Quantitative Ultrasound Imaging Pixel Analysis of the Intrinsic Plantar Muscle Tissue between Hemiparesis and Contralateral Feet in Post-Stroke Patients

 ,
, 
 ,
,  ,
, 
Abstract
:1. Introduction
2. Material and Methods
2.1. Design
2.2. Sample Size Calculation
2.3. Participants
2.4. Ethical Approval
2.5. Descriptive Data
2.6. B-Mode Ultrasound Imaging
2.7. Image J Software Analysis
2.8. Statistical Analysis
3. Results
3.1. Demographic and Descriptive Data
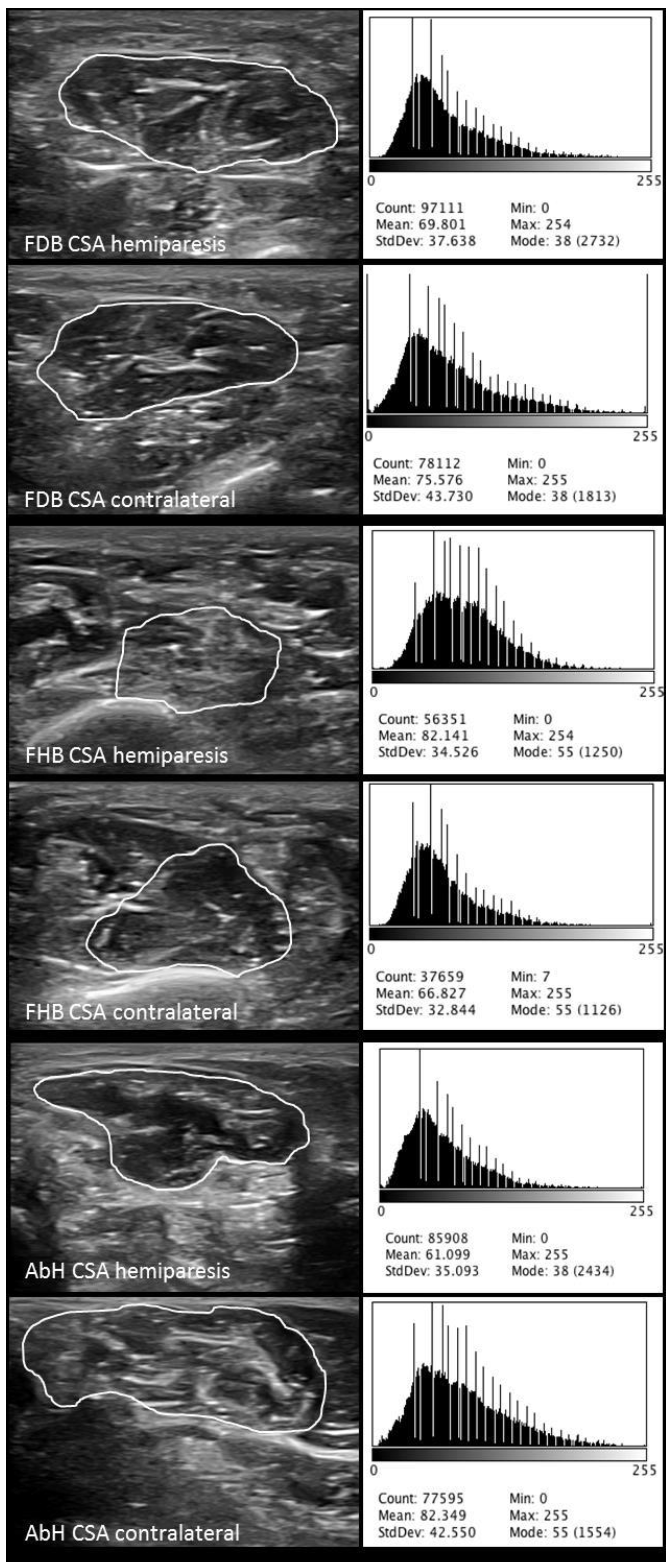
3.2. B-Mode Ultrasonography and Image J Analysis of Intrinsic Plantar Muscles
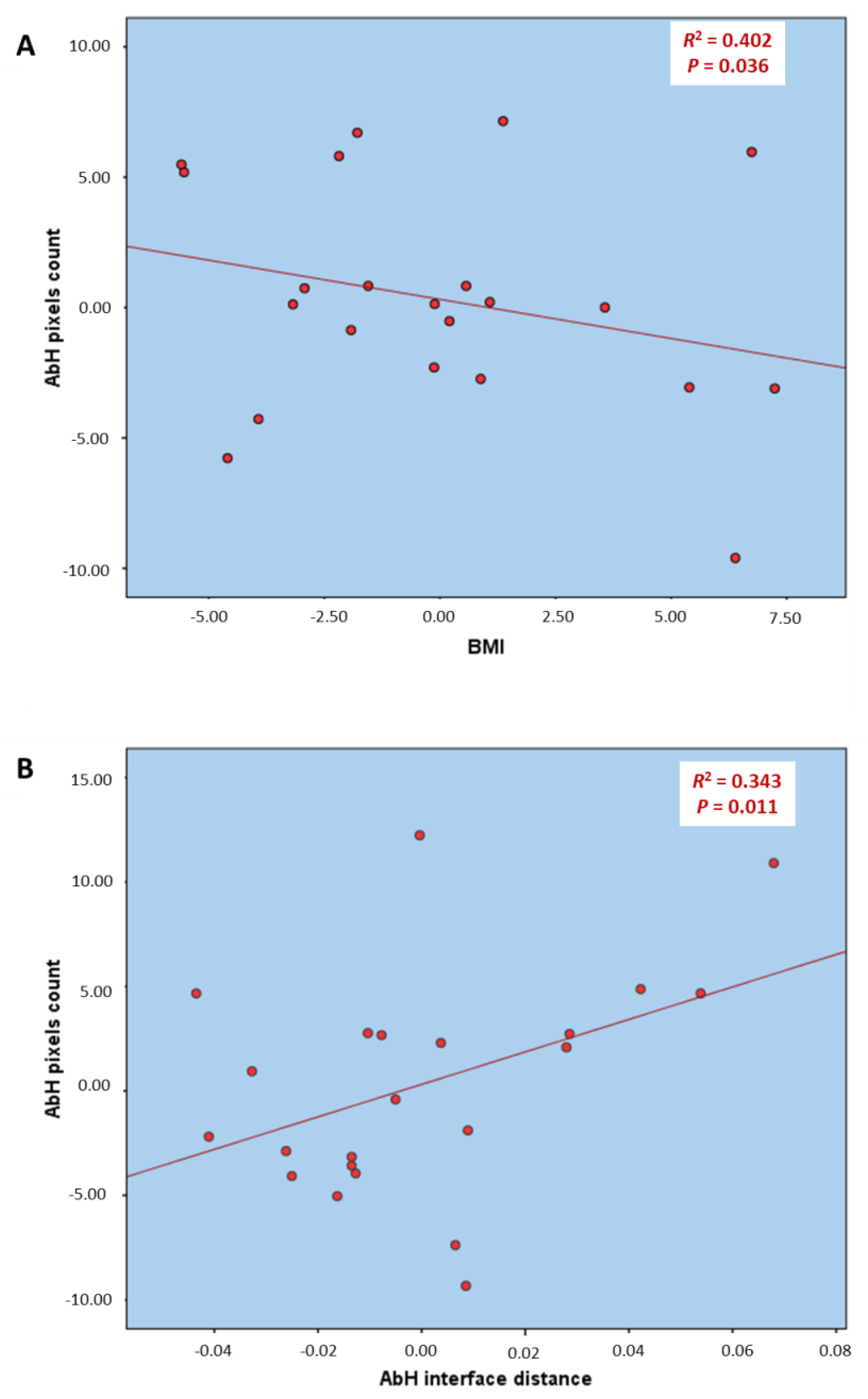
3.3. Multivariate Predictive Analysis of AbH Pixels Count
4. Discussion
4.1. Future Studies or Clinical Implications
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Zhang, Y.; Chapman, A.-M.; Plested, M.; Jackson, D.; Purroy, F. The Incidence, Prevalence, and Mortality of Stroke in France, Germany, Italy, Spain, the UK, and the US: A Literature Review. Stroke Res. Treat. 2012. [Google Scholar] [CrossRef] [PubMed]
- Vega, T.; Zurriaga, O.; Ramos, J.M.; Gil, M.; Alamo, R.; Lozano, J.E.; López, A.; Miralles, M.T.; Vaca, P.; Alvarez Mdel, M.; et al. Stroke in Spain: Epidemiologic incidence and patterns; a health sentinel network study. J. Stroke Cerebrovasc. Dis. 2009, 18, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Mar, J.; Masjuan, J.; Oliva-Moreno, J.; Gonzalez-Rojas, N.; Becerra, V.; Casado, M.Á.; Torres, C.; Yebenes, M.; Quintana, M.; Alvarez-Sabín, J.; et al. Outcomes measured by mortality rates, quality of life and degree of autonomy in the first year in stroke units in Spain. Health Qual. Life Outcomes 2015. [Google Scholar] [CrossRef] [PubMed]
- Di Carlo, A. Human and economic burden of stroke. Age Ageing 2009, 38, 4–5. [Google Scholar] [CrossRef] [PubMed]
- Santamato, A.; Francesca Micello, M.; Panza, F.; Fortunato, F.; Logroscino, G.; Picelli, A.; Manganotti, P.; Smania, N.; Fiore, P.; Ranieri, M. Extracorporeal Shock Wave Therapy for the Treatment of Poststroke Plantar-Flexor Muscles Spasticity: A Prospective Open-Label Study. Top. Stroke Rehabil. 2014, 21, S17–S24. [Google Scholar] [CrossRef] [PubMed]
