Methodological Challenges in the Economic Evaluation of Occupational Health and Safety Programmes


{kind=link}
Abstract
:1. Introduction
2. Methods
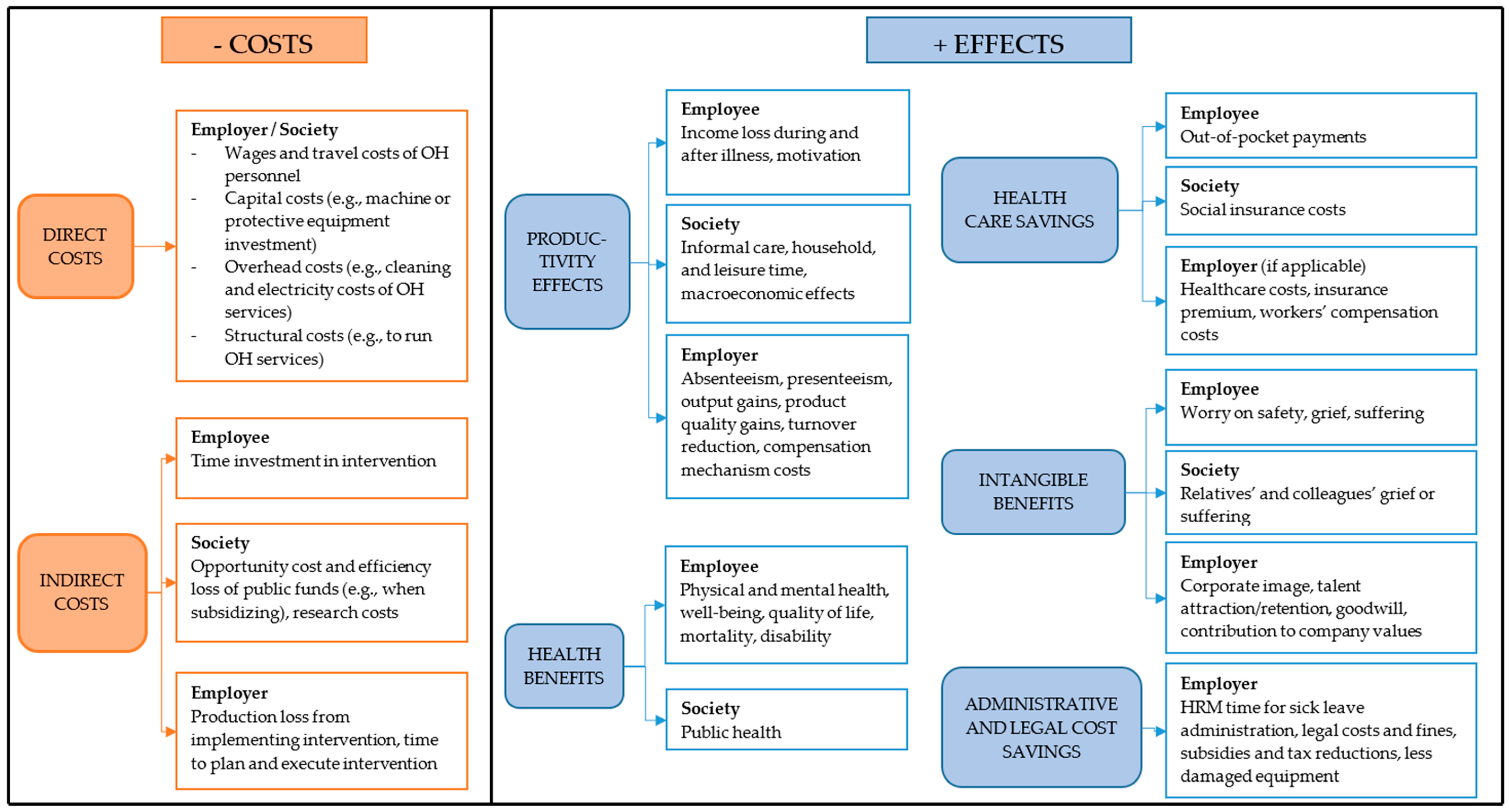
3. Three Challenges of Economic Evaluation in Occupational Health and Safety
3.1. Effects of OHS on Worker Productivity
3.2. Intangible Benefits of OHS
3.3. Accounting for the Legal and Fiscal Context
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Chandra, A.; Skinner, J. Technology growth and expenditure growth in health care. J. Econ. Lit. 2012, 50, 645–680. [Google Scholar] [CrossRef]
- Heuvel, S.; Zwaan, L.; Dam, L.V.; Oude Hengel, K.; Eekhout, I.; van Emmerik, M.; Oldenburg, C.; Brück, C.; Janowski, P.; Wilhelm, C. Estimating the Costs of Work-Related Accidents and Ill-Health: An Analysis of European Data Sources; No.: 9292409975; European Agency for Safety and Health at Work (EU-OSHA): Luxembourg, 2017. [Google Scholar]
- Burton, J.; World Health Organization. Who Healthy Workplace Framework and Model: Background and Supporting Literature and Practices; Report No.: 9241500247; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Lucchini, R.G.; London, L. Global occupational health: Current challenges and the need for urgent action. Ann. Glob. Health 2014, 80, 251–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burdorf, A. Economic evaluation in occupational health—Its goals, challenges, and opportunities. Scand. J. Work Environ. Health 2007, 161–164. [Google Scholar] [CrossRef]
- Luyten, J.; Steel, J.; Godderis, L. Economic evaluation of occupational health services: Necessary, challenging and promising. Occup. Environ. Med. 2017, 74, 847–848. [Google Scholar] [CrossRef] [PubMed]
- van der Molen, H.F.; Stocks, S.J.; Frings-Dresen, M.H. Exploring study designs for evaluation of interventions aimed to reduce occupational diseases and injuries. Saf. Health Work 2016, 7, 83–85. [Google Scholar] [CrossRef] [PubMed]
- Tompa, E.; Verbeek, J.; van Tulder, M.; de Boer, A. Developing guidelines for good practice in the economic evaluation of occupational safety and health interventions. Scand. J. Work Environ. Health 2010, 36, 313–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edwards, R.T.; Charles, J.M.; Lloyd-Williams, H. Public health economics: A systematic review of guidance for the economic evaluation of public health interventions and discussion of key methodological issues. BMC Publ. Health 2013, 13, 1001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Payne, K.; McAllister, M.; Davies, L.M. Valuing the economic benefits of complex interventions: When maximising health is not sufficient. Health Econ. 2013, 22, 258–271. [Google Scholar] [CrossRef] [PubMed]
