Increased Risk of Ulcerative Colitis in Patients with Periodontal Disease: A Nationwide Population-Based Cohort Study

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source and Collection
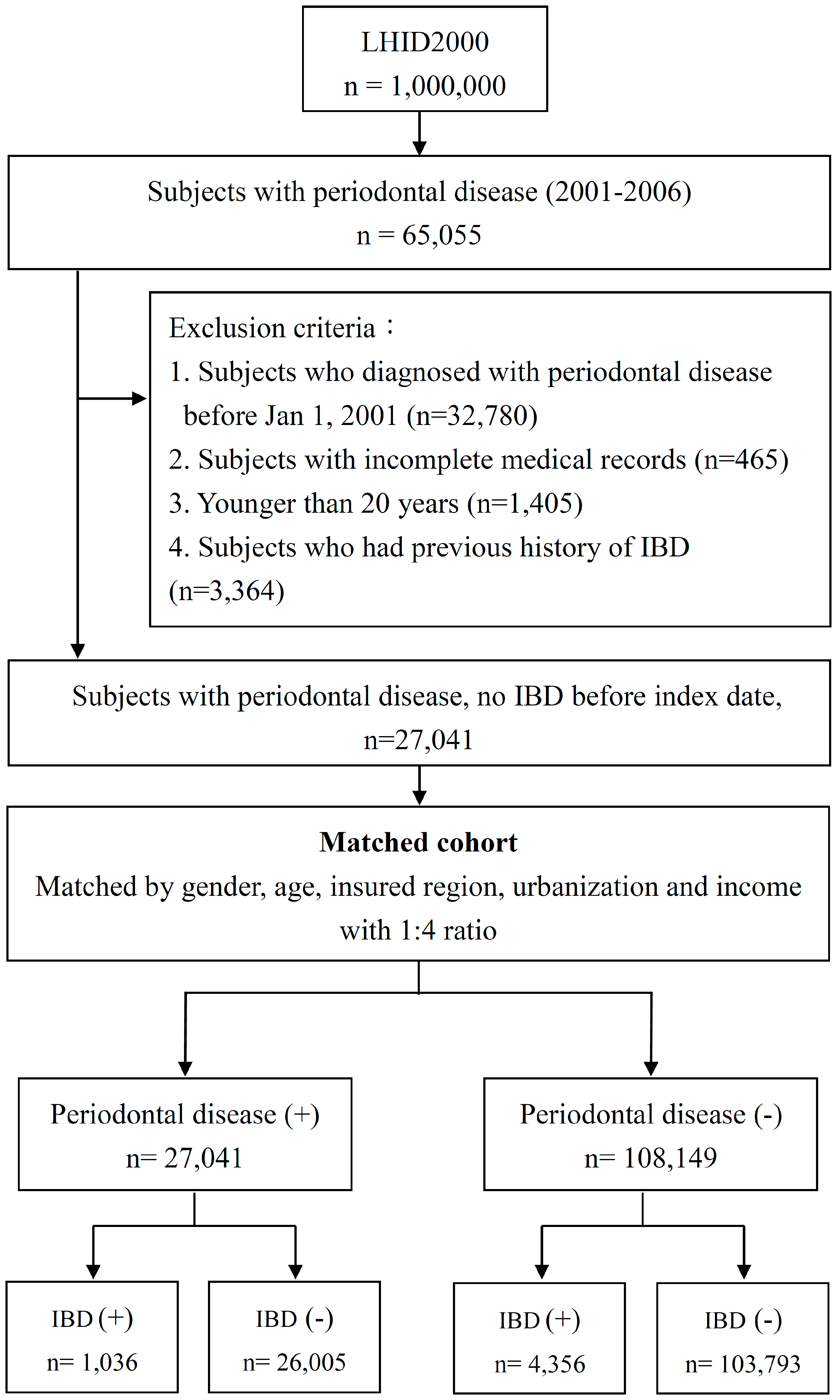
2.2. Study Population
2.3. Study Outcomes and Covariates
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kaplan, G.G.; Ng, S.C. Globalisation of inflammatory bowel disease: Perspectives from the evolution of inflammatory bowel disease in the UK and China. Lancet Gastroenterol. Hepatol. 2016, 1, 307–316. [Google Scholar] [CrossRef]
- Loftus, E.V., Jr.; Sandborn, W.J. Epidemiology of inflammatory bowel disease. Gastroenterol. Clin. N. Am. 2002, 31, 1–20. [Google Scholar] [CrossRef]
- Burisch, J.; Jess, T.; Martinato, M.; Lakatos, P.L. The burden of inflammatory bowel disease in Europe. J. Crohns Colitis 2013, 7, 322–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abraham, C.; Cho, J.H. Inflammatory bowel disease. N. Engl. J. Med. 2009, 361, 2066–2078. [Google Scholar] [CrossRef] [PubMed]
- Danese, S.; Fiocchi, C. Ulcerative colitis. N. Engl. J. Med. 2011, 365, 1713–1725. [Google Scholar] [CrossRef] [PubMed]
- Nardone, G.; Compare, D.; Rocco, A. A microbiota-centric view of diseases of the upper gastrointestinal tract. Lancet Gastroenterol. Hepatol. 2017, 2, 298–312. [Google Scholar] [CrossRef]
- Maloy, K.J.; Powrie, F. Intestinal homeostasis and its breakdown in inflammatory bowel disease. Nature 2011, 474, 298–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuoka, K.; Kanai, T. The gut microbiota and inflammatory bowel disease. Semin. Immunopatho. 2015, 37, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Kinane, D.F.; Stathopoulou, P.G.; Papapanou, P.N. Periodontal diseases. Nat. Rev. Dis. Prim. 2017, 3, 17038. [Google Scholar] [CrossRef] [PubMed]
- Nazir, M.A. Prevalence of periodontal disease, its association with systemic diseases and prevention. Int. J. Health Sci. 2017, 11, 72–80. [Google Scholar]
- Ferreira, M.C.; Dias-Pereira, A.C.; Branco-de-Almeida, L.S.; Martins, C.C.; Paiva, S.M. Impact of periodontal disease on quality of life: A systematic review. J. Periodontal Res. 2017, 52, 651–665. [Google Scholar] [CrossRef] [PubMed]
- AlJehani, Y.A. Risk factors of periodontal disease: Review of the literature. Int. J. Dentistry 2014, 2014, 182513. [Google Scholar] [CrossRef] [PubMed]
