Fruit and Vegetable Consumption among Immigrants in Portugal: A Nationwide Cross-Sectional Study


Abstract
:1. Introduction
2. Materials and Methods
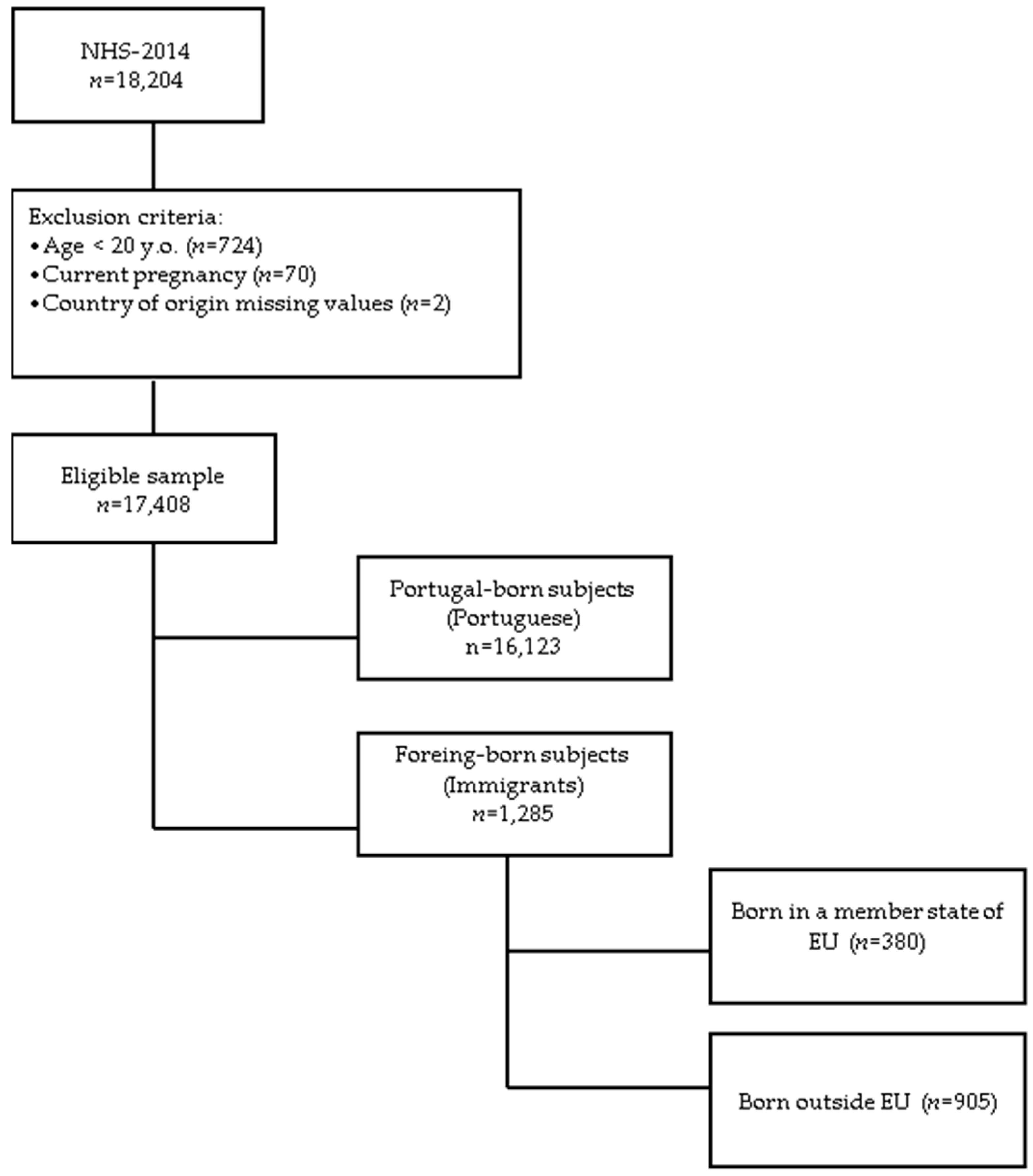
2.1. Population and Sample
2.2. Variables
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Diet, Nutrition and the Prevention of Chronic Diseases: Report of a Joint WHO/FAO Expert Consultation. Available online: http://apps.who.int/iris/bitstream/10665/42665/1/WHO_TRS_916.pdf?ua=1 (accessed on 20 May 2017).
