Oral Health-Related Quality of Life in People with Rare Hereditary Connective Tissue Disorders: Marfan Syndrome

Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Participants
2.3. Data Source
2.4. Statistical Analysis
3. Results
3.1. Participants
3.2. Diagnosis Age and Diagnosis Period
3.3. Oral Symptoms
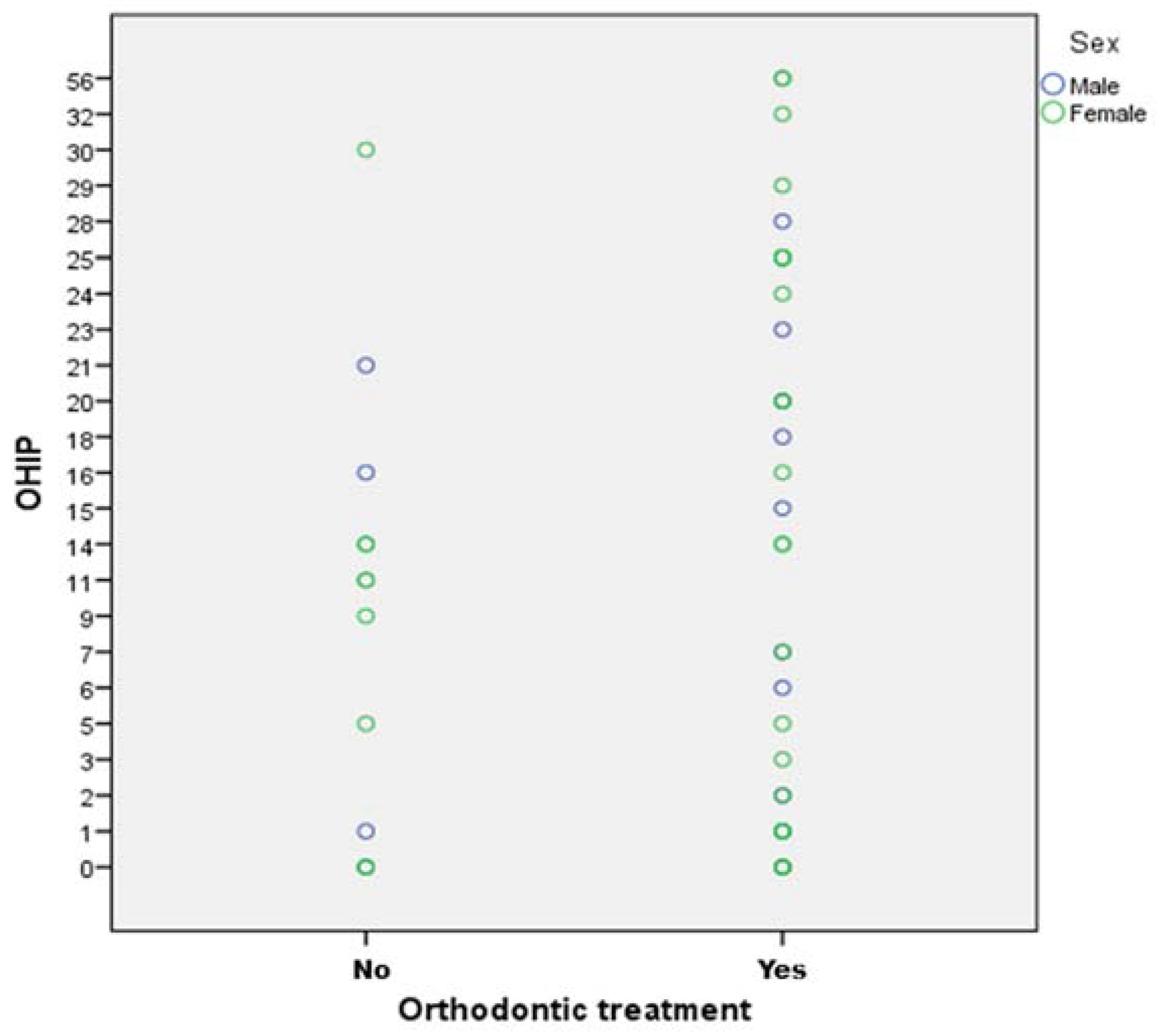
3.4. Orthodontic Treatment
3.5. OHIP Values
3.6. Statistical Analysis
4. Discussion
Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Regulation (EC) No 141/2000 of the European Parliament and of the Council of 16 December 1999 on Orphan Medical Products. Available online: http://ec.europa.eu/health/files/eudralex/vol-1/reg_2000_141_cons-2009-07/reg_2000_141_cons-2009-07_en.pdf (accessed on 9 February 2018).
- Available online: http://www.orpha.net (accessed on 1 May 2018).
