Determinants of Risk Perception Related to Exposure to Endocrine Disruptors during Pregnancy: A Qualitative and Quantitative Study on French Women

 ,
,
Abstract
:1. Introduction
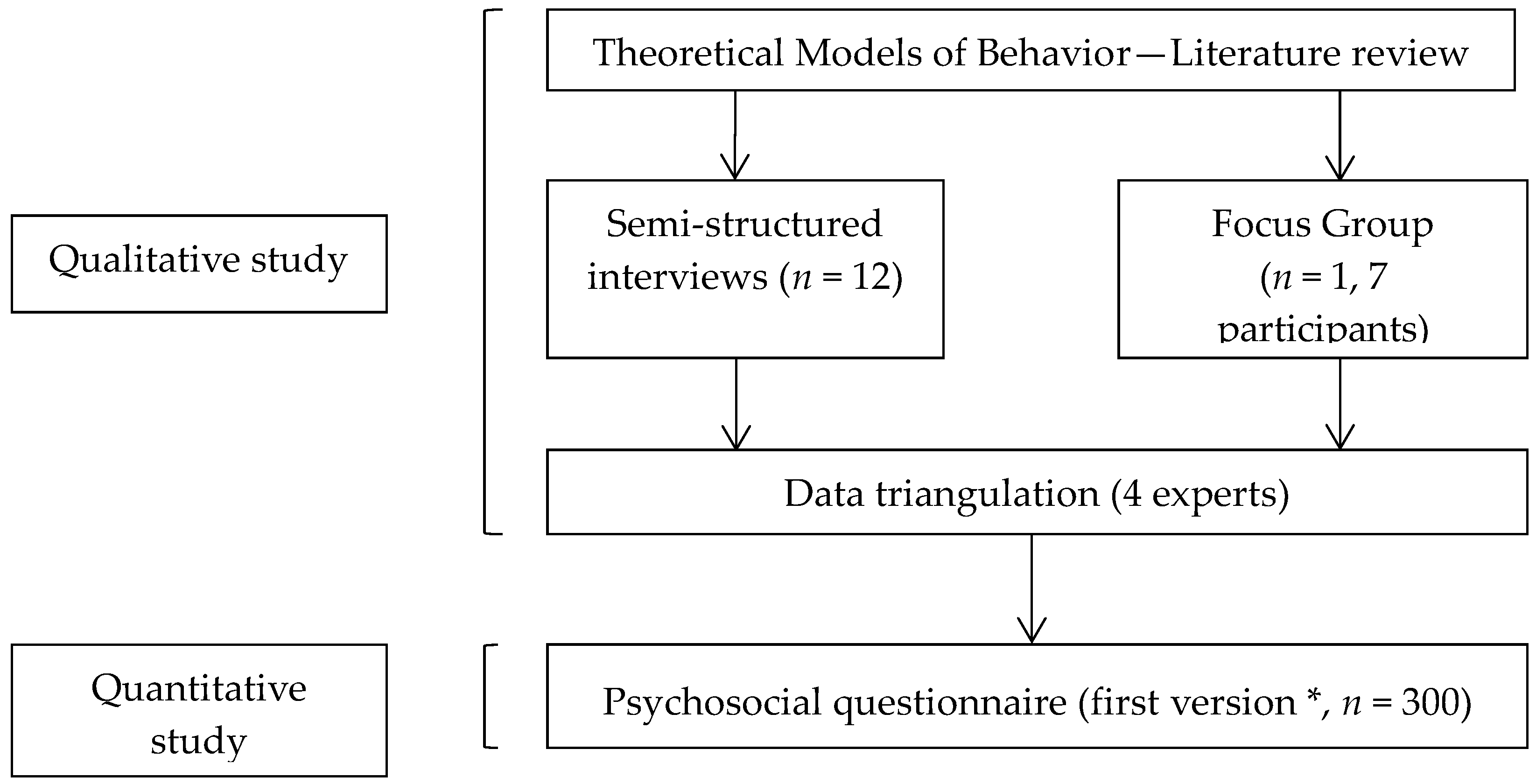
2. Materials and Methods
2.1. Theoretical Framework
2.2. Study Settings
2.2.1. Participant Sampling
2.2.2. Methods of Approach
2.2.3. Sample Size
2.2.4. Data Collection
2.2.5. Setting
2.3. Analysis
3. Results
3.1. Characteristics of Populations
3.2. EDC Risk Perception
3.2.1. Perceived Severity
3.2.2. Perceived Susceptibility
3.2.3. Score of EDC Risk Perception
3.3. Determinants of EDC Risk Perception
4. Discussion
4.1. EDC Risk Perception
4.2. Determinants of EDC Risk Perception
4.2.1. Age
4.2.2. Level of Knowledge and Mediatization
4.2.3. Other Determinants
4.3. Strengths of the Study
4.4. Bias and Limits of the Study
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Interviews of Pregnant Women | |
|---|---|---|
| N = 12 | % | |
| Age (years) | ||
| 18–24 | 3 | 25.0 |
| 25–29 | 3 | 25.0 |
| 30–34 | 3 | 25.0 |
| >35 | 3 | 25.0 |
| Employment status of pregnant women | ||
| Unemployed | 2 | 16.7 |
| Artisan, Merchant, Business leader | 1 | 8.3 |
| Executive, Higher intellectual profession | 2 | 16.7 |
| Intermediate profession | 2 | 16.7 |
| Employed | 5 | 41.7 |
| Employment status of the husband | ||
| Unemployed | 1 | 8.3 |
| Artisan, Merchant, Business leader | 1 | 8.3 |
| Executive, Superior intellectual profession | 4 | 33.3 |
| Intermediate profession | 1 | 8.3 |
| Employed | 5 | 41.7 |
| Place of residence | ||
| Urban | 7 | 58.3 |
| Rural | 5 | 41.7 |
| Accomodation type | ||
| House | 10 | 83.3 |
| Apartment | 2 | 16.7 |
| Primiparity | ||
| No | 4 | 33.3 |
| Yes | 8 | 66.7 |
| Gender | Profession | Workplace | |
|---|---|---|---|
| 1 | Female | Midwife (student) | University Hospital |
| 2 | Female | Pediatric nurse | French departmental structure responsible for mothers and their children’s protection |
| 3 | Female | Prevention psychology (student) | French association involved in health education and promotion |
| 4 | Female | Project leader | French health care mutual |
| 5 | Female | Workshop organizer | French health care mutual |
| 6 | Male | Project leader | French association involved in health education and promotion |
| 7 | Male | PhD student | University Hospital |
References
- Barouki, R.; Gluckman, P.D.; Grandjean, P.; Hanson, M.; Heindel, J.J. Developmental origins of non-communicable disease: Implications for research and public health. Environ. Heal. Glob. Access Sci. Source 2012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Global Assessment of the State-of-the-Science of Endocrine Disruptors. Available online: http://www.who.int/ipcs/publications/new_issues/endocrine_disruptors/en/ (accessed on 20 July 2017).
- ANSES’s Working Group on « Endocrine disruptors »; ANSES’s Expert Committee on « Chemicals covered by the REACh and CLP Regulations »; Pouzaud, F.; Thierry-Mieq, M.; Burqa, K.; Vérines-Jouin, L.; Fiore, K.; Beausoleil, C.; Michel, C.; Rousselle, C.; Pasquier, E. Concerns related to ED-mediated effects of Bisphenol A and their regulatory consideration. Mol. Cell. Endocrinol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Fukazawa, H.; Watanabe, M.; Shiraishi, F.; Shiraishi, H.; Shiozawa, T.; Matsushita, H.; Terao, Y. Formation of chlorinated derivatives of bisphenol A in waste paper recycling plants and their estrogenic activities. J. Heal. Sci. 2002, 48, 242–249. [Google Scholar] [CrossRef]
