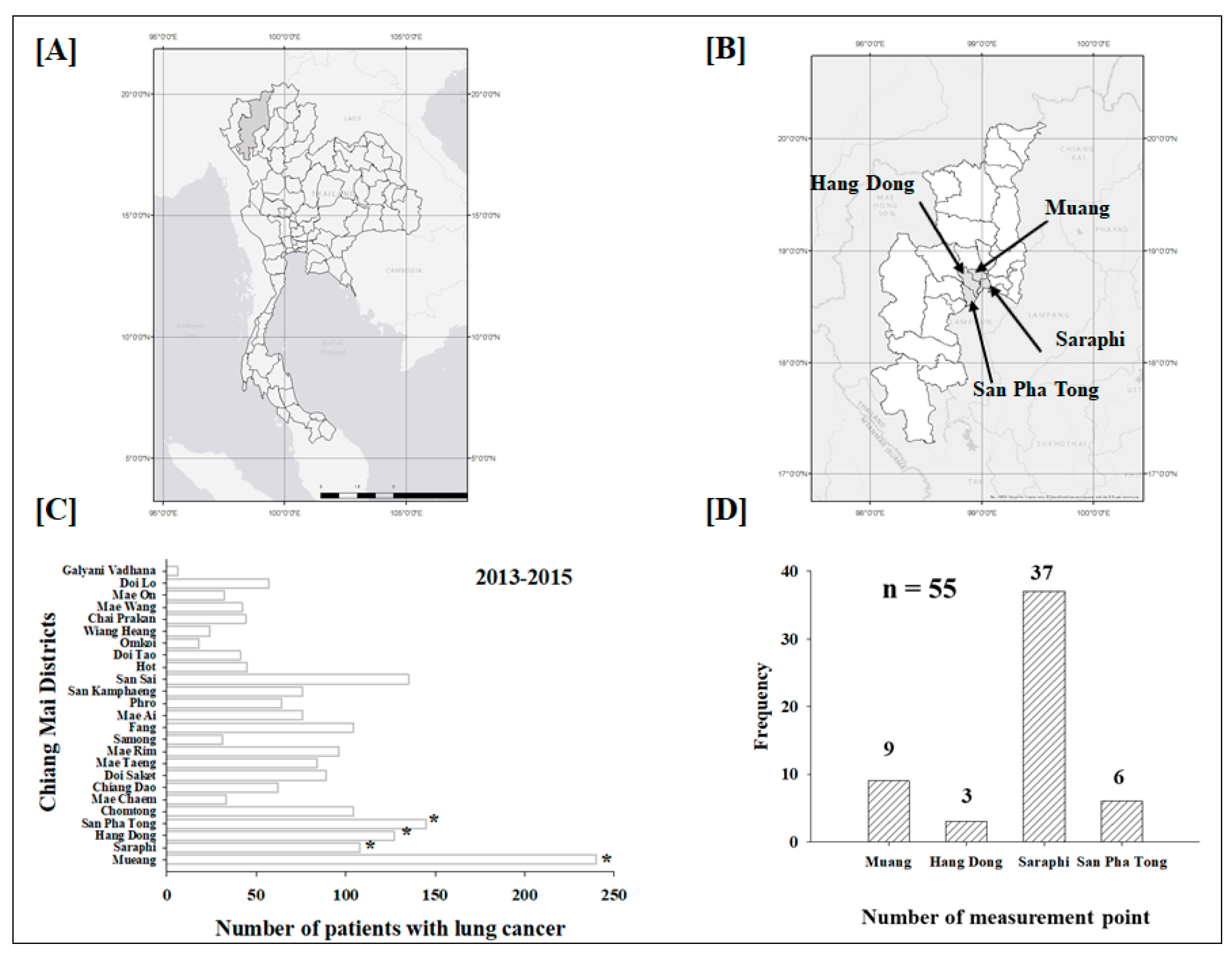
2.1. Study Area
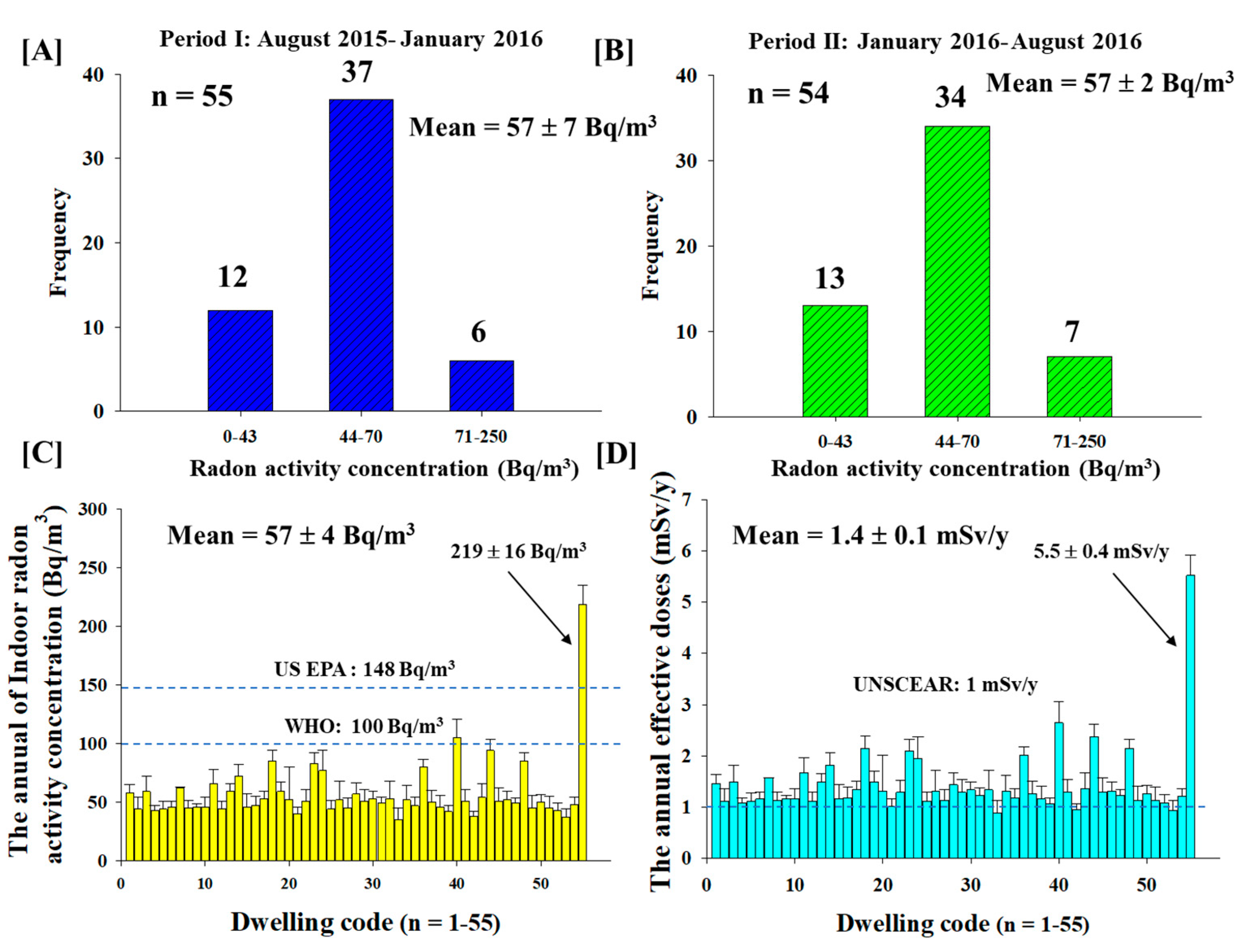
2.2. Long Term Measurement of Indoor Radon Exposure Using a Passive Method
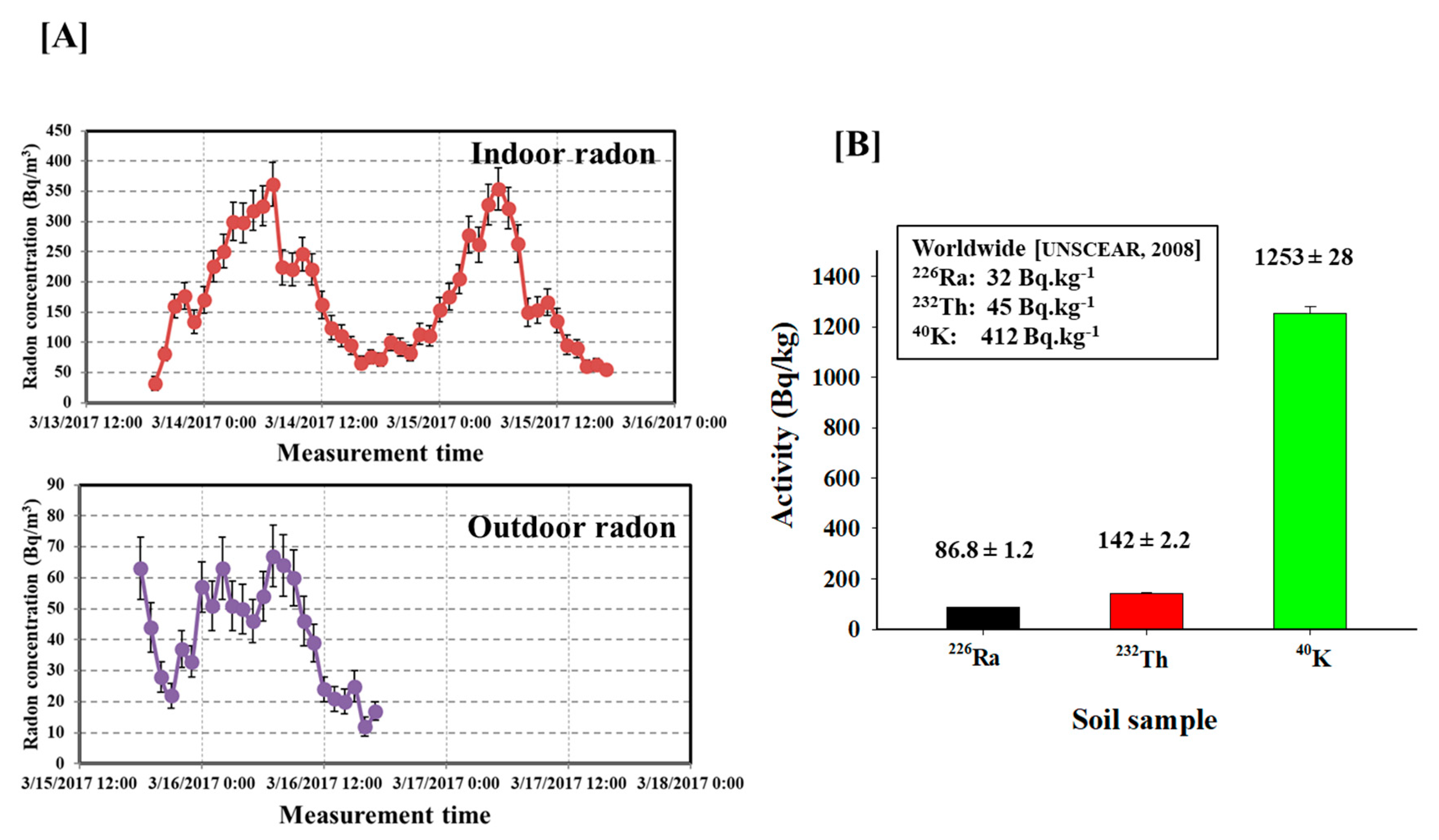
2.3. Short Term Measurement of Indoor and Outdoor Radon Using an Active Method
2.4. Estimation of the Average Annual Effective Dose
2.5. Soil Sample Preparation and Analysis
2.6. Ethics Statement
2.7. Study Design and Characteristics of Study Population
2.8. Blood Samples and Genomic DNA Extraction
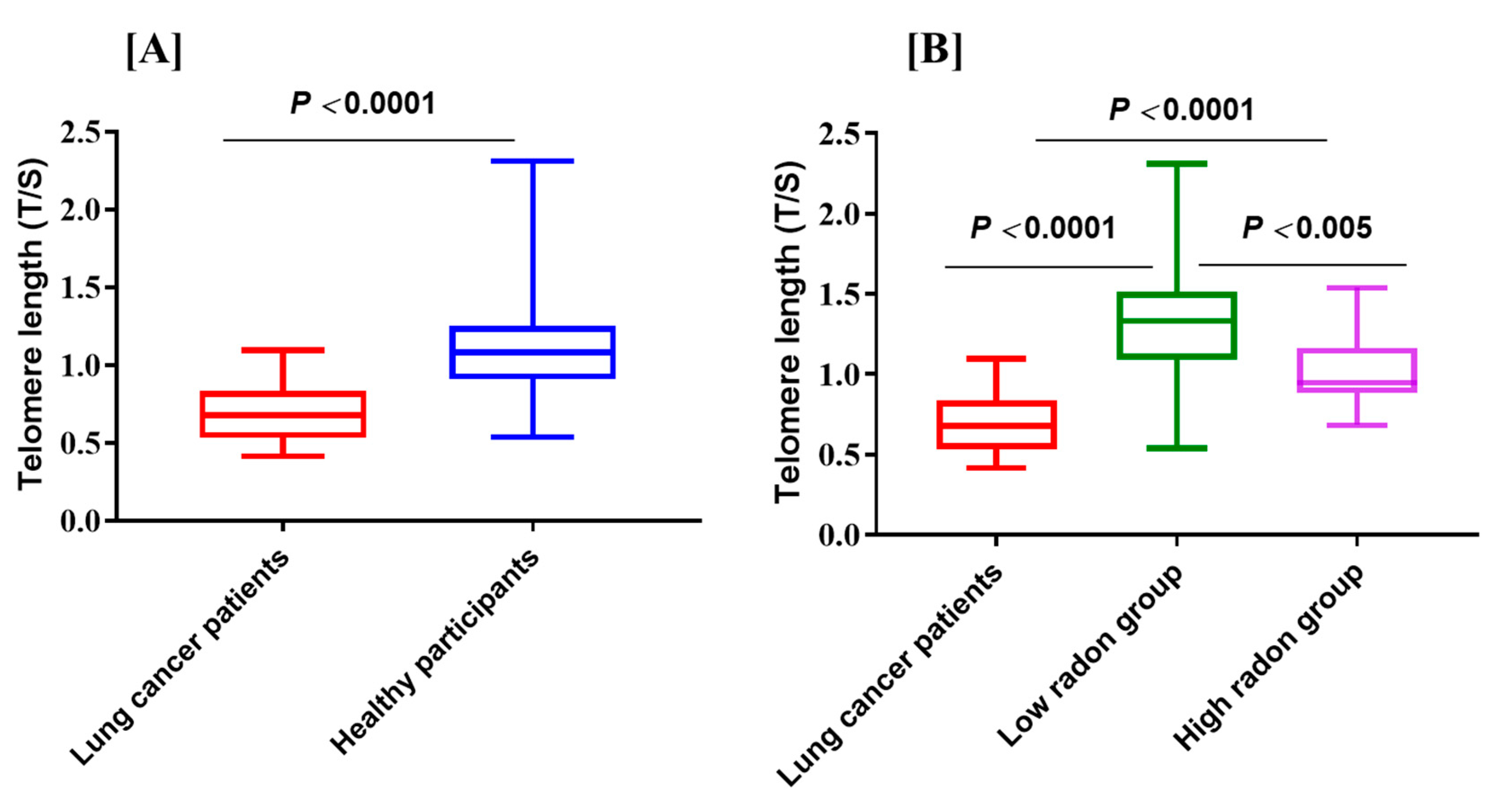
2.9. Telomere Length Measurement
2.10. Statistical Analysis
3. Result and Discussion
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lemjabbar-Alaoui, H.; Hassan, O.U.; Yang, Y.W.; Buchanan, P. Lung cancer: Biology and treatment options. Biochim. Biophys. Acta 2015, 1856, 189–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiwatanadate, P. Lung cancer related to environmental and occupational hazards and epidemiology in Chiang Mai, Thailand. Genes Environ. 2011, 33, 120–127. [Google Scholar] [CrossRef]
- Autsavapromporn, N.; de Toledo, S.M.; Little, J.B.; Jay-Gerin, J.P.; Harris, A.L.; Azzam, E.I. The role of gap junction communication and oxidative stress in the propagation of toxic effects among high-dose-α particle-irradiated human cells. Radiat. Res. 2011, 175, 347–357. [Google Scholar] [CrossRef] [PubMed]