- World Health Organization. Fruit and Vegetable Promotion Initiative: A Meeting Report, 25–27 August, Geneva. Available online: http://apps.who.int/iris/bitstream/10665/68395/1/WHO_NMH_NPH_NNP_0308.pdf (accessed on 20 May 2017).
- Gil, Á.; Martinez de Victoria, E.; Olza, J. Indicators for the evaluation of diet quality. Nutr. Hosp. 2015, 31 (Suppl. 3), 128–144. [Google Scholar] [PubMed]
- Slavin, J.L.; Lloyd, B. Health benefits of fruits and vegetables. Adv. Nutr. 2012, 3, 506–516. [Google Scholar] [CrossRef] [PubMed]
- Miller, V.; Mente, A.; Dehghan, M.; Rangarajan, S.; Zhang, X.; Swaminathan, S.; Dagenais, G.; Gupta, R.; Mohan, V.; Lear, S.; et al. Fruit, vegetable, and legume intake, and cardiovascular disease and deaths in 18 countries (PURE): A prospective cohort study. Lancet 2017, 390, 2037–2049. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Schwedhelm, C.; Hoffmann, G.; Lampousi, A.M.; Knüppel, S.; Iqbal, K.; Bechthold, A.; Schlesinger, S.; Boeing, H. Food groups and risk of all-cause mortality: A systematic review and meta-analysis of prospective studies. Am. J. Clin. Nutr. 2017, 105, 1462–1473. [Google Scholar] [CrossRef] [PubMed]
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 776–781. [Google Scholar] [CrossRef]
- Lopes, C.; Torres, D.; Oliveira, A.; Severo, M.; Alarcão, V.; Guiomar, S.; Mota, J.; Teixeira, P.; Rodrigues, S.; Lobato, L.; et al. Inquérito Alimentar Nacional e de Atividade Física 2015–2016. Available online: https://ian-af.up.pt/ (accessed on 3 October 2017).
- Eurostat. Migration and Migrant Population Statistics—Statistics Explained. Available online: http://ec.europa.eu/eurostat/statistics-explained/index.php/Migration_and_migrant_population_statistics (accessed on 23 August 2017).
- OECD. Foreign-Born Population (indicator). Available online: https://data.oecd.org/migration/foreign-born-population.htm (accessed on 23 August 2017).
- Wandel, M.; Råberg, M.; Kumar, B.; Holmboe-Ottesen, G. Changes in food habits after migration among South Asians settled in Oslo: The effect of demographic, socio-economic and integration factors. Appetite 2008, 50, 376–385. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, P.A.; Khokhar, S. Changing dietary habits of ethnic groups in Europe and implications for health. Nutr. Rev. 2008, 66, 203–215. [Google Scholar] [CrossRef] [PubMed]
- Popovic-Lipovac, A.; Strasser, B. A Review on Changes in Food Habits among Immigrant Women and Implications for Health. J. Immigr. Minor. Health 2015, 17, 582–590. [Google Scholar] [CrossRef] [PubMed]
- Satia-Abouta, J. Dietary acculturation: Definition, process, assessment, and implications. Int. J. Hum. Ecol. 2003, 4, 71–86. [Google Scholar]
- Sanou, D.; O’Reilly, E.; Ngnie-Teta, I.; Batal, M.; Mondain, N.; Andrew, C.; Newbold, B.K.; Bourgeault, I.L. Acculturation and nutritional health of immigrants in Canada: A scoping review. J. Immigr. Minor. Health 2014, 16, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Goulão, B.; Santos, O.; Carmo, I.D. The impact of migration on body weight: A review. Cad Saude Publica. 2015, 31, 229–245. [Google Scholar]
- Talegawkar, S.A.; Kandula, N.R.; Gadgil, M.D.; Desai, D.; Kanaya, A.M. Dietary intakes among South Asian adults differ by length of residence in the USA. Public Health Nutr. 2016, 19, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Satia-Abouta, J. Dietary acculturation and the nutrition transition: An overview. Appl. Physiol. Nutr. Metab. 2010, 35, 219–223. [Google Scholar]
- Leung, G.; Stanner, S. Diets of minority ethnic groups in the UK: Influence on chronic disease risk and implications for prevention. Nutr. Bull. 2011, 36, 161–198. [Google Scholar] [CrossRef]