- Ding, K.; Kong, X.; Wang, J.; Lu, L.; Zhou, W.; Zhan, T.; Zhang, C.; Zhuang, S. Side chains of parabens modulate antiandrogenic activity: In vitro and molecular docking studies. Environ. Sci. Technol. 2017, 51, 6452–6460. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, O.; Oishi, S. Disposition of orally administered 2,2-Bis (4-hydroxyphenyl) propane (Bisphenol A) in pregnant rats and the placental transfer to fetuses. Environ. Heal. Perspect. 2000, 108, 931–935. [Google Scholar] [CrossRef] [PubMed]
- Kosarac, I.; Kubwabo, C.; Lalonde, K.; Foster, W. A novel method for the quantitative determination of free and conjugated bisphenol A in human maternal and umbilical cord blood serum using a two-step solid phase extraction and gas chromatography/tandem mass spectrometry. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2012, 898, 90–94. [Google Scholar] [CrossRef] [PubMed]
- Chou, W.-C.; Chen, J.-L.; Lin, C.-F.; Chen, Y.-C.; Shih, F.-C.; Chuang, C.-Y. Biomonitoring of bisphenol A concentrations in maternal and umbilical cord blood in regard to birth outcomes and adipokine expression: A birth cohort study in Taiwan. Environ. Heal. Glob. Access Sci. Source 2011, 10, 94. [Google Scholar] [CrossRef] [PubMed]
- Schönfelder, G.; Wittfoht, W.; Hopp, H.; Talsness, C.E.; Paul, M.; Chahoud, I. Parent bisphenol A accumulation in the human maternal-fetal-placental unit. Environ. Heal. Perspect. 2002, 110, A703–A707. [Google Scholar] [CrossRef]
- Mortensen, M.E.; Calafat, A.M.; Ye, X.; Wong, L.-Y.; Wright, D.J.; Pirkle, J.L.; Merrill, L.S.; Moye, J. Urinary concentrations of environmental phenols in pregnant women in a pilot study of the National Children’s Study. Environ. Res. 2014, 129, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.; Kim, S.; Park, J.; Kim, H.-J.; Lee, J.; Choi, G.; Choi, S.; Kim, S.; Kim, S.Y.; Moon, H.-B.; et al. Urinary paraben concentrations among pregnant women and their matching newborn infants of Korea, and the association with oxidative stress biomarkers. Sci. Total Environ. 2013. [Google Scholar] [CrossRef] [PubMed]
- Casas, L.; Fernández, M.F.; Llop, S.; Guxens, M.; Ballester, F.; Olea, N.; Irurzun, M.B.; Rodríguez, L.S.M.; Riaño, I.; Tardón, A.; et al. Urinary concentrations of phthalates and phenols in a population of Spanish pregnant women and children. Environ. Int. 2011, 37, 858–866. [Google Scholar] [CrossRef] [PubMed]
- Migeot, V.; Dupuis, A.; Cariot, A.; Albouy-Llaty, M.; Pierre, F.; Rabouan, S. Bisphenol a and its chlorinated derivatives in human colostrum. Environ. Sci. Technol. 2013, 47, 13791–13797. [Google Scholar] [CrossRef] [PubMed]
- Metz, C.M. Bisphenol A: Understanding the Controversy. Workplace Heal. Saf. 2016, 64, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, K.K.; Peterson, K.E.; Lee, J.M.; Mercado-García, A.; Blank-Goldenberg, C.; Téllez-Rojo, M.M.; Meeker, J.D. Prenatal and peripubertal phthalates and bisphenol A in relation to sex hormones and puberty in boys. Reprod. Toxicol. 2014, 47, 70–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mikołajewska, K.; Stragierowicz, J.; Gromadzińska, J. Bisphenol A—Application, sources of exposure and potential risks in infants, children and pregnant women. Int. J. Occup. Med. Environ. Heal. 2015, 28, 209–241. [Google Scholar] [CrossRef] [PubMed]
