Food Allergy Prevalence in Salvadoran Schoolchildren Estimated by Parent-Report

 ,
,  , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population Survery
2.2. Questionnaire
2.3. Definitions
2.4. Statistical Analyses
3. Results
3.1. Participants and Demographic Characteristics
3.2. Parent-Reported Prevalence Rates of Adverse Food Reactions and FA
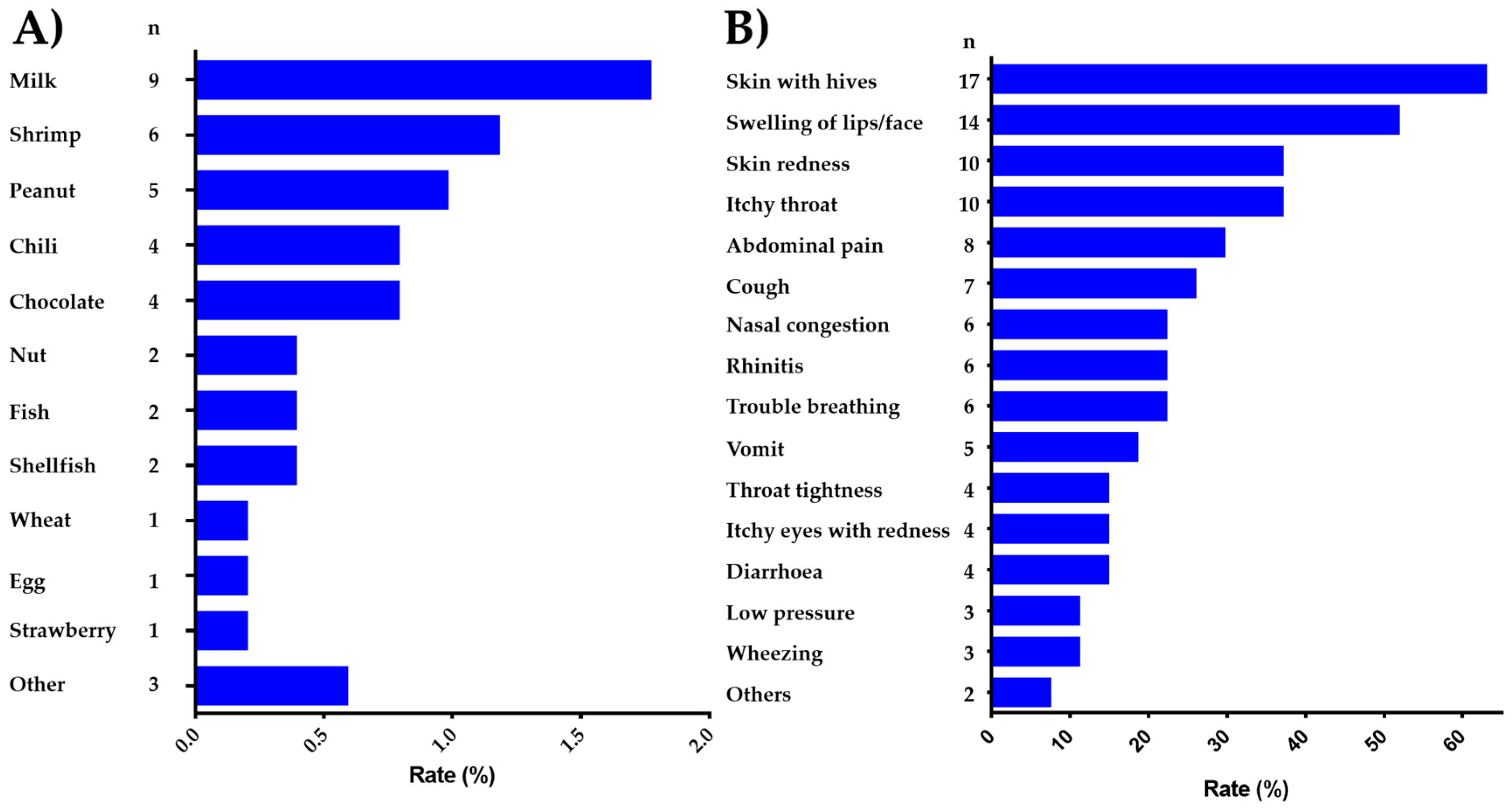
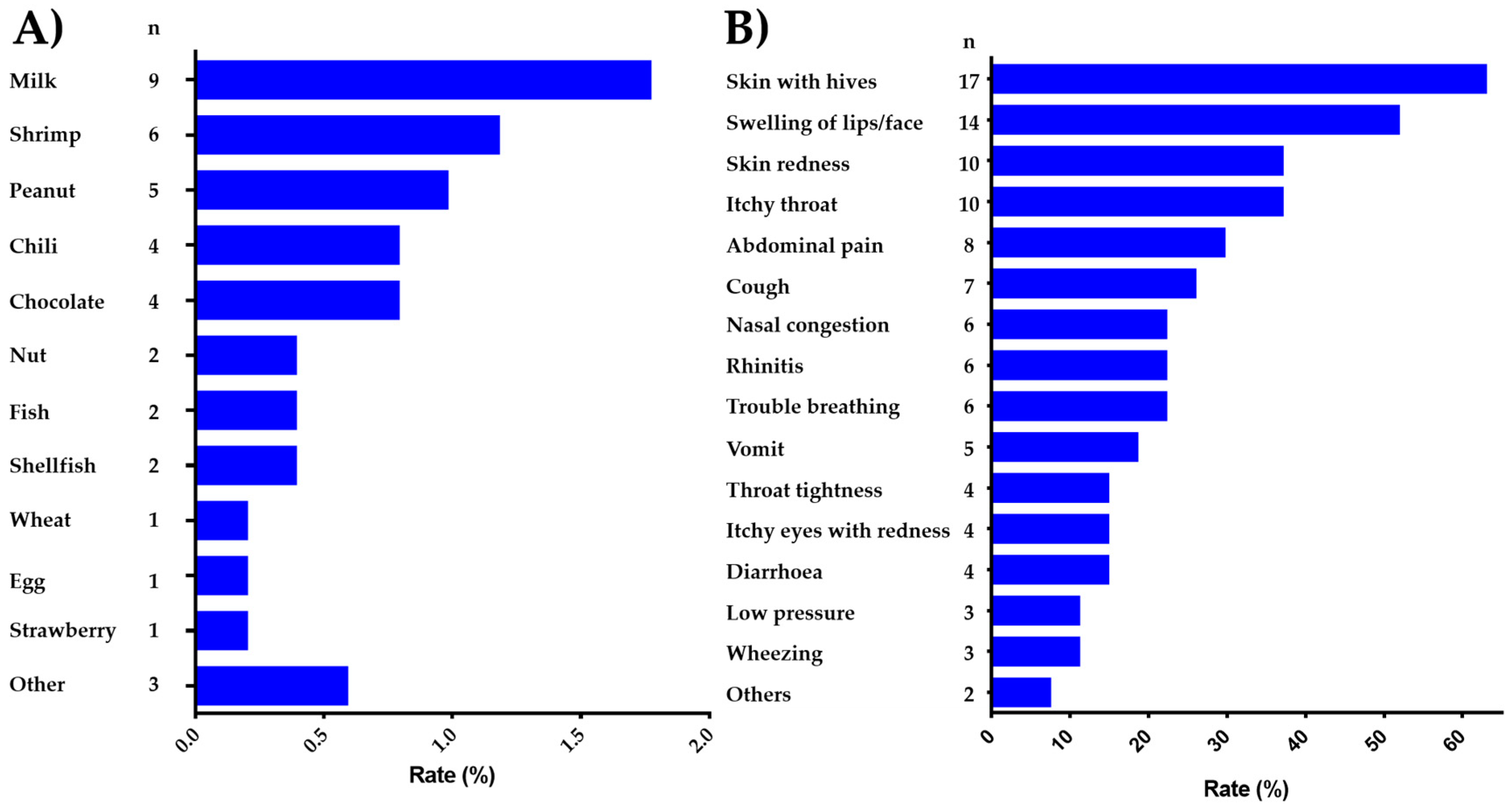
3.3. Foods Implicated in Adverse Food Reactions
3.4. Common Food Allergens and Clinical Characteristics of FA
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hoyos-Bachiloglu, R.; Ivanovic-Zuvic, D.; Alvarez, J.; Linn, K.; Thöne, N.; de Los Ángeles Paul, M.; Borzutzky, A. Prevalence of parent-reported immediate hypersensitivity food allergy in chilean school-aged children. Allergol. Immunopathol. 2014, 42, 527–532. [Google Scholar] [CrossRef] [PubMed]
- Ontiveros, N.; Valdez-Meza, E.; Vergara-Jiménez, M.; Canizalez-Román, A.; Borzutzky, A.; Cabrera-Chávez, F. Parent-reported prevalence of food allergy in mexican schoolchildren: A population-based study. Allergol. Immunopathol. 2016, 44, 563–570. [Google Scholar] [CrossRef] [PubMed]
- DunnGalvin, A.; Dubois, A.; Flokstra-de Blok, B.; Hourihane, J.O.B. The effects of food allergy on quality of life. In Food Allergy: Molecular Basis and Clinical Practice; Karger Publishers: Basel, Switzerland, 2015; Volume 101, pp. 235–252. [Google Scholar]
- Gupta, R.; Holdford, D.; Bilaver, L.; Dyer, A.; Holl, J.L.; Meltzer, D. The economic impact of childhood food allergy in the united states. JAMA Pediatr. 2013, 167, 1026–1031. [Google Scholar] [CrossRef] [PubMed]
- Stensgaard, A.; Bindslev-Jensen, C.; Nielsen, D.; Munch, M.; DunnGalvin, A. Quality of life in childhood, adolescence and adult food allergy: Patient and parent perspectives. Clin. Exp. Allergy 2017, 47, 530–539. [Google Scholar] [CrossRef] [PubMed]
- Hefle, S.L.; Furlong, T.J.; Niemann, L.; Lemon-Mule, H.; Sicherer, S.; Taylor, S.L. Consumer attitudes and risks associated with packaged foods having advisory labeling regarding the presence of peanuts. J. Allergy Clin. Immunol. 2007, 120, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Prescott, S.L.; Pawankar, R.; Allen, K.J.; Campbell, D.E.; Sinn, J.K.; Fiocchi, A.; Ebisawa, M.; Sampson, H.A.; Beyer, K.; Lee, B.-W. A global survey of changing patterns of food allergy burden in children. World Allergy Organ. J. 2013, 6, 1. [Google Scholar] [CrossRef] [PubMed]
