The Effect of Detraining after a Period of Training on Cardiometabolic Health in Previously Sedentary Individuals

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cardiometabolic Health
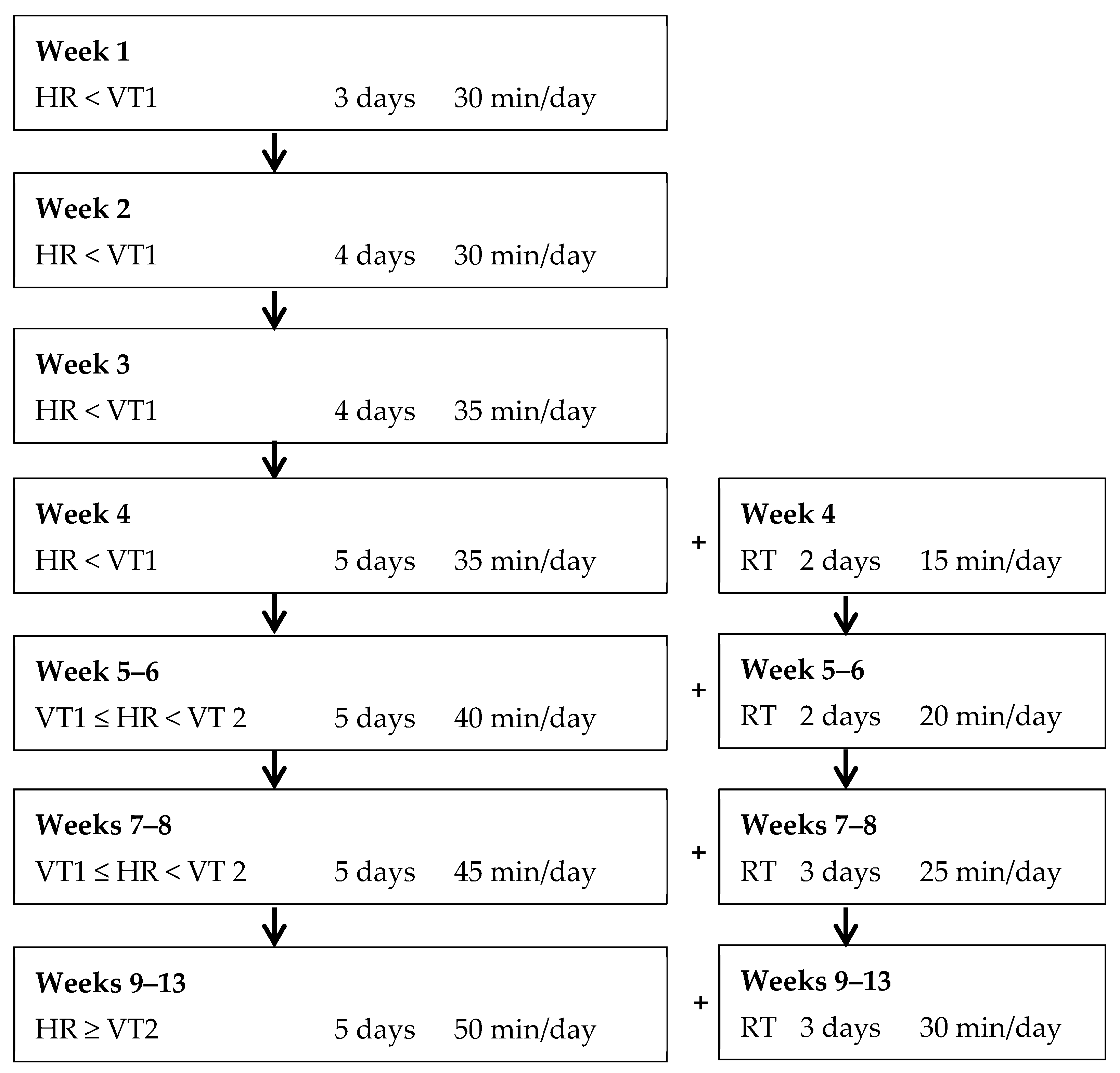
2.2. Exercise Prescription
2.3. Statistical Analyses
Post-Training Period
3. Results
3.1. Maintain Regular Exercise Training
3.2. Detrain from Exercise Training
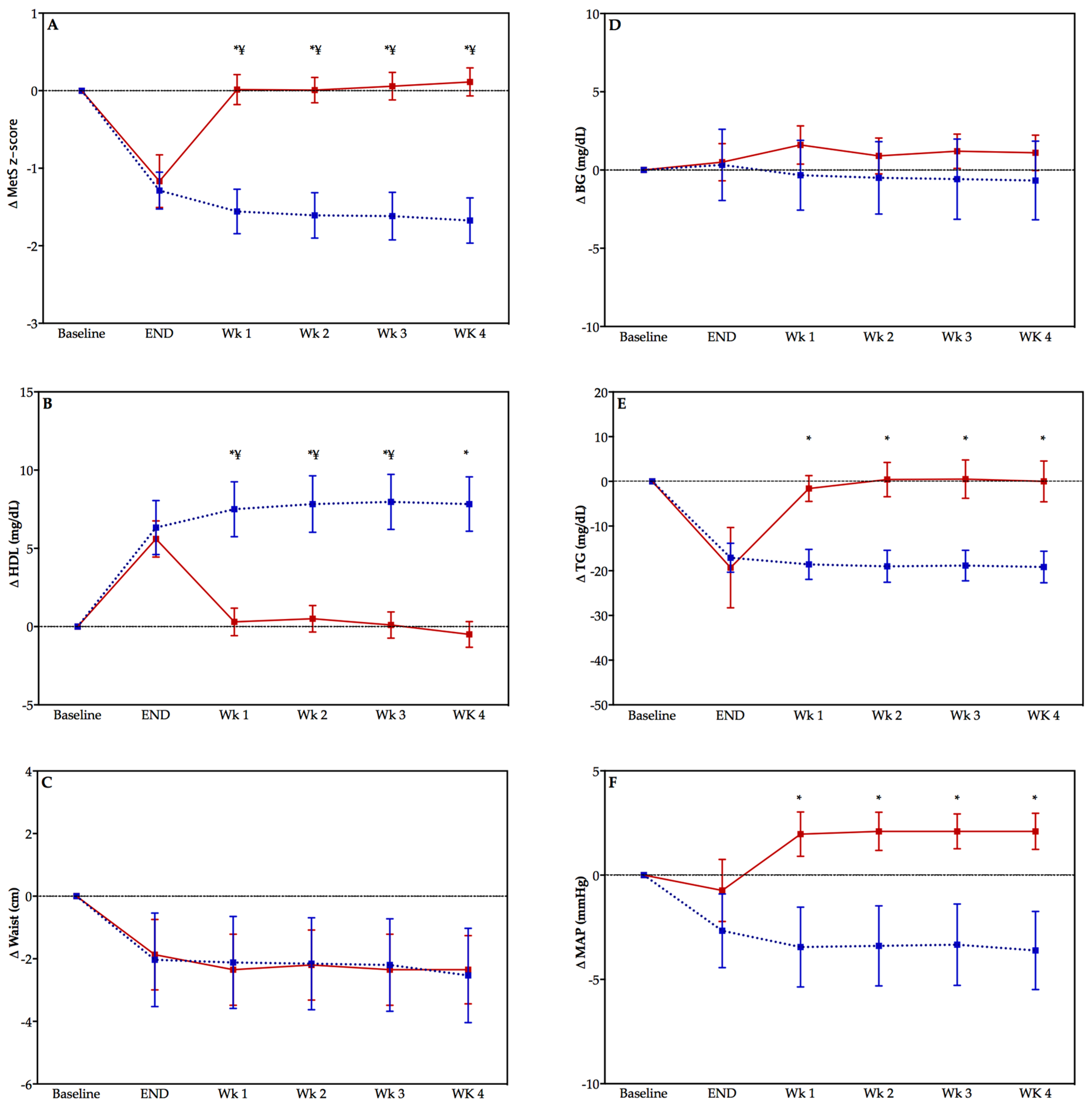
3.3. Change in Cardiometabolic Health in the Post-Training Period
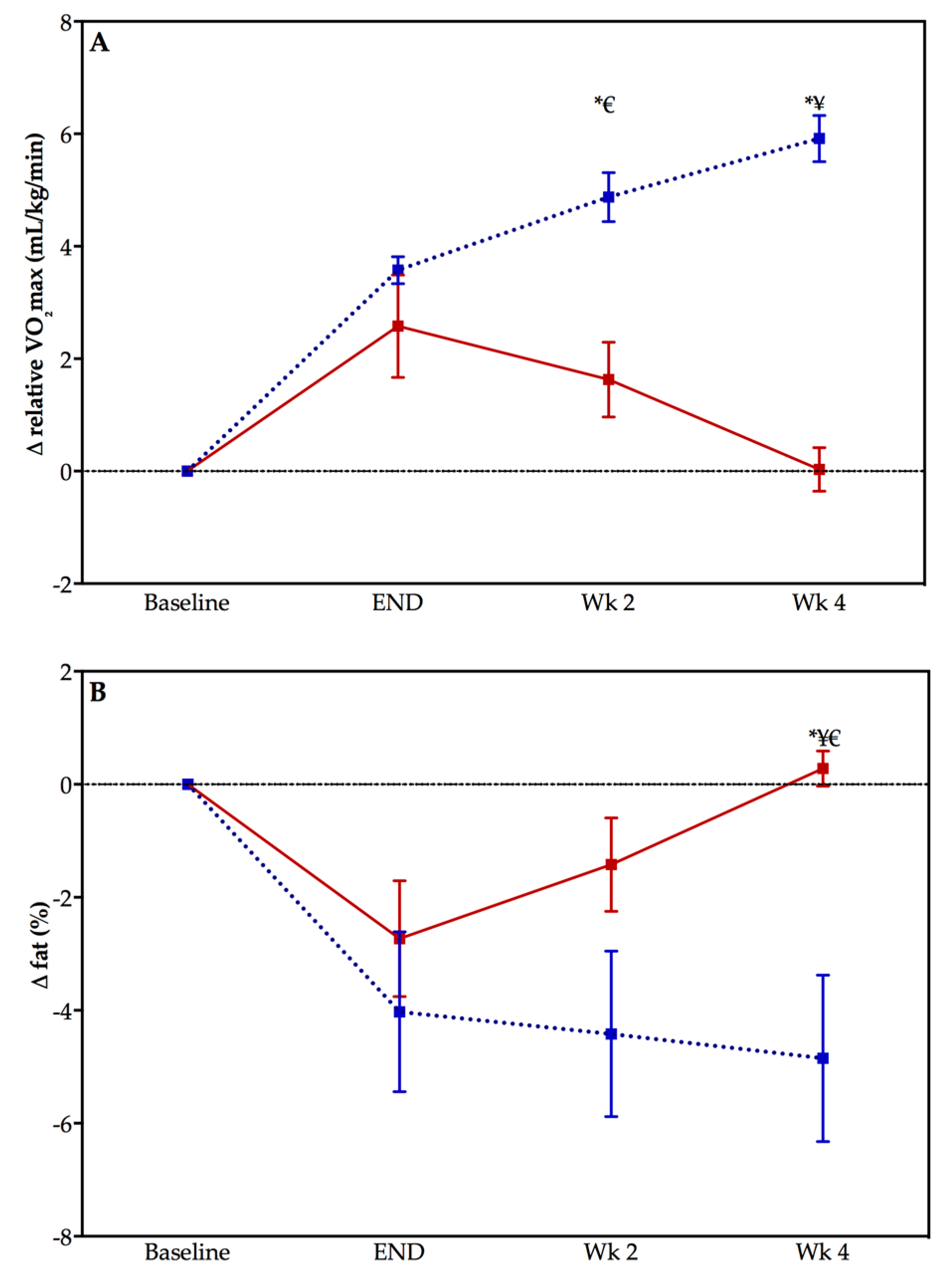
3.4. Change in CRF and Body Fat Percentage in the Post-Training Period
4. Discussion
4.1. Primary Prevention of Chronic Disease Perspective
4.2. Methodological Considerations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Blair, S.N.; Kampert, J.B.; Kohl, H.W.; Barlow, C.E.; Macera, C.A.; Paffenbarger, R.S.; Gibbons, L.W. Influences of cardiorespiratory fitness and other precursors on cardiovascular disease and all-cause mortality in men and women. J. Am. Med. Assoc. 1996, 276, 205–210. [Google Scholar] [CrossRef]
- Barlow, C.E.; DeFina, L.F.; Radford, N.B.; Berry, J.D.; Cooper, K.H.; Haskell, W.L.; Jones, L.W.; Lakoski, S.G. Cardiorespiratory fitness and long-term survival in “low-risk” adults. J. Am. Heart Assoc. 2012, 1, e001354. [Google Scholar] [CrossRef] [PubMed]
- Lavie, C.J.; Arena, R.; Swift, D.L.; Johannsen, N.M.; Sui, X.; Lee, D.C.; Earnest, C.P.; Church, T.S.; O’Keefe, J.H.; Milani, R.V.; et al. Exercise and the cardiovascular system: Clinical science and cardiovascular outcomes. Circ. Res. 2015, 117, 207–219. [Google Scholar] [CrossRef] [PubMed]