- Wigle, D.T.; Turner, M.C.; Krewski, D. A systematic review and meta-analysis of childhood leukemia and parental occupational pesticide exposure. Environ. Heal. Perspect. 2009, 117, 1505–1513. [Google Scholar] [CrossRef] [PubMed]
- Darbre, P.D. Environmental oestrogens, cosmetics and breast cancer. Best Pract. Res. Clin. Endocrinol. Metab. 2006, 20, 121–143. [Google Scholar] [CrossRef] [PubMed]
- Darbre, P.D.; Harvey, P.W. Paraben esters: Review of recent studies of endocrine toxicity, absorption, esterase and human exposure, and discussion of potential human health risks. J. Appl. Toxicol. 2008, 28, 561–578. [Google Scholar] [CrossRef] [PubMed]
- Trasande, L.; Zoeller, R.T.; Hass, U.; Kortenkamp, A.; Grandjean, P.; Myers, J.P.; DiGangi, J.; Hunt, P.M.; Rudel, R.; Sathyanarayana, S.; et al. Burden of disease and costs of exposure to endocrine disrupting chemicals in the European Union: An updated analysis. Andrology 2016, 4, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Troisi, J.; Mikelson, C.; Richards, S.; Symes, S.; Adair, D.; Zullo, F.; Guida, M. Placental concentrations of bisphenol A and birth weight from births in the Southeastern U.S. Placenta 2014, 35, 947–952. [Google Scholar] [CrossRef] [PubMed]
- Veiga-Lopez, A.; Kannan, K.; Liao, C.; Ye, W.; Domino, S.E.; Padmanabhan, V. Gender-specific effects on gestational length and birth weight by early pregnancy BPA exposure. J. Clin. Endocrinol. Metab. 2015, jc20151724. [Google Scholar] [CrossRef] [PubMed]
- Maitre, L.; Fthenou, E.; Athersuch, T.; Coen, M.; Toledano, M.B.; Holmes, E.; Kogevinas, M.; Chatzi, L.; Keun, H.C. Urinary metabolic profiles in early pregnancy are associated with preterm birth and fetal growth restriction in the Rhea mother-child cohort study. BMC Med. 2014, 12, 110. [Google Scholar] [CrossRef] [PubMed]
- Kalkbrenner, A.E.; Schmidt, R.J.; Penlesky, A.C. Environmental chemical exposures and autism spectrum disorders: A review of the epidemiological evidence. Curr. Probl. Pediatr. Adolesc. Heal. Care 2014, 44, 277–318. [Google Scholar] [CrossRef] [PubMed]
- Braun, J.M.; Kalkbrenner, A.E.; Just, A.C.; Yolton, K.; Calafat, A.M.; Sjödin, A.; Hauser, R.; Webster, G.M.; Chen, A.; Lanphear, B.P. Gestational exposure to endocrine-disrupting chemicals and reciprocal social, repetitive, and stereotypic behaviors in 4- and 5-year-old children: The HOME study. Environ. Heal. Perspect. 2014, 122, 513–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braun, J.M.; Yolton, K.; Stacy, S.L.; Erar, B.; Papandonatos, G.D.; Bellinger, D.C.; Lanphear, B.P.; Chen, A. Prenatal environmental chemical exposures and longitudinal patterns of child neurobehavior. Neurotoxicology 2017, 62, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Gascon, M.; Casas, M.; Morales, E.; Valvi, D.; Ballesteros-Gómez, A.; Luque, N.; Rubio, S.; Monfort, N.; Ventura, R.; Martínez, D.; et al. Prenatal exposure to bisphenol A and phthalates and childhood respiratory tract infections and allergy. J. Allergy Clin. Immunol. 2015, 135, 370–378. [Google Scholar] [CrossRef] [PubMed]