- Dietz, H.C.; Cutting, G.R.; Pyeritz, R.E.; Maslen, C.L.; Sakai, L.Y.; Corson, G.M.; Puffenberger, E.G.; Hamosh, A.; Nanthakumar, E.J.; Curristin, S.M. Marfan syndrome caused by a recurrent de novo missense mutation in the fibrillin gene. Nature 1991, 352, 337–339. [Google Scholar] [CrossRef] [PubMed]
- Available online: http://omim.org/entry/154700 (accessed on 2 May 2018).
- Sponseller, P.D.; Hobbs, W.; Riley, L.H., III; Pyeritz, R.E. The thoracolumbar spine in Marfan syndrome. J. Bone Joint Surg. Am. 1995, 77, 867–876. [Google Scholar] [CrossRef] [PubMed]
- De Vries, B.B.A.; Pals, G.; Odink, R.; Hamel, B.C.J. Homozygosity for a FBN1 missense mutation: Clinical and molecular evidence for recessive Marfan syndrome. Eur. J. Hum. Genet. 2007, 15, 930–935. [Google Scholar] [CrossRef] [PubMed]
- Westling, L.; Mohlin, B.; Bresin, A. Craniofacial manifestations in the Marfan syndrome: Palatal dimensions and a comparative cephalometric analysis. J. Craniofac. Genet. Dev. Biol. 1998, 18, 211–218. [Google Scholar] [PubMed]
- Hennekam, R.C.M.; Allanson, J.E.; Krantz, I.D.; Gorlin, R.J. Gorlin’s Syndromes of the Head and Neck, 5th ed.; Oxford University Press: Oxford, UK; New York, NY, USA, 2010. [Google Scholar]
- Mallineni, S.K.; Jayaraman, J.; Yiu, C.K.; King, N.M. Concomitant occurrence of hypohyperdontia in a patient with Marfan syndrome: A review of the literature and report of a case. J. Investig. Clin. Dent. 2012, 3, 253–257. [Google Scholar] [CrossRef] [PubMed]
- Hanisch, M.; Jung, S.; Kleinheinz, J. Oral Health-Related Quality of Life in Rare Diseases with Oral Manifestations. Gesundheitswesen 2018. [Google Scholar] [CrossRef]
- Slade, G.D. Derivation and validation of a short-Form oral health impact profile. Community Dent. Oral Epidemiol. 1997, 25, 284–290. [Google Scholar] [CrossRef] [PubMed]
- John, M.T.; Miglioretti, D.L.; LeResche, L.; Koepsell, T.D.; Hujoel, P.; Micheelis, W. German short forms of the Oral Health Impact Profile. Community Dent. Oral Epidemiol. 2006, 34, 277–288. [Google Scholar] [CrossRef] [PubMed]
- Schmitt-Sausen, N. Tag der Seltenen Erkrankungen: Mehr Aufmerksamkeit für Waisenkinder der Medizin. Dtsch Arztebl 2010, 107, A-430/B-381/C-373. [Google Scholar]
- Available online: https://globalgenes.org/wp-content/uploads/2013/04/ShireReport-1.pdf (accessed on 12 October 2018).
- Roll, K. The influence of regional health care structures on delay in diagnosis of rare diseases: The case of Marfan Syndrome. Health Policy 2012, 105, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Groth, K.A.; Hove, H.; Kyhl, K.; Folkestad, L.; Gaustadnes, M.; Vejlstrup, N.; Stochholm, K.; Østergaard, J.R.; Andersen, N.H.; Gravholt, C.H. Prevalence, incidence, and age at diagnosis in Marfan Syndrome. Orphanet J. Rare Dis. 2015, 10, 153. [Google Scholar] [CrossRef] [PubMed]
- Erkula, G.; Jones, K.B.; Sponseller, P.D.; Dietz, H.C.; Pyeritz, R.E. Growth and maturation in Marfan syndrome. Am. J. Med. Genet. 2002, 109, 100–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mueller, G.C.; Stark, V.; Steiner, K.; von Kodolitsch, Y.; Rybczynski, M.; Weil, J.; Mir, T.S. Impact of age and gender on cardiac pathology in children and adolescents with Marfan syndrome. Pediatr. Cardiol. 2013, 34, 991–998. [Google Scholar] [CrossRef] [PubMed]
- Groth, K.A.; Stochholm, K.; Hove, H.; Kyhl, K.; Gregersen, P.A.; Vejlstrup, N.; Østergaard, J.R.; Gravholt, C.H.; Andersen, N.H. Aortic events in a nationwide Marfan syndrome cohort. Clin. Res. Cardiol. 2017, 106, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Altayó, F.; Siegert, A.M.; Bonorino, F.; Meirelles, T.; Barberà, L.; Dantas, A.P.; Vila, E.; Egea, G. Differences in the Thoracic Aorta by Region and Sex in a Murine Model of Marfan Syndrome. Front Physiol. 2017, 8, 933. [Google Scholar] [CrossRef] [PubMed]