- National Research Council. Biological Effects of Ionizing Radiation (BEIR) VI Report: The Health Effects of Exposure to Radon; National Academy Press: Washington, DC, USA, 1999. [Google Scholar]
- United Nations Scientific Committee on the Effects of Atomic Radiation. Sources and Effects of Ionizing Radiation: United Nations Scientific Committee on the Effects of Atomic Radiation: UNSCEAR 2000 Report to the General Assembly, with Scientific Annexes; United Nations: New York, NY, USA, 2000. [Google Scholar]
- WHO. WHO Handbook on Indoor Radon—A Public Health Perspective; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Al-Zoughool, M.; Krewski, D. Health effects of radon: A review of the literature. Int. J. Radiat. Biol. 2009, 85, 57–69. [Google Scholar] [CrossRef] [PubMed]
- Gansner, J.M.; Rosas, I.O. Telomeres in lung disease. Transl. Res. 2013, 162, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Hou, L.; Zhang, X.; Gawron, A.J.; Liu, J. Surrogate tissue telomere length and cancer risk: Shorter or longer? Cancer Lett. 2012, 319, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Jang, J.S.; Choi, Y.Y.; Lee, W.K.; Choi, J.E.; Cha, S.I.; Kim, Y.J.; Kim, C.H.; Kam, S.; Jung, T.H.; Park, J.Y. Telomere length and the risk of lung cancer. Cancer Sci. 2008, 99, 1385–1389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, J.-M.; Beckman, K.B.; Wang, R.; Bull, C.; Adams-Haduch, J.; Huang, J.Y.; Jin, A.; Opresko, P.; Newman, A.B.; Zheng, Y.L.; et al. Leukocyte telomere length in relation to risk of lung adenocarcinoma incidence: Findings from the Singapore Chinese health study. Int. J. Cancer. 2018, 142, 2234–2243. [Google Scholar] [CrossRef] [PubMed]