- Badran, Z.; Struillou, X.; Verner, C.; Clee, T.; Rakic, M.; Martinez, M.C.; Soueidan, A. Periodontitis as a risk factor for systemic disease: Are microparticles the missing link? Med. Hypotheses 2015, 84, 555–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alexander, M.B.; Damoulis, P.D. The role of cytokines in the pathogenesis of periodontal disease. Curr. Opin. Periodontol. 1994, 39–53. [Google Scholar]
- Figueredo, C.M.; Brito, F.; Barros, F.C.; Menegat, J.S.; Pedreira, R.R.; Fischer, R.G.; Gustafsson, A. Expression of cytokines in the gingival crevicular fluid and serum from patients with inflammatory bowel disease and untreated chronic periodontitis. J. Periodontal Res. 2011, 46, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Muñoz, F.; Dominguez-Lopez, A.; Yamamoto-Furusho, J.K. Role of cytokines in inflammatory bowel disease. World J. Gastroenterol. 2008, 14, 4280–4288. [Google Scholar] [CrossRef] [PubMed]
- Papageorgiou, S.N.; Hagner, M.; Nogueira, A.V.; Franke, A.; Jager, A.; Deschner, J. Inflammatory bowel disease and oral health: Systematic review and a meta-analysis. J. Clin. Periodontol. 2017, 44, 382–393. [Google Scholar] [CrossRef] [PubMed]
- Agossa, K.; Dendooven, A.; Dubuquoy, L.; Gower-Rousseau, C.; Delcourt-Debruyne, E.; Capron, M. Periodontal manifestations of inflammatory bowel disease: Emerging epidemiologic and biologic evidence. J. Periodontal Res. 2017, 52, 313–324. [Google Scholar] [CrossRef] [PubMed]
- Brito, F.; de Barros, F.C.; Zaltman, C.; Carvalho, A.T.; Carneiro, A.J.; Fischer, R.G.; Gustafsson, A.; Figueredo, C.M. Prevalence of periodontitis and dmft index in patients with crohn’s disease and ulcerative colitis. J. Clin. Periodontol. 2008, 35, 555–560. [Google Scholar] [CrossRef] [PubMed]
- Flemmig, T.F.; Shanahan, F.; Miyasaki, K.T. Prevalence and severity of periodontal disease in patients with inflammatory bowel disease. J. Clin. Periodontol. 1991, 18, 690–697. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.Y.; Chang, F.W.; Yang, J.J.; Chang, C.H.; Yeh, C.L.; Lei, W.T.; Huang, C.F.; Liu, J.M.; Hsu, R.J. Increased risk of bipolar disorder in patients with scabies: A nationwide population-based matched-cohort study. Psychiatry Res. 2017, 257, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.Y.; Chen, C.H.; Li, C.Y.; Lai, M.L. Validating the diagnosis of acute ischemic stroke in a national health insurance claims database. J. Formos. Med. Assoc. 2015, 114, 254–259. [Google Scholar] [CrossRef] [PubMed]
