Using Cross-Sectional Data to Identify and Quantify the Relative Importance of Factors Associated with and Leading to Food Insecurity

 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample and Measures
2.2. Analysis
3. Results
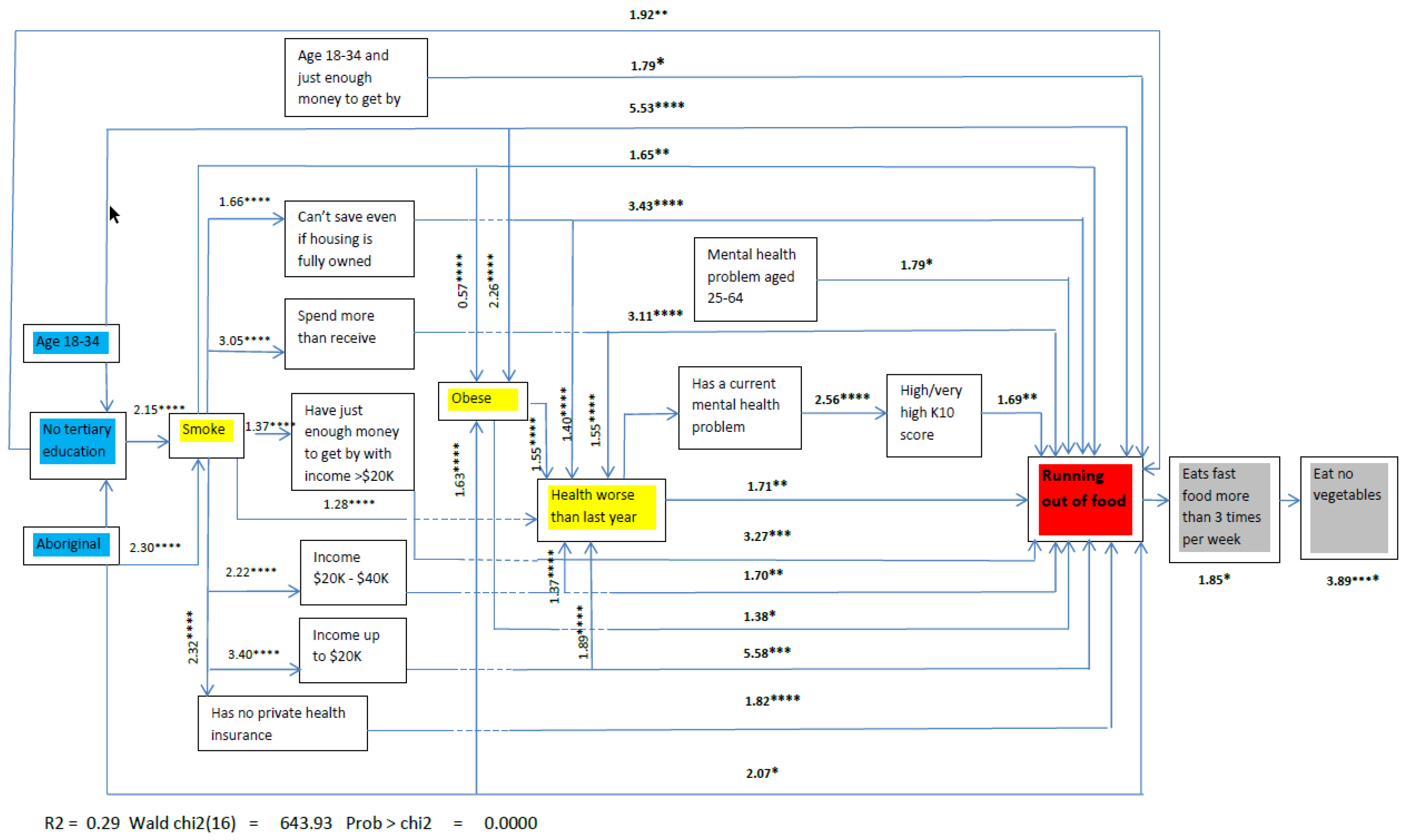
3.1. Direct Associations with Food Insecurity
3.2. Effect Modifiers in the Food Insecurity Path
3.3. Adjustment for Covariates and Indicators of Hypothetical Causality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Food and Agriculture Organization. Rome Declaration on World Food Security and World Food Summit Plan of Action: World Food Summit 13–17 November; FAO: Rome, Italy, 1996. [Google Scholar]
- Anderson, S.A. Core indicators of nutritional state for difficult-to-sample populations. J. Nutr. 1990, 120, 1555–1600. [Google Scholar] [CrossRef] [PubMed]
- Riches, G. Food Bank Nations: Poverty, Corporate Charity and the Right to Food; Routledge: New York, NJ, USA, 2018. [Google Scholar]
- Hanson, K.L.; Connor, L.M. Food insecurity and dietary quality in us adults and children: A systematic review. Am. J. Clin. Nutr. 2014, 100, 684–692. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.D.; Ngure, F.M.; Pelto, G.; Young, S.L. What are we assessing when we measure food security? A compendium and review of current metrics. Adv. Nutr. 2013, 4, 481–505. [Google Scholar] [CrossRef] [PubMed]
- Robaina, K.A.; Martin, K.S. Food insecurity, poor diet quality, and obesity among food pantry participants in hartford, ct. J. Nutr. Educ. Behav. 2013, 45, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Dowler, E. Symposium on ‘intervention policies for deprived households’ policy initiatives to address low-income households’ nutritional needs in the uk. Proc. Nutr. Soc. 2008, 67, 289–300. [Google Scholar] [CrossRef] [PubMed]
- Mook, K.; Laraia, B.A.; Oddo, V.M.; Jones-Smith, J.C. Food security status and barriers to fruit and vegetable consumption in two economically deprived communities of oakland, california, 2013–2014. Prev. Chronic Dis. 2016, 13, E21. [Google Scholar] [CrossRef] [PubMed]
- Tingay, R.S.; Tan, C.J.; Tan, N.C.; Tang, S.; Teoh, P.F.; Wong, R.; Gulliford, M.C. Food insecurity and low income in an english inner city. J. Public Health Med. 2003, 25, 156–159. [Google Scholar] [CrossRef] [PubMed]