- Ma, H.; Zhou, Z.; Wei, S.; Liu, Z.; Pooley, K.A.; Dunning, A.M.; Svenson, U.; Roos, G.; Hosgood, H.D.; Shen, M.; et al. Shortened telomere length is associated with increased risk of cancer: A meta-analysis. PLoS ONE 2011, 6, e20466. [Google Scholar] [CrossRef] [PubMed]
- Sun, B.; Wang, Y.; Kota, K.; Shi, Y.; Motlak, S.; Makambi, K.; Loffredo, C.A.; Shields, P.G.; Yang, Q.; Harris, C.C.; et al. Telomere length variation: A potential new telomere biomarker for lung cancer risk. Lung Cancer 2015, 88, 297–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tokonami, S.; Zhuo, W.; Ryuo, H.; Yonehara, H.; Yamada, Y.; Shimo, M. Instrument performance of a measuring system with alpha-track detection technique. Radiat. Prot. Dosim. 2003, 103, 69–72. [Google Scholar] [CrossRef]
- Tokonami, S.; Takahashi, H.; Kobayashi, Y.; Zhuo, W. Up-to-date radon-thoron discriminative detector for a large scale survey. Rev. Sci. Instrum. 2005, 76, 113505. [Google Scholar] [CrossRef]
- International Organization for Standardization (ISO). Measurement of Radioactivity in the Environment-Air-Radon 220: INTEGRATED Measurement Methods for the Determination of the Average Activity Concentration Using Passive Solid State Nuclear Track Detectors; ISO 16641; International Organization for Standardization: Geneva, 2014. [Google Scholar]