- Guida, M.; Troisi, J.; Ciccone, C.; Granozio, G.; Cosimato, C.; Di Spiezio Sardo, A.; Ferrara, C.; Guida, M.; Nappi, C.; Zullo, F.; et al. Bisphenol A and congenital developmental defects in humans. Mutat. Res. 2015, 774, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Michalakis, M.; Tzatzarakis, M.N.; Kovatsi, L.; Alegakis, A.K.; Tsakalof, A.K.; Heretis, I.; Tsatsakis, A. Hypospadias in offspring is associated with chronic exposure of parents to organophosphate and organochlorine pesticides. Toxicol. Lett. 2014, 230, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Kalfa, N.; Paris, F.; Soyer-Gobillard, M.-O.; Daures, J.-P.; Sultan, C. Prevalence of hypospadias in grandsons of women exposed to diethylstilbestrol during pregnancy: A multigenerational national cohort study. Fertil. Steril. 2011, 95, 2574–2577. [Google Scholar] [CrossRef] [PubMed]
- Cohn, B.A.; La Merrill, M.; Krigbaum, N.Y.; Yeh, G.; Park, J.-S.; Zimmermann, L.; Cirillo, P.M. DDT exposure in utero and breast cancer. J. Clin. Endocrinol. Metab. 2015, 100, 2865–2872. [Google Scholar] [CrossRef] [PubMed]
- Herbst, A.L.; Scully, R.E. Adenocarcinoma of the vagina in adolescence. A report of 7 cases including 6 clear-cell carcinomas (so-called mesonephromas). Cancer 1970, 25, 745–757. [Google Scholar] [CrossRef]
- Fénichel, P.; Brucker-Davis, F.; Chevalier, N. The history of Distilbène® (Diethylstilbestrol) told to grandchildren—The transgenerational effect. Ann. Endocrinol. 2015, 76, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Tournaire, M.; Devouche, E.; Espié, M.; Asselain, B.; Levadou, A.; Cabau, A.; Dunbavand, A.; Grosclaude, P.; Epelboin, S. Cancer risk in women exposed to diethylstilbestrol in utero. Thérapie 2015, 70, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Svingen, T.; Vinggaard, A.M. The risk of chemical cocktail effects and how to deal with the issue. J. Epidemiol. Community Heal. 2016, 70, 322–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kortenkamp, A. Low dose mixture effects of endocrine disrupters and their implications for regulatory thresholds in chemical risk assessment. Curr. Opin. Pharmacol. 2014, 19, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Gaudriault, P.; Mazaud-Guittot, S.; Lavoué, V.; Coiffec, I.; Lesné, L.; Dejucq-Rainsford, N.; Scholze, M.; Kortenkamp, A.; Jégou, B. Endocrine disruption in human fetal testis explants by individual and combined exposures to selected pharmaceuticals, pesticides, and environmental pollutants. Environ. Heal. Perspect. 2017, 125, 087004. [Google Scholar] [CrossRef] [PubMed]
- Delfosse, V.; Dendele, B.; Huet, T.; Grimaldi, M.; Boulahtouf, A.; Gerbal-Chaloin, S.; Beucher, B.; Roecklin, D.; Muller, C.; Rahmani, R.; et al. Synergistic activation of human pregnane X receptor by binary cocktails of pharmaceutical and environmental compounds. Nat. Commun. 2015, 6, 8089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- French National Authority for Health (HAS). Improving Information Provision for Pregnant Women. Available online: http://www.has-sante.fr/portail/jcms/c_454394/fr/comment-mieux-informer-les-femmes-enceintes (accessed on 20 August 2018).