- Staufenbiel, I.; Hauschild, C.; Kahl-Nieke, B.; Vahle-Hinz, E.; von Kodolitsch, Y.; Berner, M.; Bauss, O.; Geurtsen, W.; Rahman, A. Periodontal conditions in patients with Marfan syndrome—A multicenter case control study. BMC Oral Health 2013, 13, 59. [Google Scholar] [CrossRef] [PubMed]
- De Coster, P.J.; Martens, L.C.; De Paepe, A. Oral manifestations of patients with Marfan syndrome: A case-control study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2002, 93, 564–572. [Google Scholar] [CrossRef]
- Hanisch, M.; Fröhlich, L.F.; Kleinheinz, J. Gingival hyperplasia as first sign of recurrence of granulomatosis with polyangiitis (Wegener´s granulomatosis): Case report and review of the literature. BMC Oral Health 2017, 17, 33. [Google Scholar] [CrossRef] [PubMed]
- Bauss, O.; Sadat-Khonsari, R.; Fenske, C.; Engelke, W.; Schwestka-Polly, R. Temporomandibular joint dysfunction in Marfan syndrome. Oral Surg Oral Med Oral Pathol Oral Radiol Endodontol. 2004, 97, 592–598. [Google Scholar] [CrossRef]
- Franken, R.; Heesterbeek, T.J.; de Waard, V.; Zwinderman, A.H.; Pals, G.; Mulder, B.J.M.M. Diagnosis 297 and genetics of Marfan syndrome. Expert Opin. Orphan Drugs 2014. [Google Scholar] [CrossRef]
- John, M.T.; Micheelis, W. Mundgesundheitsbezogene Lebensqualität in der Bevölkerung: Grundlagen und Ergebnisse des OHIP aus einer repräsentativen Stichprobe in Deutschland, IDZ Information 1/2003. Available online: https://www.idz.institute/fileadmin/Content/Publikationen-PDF/IDZ-Info_1_2003-Mundgesundheitsbezogene_Lebensqualitaet_in_der_Bevoelkerung.pdf (accessed on 26 October 2018).
- John, M.T.; Micheelis, W.; Biffar, R. Norrmwerte Mundgesundheitsbezogener Lebensqualität für Kurzversionen des OHIP. Schweiz. Monatsschr. Zahnmed. 2004, 114, 784–791. [Google Scholar] [PubMed]


{kind=link}
| Mean ± SD | Median | Interquartile Range | 95% CI | |||
|---|---|---|---|---|---|---|
| Inferior | Superior | |||||
| Age during diagnosis | M | 7.28 ± 7.06 | 5.00 | 14 | 0.75 | 13.81 |
| F | 20.92 ± 11.61 | 23.00 | 19 | 16.33 | 25.51 | |
| Time between diagnosis and first symptom | M | 4.14 ± 5.52 | 2.00 | 8 | −0.96 | 9.25 |
| F | 14.05 ± 11.96 | 14.00 | 24 | 9.31 | 18.78 | |
| OHIP values | M | 10.57 ± 11.50 | 6.00 | 22 | −0.07 | 21.21 |
| F | 15.89 ± 15.83 | 14.00 | 24 | 9.62 | 22.15 | |
| Sex | Oral Manifestations |
|---|---|
| Dysgnathia | |
| Yes | |
| M | 11 |
| F | 23 |
| Total | 34 |
| High arched Palate | |
| Yes | |
| M | 1 |
| F | 13 |
| Total | 14 |
| Malocclusion | |
| Yes | |
| M | 5 |
| F | 16 |
| Total | 21 |
| Crowding | |
| Yes | |
| M | 3 |
| F | 11 |
| Total | 14 |
| Mineralisation disorder of the teeth | |
| Yes | |
| M | 2 |
| F | 2 |
| Total | 4 |
| Microdontia | |
| Yes | |
| M | 0 |
| F | 3 |
| Total | 3 |
| Hypodontia | |
| Yes | |
| M | 2 |
| F | 4 |
| Total | 6 |
| Temporomandibular disorder | |
| Yes | |
| M | 0 |
| F | 6 |
| Total | 6 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hanisch, M.; Wiemann, S.; Jung, S.; Kleinheinz, J.; Bohner, L. Oral Health-Related Quality of Life in People with Rare Hereditary Connective Tissue Disorders: Marfan Syndrome. Int. J. Environ. Res. Public Health 2018, 15, 2382. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15112382
Hanisch M, Wiemann S, Jung S, Kleinheinz J, Bohner L. Oral Health-Related Quality of Life in People with Rare Hereditary Connective Tissue Disorders: Marfan Syndrome. International Journal of Environmental Research and Public Health. 2018; 15(11):2382. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15112382
Chicago/Turabian StyleHanisch, Marcel, Sabrina Wiemann, Susanne Jung, Johannes Kleinheinz, and Lauren Bohner. 2018. "Oral Health-Related Quality of Life in People with Rare Hereditary Connective Tissue Disorders: Marfan Syndrome" International Journal of Environmental Research and Public Health 15, no. 11: 2382. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15112382