- Booth, F.W.; Gordon, S.E.; Carlson, C.J.; Hamilton, M.T.; Frank, W.; Gordon, S.E.; Carlson, C.J. Waging war on modern chronic diseases: Primary prevention through exercise biology. J. Appl. Physiol. 2000, 88, 774–787. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.; Sui, X.; Church, T.S.; Lavie, C.J.; Jackson, A.S.; Blair, S.N. Changes in fitness and fatness on the development of cardiovascular disease risk factors: Hypertension, metabolic syndrome, and hypercholesterolemia. J. Am. Coll. Cardiol. 2012, 59, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Morales-Palomo, F.; Ramirez-Jimenez, M.; Ortega, J.F.; Lopez-Galindo, P.L.; Fernandez-Martin, J.; Mora-Rodriguez, R. Effects of repeated yearly exposure to exercise-training on blood pressure and metabolic syndrome evolution. J. Hypertens. 2017, 35, 1992–1999. [Google Scholar] [CrossRef] [PubMed]
- Pescatello, L.S.; American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 9th ed.; Wolters Kluwer/Lippincott Williams & Wilkins Health: Philadelphia, PA, USA, 2014. [Google Scholar]
- Bryant, C.X.; Green, D.J. American Council on Exercise Personal Trainer Manual; American Council on Exercise: San Diego, CA, USA, 2010. [Google Scholar]
- Ramos, J.S.; Dalleck, L.C.; Borrani, F.; Beetham, K.S.; Wallen, M.P.; Mallard, A.R.; Clark, B.; Gomersall, S.; Keating, S.E.; Fassett, R.G.; et al. Low-volume high-intensity interval training is sufficient to ameliorate the severity of metabolic syndrome. Metab. Syndr. Relat. Disord. 2017, 15, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Malin, S.K.; Nightingale, J.; Choi, S.E.; Chipkin, S.R.; Braun, B. Metformin modifies the exercise training effects on risk factors for cardiovascular disease in impaired glucose tolerant adults. Obesity (Silver Spring) 2013, 21, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Wolpern, A.E.; Burgos, D.J.; Janot, J.M.; Dalleck, L.C. Is a threshold-based model a superior method to the relative percent concept for establishing individual exercise intensity? A randomized controlled trial. BMC Sports Sci. Med. Rehabil. 