- Hosoda, M.; Tokonami, S.; Omori, Y.; Ishikawa, T.; Iwoaka, K. Comparison of the dose from natural radionuclide and artificial radionuclides after the Fukushima nuclear accident. J. Radiat. Res. 2016, 57, 422–430. [Google Scholar] [CrossRef] [PubMed]
- Krisananuwat, R.; Chanyotha, S.; Kranrod, C.; Pengvanich, P. Transfer factor of 226Ra, 232Th and 40K from soil to Alpinia Galangal plant grown in Northern Thailand. J. Phys. Conf. Ser. 2017, 860, 012008. [Google Scholar] [CrossRef]
- Cawthon, R.M. Telomere length measurement by a novel monochrome multiplex quantitative PCR method. Nucleic Acids Res. 2009, 37, e21. [Google Scholar] [CrossRef] [PubMed]
- Shen, M.; Cawthon, R.; Rothman, N.; Weinstein, S.J.; Virtamo, J.; Hosgood, H.D.; Hu, W.; Lim, U.; Albanes, D.; Lan, Q. A prospective study of telomere length measured by monochrome multiplex quantitative PCR and risk of lung cancer. Lung Cancer 2011, 73, 133–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Internal Commission on Radiological Protection. Radiological Protection Against Radon; ICRP Publication 103, Ann ICRP 37; Pergamon Press: Oxford, UK; New York, NY, USA, 2014. [Google Scholar]
- Little, J.B. What are the risks of low-level exposure to α radiation from radon? Proc. Natl. Acad. Sci. USA 1997, 94, 5996–5997. [Google Scholar] [CrossRef] [PubMed]