- Raza, Q.; Snijder, M.B.; Seidell, J.C.; Peters, R.J.G.; Nicolaou, M. Comparison of cardiovascular risk factors and dietary intakes among Javanese Surinamese and South-Asian Surinamese in the Netherlands. The HELIUS study. BMC Res. Notes 2017, 10, 23. [Google Scholar] [CrossRef] [PubMed]
- Wang, K. Availability and Consumption of Fruits and Vegetables among Non-Hispanic Whites, Blacks, Hispanics, and Asians in the USA: Findings from the 2011–2012 California Health Interview Adult Survey. J. Racial Ethn. Health Disparities 2017, 4, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Tichenor, N.; Conrad, Z. Inter- and independent effects of region and race/ethnicity on variety of fruit and vegetable consumption in the USA: 2011 Behavioral Risk Factor Surveillance System (BRFSS). Public Health Nutr. 2016, 19, 104–113. [Google Scholar] [CrossRef] [PubMed]
- Satia, J.A. Diet-related disparities: Understanding the problem and accelerating solutions. J. Am. Diet. Assoc. 2009, 109, 610–615. [Google Scholar] [CrossRef] [PubMed]
- Yeh, M.-C.; Ickes, S.B.; Lowenstein, L.M.; Shuval, K.; Ammerman, A.S.; Farris, R.; Katz, D.L. Understanding barriers and facilitators of fruit and vegetable consumption among a diverse multi-ethnic population in the USA. Health Promot. Int. 2008, 23, 42–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landman, J.; Cruickshank, J.K. A review of ethnicity, health and nutrition-related diseases in relation to migration in the United Kingdom. Public Health Nutr. 2001, 4, 647–657. [Google Scholar] [CrossRef] [PubMed]
- Holmboe-Ottesen, G.; Wandel, M. Changes in dietary habits after migration and consequences for health: A focus on South Asians in Europe. Food Nutr. Res. 2012, 56. [Google Scholar] [CrossRef] [PubMed]
- Osei-Kwasi, H.A.; Nicolaou, M.; Powell, K.; Terragni, L.; Maes, L.; Stronks, K.; Lien, N.; Holdsworth, M. Systematic mapping review of the factors influencing dietary behaviour in ethnic minority groups living in Europe: A DEDIPAC study. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 85. [Google Scholar] [CrossRef] [PubMed]
- Dias, C.M. 25 anos de Inquérito Nacional de Saúde em Portugal. Available online: https://run.unl.pt/handle/10362/4409 (accessed on 10 April 2017).
- INE, INSA. Inquérito Nacional de Saúde 2014. Available online: https://www.ine.pt/xportal/xmain?xpid=INE&xpgid=ine_publicacoes&PUBLICACOESpub_boui=263714091&PUBLICACOEStema=55538&PUBLICACOESmodo=2 (accessed on 10 April 2017).
- Chkotua, S.; Peleteiro, B. Mammography Use in Portugal: National Health Survey 2014. Prev. Chronic. Dis. 2017, 14, E100. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; Strobe, I. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. BMJ 2007, 335, 806–808. [Google Scholar] [CrossRef] [PubMed]
- European Commission. European Health Interview Survey (EHIS wave 2)—Methodological manual. Available online: https://ec.europa.eu/eurostat/documents/3859598/5926729/KS-RA-13-018-EN.PDF/26c7ea80-01d8-420e-bdc6-e9d5f6578e7c (accessed on 13 January 2018).
- Da Costa, L.P.; Dias, S.F.; Martins, M.R.O. Association between length of residence and overweight among adult immigrants in Portugal: A nationwide cross-sectional study. BMC Public Health 2017, 17, 316. [Google Scholar] [CrossRef] [PubMed]
- The Asia-Pacific Perspective: Redefining Obesity and Its Treatment. Obesity: Preventing and Managing the Global Epidemic Geneva: WHO. 2000. Available online: http://www.wpro.who.int/nutrition/documents/docs/Redefiningobesity.pdf (accessed on 25 January 2016).