- Cho, K.H.; Lee, H.J.; Lee, W.H. Reliability of rehabilitative ultrasound imaging for the medial gastrocnemius muscle in poststroke patients. Clin. Physiol. Funct. Imaging 2014, 34, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Gao, F.; Ren, Y.; Roth, E.J.; Harvey, R.; Zhang, L.-Q. Effects of repeated ankle stretching on calf muscle-tendon and ankle biomechanical properties in stroke survivors. Clin. Biomech. 2011, 26, 516–522. [Google Scholar] [CrossRef] [PubMed]
- Crofts, G.; Angin, S.; Mickle, K.J.; Hill, S.; Nester, C.J. Reliability of ultrasound for measurement of selected foot structures. Gait Posture 2014, 39, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Angin, S.; Crofts, G.; Mickle, K.J.; Nester, C.J. Ultrasound evaluation of foot muscles and plantar fascia in pes planus. Gait Posture 2014, 40, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Lobo, C.C.; Marín, A.G.; Sanz, D.R.; López, D.L.; López, P.P.; Morales, C.R.; Corbalán, I.S. Ultrasound evaluation of intrinsic plantar muscles and fascia in hallux valgus: A. case-control study. Medicine 2016, 95, e5243. [Google Scholar] [CrossRef] [PubMed]
- Calvo-Lobo, C.; Useros-Olmo, A.I.; Almazán-Polo, J.; Becerro-de-Bengoa-Vallejo, R.; Losa-Iglesias, M.E.; Palomo-López, P.; Rodríguez-Sanz, D.; López-López, D. Rehabilitative ultrasound imaging of the bilateral intrinsic plantar muscles and fascia in post-stroke survivors with hemiparesis: A. case-control study. Int. J. Med. Sci. 2018, 15, 907–914. [Google Scholar] [CrossRef] [PubMed]
- Coppieters, M.W.; Hough, A.D.; Dilley, A. Different nerve-gliding exercises induce different magnitudes of median nerve longitudinal excursion: An in vivo study using dynamic ultrasound imaging. J. Orthop. Sport. Phys. Ther. 2009, 39, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Ellis, R.; Osborne, S.; Whitfield, J.; Parmar, P.; Hing, W. The effect of spinal position on sciatic nerve excursion during seated neural mobilisation exercises: An in vivo study using ultrasound imaging. J. Man. Manip. Ther. 2017, 25, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; He, W.; Du, L.