- United Nations Scientific Committee on the Effects of Atomic Radiation. Sources and Effects of Ionizing Radiation: United Nations Scientific Committee on the Effects of Atomic Radiation: UNSCEAR 2008 Report to the General Assembly, with Scientific Annexes; United Nations: New York, NY, USA, 2008. [Google Scholar]
- Lantz, P.M.; Mendez, D.; Philbert, M.A. Radon, smoking, and lung cancer: The need to refocus radon control policy. Am. J. Public Health 2013, 103, 443–447. [Google Scholar] [CrossRef] [PubMed]
- Meenakshi, C.; Sivasubramanian, K.; Venkatraman, B. Nucleoplasmic bridges as a biomarker of DNA damage exposed to radon. Mutat. Res./Genet. Toxicol. Environ. Mutagen. 2017, 814, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Qian, Y.; Ding, T.; Wei, L.; Cao, S.; Yang, L. Shorter telomere length of T-cells in peripheral blood of patients with lung cancer. OncoTargets Ther. 2016, 9, 2675–2682. [Google Scholar]
- Das, B.; Saini, D.; Seshadri, M. Telomere length in human adults and high level natural background radiation. PLoS ONE 2009, 4, e8440. [Google Scholar] [CrossRef] [PubMed]
- Lansdorp, P.M. Telomere length and proliferation potential of hematopoietic stem cells. J. Cell Sci. 1995, 108, 1–6. [Google Scholar] [PubMed]
- Hansen, M.E.B.; Hunt, S.C.; Stone, R.C.; Horvath, K.; Herbig, U.; Ranciaro, A.; Hirbo, J.; Beggs, W.; Reiner, A.P.; Wilson, J.G.; et al. Shorter telomere length in Europeans than in Africans due to polygenetic adaptation. Hum. Mol. Genet. 2016, 25, 2324–2330. [Google Scholar] [CrossRef] [PubMed]