- Ontiveros, N.; Flores-Mendoza, L.; Canizalez-Román, V.; Cabrera-Chavez, F. Food allergy: Prevalence and food technology approaches for the control of IgE-mediated food allergy. Austin J. Nutr. Food Sci. 2014, 2. Available online: http://www.austinpublishinggroup.com/nutrition-food-sciences/fulltext/ajnfs-v2-id1029.php (accessed on 1 October 2018).
- Rona, R.J.; Keil, T.; Summers, C.; Gislason, D.; Zuidmeer, L.; Sodergren, E.; Sigurdardottir, S.T.; Lindner, T.; Goldhahn, K.; Dahlstrom, J. The prevalence of food allergy: A meta-analysis. J. Allergy Clin. Immunol. 2007, 120, 638–646. [Google Scholar] [CrossRef] [PubMed]
- McBride, D.; Keil, T.; Grabenhenrich, L.; Dubakiene, R.; Drasutiene, G.; Fiocchi, A.; Dahdah, L.; Sprikkelman, A.; Schoemaker, A.; Roberts, G. The europrevall birth cohort study on food allergy: Baseline characteristics of 12,000 newborns and their families from nine european countries. Pediatr. Allergy Immunol. 2012, 23, 230–239. [Google Scholar] [CrossRef] [PubMed]
- McGowan, E.C.; Matsui, E.; McCormack, M.C.; Pollack, C.E.; Roger, P.; Keet, C.A. The effect of poverty, urbanization, and race/ethnicity on perceived food allergy in the united states. Ann. Allergy Asthma Immunol. 2015, 115, 85. [Google Scholar] [CrossRef] [PubMed]
- Soller, L.; Ben-Shoshan, M.; Harrington, D.W.; Knoll, M.; Fragapane, J.; Joseph, L.; Pierre, Y.S.; La Vieille, S.; Wilson, K.; Elliott, S.J. Prevalence and predictors of food allergy in Canada: A focus on vulnerable populations. J. Allergy Clin. Immunol. 2015, 3, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Marrugo, J.; Hernández, L.; Villalba, V. Prevalence of self-reported food allergy in Cartagena (Colombia) population. Allergol. Immunopathol. 2008, 36, 320–324. [Google Scholar] [CrossRef]
- Guimarães, T.; Gonçalves, L.; Silva, R.; da Silva Segundo, G.R. Prevalence of parent-reported food allergy in infants and preschoolers in brazil. Allergol. Immunopathol. 2015, 43, 424–425. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.I.; Shin, M.H.; Lee, H.B.; Lee, J.S.; Son, B.K.; Koh, Y.Y.; Kim, K.E.; Ahn, Y.O. Prevalences of symptoms of asthma and other allergic diseases in Korean children: A nationwide questionnaire survey. J. Korean Med. Sci. 2001, 16, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Leung, T.F.; Yung, E.; Wong, Y.S.; Lam, C.W.; Wong, G.W. Parent-reported adverse food reactions in Hong Kong Chinese pre-schoolers: Epidemiology, clinical spectrum and risk factors. Pediatr. Allergy Immunol. 2009, 20, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, L.; Guimarães, T.; Silva, R.; Cheik, M.; de Ramos Nápolis, A.; e Silva, G.B.; Segundo, G. Prevalence of food allergy in infants and pre-schoolers in brazil. Allergol. Immunopathol. 2016, 44, 497–503. [Google Scholar] [CrossRef] [PubMed]
- Woods, R.; Abramson, M.; Bailey, M.; Walters, E. International prevalences of reported food allergies and intolerances. Comparisons arising from the European Community Respiratory Health Survey (ECRHS) 1991–1994. Eur. J. Clin. Nutr. 2001, 55, 298. [Google Scholar] [CrossRef] [PubMed]
- Sicherer, S.H. Epidemiology of food allergy. J. Allergy Clin. Immunol. 2011, 127, 594–602. [Google Scholar] [CrossRef] [PubMed]
- Tosca, M.; Pistorio, A.; Accogli, A.; Rossi, G.A.; Ciprandi, G. Food anaphylaxis in children: Peculiarity of characteristics. Allergol. Immunopathol. 2015, 43, 421–423. [Google Scholar] [CrossRef] [PubMed]
- Panesar, S.; Javad, S.; De Silva, D.; Nwaru, B.; Hickstein, L.; Muraro, A.; Roberts, G.; Worm, M.; Bilò, M.; Cardona, V. The epidemiology of anaphylaxis in Europe: A systematic review. Allergy 2013, 68, 1353–1361. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.C.; Tsai, T.C.; Huang, C.F.; Chang, F.Y.; Lin, C.C.; Huang, I.F.; Chu, C.H.; Lau, B.H.; Wu, L.; Peng, H.J. Prevalence of food allergy in Taiwan: A questionnaire-based survey. Intern. Med. J. 2012, 42, 1310–1315. [Google Scholar] [CrossRef] [PubMed]
- Ibranji, A.; Nikolla, E.; Loloci, G.; Mingomataj, E. A case report on transitory histamine intolerance from strawberry intake in a 15 month old child with acute gastroenteritis. Clin. Transl. Allergy 2015, 5, P61. [Google Scholar] [CrossRef]
- Kovacova-Hanuskova, E.; Buday, T.; Gavliakova, S.; Plevkova, J. Histamine, histamine intoxication and intolerance. Allergol. Immunopathol. 