- Stotland, N.E.; Sutton, P.; Trowbridge, J.; Atchley, D.S.; Conry, J.; Trasande, L.; Gerbert, B.; Charlesworth, A.; Woodruff, T.J. Counseling patients on preventing prenatal environmental exposures—A mixed-methods study of obstetricians. PLoS ONE 2014, 9, e98771. [Google Scholar] [CrossRef] [PubMed]
- Di Renzo, G.C.; Conry, J.A.; Blake, J.; DeFrancesco, M.S.; DeNicola, N.; Martin, J.N.; McCue, K.A.; Richmond, D.; Shah, A.; Sutton, P.; et al. International Federation of Gynecology and Obstetrics opinion on reproductive health impacts of exposure to toxic environmental chemicals. Int. J. Gynecol. Obstet. 2015, 131, 219–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sathyanarayana, S.; Focareta, J.; Dailey, T.; Buchanan, S. Environmental exposures: How to counsel preconception and prenatal patients in the clinical setting. Am. J. Obstet. Gynecol. 2012, 207, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Habert, R. Impact des facteurs environnementaux sur la reproduction masculine [Impact of environment factors on male reproduction]. La Lettre du Gynécologue 2014, 16–21. [Google Scholar]
- Ferrari, R.M.; Siega-Riz, A.M.; Evenson, K.R.; Moos, M.-K.; Carrier, K.S. A qualitative study of women’s perceptions of provider advice about diet and physical activity during pregnancy. Patient Educ. Couns. 2013, 91, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Aubin-Auger, I.; Mercier, A.; Baumann, L. Introduction à la recherche qualitative [Introduction to qualitative research]. Exercer la Revue Française de Médecine Générale 2008, 84, 142–145. [Google Scholar]
- Rouillon, S.; Deshayes-Morgand, C.; Enjalbert, L.; Rabouan, S.; Hardouin, J.-B.; Group DisProSE; Migeot, V.; Albouy-Llaty, M. Endocrine disruptors and pregnancy: Knowledge, attitudes and prevention behaviors of French women. Int. J. Environ. Res. Public. Heal. 2017, 14. [Google Scholar] [CrossRef] [PubMed]
- Huang, R. RQDA: R-Based Qualitative Data Analysis. R Package Version 0.2-8. Available online: http://rqda.r-forge.r-project.org/ (accessed on 9 October 2018).
- Wallston, K.; Wallston, B.; DeVellis, R. Development of the multidimensional health locus of control (MHLC) scales. Heal. Educ. Behav. 1978. [Google Scholar] [CrossRef]
- Bruchon-Schweitzer, M. Psychologie de la Santé—Modèles, Concepts et Méthodes [Health Psychology. Models, Concepts and Methods]; Dunod: Paris, France, 2002. [Google Scholar]
- Vallieres, E.; Vallerand, R. Traduction Et Validation Canadienne-Française De L’échelle De L’estime De Soi De Rosenberg [The Rosenberg’s self esteem scale—French-Canadian translation and validation]. Int. J. Psychol. 1990. [Google Scholar] [CrossRef]
- Slovic, P. Perception of risk. Science 1987, 236, 280–285. [Google Scholar] [CrossRef] [PubMed]
- De Zwart, O.; Veldhuijzen, I.K.; Elam, G.; Aro, A.R.; Abraham, T.; Bishop, G.D.; Voeten, H.A.C.M.; Richardus, J.H.; Brug, J. Perceived threat, risk perception, and efficacy beliefs related to SARS and other (emerging) infectious diseases: Results of an international survey. Int. J. Behav. Med. 2009, 16, 30–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Che, S.-R.; Barrett, E.S.; Velez, M.; Conn, K.; Heinert, S.; Qiu, X. Using the health belief model to illustrate factors that influence risk assessment during pregnancy and implications for prenatal education about endocrine disruptors. Policy Futur. Educ. 2014, 12, 961–974. [Google Scholar] [CrossRef]
- French Agency for Food, Environmental and Occupational Health & Safety (ANSES). Évaluation des Risques du Bisphénol A (BPA) Pour la Santé Humaine [Risk Assessment of Bisphenol A (BPA) on Human Health]. Available online: https://www.anses.fr/fr/system/files/CHIM2009sa0331Ra-0.pdf (accessed on 9 October 2018).
- Boissonnot, R. Risques Sanitaires et Perception Chez Les Agriculteurs Utilisateurs de Produits Phytopharmaceutiques [Health Risks and Perception among Farmers Users of Plant Protection Products. Food and Nutrition]. Conservatoire National Des Arts et Metiers—CNAM: Paris, France. Available online: https://tel.archives-ouvertes.fr/tel-01136658 (accessed on 9 October 2018).
- Chauvin, B. La Perception des Risques [The risk perception]; De Boeck Superieur: Paris, France, 2014. [Google Scholar]
- Dosman, D.M.; Adamowicz, W.L.; Hrudey, S.E. Socioeconomic determinants of health-and food safety-related risk perceptions. Risk Anal. Off. Publ. Soc. Risk Anal. 2001, 21, 307–317. [Google Scholar] [CrossRef]
- Grason, H.A.; Misra, D.P. Reducing exposure to environmental toxicants before birth: Moving from risk perception to risk reduction. Public Heal. Rep. 2009, 124, 629–641. [Google Scholar] [CrossRef] [PubMed]
- Orfali, B.; Joffe, H. From the perception to the representation of risks: The media-mind link. Hermès 2005, 121–129. [Google Scholar] [CrossRef]
- Julia, C.; Péneau, S.; Buscail, C.; Gonzalez, R.; Touvier, M.; Hercberg, S.; Kesse-Guyot, E. Perception of different formats of front-of-pack nutrition labels according to sociodemographic, lifestyle and dietary factors in a French population: Cross-sectional study among the NutriNet-Santé cohort participants. BMJ Open 2017. [Google Scholar] [CrossRef] [PubMed]
- Institute of Radioprotection and Nuclear Safety. Baromètre (IRSN) 2014: La Perception des Risques et de la Sécurité par les Français. Available online: http://www.irsn.fr/FR/IRSN/Publications/barometre/Documents/IRSN_Barometre_2014.pdf (accessed on 20 August 2018).