- American Hospital Association; American Medical Record Association; Health Care Financing Administration; National Center for Health Statistics. Icd-9-cm coding and reporting official guidelines. American hospital association, american medical record association, health care financing administration, national center for health statistics. J. Am. Med. Rec. Assoc. 1990, 61, 1–17. [Google Scholar]
- Maaser, C.; Sturm, A.; Vavricka, S.R.; Kucharzik, T.; Fiorino, G.; Annese, V.; Calabrese, E.; Baumgart, D.C.; Bettenworth, D.; Borralho, N.P.; et al. ECCO-ESGAR guideline for diagnostic assessment in inflammatory bowel disease. J. Crohns Colitis 2018. [Google Scholar] [CrossRef]
- Su, H.J.; Chiu, Y.T.; Chiu, C.T.; Lin, Y.C.; Wang, C.Y.; Hsieh, J.Y.; Wei, S.C. Inflammatory bowel disease and its treatment in 2018: Global and Taiwanese status updates. J. Formos. Med. Assoc. 2018. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.; van Winkelhoff, A.J. Periodontal infections: Understanding the complexity—Consensus of the seventh European workshop on periodontology. J. Clin. Periodontol. 2011, 38 (Suppl. 11), 3–6. [Google Scholar] [CrossRef]
- Lira-Junior, R.; Figueredo, C.M. Periodontal and inflammatory bowel diseases: Is there evidence of complex pathogenic interactions? World J. Gastroenterol. 2016, 22, 7963–7972. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, C.; Watt, R.; Hamer, M. Toothbrushing, inflammation, and risk of cardiovascular disease: Results from scottish health survey. BMJ (Clin. Res. Ed.) 2010, 340, c2451. [Google Scholar] [CrossRef] [PubMed]
- Figueredo, C.M.; Martins, A.P.; Lira-Junior, R.; Menegat, J.B.; Carvalho, A.T.; Fischer, R.G.; Gustafsson, A. Activity of inflammatory bowel disease influences the expression of cytokines in gingival tissue. Cytokine 2017, 95, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Jaedicke, K.M.; Preshaw, P.M.; Taylor, J.J. Salivary cytokines as biomarkers of periodontal diseases. Periodontology 2000 2016, 70, 164–183. [Google Scholar] [CrossRef] [PubMed]