2015, 43, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Simons, F.E.R.; Ardusso, L.R.; Bilò, M.B.; El-Gamal, Y.M.; Ledford, D.K.; Ring, J.; Sanchez-Borges, M.; Senna, G.E.; Sheikh, A.; Thong, B.Y. World allergy organization guidelines for the assessment and management of anaphylaxis. World Allergy Organ. J. 2011, 4, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardona, V.; Álvarez-Perea, A.; Ansotegui, I.J.; Arias-Cruz, A.; González-Díaz, S.N.; Latour-Staffeld, P.; Ivancevich, J.C.; Sánchez-Borges, M.; Serrano, C.; Solé, D. Management of anaphylaxis in Latin America: Current situation. Rev. Alerg. Mex. 2017, 64, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Sicherer, S.H.; Burks, A.W.; Sampson, H.A. Clinical features of acute allergic reactions to peanut and tree nuts in children. Pediatrics 1998, 102, e6. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Condition | Criteria |
|---|---|
| Perceived FA, ever | The parents stated that their child has had allergic reactions to food. |
| Adverse food reaction | Any symptomatic recurrent adverse reaction to a specific food potentially mediated or not by immune mechanisms. |
| Immediate-type FA, ever | Having symptomatic recurrent adverse food reactions that were convincing of immediate-type hypersensitivity allergic reactions. |
| Immediate-type FA, current | Those cases that met criteria for “immediate-type FA, ever”, but answered negatively to the question “is your child now able to eat the suspected food(s) without any reactions”. |
| Food-dependent anaphylaxis | Those cases that met criteria for “immediate-type FA, current” and according to the three following criteria: (1) Acute onset of an illness with involvement of the skin, mucosal tissue or both and respiratory compromise or reduced blood pressure. (2) Two or more of the following that occur rapidly after food ingestion: (a) involvement of the skin-mucosal tissue, (b) respiratory compromise, (c) reduced blood pressure, (d) persistent gastrointestinal symptoms. (3) Reduced blood pressure after exposure to a food allergen. |
| Parent-reported physician-diagnosed (PR-PD) FA, ever | Those cases that answered positively to the question, “Has a doctor ever told you that your child has FA?”. |
| Variable | |
|---|---|
| Mean age in years (range) | 9.2 (4–12) |
| Gender | n (%) |
| Female | 248 (48.81) |
| Male | 260 (51.18) |
| Known allergic diseases other than FA | |
| Allergic rhinitis | 64 (12.59) |
| Atopic dermatitis | 34 (6.69) |
| Insect sting allergy | 84 (16.53) |
| Asthma | 43 (8.46) |