- Institute of Radioprotection and Nuclear Safety. Baromètre (IRSN) 2015: La Perception des Risques et de la Sécurité par les Français. Available online: http://www.irsn.fr/FR/IRSN/Publications/barometre/Documents/IRSN_Barometre_2015.pdf (accessed on 20 August 2018).
- Davidson, D.J.; Freudenburg, W.R. Gender and environmental risk concerns: A review and analysis of available research. Environ. Behav. 1996, 28, 302–339. [Google Scholar] [CrossRef]
- World Health Organization. Rapport sur la Santé dans le Monde [Report on Health in the World]. Available online: http://www.who.int/whr/2002/en/chapter3fr.pdf (accessed on 9 October 2018).
- Guyon, L.; Audet, C.; April, N.; De Koninck, M. Tabagisme et grossesse. Représentations sociales chez des mères québécoises [Smoking and pregnancy. Social representations in Quebec mothers]. Drogue Santé Société 2007, 6, 105. [Google Scholar] [CrossRef] [Green Version]
- Thierauf, A.; Weinmann, W.; Auwärter, V.; Vennemann, B.; Bohnert, M. A survey of warning colours of pesticides. Forensic Sci. Med. Pathol. 2010, 6, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Doria, M.F. Bottled water versus tap water: Understanding consumers’ preferences. J. Water Heal. 2006, 4, 271–276. [Google Scholar] [CrossRef]
- Abtey, C. La Confiance Chez les Femmes Primipares de la Grossesse au Post-Partum [Confidence in Primiparous Women from Pregnancy to Post-Partum]. University of Nantes: Nantes, France. Available online: https://tel.archives-ouvertes.fr/tel-00347470 (accessed on 9 October 2018).
- Tansey, J.; O’Riordan, T. Cultural theory and risk: A review. Health Risk Soc. 1999, 1, 71–90. [Google Scholar] [CrossRef]



| Characteristic | N | % |
|---|---|---|
| Status | ||
| Pregnancy | 153 | 51.0 |
| Postpartum period | 147 | 49.0 |
| Cared for by | ||
| University Hospital | 193 | 64.3 |
| Local hospital | 38 | 12.7 |
| Private clinic | 20 | 6.7 |
| External office | 49 | 16.3 |
| Age (years old) | ||
| 18–25 | 33 | 11.0 |
| 26–35 | 206 | 68.7 |
| >35 | 61 | 20.3 |
| Educational Level | ||
| Missing data | 22 | 7.3 |
| Elementary, secondary school (N, %) | 29 | 9.7 |
| High school (N, %) | 35 | 11.7 |
| University level (N, %) | 214 | 71.3 |
| Verbatim |
|---|
| “[…] when you apply a cream on your skin and you have an allergy, maybe this is due to parabens or perfume […], these are things to be avoided” (FG). |
| “As I am allergic to parabens, every time I buy a cosmetic product or a personal hygiene product, […], I always look at the label” (PW No. 2). |
| “Pregnant women talked about the fear that their child would be likely to develop allergies” (FG). |
| “Pregnant women didn’t really evoke the low birth weight” (FG). |
| “It [EDC] is not good because according to them [pregnant women] it goes to the blood, and it is bad for the health” (FG). |
| “[pregnant women] really have the impression that the skin is a barrier, so nothing can pass through it” (FG). |
| Determinants | Verbatim |
|---|---|
| Age | “the more the women are advanced in age, in pregnancies, the more likely they are to be concerned about that, because they take time to read and get informed” (FG, participant No. 1). “[A young woman] has other concerns, such as unwanted pregnancies among those with precarious social backgrounds” (FG, participant No. 2). |
| Strong maternal figure | “So, it is always the mom who has, I think, a big influence on a pregnant woman, the patient’s mother really has an advisory role and sometimes she is more listened to than the midwife” (FG, participant No. 1). “[…] not necessarily towards their mother, but a strong maternal figure anyway” (FG, participant No. 1). “because the mother already had children, she knows what to do in such or such a case” (FG, participant No. 1). “What were you told, my girl? I had many children and had no problems with that, it doesn’t matter” (FG, participant No. 6). |