- Olsen, O.; Albertsen, K.; Nielsen, M.L.; Poulsen, K.B.; Gron, S.M.F.; Brunnberg, H.L. Workplace restructurings in intervention studies—A challenge for design, analysis and interpretation. BMC Med. Res. Methodol. 2008, 8, 39. [Google Scholar] [CrossRef] [PubMed]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M.; Medical Research Council, G. Developing and evaluating complex interventions: The new medical research council guidance. BMJ 2008, 337, a1655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiell, A.; Hawe, P.; Gold, L. Complex interventions or complex systems? Implications for health economic evaluation. BMJ 2008, 336, 1281. [Google Scholar] [CrossRef] [PubMed]
- Drummond, M.F.; Sculpher, M.J.; Claxton, K.; Stoddart, G.L.; Torrance, G.W. Methods for the Economic Evaluation of Health care Programmes, 4th ed.; Oxford Univ Press: Oxford, UK, 2015; ISBN 0191643580. [Google Scholar]
- Tompa, E.; Dolinschi, R.; de Oliveira, C. Practice and potential of economic evaluation of workplace-based interventions for occupational health and safety. J. Occup. Rehabil. 2006, 16, 375–400. [Google Scholar] [CrossRef] [PubMed]
- Hamberg-van Reenen, H.H.; Proper, K.I.; van den Berg, M. Worksite mental health interventions: A systematic review of economic evaluations. Occup. Environ. Med. 2012, 69, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Uegaki, K.; de Bruijne, M.C.; Lambeek, L.; Anema, J.R.; van der Beek, A.J.; van Mechelen, W.; van Tulder, M.W. Economic evaluations of occupational health interventions from a corporate perspective—A systematic review of methodological quality. Scand. J. Work Environ. Health 2010, 36, 273–288. [Google Scholar] [CrossRef] [PubMed]
- Niven, K.J. A review of the application of health economics to health and safety in healthcare. Health Policy 2002, 61, 291–304. [Google Scholar] [CrossRef]
- Tompa, E.; Culyer, A.J.; Dolinschi, R. Economic Evaluation of Interventions for Occupational Health and Safety: Developing Good Practice; Oxford Univ Press: Oxford, UK, 2008; ISBN 0199533598. [Google Scholar]
- Mossink, J.; de Greef, M. Inventory of Socioeconomic Costs of Work Accidents; 9295007670; Office for Official Publications of the European Communities: Luxembourg, 2002. [Google Scholar]
- Steel, J.; Godderis, L.; Luyten, J. Productivity estimation in economic evaluations of occupational health and safety interventions: A systematic review. Scand. J. Work Environ. Health 2018. [Google Scholar] [CrossRef] [PubMed]
- Steel, J.; Luyten, J.; Godderis, L. Occupational Health: The Global Evidence And Value; Society of Occupational Medicine (SOM): London, UK, 2018; pp. 1–92. [Google Scholar]
- Van Dongen, J.M.; Tompa, E.; Clune, L.; Sarnocinska-Hart, A.; Bongers, P.M.; van Tulder, M.W.; van der Beek, A.J.; van Wier, M.F. Bridging the gap between the economic evaluation literature and daily practice in occupational health: A qualitative study among decision-makers in the healthcare sector. Implement Sci. 2013, 8, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tompa, E.; Dolinschi, R.; de Oliveira, C.; Irvin, E. A systematic review of occupational health and safety interventions with economic analyses. J. Occup. Environ. Med./Am. Coll. Occup. Environ. Med. 2009, 51, 1004–1023. [Google Scholar] [CrossRef] [PubMed]