-J.; Chen, J.; Park, D.; Wells, M.; Fowlkes, B.; O’Dell, M. Quantitative Ultrasound Imaging to Assess the Biceps Brachii Muscle in Chronic Post-Stroke Spasticity: Preliminary Observation. Ultrasound Med. Biol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Koppaka, S.; Shklyar, I.; Rutkove, S.B.; Darras, B.T.; Anthony, B.W.; Zaidman, C.M.; Wu, J.S. Quantitative Ultrasound Assessment of Duchenne Muscular Dystrophy Using Edge Detection Analysis. J. Ultrasound Med. 2016, 35, 1889–1897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, C.A.; Rasband, W.S.; Eliceiri, K.W. NIH Image to Image J: 25 years of image analysis. Nat. Methods 2012, 9, 671–675. [Google Scholar] [CrossRef] [PubMed]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; STROBE Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Int. J. Surg. 2014, 12, 1500–1524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cartwright, M.S.; Walker, F.O. Neuromuscular ultrasound in common entrapment neuropathies. Muscle Nerve 2013, 48, 696–704. [Google Scholar] [CrossRef] [PubMed]
- Holt, G.R. Declaration of Helsinki—The World’s Document of Conscience and Responsibility. South. Med. J. 2014, 107, 407. [Google Scholar] [CrossRef] [PubMed]
- Nayar, M.; Vanderstay, R.; Siegert, R.J.; Turner-Stokes, L. The UK Functional Assessment Measure (UK FIM+FAM): Psychometric Evaluation in Patients Undergoing Specialist Rehabilitation following a Stroke from the National UK Clinical Dataset. PLoS ONE 2016, 11, e0147288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, K.M.; Hamilton, B.B.; Gordon, W.A.; Zasler, N.D. Characteristics and comparisons of functional assessment indices. J. Head. Trauma Rehabil. 1993, 8, 60–74. [Google Scholar] [CrossRef]
- Huertas Hoyas, E.; Pedrero Pérez, E.J.; Águila Maturana, A.M.; García López-Alberca, S.; González Alted, C. Predictores de funcionalidad en el daño cerebral adquirido. Neurología 2015, 30, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Martín, P.; Fernández-Mayoralas, G.; Frades-Payo, B.; Rojo-Pérez, F.; Petidier, R.; Rodríguez-Rodríguez, V.; Forjaz, M.J.; Prieto-Flores, M.E.; de Pedro Cuesta, J. Validation of the functional independence scale. Gac. Sanit. 2009, 23, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Mishra, C.; Ganesh, G.S. Inter-Rater Reliability of Modified Modified Ashworth Scale in the Assessment of Plantar Flexor Muscle Spasticity in Patients with Spinal Cord Injury. Physiother. Res. Int. 2014, 19, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Hua, Y.; Feng, W.; Ovbiagele, B. Multimodality ultrasound imaging in stroke: Current concepts and future focus. Expert. Rev. Cardiovasc. Ther. 2016, 14, 1325–1333. [Google Scholar] [CrossRef] [PubMed]