| Socio-economic category | “Regarding bisphenol-A, the moms who came to see me to ask what can be used as baby bottles, they were people with a higher socio-economic level” (FG, participant No. 2). “the (women with) lower socio-economic background used more canned food” (FG, participant No. 2). The interviewed women with a higher intellectual or intermediate profession consumed little canned food, whereas the unemployed women admitted to consuming cans of food, without indicating the frequency.—We found that unemployed women cooked some of their food in microwave oven, in plastic containers, whereas women having a higher intellectual profession avoided it. |
| Level of information: - Level of knowledge about EDC - Media visibility | “bisphenol-A, they [pregnant women] understand, because there was the big issue with it, there were the baby bottles made of bisphenol-A” (FG, participant No. 1); “[parabens] were mediatized as bad products and people tried to remove them as best they could” (PW No. 12, about cosmetics containing parabens). “we have seen that bisphenol-A is now forbidden” (PW No. 4). “The communication of manufacturers on labels without parabens, or without bisphenol A, is contributory [to heightened EDC risk perception]” (FG, participant No. 5). Mediatized information about EDC was perceived by pregnant women as: Stressful: “[…] Scientific considerations, which can also be stressful, even counterproductive” (FG, participant No. 7). Incomprehensible: “It still raises a problem for them because labels are incomprehensible” (FG, participant No. 1), “I find it is really hard to analyze labels” (PW No. 4, about choice of cosmetics). |
| Invisibility and ubiquity of EDC exposure (Involuntary exposure) | “It [EDC] is less visible [than alcohol or tobacco], on the bottle we can see it, on the pack of cigarettes we can see it” (FG, participant No. 1). “It [EDC] can be toxic, like cigarettes, tobacco, alcohol, but it is less visible” (FG, participant No. 2). “Tobacco is smoked; alcohol is drunk, whereas for the EDCs we cannot talk about “air consumption” or “container consumption” and it makes a big difference” (FG, participant No. 2). “That is what is stressful about them [of EDC], we do not know, we do not see” (FG, participant No. 1) |
| Determinant | n | % | Mean score of EDC Risk Perception | CI 95% | Crude β | 95% CI | p | Adjusted β | 95% CI | p | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age (years old) | 0.004 | 0.032 | ||||||||||||
| 18–25 | 33 | 11.0 | 48.7 | [42.5; 54.9] | Ref | Ref | ||||||||
| 26–35 | 206 | 68.7 | 54.1 | [51.6; 56.6] | 5.4 | [−1.3; 12.1] | 4.2 | [−2.6; 10.9] | ||||||
| >35 | 61 | 20.3 | 61.2 | [56.6; 65.7] | 12.4 | [4.7; 20.1] | 9.7 | [1.9; 17.6] | ||||||
| Knowledge Score | <0.0001 | <0.0001 | ||||||||||||
| Q1 | 93 | 31.0 | 46.3 | [42.8; 49.7] | Ref | Ref | ||||||||
| Q2 | 63 | 21.0 | 53.1 | [48.9; 57.3] | 6.8 | [1.3; 12.4] | 8.2 | [2.4; 14.1] | ||||||
| Q3 | 71 | 23.7 | 59.6 | [55.6; 63.6] | 13.4 | [8.1; 18.7] | 12.6 | [7.1; 18.2] | ||||||
| Q4 | 73 | 24.3 | 63.1 | [59.2; 67.1] | 16.9 | [11.6; 22.1] | 15.8 | [10.1; 21.6] | ||||||
| Educational Level | 0.076 | 0.900 | ||||||||||||
| Missing Data | 22 | 7.3 | N/A | N/A | N/A | N/A | ||||||||
| Elementary, Secondary School | 29 | 9.7 | 48.0 | [41.3; 54.7] | Ref | Ref | ||||||||
| High School | 35 | 11.7 | 54.8 | [48.7; 60.9] | 6.8 | [−2.3; 15.9] | 1.9 | [−6.8; 10.5] | ||||||
| University Level | 214 | 71.3 | 56.3 | [53.8; 58.7] | 8.3 | [1.1; 15.4] | 1.6 | [−5.7; 8.8] | ||||||
| Status | 0.070 | 0.159 | ||||||||||||
| Pregnancy | 153 | 50.3 | 53.7 | [50.2; 56.0] | Ref | Ref | ||||||||