- Colosio, C.; Mandic-Rajcevic, S.; Godderis, L.; van der Laan, G.; Hulshof, C.; van Dijk, F. Workers’ health surveillance: Implementation of the directive 89/391/eec in europe. Occup Med.-C 2017, 67, 574–578. [Google Scholar] [CrossRef] [PubMed]
- Ison, T.G. Worker’s compensation systems. In Encyclopaedia of Occupational Health and Safety, 4th ed.; Stellman, J.M., Ed.; International Labour Organization: Geneva, Switzerland, 1998. [Google Scholar]
- Syverson, C. What determines productivity? J. Econ. Lit. 2011, 49, 326–365. [Google Scholar] [CrossRef]
- Anders, B.; Ommen, O.; Pfaff, H.; Lüngen, M.; Lefering, R.; Thüm, S.; Janssen, C. Direct, indirect, and intangible costs after severe trauma up to occupational reintegration—An empirical analysis of 113 seriously injured patients. GMS Psycho-Soc.-Med. 2013, 10. [Google Scholar] [CrossRef]
- Krol, M.; Brouwer, W.; Rutten, F. Productivity costs in economic evaluations: Past, present, future. Pharm. Econom. 2013, 31, 537–549. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Bansback, N.; Anis, A.H. Measuring and valuing productivity loss due to poor health: A critical review. Soc. Sci. Med. 2011, 72, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Krol, M.; Brouwer, W. How to estimate productivity costs in economic evaluations. Pharmacoeconomics 2014, 32, 335–344. [Google Scholar] [CrossRef] [PubMed]
- Mattke, S.; Balakrishnan, A.; Bergamo, G.; Newberry, S.J. A review of methods to measure health-related productivity loss. Am. J. Manag. Care 2007, 13, 211–217. [Google Scholar] [PubMed]
- Koopmanschap, M.A.; Rutten, F.F.; van Ineveld, B.M.; van Roijen, L. The friction cost method for measuring indirect costs of disease. J. Health Econ. 1995, 14, 171–189. [Google Scholar] [CrossRef]
- Kigozi, J.; Jowett, S.; Lewis, M.; Barton, P.; Coast, J. Valuing productivity costs using the friction-cost approach: Estimating friction-period estimates by occupational classifications for the uk. Health Econ. 2017. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, S.; Pauly, M.V.; Polsky, D.; Sharda, C.; Szrek, H.; Berger, M.L. Measuring the effects of work loss on productivity with team production. Health Econ. 2006, 15, 111–123. [Google Scholar] [CrossRef] [PubMed]
- Pauly, M.V.; Nicholson, S.; Xu, J.; Polsky, D.; Danzon, P.M.; Murray, J.F.; Berger, M.L. A general model of the impact of absenteeism on employers and employees. Health Econ. 2002, 11, 221–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oostenbrink, J.B.; Koopmanschap, M.A.; Rutten, F.F. Standardisation of costs: The dutch manual for costing in economic evaluations. Pharmacoeconomics 2002, 20, 443–454. [Google Scholar] [CrossRef] [PubMed]