2015, 7, 16. [Google Scholar] [CrossRef] [PubMed]
- Dalleck, L.C.; Haney, D.E.; Buchanan, C.A.; Weatherwax, R.M. Does a personalised exercise prescription enhance training efficacy and limit training unresponsiveness? A randomised controlled trial. J. Fit. Res. 2016, 5, 15–27. [Google Scholar]
- Williams, P.T. Physical fitness and activity as separate heart disease risk factors: A meta-analysis. Med. Sci. Sports Exerc. 2001, 33, 754–761. [Google Scholar] [CrossRef] [PubMed]
- Blair, S.N. Physical inactivity: The biggest public health problem of the 21st century. Br. J. Sports Med. 2009, 43, 1–2. [Google Scholar] [PubMed]
- Lobelo, F.; Pate, R.R.; Dowda, M.; Liese, A.D.; Daniels, S.R. Cardiorespiratory fitness and clustered cardiovascular disease risk in U.S. adolescents. J. Adolesc. Health 2010, 47, 352–359. [Google Scholar] [CrossRef] [PubMed]
- Dela, F.; Mikines, K.J.; Von Linstow, M.; Secher, N.H.; Galbo, H. Effect of training on insulin-mediated glucose uptake in human muscle 20. Am. J. Physiol. 1992, 263, E1134–E1143. [Google Scholar] [PubMed]
- Bajpeyi, S.; Tanner, C.J.; Slentz, C.A.; Duscha, B.D.; McCartney, J.S.; Hickner, R.C.; Kraus, W.E.; Houmard, J.A. Effect of exercise intensity and volume on persistence of insulin sensitivity during training cessation. J. Appl. Physiol. 2009, 106, 1079–1085. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nikseresht, M.; Hafezi Ahmadi, M.R.; Hedayati, M. Detraining-induced alterations in adipokines and cardiometabolic risk factors after nonlinear periodized resistance and aerobic interval training in obese men. Appl. Physiol. Nutr. Metab. 2016, 41, 1018–1025. [Google Scholar] [CrossRef] [PubMed]