- Menegat, J.S.; Lira-Junior, R.; Siqueira, M.A.; Brito, F.; Carvalho, A.T.; Fischer, R.G.; Figueredo, C.M. Cytokine expression in gingival and intestinal tissues of patients with periodontitis and inflammatory bowel disease: An exploratory study. Arch. Oral Biol. 2016, 66, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Neurath, M.F. Cytokines in inflammatory bowel disease. Nat. Rev. Immunol. 2014, 14, 329–342. [Google Scholar] [CrossRef] [PubMed]
- Chandan, J.S.; Thomas, T. The impact of inflammatory bowel disease on oral health. Br. Dent. J. 2017, 222, 549–553. [Google Scholar] [CrossRef] [PubMed]
- Grossner-Schreiber, B.; Fetter, T.; Hedderich, J.; Kocher, T.; Schreiber, S.; Jepsen, S. Prevalence of dental caries and periodontal disease in patients with inflammatory bowel disease: A case-control study. J. Clin. Periodontol. 2006, 33, 478–484. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.X.; Brand, H.S.; de Boer, N.K.; Forouzanfar, T. Gastrointestinal diseases and their oro-dental manifestations: Part 2: Ulcerative colitis. Br. Dent. J. 2017, 222, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Vavricka, S.R.; Manser, C.N.; Hediger, S.; Vogelin, M.; Scharl, M.; Biedermann, L.; Rogler, S.; Seibold, F.; Sanderink, R.; Attin, T.; et al. Periodontitis and gingivitis in inflammatory bowel disease: A case-control study. Inflamm. Bowel Dis. 2013, 19, 2768–2777. [Google Scholar] [CrossRef] [PubMed]
- Habashneh, R.A.; Khader, Y.S.; Alhumouz, M.K.; Jadallah, K.; Ajlouni, Y. The association between inflammatory bowel disease and periodontitis among jordanians: A case-control study. J. Periodontal Res. 2012, 47, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.X.; Brand, H.S.; de Boer, N.K.; Forouzanfar, T. Gastrointestinal diseases and their oro-dental manifestations: Part 1: Crohn’s disease. Br. Dent. J. 2016, 221, 794–799. [Google Scholar] [CrossRef] [PubMed]
- Parkes, G.C.; Whelan, K.; Lindsay, J.O. Smoking in inflammatory bowel disease: Impact on disease course and insights into the aetiology of its effect. J. Crohns Colitis 2014, 8, 717–725. [Google Scholar] [CrossRef] [PubMed]
- Bastida, G.; Beltrán, B. Ulcerative colitis in smokers, non-smokers and ex-smokers. World J. Gastroenterol. 2011, 17, 2740–2747. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Number of Individuals | p-Value | |
|---|---|---|---|
| PD | Without PD | ||
| n = 27,041 | n = 108,149 | ||
| Gender | |||
| Female | 13,068 (48.3%) | 52,267 (48.3%) | 0.995 |