- Lensberg, B.R.; Drummond, M.F.; Danchenko, N.; Despiegel, N.; Francois, C. Challenges in measuring and valuing productivity costs, and their relevance in mood disorders. ClinicoEcon. Outcomes Res. 2013, 5, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.S.; Bouwmans, C.A.; Rutten, F.F.; Hakkaart-van Roijen, L. Update of the dutch manual for costing in economic evaluations. Int. J. Technol. Assess Health Care 2012, 28, 152–158. [Google Scholar] [CrossRef] [PubMed]
- van Wier, M.F.; Verweij, L.M.; Proper, K.I.; Hulshof, C.T.; van Tulder, M.W.; van Mechelen, W. Economic evaluation of an occupational health care guideline for prevention of weight gain among employees. J. Occup. Environ. Med./Am. Coll. Occup. Environ. Med. 2013, 55, 1100–1109. [Google Scholar] [CrossRef] [PubMed]
- Lofland, J.H.; Pizzi, L.; Frick, K.D. A review of health-related workplace productivity loss instruments. Pharmacoeconomics 2004, 22, 165–184. [Google Scholar] [CrossRef] [PubMed]
- Kigozi, J.; Jowett, S.; Lewis, M.; Barton, P.; Coast, J. The estimation and inclusion of presenteeism costs in applied economic evaluation: A systematic review. Value Health 2017, 20, 496–506. [Google Scholar] [CrossRef] [PubMed]
- Jeanrenaud, C.; Pellegrini, S. Valuing intangible costs of alcohol dependence: A contingent valuation study. Rev. Econ. Polit. 2007, 117, 813–825. [Google Scholar] [CrossRef]
- Brymer, R.A.; Molloy, J.C.; Gilbert, B.A. Human capital pipelines: Competitive implications of repeated interorganizational hiring. J. Manag. 2014, 40, 483–508. [Google Scholar] [CrossRef]
- Kucherov, D.; Zavyalova, E. Hrd practices and talent management in the companies with the employer brand. Eur. J. Train. Dev. 2012, 36, 86–104. [Google Scholar] [CrossRef]
- Troman, G.; Woods, P. Careers under stress: Teacher adaptations at a time of intensive reform. J. Educ. Chang. 2000, 1, 253–275. [Google Scholar] [CrossRef]
- Buchan, J.; Campbell, J. Challenges posed by the global crisis in the health workforce. BMJ 2013, 347, f6201. [Google Scholar] [CrossRef] [PubMed]
- Ponsonby, W. Global occupational health. Occup. Med. (Lond.) 2017, 67, 331–333. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, M.F.; Tanim, T.R. Industrial accidents in bangladesh apparel manufacturing sector: An analysis of the two most deadliest accidents in history. Asian J. Soc. Sci. Manag. Stud. 2016, 3, 115–126. [Google Scholar] [CrossRef]
- McCurry, J. Japanese woman ‘dies from overwork’ after logging 159 hours of overtime in a month. The Guardian, 5 October 2017. [Google Scholar]
- Smallman, C.; John, G. British directors perspectives on the impact of health and safety on corporate performance. Saf. Sci. 2001, 38, 227–239. [Google Scholar] [CrossRef]
- Clarke, V. Honesty and Integrity: Is This the Edge Businesses Need in a Stagnant Economy? Available online: https://www.ipsos.com/ipsos-mori/en-uk/honesty-and-integrity-edge-businesses-need-stagnant-economy (accessed on 27 September 2018).