- Rutkove, S.B.; Geisbush, T.R.; Mijailovic, A.; Shklyar, I.; Pasternak, A.; Visyak, N.; Wu, J.S.; Zaidman, C.; Darras, B.T. Cross-sectional Evaluation of Electrical Impedance Myography and Quantitative Ultrasound for the Assessment of Duchenne Muscular Dystrophy in a Clinical Trial Setting. Pediatr. Neurol. 2014, 51, 88–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez-Payá, J.J.; Ríos-Díaz, J.; Medina-Mirapeix, F.; Vázquez-Costa, J.F.; del Baño-Aledo, M.E. Monitoring Progression of Amyotrophic Lateral Sclerosis Using Ultrasound Morpho-Textural Muscle Biomarkers: A Pilot Study. Ultrasound Med. Biol. 2018, 44, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Payá, J.J.; Ríos-Díaz, J.; del Baño-Aledo, M.E.; Tembl-Ferrairó, J.I.; Vazquez-Costa, J.F.; Medina-Mirapeix, F. Quantitative Muscle Ultrasonography Using Textural Analysis in Amyotrophic Lateral Sclerosis. Ultrason. Imaging 2017, 39, 357–368. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Payá, J.J.; del Baño-Aledo, M.E.; Ríos-Díaz, J.; Tembl-Ferrairó, J.I.; Vázquez-Costa, J.F.; Medina-Mirapeix, F. Muscular Echovariation: A New Biomarker in Amyotrophic Lateral Sclerosis. Ultrasound Med. Biol. 2017, 43, 1153–1162. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameter | Hemiparesis Feet Mean ± SD (n = 11) | Contralateral Feet Mean ± SD (n = 11) | p-Value * |
|---|---|---|---|
| Interface (cm) | |||
| FDB | 0.40 ± 0.06 (0.30–0.50) | 0.39 ± 0.05 (0.32–0.49) | 0.672 |
| FHB | 0.55 ± 0.07 (0.43–0.67) | 0.52 ± 0.10 (0.35–0.66) | 0.463 |
| AbH | 0.15 ± 0.03 (0.11–0.21) | 0.15 ± 0.03 (0.11–0.23) | 1.000 |
| CSA (cm2) | |||
| FDB | 2.31 ± 0.58 (1.39–3.37) | 2.57 ± 0.68 (1.34–3.43) | 0.341 |
| FHB | 2.08 ± 0.46 (1.11–3.86) | 1.97 ± 0.45 (1.31–2.52) | 0.611 |
| AbH | 2.38 ± 0.56 (1.39–3.53) | 2.78 ± 0.74 (1.84–4.42) | 0.167 |
| Pixel count | |||
| FDB | 65,249.90 ± 18,089.52 (46,028.00–95,940.00) | 83,075.51 ± 23,339.07 (39,728.00–13,8092.67) | 0.102 |