| Postpartum Period | 147 | 49.7 | 56.9 | [54.0; 59.9] | 3.8 | [−0.3; 8.0] | 3.0 | [−1.2; 7.1] | ||||||
| Locus of Control (Internal) | 0.064 | 0.243 | ||||||||||||
| ≤Median | 136 | 45.3 | 52.8 | [49.7; 55.9] | Ref | Ref | ||||||||
| >Median | 164 | 54.7 | 56.8 | [54.0; 59.6] | 3.9 | [−0.2; 8.1] | 2.4 | [−1.7; 6.5] | ||||||
| Locus of Control (Chance) | 0.410 | NS | ||||||||||||
| ≤Median | 143 | 47.7 | 55.9 | [52.9; 58.9] | Ref | - | - | - | ||||||
| >Median | 157 | 52.3 | 54.1 | [51.2; 57.0] | 1.7 | [−2.3; 5.6] | - | - | - | |||||
| Locus of Control (Other Powerful Persons) | 0.470 | NS | ||||||||||||
| ≤Median | 148 | 49.3 | 55.7 | [52.8; 58.7] | Ref | - | - | - | ||||||
| >Median | 152 | 50.7 | 54.2 | [51.3; 57.1] | 1.5 | [−2.5; 5.4] | - | - | - | |||||
| Invisibility of Risk: “Regarding my own health, I only believe what I see” | 0.019 | 0.060 | ||||||||||||
| Strongly disagree | 35 | 11.7 | 63.0 | [57.0; 69.1] | Ref | Ref | ||||||||
| Disagree | 150 | 50.0 | 54.2 | [51.3; 57.1] | −8.8 | [−15.5; −2.1] | −7.7 | [−14.2; −1.1] | ||||||
| Agree | 99 | 33.0 | 52.5 | [48.9; 56.1] | −10.5 | [−17.6; −3.5] | −8.1 | [−15.0; −1.1] | ||||||
| Strongly agree | 16 | 5.33 | 59.6 | [50.6; 68.5] | −3.5 | [−14.3; 7.3] | −1.5 | [−12.1; 9.1] | ||||||
| Strong Maternal Figure | 0.657 | NS | ||||||||||||
| Spouse | 199 | 66.3 | 55.7 | [53.1; 58.2] | Ref | - | - | - | ||||||
| Mother, grandmother, sister, mother-in-law, sister-in-law, aunt | 67 | 22.3 | 53.5 | [49.1; 57.9] | 2.2 | [−2.6; 7.1] | - | - | - | |||||
| Other relative | 34 | 11.4 | 53.8 | [47.6; 60.0] | 1.6 | [−4.8; 7.9] | - | - | - | |||||
| Self-esteem Score | 0.383 | NS | ||||||||||||
| Q1 | 82 | 27.3 | 57.1 | [53.1; 61.1] | Ref | - | - | - | ||||||
| Q2 | 68 | 22.7 | 52.0 | [47.7; 56.4] | 4.8 | [−0.8; 10.4] | - | - | - | |||||
| Q3 | 85 | 28.3 | 54.5 | [50.6; 58.4] | 2.5 | [−2.8; 7.8] | - | - | - | |||||
| Q4 | 65 | 21.7 | 56.0 | [51.5; 60.4] | 1.0 | [−4.7; 6.7] | - | - | - | |||||
| Perceived Health | 0.668 | NS | ||||||||||||
| Q1 | 78 | 26.0 | 53.5 | [49.4; 57.6] | Ref | - | - | - | ||||||
| Q2 | 74 | 24.7 | 54.7 | [50.5; 58.9] | 1.2 | [−4.7; 7.1] | - | - | - | |||||
| Q3 | 67 | 22.3 | 57.2 | [52.8; 61.6] | 3.8 | [−2.3; 9.8] | - | - | - | |||||
| Q4 | 81 | 27.0 | 54.8 | [50.8; 58.8] | 1.3 | [−4.4; 7.1] | - | - | - | |||||
| Perceived Anxiety Trait | 0.254 | NS | ||||||||||||
| Q1 | 76 | 25.3 | 55.5 | [51.4; 59.6] | Ref | - | - | - | ||||||
| Q2 | 78 | 26.0 | 51.8 | [47.7; 55.9] | −3.7 | [−9.5; 2.1] | - | - | - | |||||
| Q3 | 71 | 23.7 | 54.9 | [50.6; 59.2] | −0.6 | [−6.5; 5.4] | - | - | - | |||||
| Q4 | 75 | 25.0 | 57.7 | [53.6; 61.9] | 2.2 | [−3.7; 8.1] | - | - | - | |||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rouillon, S.; El Ouazzani, H.; Rabouan, S.; Migeot, V.; Albouy-Llaty, M. Determinants of Risk Perception Related to Exposure to Endocrine Disruptors during Pregnancy: A Qualitative and Quantitative Study on French Women. Int. J. Environ. Res. Public Health 2018, 15, 2231. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15102231
Rouillon S, El Ouazzani H, Rabouan S, Migeot V, Albouy-Llaty M. Determinants of Risk Perception Related to Exposure to Endocrine Disruptors during Pregnancy: A Qualitative and Quantitative Study on French Women. International Journal of Environmental Research and Public Health. 2018; 15(10):2231. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15102231
Chicago/Turabian StyleRouillon, Steeve, Houria El Ouazzani, Sylvie Rabouan, Virginie Migeot, and Marion Albouy-Llaty. 2018. "Determinants of Risk Perception Related to Exposure to Endocrine Disruptors during Pregnancy: A Qualitative and Quantitative Study on French Women" International Journal of Environmental Research and Public Health 15, no. 10: 2231. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15102231