- Volken, T.; Rüesch, P.; Guggisberg, J. Fruit and vegetable consumption among migrants in Switzerland. Public Health Nutr. 2013, 16, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Kumar, B.N.; Grøtvedt, L.; Meyer, H.E.; Søgaard, A.-J.; Strand, B.H. The Oslo Immigrant Health Profile. Available online: https://brage.bibsys.no/xmlui/bitstream/handle/11250/220525/Kumar_2008_The.pdf?sequence=3 (accessed on 22 May 2017).
- Adebayo, F.A.; Itkonen, S.T.; Koponen, P.; Prättälä, R.; Härkänen, T.; Lamberg-Allardt, C.; Erkkola, M. Consumption of healthy foods and associated socio-demographic factors among Russian, Somali and Kurdish immigrants in Finland. Scand. J. Public Health 2017, 45, 277–287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayén, A.-L.; Marques-Vidal, P.; Paccaud, F.; Bovet, P.; Stringhini, S. Socioeconomic determinants of dietary patterns in low- and middle-income countries: A systematic review. Am. J. Clin. Nutr. 2014, 100, 1520–1531. [Google Scholar] [CrossRef] [PubMed]
- Kandola, K.; Sandhu, S.; Tang, T. Immigration and dietary patterns in South Asian Canadians at risk for diabetes. J. Diabetes Complicat. 2016, 30, 1462–1466. [Google Scholar] [CrossRef] [PubMed]
- Garduño-Diaz, S.D.; Khokhar, S. South Asian dietary patterns and their association with risk factors for the metabolic syndrome. J. Hum. Nutr. Diet. 2013, 26, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Ayala, G.X.; Baquero, B.; Klinger, S. A systematic review of the relationship between acculturation and diet among Latinos in the United States: Implications for future research. J. Am. Diet. Assoc. 2008, 108, 1330–1344. [Google Scholar] [CrossRef] [PubMed]
- Alegria, M. The Challenge of Acculturation Measures: What are we missing? A commentary on Thomson & Hoffman-Goetz. Soc. Sci. Med. 2009, 69, 996–998. [Google Scholar] [PubMed]
- Oliveira, C.R.D.; Gomes, N. Indicadores de Integração de Imigrantes. Relatório Estatístico Anual. Outubro de 2016, Coleção Imigração em Números. Observatório das Migrações. Available online: http://www.om.acm.gov.pt/publicacoes-om/colecao-imigracao-em-numeros/relatorios-anuais (accessed on 28 May 2017).
- Conde, W.L.; Monteiro, C.A. Nutrition transition and double burden of undernutrition and excess of weight in Brazil. Am. J. Clin. Nutr. 2014, 100, 1617S–1622S. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M. Synthesis and Implications: China’s Nutrition Transition in the Context of Changes Across other Low and Middle Income Countries. Obes. Rev. 2014, 15. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M. The shift in stages of the nutrition transition in the developing world differs from past experiences! Public Health Nutr. 2002, 5, 205–214. [Google Scholar] [PubMed]
- Gill, M.; Feliciano, D.; Macdiarmid, J.; Smith, P. The environmental impact of nutrition transition in three case study countries. Food Secur. 2015, 7, 493–504. [Google Scholar] [CrossRef] [Green Version]
- Malta, D.C.; Silva , J.B.D., Jr. O Plano de Ações Estratégicas para o Enfrentamento das Doenças Crônicas Não Transmissíveis no Brasil e a Definição das Metas Globais para o Enfrentamento Dessas Doenças até 2025: Uma Revisão. Epidemiologia Serviços Saúde 2013, 22, 151–164. [Google Scholar] [CrossRef]