| Male | 13,973 (51.7%) | 55,882 (51.7%) | |
| Age Group | 1 | ||
| 20–29 | 4524 (16.7%) | 18,096 (16.7%) | |
| 30–39 | 4567 (16.9%) | 18,268 (16.9%) | |
| 40–49 | 6557 (24.2%) | 26,228 (24.3%) | |
| 50–59 | 5746 (21.2%) | 22,972 (21.2%) | |
| 60–69 | 3131 (11.6%) | 12,519 (11.6%) | |
| >69 | 2516 (9.3%) | 10,066 (9.3%) | |
| Income Group | <0.001 | ||
| <20000 | 17,429 (64.5%) | 78,921 (73%) | |
| 20000–39999 | 4964 (18.4%) | 17,995 (16.6%) | |
| 40000–59999 | 3032 (11.2%) | 8090 (7.5%) | |
| ≥60000 | 1616 (6%) | 3143 (2.9%) | |
| Geography | <0.001 | ||
| North | 13,351 (49.4%) | 55,469 (51.3%) | |
| Central | 5467 (20.2%) | 18,679 (17.3%) | |
| South | 7570 (28%) | 31,141 (28.8%) | |
| Other | 653 (2.4%) | 2860 (2.6%) | |
| Urbanization | <0.001 | ||
| 1 (highest) | 14,199 (52.5%) | 47,711 (44.1%) | |
| 2 | 6613 (24.5%) | 28,190 (26.1%) | |
| 3 | 4543 (16.8%) | 22,174 (20.5%) | |
| 4 (lowest) | 1686 (6.2%) | 10,074 (9.3%) | |
| Comorbidity | |||
| DM | 6202 (22.9%) | 18,593 (17.2%) | <0.001 |
| Hypertension | 10,262 (37.9%) | 34,099 (31.5%) | <0.001 |
| Hyperlipidemia | 9678 (35.8%) | 27,903 (25.8%) | <0.001 |
| CAD | 5418 (20%) | 15,657 (14.5%) | <0.001 |
| Stroke | 3447 (12.7%) | 10,738 (9.9%) | <0.001 |
| Alcoholism | 481 (1.8%) | 2213 (2%) | <0.05 |
| Obesity | 436 (1.6%) | 1292 (1.2%) | <0.001 |
| Tobacco use disorder | 4373 (16.2%) | 12,026 (11.1%) | <0.001 |
| PD (n = 27,041) | Without PD (n = 108,149) | Crude | Adjusted | |||||
|---|---|---|---|---|---|---|---|---|
| Disease | n | PY | IR | n | PY | IR | HR (95% CI) | HR * (95% CI) |
| Inflammatory bowel disease (IBD) | 1036 (3.83%) | 230,635 | 4.49 | 4356 (4.03%) | 915,520 | 4.76 | 0.95 (0.88–1.01) | 1.01 (0.94–1.08) |
| Crohn’s disease | 985 (3.64%) | 230,872 | 4.27 | 4235 (3.92%) | 916,252 | 4.62 | 0.92 (0.86–0.99) | 0.99 (0.92–1.06) |
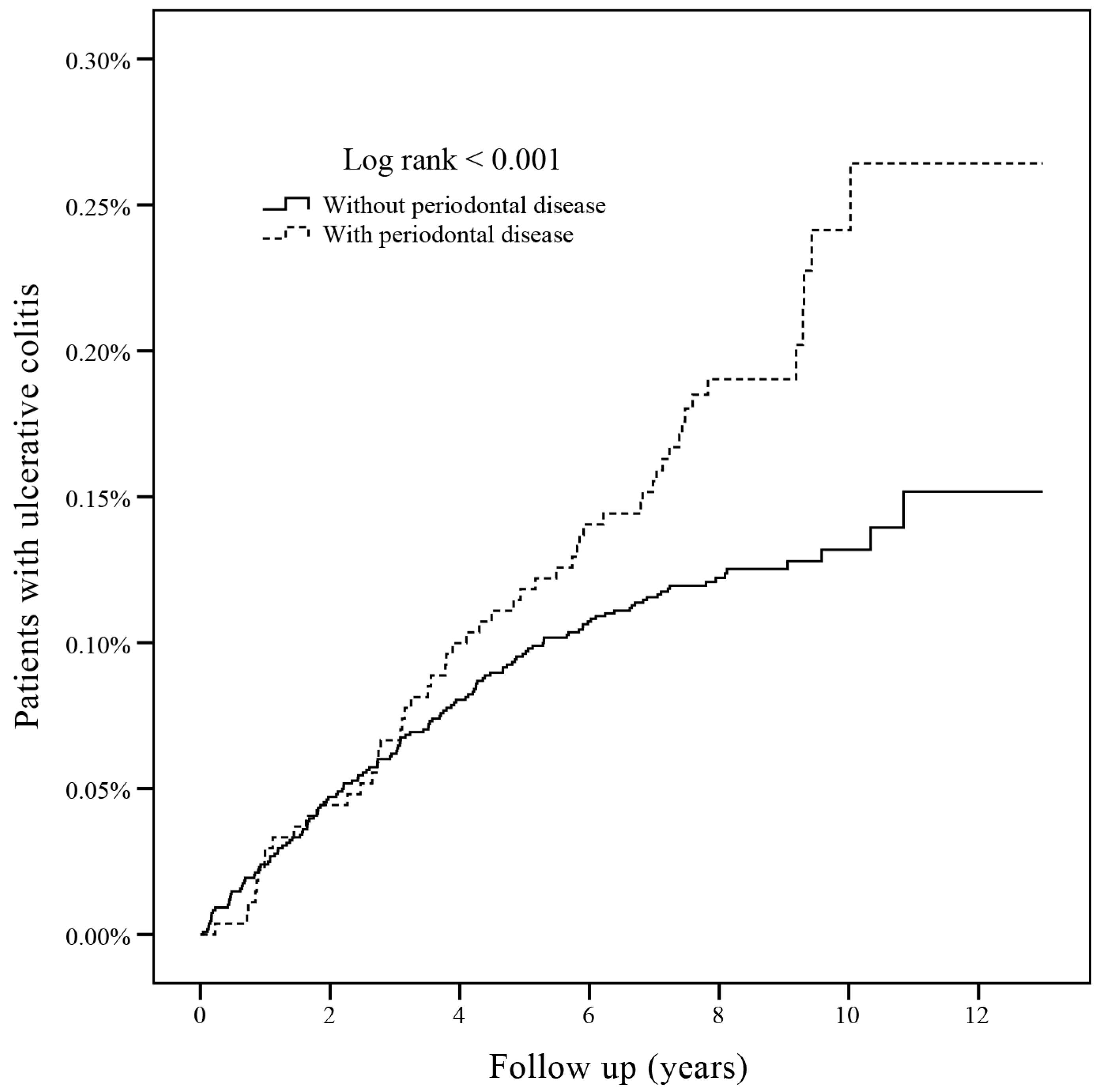
| Ulcerative colitis | 55 (0.20%) | 235,357 | 0.23 | 137 (0.12%) | 941,514 | 0.15 | 1.61 (1.17–2.20) † | 1.56 (1.13–2.15) † |
| Variable | Crude | Adjusted | |
|---|---|---|---|
| HR (95% CI) | HR * (95% CI) | ||
| PD | 1.61 (1.17–2.20) † | 1.56 (1.13–2.15) † | |
| Gender | |||
| Female | 1 | 1 | |
| Male | 1.01 (0.76–1.34) | 0.96 (0.72–1.29) | |
| Age | |||
| 20–29 | 1 | 1 | |
| 30–39 | 0.47 (0.26–0.86) † | 0.46 (0.25–0.85) † | |
| 40–49 | 0.82 (0.52–1.3) | 0.79 (0.49–1.28) | |