- Mora-Rodriguez, R.; Ortega, J.F.; Hamouti, N.; Fernandez-Elias, V.E.; Cañete Garcia-Prieto, J.; Guadalupe-Grau, A.; Saborido, A.; Martin-Garcia, M.; Guio de Prada, V.; Ara, I.; et al. Time-course effects of aerobic interval training and detraining in patients with metabolic syndrome. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 792–798. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.H.; Sung, Y.C.; Chou, C.C.; Chen, C.Y. Eight-week training cessation suppresses physiological stress but rapidly impairs health metabolic profiles and aerobic capacity in elite taekwondo athletes. PLoS ONE 2016, 11, e0160167. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameter | TRAIN (n = 12) | DETRAIN (n = 10) | ||
|---|---|---|---|---|
| Baseline | 13 Weeks | Baseline | 13 Weeks | |
| Age (years) | 40 ± 3 | ____ | 36 ± 5 | ____ |
| Height (cm) | 167.9 ± 1.9 | ____ | 169.7 ± 4.0 | ____ |
| Weight (kg) | 78.1 ± 8.6 | 78.9 ± 7.3 | 72.7 ± 16.2 | 72.2 ± 16.1 |
| Waist circumference (cm) | 86.5 ± 6.7 | 84.5 ± 3.6 | 81.7 ± 11.2 | 79.8 ± 10.1 |
| Body fat (%) | 31.1 ± 6.5 | 27.0 ± 2.2 * | 28.5 ± 7.0 | 25.8 ± 9.1 * |
| VO2max (mL·kg−1·min−1) | 30.6 ± 8.4 | 34.2 ± 8.7 * | 33.7 ± 9.4 | 36.3 ± 7.4 * |
| Systolic BP (mmHg) | 120 ± 4 ¥ | 117 ± 6 * | 113 ± 8 | 108 ± 14 |
| Diastolic BP (mmHg) | 82 ± 10 ¥ | 80 ± 7 | 72 ± 8 | 74 ± 7 |
| Total cholesterol (mg·dL−1) | 163 ± 34 | 177 ± 25 * | 188 ± 36 | 201 ± 34 |
| HDL cholesterol (mg·dL−1) | 55 ± 11 | 61 ± 14 * | 57 ± 15 | 63 ± 15 * |
| LDL cholesterol (mg·dL−1) | 89 ± 29 | 95 ± 19 | 112 ± 33 | 125 ± 41 * |