- Du, S.; Lu, B.; Zhai, F.; Popkin, B.M. A new stage of the nutrition transition in China. Public Health Nutr. 2002, 5, 169–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaiyasong, S.; Huckle, T.; Mackintosh, A.-M.; Meier, P.; Parry, C.D.H.; Callinan, S.; Cuong, P.V.; Kazantseva, E.; Gray-Phillip, G.; Parker, K.; et al. Drinking patterns vary by gender, age and country-level income: Cross-country analysis of the International Alcohol Control Study. Drug Alcohol Rev. 2018, 37, S53–S62. [Google Scholar] [CrossRef] [PubMed]
- Sluik, D.; Bezemer, R.; Sierksma, A.; Feskens, E. Alcoholic Beverage Preference and Dietary Habits: A Systematic Literature Review. Crit. Rev. Food Sci. Nutr. 2016, 56, 2370–2382. [Google Scholar] [CrossRef] [PubMed]
- Breslow, R.A.; Guenther, P.M.; Smothers, B.A. Alcohol Drinking Patterns and Diet Quality: The 1999–2000 National Health and Nutrition Examination Survey. Am. J. Epidemiol. 2006, 163, 359–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erol, A.; Karpyak, V.M. Sex and gender-related differences in alcohol use and its consequences: Contemporary knowledge and future research considerations. Drug Alcohol Depend. 2015, 156, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Meshefedjian, G.A.; Leaune, V.; Simoneau, M.-È.; Drouin, M. Disparities in Lifestyle Habits and Health Related Factors of Montreal Immigrants: Is Immigration an Important Exposure Variable in Public Health? J. Immigr. Minor. Health 2014, 16, 790–797. [Google Scholar] [CrossRef] [PubMed]
- Azagba, S.; Sharaf, M.F. Disparities in the frequency of fruit and vegetable consumption by socio-demographic and lifestyle characteristics in Canada. Nutr. J. 2011, 10, 118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raza, Q.; Nicolaou, M.; Dijkshoorn, H.; Seidell, J.C. Comparison of general health status, myocardial infarction, obesity, diabetes, and fruit and vegetable intake between immigrant Pakistani population in the Netherlands and the local Amsterdam population. Ethn. Health 2017, 22, 551–564. [Google Scholar] [CrossRef] [PubMed]
- Raza, Q.; Nicolaou, M.; Snijder, M.B.; Stronks, K.; Seidell, J.C. Dietary acculturation among the South-Asian Surinamese population in the Netherlands: The HELIUS study. Public Health Nutr. 2017, 20, 1983–1992. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.; Wilmot, K.A.; Ghasemzadeh, N.; Molloy, D.L.; Burkman, G.; Mekonnen, G.; Gongora, M.C.; Quyyumi, A.A.; Sperling, L.S. Mediterranean Dietary Patterns and Cardiovascular. Health. Annu. Rev. Nutr. 2015, 35, 425–449. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Cesari, F.; Abbate, R.; Gensini, G.F.; Casini, A. Adherence to Mediterranean diet and health status: Meta-analysis. BMJ 2008, 337, a1344. [Google Scholar] [CrossRef] [PubMed]
- Lisboa, Portugal: Instituto Nacional de Estatística, I.P. Portuguese Food Balance Sheet 2012–2016. Available online: https://www.ine.pt/xportal/xmain?xpid=INE&xpgid=ine_publicacoes&PUBLICACOESpub_boui=290053341&PUBLICACOESmodo=2&xlang=en (accessed on 9 June 2017).
- Pomerleau, J.; Lock, K.; McKee, M.; Altmann, D.R. The Challenge of Measuring Global Fruit and Vegetable Intake. J. Nutr. 2004, 134, 1175–1180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agudo, A. Measuring Intake of Fruit and Vegetables. Workshop on Fruit and Vegetables for Health, 1–3 September 2004, Kobe, Japan. Available online: http://www.who.int/dietphysicalactivity/publications/f&v_intake_measurement.pdf. (accessed on 9 June 2017).