| FHB | 62,931.63 ± 11,849.62 (48,161.33–83,519.33) | 71,732.91 ± 19,720.70 (37,901.00–10,3927.00) | 0.219 |
| AbH | 66,572.48 ± 12,770.22 (47,111.00–85,467.67) | 87,513.18 ± 15,644.87 (57,851.33–11,4668.00) | 0.003 |
| Pixel mean | |||
| FDB | 86.35 ± 10.59 (69.53–103.20) | 75.57 ± 17.10 (47.72–111.09) | 0.091 |
| FHB | 88.19 ± 9.30 (71.39–99.70) | 76.86 ± 15.62 (58.04–100.14) | 0.055 |
| AbH | 75.87 ± 12.81 (60.70–104.81) | 67.13 ± 11.15 (60.70–104.81) | 0.107 |
| Pixel SD | |||
| FDB | 41.08 ± 5.90 (34.91–52.23) | 38.57 ± 5.98 (29.69–49.77) | 0.334 |
| FHB | 33.04 ± 3.14 (28.81–36.50) | 31.83 ± 5.79 (22.68–45.91) | 0.552 |
| AbH | 37.42 ± 0.25 (27.46–44.35) | 38.05 ± 4.77 (31.39–47.06) | 0.760 |
| Parameter | Model | R2 Change † | Model R2 |
|---|---|---|---|
| AbH pixels count | 43.057 | ||
| −0.935 * BMI | 0.402 | 0.745 | |
| +86.432 * AbH interface distance | 0.343 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calvo-Lobo, C.; Useros-Olmo, A.I.; Almazán-Polo, J.; Martín-Sevilla, M.; Romero-Morales, C.; Sanz-Corbalán, I.; Rodríguez-Sanz, D.; López-López, D. Quantitative Ultrasound Imaging Pixel Analysis of the Intrinsic Plantar Muscle Tissue between Hemiparesis and Contralateral Feet in Post-Stroke Patients. Int. J. Environ. Res. Public Health 2018, 15, 2519. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15112519
Calvo-Lobo C, Useros-Olmo AI, Almazán-Polo J, Martín-Sevilla M, Romero-Morales C, Sanz-Corbalán I, Rodríguez-Sanz D, López-López D. Quantitative Ultrasound Imaging Pixel Analysis of the Intrinsic Plantar Muscle Tissue between Hemiparesis and Contralateral Feet in Post-Stroke Patients. International Journal of Environmental Research and Public Health. 2018; 15(11):2519. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15112519
Chicago/Turabian StyleCalvo-Lobo, Cesar, Ana Isabel Useros-Olmo, Jaime Almazán-Polo, Miriam Martín-Sevilla, Carlos Romero-Morales, Irene Sanz-Corbalán, David Rodríguez-Sanz, and Daniel López-López. 2018. "Quantitative Ultrasound Imaging Pixel Analysis of the Intrinsic Plantar Muscle Tissue between Hemiparesis and Contralateral Feet in Post-Stroke Patients" International Journal of Environmental Research and Public Health 15, no. 11: 2519. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15112519