- Aven, T. On how to define, understand and describe risk. Reliab. Eng. Syst. Saf. 2010, 95, 623–631. [Google Scholar] [CrossRef]
- Aven, T.; Zio, E. Foundational issues in risk assessment and risk management. Risk Anal. 2014, 34, 1164–1172. [Google Scholar] [CrossRef] [PubMed]
- Paté-Cornell, E. On “black swans” and “perfect storms”: Risk analysis and management when statistics are not enough. Risk Anal. 2012, 32, 1823–1833. [Google Scholar] [CrossRef] [PubMed]
- Apostolakis, G.E. How useful is quantitative risk assessment? Risk Anal. 2004, 24, 515–520. [Google Scholar] [CrossRef] [PubMed]
- Briggs, A.; Sculpher, M.; Claxton, K. Decision Modelling for Health Economic Evaluation; Oxford University Press: Oxford, UK, 2006; ISBN 0198526629. [Google Scholar]
- Slovic, P. Perception of risk. Science 1987, 236, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Miller, P.; Haslam, C. Why employers spend money on employee health: Interviews with occupational health and safety professionals from british industry. Saf. Sci. 2009, 47, 163–169. [Google Scholar] [CrossRef]
- Drummond, M.F.; Sculpher, M.J.; Torrance, G.W.; O’Brien, B.J.; Stoddart, G.L. Methods for the Economic Evaluation of Health Care Programmes, 3rd ed.; Oxford University Press: Oxford, UK, 2005; ISBN 0198529487. [Google Scholar]
- Ware, J.E., Jr.; Sherbourne, C.D. The mos 36-item short-form health survey (sf-36): I. Conceptual framework and item selection. Med Care 1992, 473–483. [Google Scholar] [CrossRef]
- Sancroft. Maximising the Value of Occupational Health & Safety and Workplace Wellness reporting for a Global Workforce: A Practical Guide for Internationally Operating Employers; International SOS Foundation: London, UK, 2017. [Google Scholar]
- Evangelinos, K.; Fotiadis, S.; Skouloudis, A.; Khan, N.; Konstandakopoulou, F.; Nikolaou, I.; Lundy, S. Occupational health and safety disclosures in sustainability reports: An overview of trends among corporate leaders. Corp. Soc. Responsib. Environ. Manag. 2018. [Google Scholar] [CrossRef]
- Gagné, M.; Forest, J.; Gilbert, M.-H.; Aubé, C.; Morin, E.; Malorni, A. The motivation at work scale: Validation evidence in two languages. Educ. Psychol. Meas. 2010, 70, 628–646. [Google Scholar] [CrossRef]
- Piko, B.F. Burnout, role conflict, job satisfaction and psychosocial health among hungarian health care staff: A questionnaire survey. Int. J. Nurs. Stud. 2006, 43, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Cravens, K.; Oliver, E.G.; Ramamoorti, S. The reputation index: Measuring and managing corporate reputation. Eur. Manag. J. 2003, 21, 201–212. [Google Scholar] [CrossRef]
- Barling, J.; Hutchinson, I. Commitment vs. Control-based safety practices, safety reputation, and perceived safety climate. Can. J. Adm. Sci. 2000, 17, 76–84. [Google Scholar] [CrossRef]
- Dekker, S.W. The bureaucratization of safety. Saf. Sci. 2014, 70, 348–357. [Google Scholar] [CrossRef]
- Esler, D.; Eeckelaert, L.; Knight, A.; Treutlein, D.; Pecillo, M.; Elo-Schäfer, J.; Roskams, N.; Zwinkels, W.; Koukoulaki, T.; Dontas, S. Economic Incentives to improve Occupational Safety and Health: A Review from the European Perspective; European Union: Brussels, Belgium, 2010. [Google Scholar]
- Lalloo, D.; Demou, E.; Smedley, J.; Madan, I.; Asanati, K.; Macdonald, E.B. Current research priorities for uk occupational physicians and occupational health researchers: A modified delphi study. Occup. Environ. Med. 2018. [Google Scholar] [CrossRef] [PubMed]
- Krol, M.; Stolk, E.; Brouwer, W. Predicting productivity based on eq-5d: An explorative study. Eur. J. Health Econ. 2014, 15, 465–475. [Google Scholar] [CrossRef] [PubMed]
- Jones, C. The Economics of Presenteeism in the Context of Rheumatoid Arthritis, Ankylosing Spondylitis and Psoriatic Arthritis; University of Manchester: Manchester, UK, 2018. [Google Scholar]
- Ambler, T.; Roberts, J.H. Assessing marketing performance: Don’t settle for a silver metric. J. Market. Manag. 2008, 24, 733–750. [Google Scholar] [CrossRef]
- Rosen, H.S.; Gayer, T. Public Finance, 9th ed.; Mc Graw Hill: New York, NY, USA, 2010; ISBN 9780071267885. [Google Scholar]
- Steen, A.; Welch, D. Are accounting metrics applicable to human resources? The case of return on valuing assignments. Australas. Account. Bus. Financ. J. 2011, 5, 57–72. [Google Scholar]

© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Steel, J.; Godderis, L.; Luyten, J. Methodological Challenges in the Economic Evaluation of Occupational Health and Safety Programmes. Int. J. Environ. Res. Public Health 2018, 15, 2606. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15112606
Steel J, Godderis L, Luyten J. Methodological Challenges in the Economic Evaluation of Occupational Health and Safety Programmes. International Journal of Environmental Research and Public Health. 2018; 15(11):2606. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15112606
Chicago/Turabian StyleSteel, Jonas, Lode Godderis, and Jeroen Luyten. 2018. "Methodological Challenges in the Economic Evaluation of Occupational Health and Safety Programmes" International Journal of Environmental Research and Public Health 15, no. 11: 2606. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15112606