- Roark, R.A.; Niederhauser, V.P. Fruit and vegetable intake: Issues with definition and measurement. Public Health Nutr. 2013, 16, 2–7. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Portuguese | Immigrants | |||||
|---|---|---|---|---|---|---|
| Variables | T % (95% CI) | M % (95% CI) | F % (95% CI) | T % (95% CI) | M % (95% CI) | F % (95% CI) |
| n = 16,123 | n = 7037 | n = 9086 | n = 1285 | n = 539 | n = 746 | |
| Age (years) | ||||||
| 20–30 | 21.1 (20.4–25.9) | 22.6 (21.6–23.6) | 19.9 (19.1–21.7) | 22.5 (20.2–24.8) | 25.8 (22.1–29.5) | 19.8 (16.9–22.7) |
| 35–49 | 26.6 (25.9–27.3) | 27.7 (26.7–28.7) | 25.5 (24.6–26.4) | 45.5 (42.8–48.2) | 44.0 (39.8–41.2) | 46.8 (43.2–50.4) |
| 50–64 | 25.5 (24.8–26.2) | 25.7 (24.7–26.7) | 25.3 (24.4–26.2) | 23.4 (21.1–25.7) | 24.8 (21.2–28.4) | 22.1 (19.1–25.1) |
| 65+ | 26.8 (26.1–27.5) | 24.0 (23.0–25.0) | 29.3 (28.4–30.2) | 8.6 (7.1–10.1) | 5.4 (3.5–7.3) | 11.3 (9.0–13.6) |
| p value | 0.000 * | 0.000 ** | 0.000 ** | |||
| Education level | ||||||
| None or basic | 64.4 (63.7–65.1) | 65.6 (64.5–66.7) | 63.4 (62.4–64.4) | 38.9 (36.2–41.6) | 40.0 (35.9–44.1) | 37.9 (34.4–41.4) |
| Secondary | 17.2 (16.6–17.8) | 18.4 (17.5–19.3) | 16.2 (15.4–17.0) | 31.7 (29.2–34.2) | 34.4 (30.4–38.4) | 29.4 (26.1–32.7) |
| Higher education | 18.4 (17.8–19.0) | 16.0 (15.1–16.9) | 20.4 (19.6–21.2) | 29.4 (26.9–31.9) | 25.6 (21.9–29.3) | 32.6 (29.2–36.0) |
| p value | 0.000 * | 0.000 ** | 0.000 ** | |||
| Legal marital status | ||||||
| Married | 60.3 (59.5–61.1) | 64.0 (62.9–65.1) | 56.9 (55.9–57.9) | 54.9 (52.2–57.6) | 55.7 (51.5–59.9) | 54.2 (50.6–57.8) |
| p value | 0.000 * | 0.000 ** | 0.000 ** | |||
| Job status | ||||||
| Employed | 48.6 (47.8–49.4) | 54.0 (52.8–55.2) | 43.9 (42.9–44.9) | 62.2 (59.5–64.9) | 69.4 (65.5–73.3) | 56.0 (52.4–59.6) |
| p value | 0.000 * | 0.000 ** | 0.000 ** | |||
| Urbanisation degree | ||||||
| Densely | 42.2 (41.4–43.0) | 41.4 (40.2–42.6) | 42.9 (41.9–43.9) | 56.6 (53.9–59.3) | 54.8 (50.6–59.0) | 58.1 (54.6–61.6) |
| Intermediate | 30.1 (29.4–30.8) | 30.2 (29.1–31.3) | 30.0 (29.1–30.9) | 24.8 (22.4–27.2) | 27.5 (23.7–31.3) | 22.6 (19.6–25.6) |
| Thinly | 27.7 (27.0–28.4) | 28.4 (27.3–29.5) | 27.1 (26.2–28.0) | 18.6 (16.5–20.7) | 17.7 (14.5–20.9) | 19.3 (16.5–22.1) |
| p value | 0.000 * | 0.000 ** | 0.000 ** | |||
| Anthropometric | ||||||
| Overweight | 54.4 (53.6–55.2) | 58.8 (58.0–60.0) | 50.6 (50.0–51.6) | 47.4 (44.7–50.1) | 51.3 (47.1–55.5) | 44.1 (40.5–47.7) |
| p value | 0.000 * | 0.000 ** | 0.000 ** | |||
| F&V intake | ||||||
| ≥5 servings/day | 18.5 (17.9–19.1) | 15.7 (14.8–16.5) | 21.0 (20.2–21.8) | 21.1 (19.0–23.4) | 16.6 (13.5–19.7) | 25.0 (21.9–28.1) |