| Triglycerides (mg·dL−1) | 114 ± 28 | 97 ± 27 * | 112 ± 34 | 92 ± 23 |
| Blood glucose (mg·dL−1) | 92 ± 9 | 92 ± 11 | 92 ± 8 | 92 ± 7 |
| MetS z-score | −3.8 ± 1.9 ¥ | −5.1 ± 1.9 ¥,* | −5.9 ± 2.1 | −7.0 ± 1.9 * |
| Parameter | Post Program | +1 Week | +2 Weeks | +3 Weeks | +4 Weeks |
|---|---|---|---|---|---|
| Weight (kg) | 78.9 ± 7.3 | 78.6 ± 7.1 | 78.4 ± 7.5 | 78.3 ± 7.2 | 78.0 ± 7.2 |
| Waist circumference (cm) | 84.5± 3.6 | 84.4 ± 3.7 | 84.3 ± 3.7 | 84.3 ± 3.9 | 84.0 ± 3.7 |
| Body fat (%) | 27.1 ± 2.2 | ____ | 26.7 ± 2.4 | ____ | 26.3 ± 2.2 *,¥ |
| VO2max (mL·kg−1·min−1) | 34.2 ± 8.7 | ____ | 35.5 ± 8.3 * | ____ | 36.5 ± 8.0 *,¥ |
| Systolic BP (mmHg) | 117 ± 6 | 116 ± 6 | 116 ± 6 | 116 ± 6 | 115 ± 6 |
| Diastolic BP (mmHg) | 80 ± 7 | 79 ± 6 | 79 ± 5 | 79 ± 6 | 79 ± 5 |
| Total cholesterol (mg·dL−1) | 177 ± 25 | 176 ± 23 | 178 ± 23 | 178 ± 24 | 180 ± 25 |
| HDL cholesterol (mg·dL−1) | 61 ± 14 | 63 ± 13 | 63 ± 13 | 63 ± 13 | 63 ± 13 |
| LDL cholesterol (mg·dL−1) | 94 ± 18 | 93 ± 18 | 94 ± 19 | 93 ± 17 | 93 ± 17 |
| Triglycerides (mg·dL−1) | 97 ± 27 | 96 ± 22 | 95 ± 21 | 96 ± 21 | 95 ± 20 |
| Blood glucose (mg·dL−1) | 92 ± 11 | 92 ± 9 | 91 ± 9 | 91 ± 10 | 91 ± 10 |
| MetS z-score | −5.1 ± 1.9 | −5.3 ± 1.8 | −5.4 ± 1.8 | −5.4 ± 1.8 | −5.5 ± 1.8 |
| Parameter | Post-Program | +1 Week | +2 Weeks | +3 Weeks | +4 Weeks |
|---|---|---|---|---|---|
| Weight (kg) | 72.2 ± 16.1 | 72.4 ± 16.2 | 72.4 ± 16.5 | 72.6 ± 16.5 | 72.6 ± 16.5 |
| Waist circumference (cm) | 79.8 ± 10.1 | 79.4 ± 10.0 | 79.5 ± 10.1 | 79.4 ± 10.0 | 79.4 ± 9.9 |
| Body fat (%) | 25.8 ± 9.1 | ____ | 27.1 ± 8.5 | ____ | 28.8 ± 6.9 * |
| VO2max (mL·kg−1·min−1) | 36.3 ± 7.4 | ____ | 35.4 ± 8.0 | ____ | 33.8 ± 8.9 *,¥ |