| 50–59 | 0.99 (0.62–1.56) | 0.98 (0.6–1.61) | |
| 60–69 | 1.5 (0.93–2.41) | 1.61 (0.95–2.74) | |
| ≥70 | 1.38 (0.83–2.31) | 1.54 (0.87–2.72) | |
| Income | |||
| <20000 | 1 | 1 | |
| 20000–39999 | 0.84 (0.56–1.27) | 0.99 (0.65–1.52) | |
| 40000–59999 | 1.02 (0.61–1.72) | 1.26 (0.73–2.17) | |
| ≥60000 | 2.09 (1.2–3.62) † | 2.29 (1.28–4.11) † | |
| Geography | |||
| North | 1 | 1 | |
| Central | 1.79 (1.27–2.51) † | 1.86 (1.29–2.66) † | |
| South | 0.87 (0.6–1.25) | 0.89 (0.61–1.31) | |
| Other | 2.27 (1.18–4.37) † | 2.38 (1.21–4.68) † | |
| Urbanization | |||
| 1 (highest) | 1 | 1 | |
| 2 | 0.77 (0.53–1.11) | 0.71 (0.49–1.03) | |
| 3 | 1.17 (0.82–1.66) | 0.99 (0.68–1.45) | |
| 4 | 0.68 (0.37–1.23) | 0.59 (0.31–1.10) | |
| Comorbidity | |||
| DM | 0.95 (0.66–1.37) | 0.85 (0.56–1.30) | |
| Hypertension | 1.22 (0.91–1.64) | 1.10 (0.75–1.60) | |
| Hyperlipidemia | 0.87 (0.63–1.20) | 0.74 (0.50–1.08) | |
| CAD | 1.31 (0.92–1.86) | 1.20 (0.80–1.80) | |
| Stroke | 1.32 (0.88–1.98) | 1.13 (0.72–1.78) | |
| Alcoholism | 1.00 (0.37–2.69) | 1.18 (0.44–3.22) | |
| Obesity | 0.39 (0.05–2.77) | 0.45 (0.06–3.24) | |
| Tobacco use disorder | 0.58 (0.34–0.98) † | 0.47 (0.27–0.81) † | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.-Y.; Tseng, K.-S.; Liu, J.-M.; Chuang, H.-C.; Lien, C.-H.; Chen, Y.-C.; Lai, C.-Y.; Yu, C.-P.; Hsu, R.-J. Increased Risk of Ulcerative Colitis in Patients with Periodontal Disease: A Nationwide Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2018, 15, 2602. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15112602
Lin C-Y, Tseng K-S, Liu J-M, Chuang H-C, Lien C-H, Chen Y-C, Lai C-Y, Yu C-P, Hsu R-J. Increased Risk of Ulcerative Colitis in Patients with Periodontal Disease: A Nationwide Population-Based Cohort Study. International Journal of Environmental Research and Public Health. 2018; 15(11):2602. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15112602
Chicago/Turabian StyleLin, Chien-Yu, Kuo-Sen Tseng, Jui-Ming Liu, Heng-Chang Chuang, Chi-Hone Lien, Yi-Chih Chen, Chun-Ying Lai, Cheng-Ping Yu, and Ren-Jun Hsu. 2018. "Increased Risk of Ulcerative Colitis in Patients with Periodontal Disease: A Nationwide Population-Based Cohort Study" International Journal of Environmental Research and Public Health 15, no. 11: 2602. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15112602