| p value | 0.000 * | 0.000 ** | 0.000 ** | |||
| Physical activity | ||||||
| Active | 63.4 (62.7–64.1) | 65.8 (66.9–69.1) | 60.5 (59.5–61.5) | 62.8 (60.2–65.4) | 64.5 (60.5–68.5) | 60.5 (57.0–64.0) |
| p value | 0.000 * | 0.000 ** | 0.000 ** | |||
| Smoke status | ||||||
| Current | 20.3 (19.7–20.9) | 28.8 (27.7–29.9) | 12.8 (12.1–13.5) | 23.7 (21.4–26.0) | 28.8 (25.0–32.6) | 19.4 (16.6–22.2) |
| p value | 0.000 * | 0.000 ** | 0.000 ** | |||
| Drinking classes | ||||||
| Regular | 46.1 (45.3–46.9) | 68.0 (66.9–69.1) | 26.9 (26.0–27.8) | 39.9 (37.2–42.6) | 57.5 (53.3–61.7) | 24.8 (21.7–27.9) |
| Light | 13.8 (13.3–14.3) | 12.6 (11.8–13.4) | 14.8 (14.1–15.5) | 18.5 (16.4–20.6) | 16.3 (13.2–19.4) | 20.4 (17.5–23.3) |
| Occasional | 40.1 (39.3–40.9) | 19.4 (18.5–20.3) | 58.3 (57.3–59.3) | 41.6 (38.9–44.3) | 26.2 (22.5–29.9) | 54.7 (51.1–58.3) |
| p value | 0.000 * | 0.000 | 0.000 | |||
| F&V ≥ 5 Servings per Day | ||||||
|---|---|---|---|---|---|---|
| Variables | Total | Men | Women | |||
| Unadjusted | Adjusted † | Unadjusted | Adjusted ‡ | Unadjusted | Adjusted ‡ | |
| Sociodemographic | ||||||
| Sex | ||||||
| Men | 1 | 1 | 1 | 1 | 1 | 1 |
| Women | 1.67 (1.65–1.69) * | 3.62 (3.54–3.70) * | n.a | n.a | n.a | n.a |
| Age | ||||||
| 20–34y | 1 | 1 | 1 | 1 | 1 | 1 |
| 35–39y | 2.50 (2.46–2.55) * | 3.35 (3.26–3.45) * | 2.70 (2.62–2.77) * | 3.44 (3.27–3.62) * | 2.25 (2.20–2.31) * | 4.44 (4.26–4.63) * |
| 50–64y | 1.81 (1.77–1.85) * | 2.00 (1.93–2.08) * | 1.10 (1.93–2.06) * | 3.20 (3.00–3.41) * | 1.65 (1.60–1.69) * | 2.02 (1.93–2.12) * |
| 65+ y | 3.60 (3.51–3.69) * | 8.10 (7.75–8.47) * | 4.83 (4.64–5.04) * | 21.19 (19.63–22.87) * | 2.73 (2.65–2.81) * | 5.69 (5.34–6.06) * |
| Education level | ||||||
| None or basic | 1 | 1 | 1 | 1 | 1 | 1 |
| High school | 1.32 (1.30–1.34) * | 1.94 (1.88–1.99) * | 1.49 (1.46–1.53) * | 1.62 (1.56–1.69) * | 1.25 (1.22–1.27) * | 1.61 (1.55–1.68) * |
| Higher educ. | 2.19 (2.16–2.22) * | 2.44 (2.37–2.51) * | 2.64 (2.58–2.71) * | 0.99 (0.95–1.03) | 1.88 (1.85–1.92) * | 3.66 (3.52–3.81) * |
| Legal marital status | ||||||
| Not married | 1 | 1 | 1 | 1 | 1 | 1 |
| Married | 1.16 (1.15–1.18) * | 0.61 (0.60–0.63) * | 1.28 (1.26–1.31) * | 0.78 (0.75–0.81) * | 1.11 (1.09–1.13) * | 0.48 (0.46–0.49) * |
| Job status | ||||||
| Not Employed | 1 | 1 | 1 | 1 | 1 | 1 |
| Employed | 1.24 (1.23–1.26) * | 1.28 (1.25–1.31) * | 1.79 (1.75–1.84) * | 1.76 (1.68–1.85) * | 1.17 (1.15–1.19) * | 0.91 (0.88–0.94) * |
| Urbanisation degree | ||||||
| Densely | 1 | 1 | 1 | 1 | 1 | 1 |