- McGrath, M.; Wong, J.Y.; Michaud, D.; De Vivo, I. Telomere length, cigarette smoking, and bladder cancer risk in men and women. Cancer Epidemiol. Biomark. Prev. 2007, 16, 815–819. [Google Scholar] [CrossRef] [PubMed]
- Von Zglinicki, T. Oxidative stress shortens telomeres. Trends Biochem. Sci. 2002, 27, 339–344. [Google Scholar] [CrossRef]
- Bekaert, S.; De Meyer, T.; Van Oostveldt, P. Telomere attrition as ageing biomarker. Anticancer Res. 2005, 25, 3011–3021. [Google Scholar] [PubMed]
- Suslova, K.G.; Khokhryakov, V.F.; Tokarskaya, Z.B.; Nifatov, A.P.; Sokolova, A.B.; Miller, S.C.; Krahenbuhl, M.P. Modifying effects of health status, physiological, and dosimetric factors on extrapulmonary organ distribution and excretion of inhaled plutonium in workers at the Mayak Production Association. Health Phys. 2006, 90, 299–311. [Google Scholar] [CrossRef] [PubMed]
- Peckham, E.C.; Scheurer, M.E.; Danysh, H.E.; Lubega, J.; Langlois, P.H.; Lupo, P.J. Residential radon exposure and incidence of childhood lymphoma in Texas, 1995–2001. Int. J. Environ. Res. Public. Health 2015, 12, 12110–12126. [Google Scholar] [CrossRef] [PubMed]
- Torres-Durán, M.; Ruano-Ravina, A.; Parente-Lamelas, I.; Leiro-Fernández, V.; Abal-Arca, J.; Montero-Martínez, C.; Pena-Álvarez, C.; Castro-Añón, O.; Golpe-Gómez, A.; Martínez, C.; et al. Residential radon and lung cancer characteristics in never smokers. Int. J. Radiat. Biol. 2015, 91, 605–610. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Lung Cancer Patients (n = 35) | Healthy Nonsmokers (n = 33) | ||