| Systolic BP (mmHg) | 108 ± 14 | 114 ± 9 | 115 ± 8 | 115 ± 8 | 115 ± 7 |
| Diastolic BP (mmHg) | 74 ± 7 | 75 ± 8 | 75 ± 8 | 75 ± 7 | 75 ± 8 |
| Total cholesterol (mg·dL−1) | 201 ± 34 | 200 ± 31 | 201 ± 31 | 202 ± 31 | 203 ± 31 |
| HDL cholesterol (mg·dL−1) | 63 ± 15 | 57 ± 17 * | 57 ± 17 * | 57 ± 17 * | 57 ± 17 * |
| LDL cholesterol (mg·dL−1) | 125 ± 41 | 125 ± 40 | 125 ± 40 | 125 ± 39 | 126 ± 40 |
| Triglycerides (mg·dL−1) | 92 ± 23 | 110 ± 40 | 112 ± 39 | 112 ± 37 * | 112 ± 36 * |
| Blood glucose (mg·dL−1) | 92 ± 7 | 93 ± 7 | 93 ± 7 | 93 ± 7 | 93 ± 7 |
| MetS z-score | −7.0 ± 1.9 | −5.8 ± 2.1 * | −5.9 ± 2.1 * | −5.9 ± 2.1 * | −5.7 ± 2.1 * |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nolan, P.B.; Keeling, S.M.; Robitaille, C.A.; Buchanan, C.A.; Dalleck, L.C. The Effect of Detraining after a Period of Training on Cardiometabolic Health in Previously Sedentary Individuals. Int. J. Environ. Res. Public Health 2018, 15, 2303. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15102303
Nolan PB, Keeling SM, Robitaille CA, Buchanan CA, Dalleck LC. The Effect of Detraining after a Period of Training on Cardiometabolic Health in Previously Sedentary Individuals. International Journal of Environmental Research and Public Health. 2018; 15(10):2303. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15102303
Chicago/Turabian StyleNolan, Paul B., Shawn M. Keeling, Chantelle A. Robitaille, Christina A. Buchanan, and Lance C. Dalleck. 2018. "The Effect of Detraining after a Period of Training on Cardiometabolic Health in Previously Sedentary Individuals" International Journal of Environmental Research and Public Health 15, no. 10: 2303. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15102303