| Intermediate | 0.59 (0.58–0.60) * | 1.67 (1.63–1.71) * | 1.66 (1.62–1.70) * | 2.34 (2.25–2.42) * | 0.98 (0.97–1.00) | 1.59 (1.54–1.65) * |
| Thinly | 0.69 (0.68–0.70) * | 1.76 (1.71–1.81) * | 2.51 (2.45–2.58) * | 3.73 (3.56–3.91) * | 1.33 (1.31–1.36) * | 1.22 (1.18–1.26) * |
| Country of origin | ||||||
| Inside EU | 1 | 1 | 1 | 1 | 1 | 1 |
| Outside EU | 0.69 (0.68–0.70) * | 0.79 (0.77–0.81) * | 0.57 (0.56–0.58) * | 0.67 (0.64–0.69) * | 0.79 (0.77–0.80) * | 0.73 (0.71–0.75) * |
| Length of residence | ||||||
| 0–9 years | 1 | 1 | 1 | 1 | 1 | 1 |
| 10–14 years | 1.23 (1.10–1.15) * | 0.20 (0.19–0.21) * | 1.00 (0.97–1.04) | 0.05 (0.05–0.05) * | 1.27 (1.23–1.31) * | 0.46 (0.43–0.49) * |
| 15+ years | 1.32 (1.29–1.34) * | 0.52 (0.50–0.53) * | 0.72 (0.70–0.74) * | 0.27 (0.26–0.29) * | 2.10 (2.04–2.16) * | 1.03 (0.98–1.09) |
| Anthropometric | ||||||
| Body mass index | ||||||
| <25 kg/m2 | 1 | 1 | 1 | 1 | 1 | 1 |
| ≥25 kg/m2 | 0.83 (0.82–0.84) * | 0.59 (0.58–0.61) * | 1.05 (1.03–1.07) * | 0.64 (0.62–0.66) * | 0.75 (0.73–0.76) * | 0.62 (0.61–0.64) * |
| Lifestyle | ||||||
| Physical activity | ||||||
| Sedentary | 1 | 1 | 1 | 1 | 1 | 1 |
| Active | 1.24 (1.22–1.26) * | 1.43 (1.40–1.46) * | 1.72 (1.67–1.78) * | 1.50 (1.44–1.55) * | 1.11 (1.08–1.14) * | 1.13 (1.10–1.16) * |
| Smoking status | ||||||
| Never/ former | 1 | 1 | 1 | 1 | 1 | 1 |
| Current | 0.49 (0.48–0.50) * | 0.46 (0.45–0.47) * | 0.36 (0.35–0.37) * | 0.19 (0.18–0.20) * | 0.67 (0.66–0.69) * | 0.72 (0.69–0.74) * |
| Drinking classes | ||||||
| Regular | 1 | 1 | 1 | 1 | 1 | 1 |
| Light | 1.12 (1.10–1.14) * | 0.70 (0.68–0.72) * | 1.12 (1.09–1.15) * | 1.42 (1.36–1.48) * | 0.90 (0.88–0.92) * | 0.57 (0.55–0.59) * |
| Occasional | 0.99 (0.97–1.00) | 0.63 (0.61–0.64) * | 0.67 (0.66–0.69) * | 0.48 (0.46–0.50) * | 0.84 (0.83–0.86) * | 0.81 (0.78–0.84) * |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costa, L.; Dias, S.; Martins, M.D.R.O. Fruit and Vegetable Consumption among Immigrants in Portugal: A Nationwide Cross-Sectional Study. Int. J. Environ. Res. Public Health 2018, 15, 2299. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15102299
Costa L, Dias S, Martins MDRO. Fruit and Vegetable Consumption among Immigrants in Portugal: A Nationwide Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2018; 15(10):2299. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15102299
Chicago/Turabian StyleCosta, Liliane, Sónia Dias, and Maria Do Rosário O. Martins. 2018. "Fruit and Vegetable Consumption among Immigrants in Portugal: A Nationwide Cross-Sectional Study" International Journal of Environmental Research and Public Health 15, no. 10: 2299. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15102299