|---|---|---|---|---|
| Low Radon (11) | High Radon (22) | Total (33) | ||
| Age in years, mean (SD) | 66.4 (9.7) | 43.5 (16.4) | 53.6 (19.6) | 50.2 (18.9) |
| Gender | ||||
| Male | 17 | 5 | 10 | 15 |
| Female | 18 | 6 | 12 | 18 |
| Telomere length, T/S ratio (SD) | 0.7 (0.2) | 1.35 (0.4) | 1.0 (0.2) | 1.12 (0.3) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Autsavapromporn, N.; Klunklin, P.; Threeratana, C.; Tuntiwechapikul, W.; Hosoda, M.; Tokonami, S. Short Telomere Length as a Biomarker Risk of Lung Cancer Development Induced by High Radon Levels: A Pilot Study. Int. J. Environ. Res. Public Health 2018, 15, 2152. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15102152
Autsavapromporn N, Klunklin P, Threeratana C, Tuntiwechapikul W, Hosoda M, Tokonami S. Short Telomere Length as a Biomarker Risk of Lung Cancer Development Induced by High Radon Levels: A Pilot Study. International Journal of Environmental Research and Public Health. 2018; 15(10):2152. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15102152
Chicago/Turabian StyleAutsavapromporn, Narongchai, Pitchayaponne Klunklin, Chalat Threeratana, Wirote Tuntiwechapikul, Masahiro Hosoda, and Shinji Tokonami. 2018. "Short Telomere Length as a Biomarker Risk of Lung Cancer Development Induced by High Radon Levels: A Pilot Study" International Journal of Environmental Research and Public Health 15, no. 10: 2152. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15102152