| Urticaria | 22 (4.33) |
| Drug allergy | 37 (7.28) |
| Conjunctivitis | 34 (6.69) |
| Anaphylaxis | 1 (0.19) |
| Animals allergy | 36 (7.08) |
| Assessment | Number of Reported Cases | Prevalence % (95% CI) | p | ||
|---|---|---|---|---|---|
| 4–8 Years, n = 174 | 9–12 Years, n = 334 | Total, n = 508 | |||
| Adverse food reactions | 81 | 13.21 (8.97–19.05) | 17.36 (13.68–21.79) | 15.94 (13.02–19.38) | 0.252 |
| Perceived FA, ever | 59 | 8.62 (5.29–13.73) | 13.17 (9.96–17.22) | 11.61 (9.11–14.69) | 0.146 |
| Physician-diagnosed FA, ever | 31 | 7.47(4.41–12.36) | 5.38 (3.43–8.35) | 6.10 (4.33–8.5) | 0.435 |
| Immediate-type FA, ever | 45 | 5.74 (3.15–10.25) | 10.47 (7.63–14.22) | 8.85 (6.68–11.65) | 0.841 |
| Immediate-type FA, current | 27 | 3.44 (1.59–7.31) | 6.28 (4.14–9.42) | 5.31 (3.67–7.62) | 0.214 |
| Food-induced anaphylaxis | 13 | 1.14 (0.31–4.09) | 3.29 (1.84–5.8) | 2.55 (1.50–4.32) | 0.235 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cabrera-Chávez, F.; Rodríguez-Bellegarrigue, C.I.; Figueroa-Salcido, O.G.; Lopez-Gallardo, J.A.; Arámburo-Gálvez, J.G.; Vergara-Jiménez, M.d.J.; Castro-Acosta, M.L.; Sotelo-Cruz, N.; Gracia-Valenzuela, M.H.; Ontiveros, N. Food Allergy Prevalence in Salvadoran Schoolchildren Estimated by Parent-Report. Int. J. Environ. Res. Public Health 2018, 15, 2446. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15112446
Cabrera-Chávez F, Rodríguez-Bellegarrigue CI, Figueroa-Salcido OG, Lopez-Gallardo JA, Arámburo-Gálvez JG, Vergara-Jiménez MdJ, Castro-Acosta ML, Sotelo-Cruz N, Gracia-Valenzuela MH, Ontiveros N. Food Allergy Prevalence in Salvadoran Schoolchildren Estimated by Parent-Report. International Journal of Environmental Research and Public Health. 2018; 15(11):2446. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15112446
Chicago/Turabian StyleCabrera-Chávez, Francisco, Cecilia Ivonne Rodríguez-Bellegarrigue, Oscar Gerardo Figueroa-Salcido, Jesús Aristeo Lopez-Gallardo, Jesús Gilberto Arámburo-Gálvez, Marcela de Jesús Vergara-Jiménez, Mónica Lizzette Castro-Acosta, Norberto Sotelo-Cruz, Martina Hilda Gracia-Valenzuela, and Noé Ontiveros. 2018. "Food Allergy Prevalence in Salvadoran Schoolchildren Estimated by Parent-Report" International Journal of Environmental Research and Public Health 15, no. 11: 2446. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15112446