- Thornton, L.E.; Pearce, J.R.; Ball, K. Sociodemographic factors associated with healthy eating and food security in socio-economically disadvantaged groups in the uk and victoria, australia. Public Health Nutr. 2013, 17, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Metallinos-Katsaras, E.; Must, A.; Gorman, K. A longitudinal study of food insecurity on obesity in preschool children. J. Acad. Nutr. Diet. 2012, 112, 1949–1958. [Google Scholar] [CrossRef] [PubMed]
- Larson, N.I.; Story, M.T. Food insecurity and weight status among u.S. Children and families: A review of the literature. Am. J. Prev. Med. 2011, 40, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Crawford, P.B.; Webb, K.L. Unraveling the paradox of concurrent food insecurity and obesity. Am. J. Prev. Med. 2011, 40, 274–275. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, D.C.; Marshall, A.; Mineo, C. Maternal depression mediates the association between intimate partner violence and food insecurity. J. Womens Health 2014, 23, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Young, S.L.; Plenty, A.H.; Luwedde, F.A.; Natamba, B.K.; Natureeba, P.; Achan, J.; Mwesigwa, J.; Ruel, T.D.; Ades, V.; Osterbauer, B.; et al. Household food insecurity, maternal nutritional status, and infant feeding practices among hiv-infected ugandan women receiving combination antiretroviral therapy. Matern. Child Health J. 2014, 18, 2044–2053. [Google Scholar] [CrossRef] [PubMed]
- Whitaker, R.C.; Phillips, S.M.; Orzol, S.M. Food insecurity and the risks of depression and anxiety in mothers and behavior problems in their preschool-aged children. Pediatrics 2006, 118, E859–E868. [Google Scholar] [CrossRef] [PubMed]
- Melchior, M.; Chastang, J.F.; Falissard, B.; Galera, C.; Tremblay, R.E.; Cote, S.M.; Boivin, M. Food insecurity and children’s mental health: A prospective birth cohort study. PLoS ONE 2012, 7, e52615. [Google Scholar] [CrossRef] [PubMed]
- Muldoon, K.A.; Duff, P.K.; Fielden, S.; Anema, A. Food insufficiency is associated with psychiatric morbidity in a nationally representative study of mental illness among food insecure canadians. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 48, 795–803. [Google Scholar] [CrossRef] [PubMed]
- Pobutsky, A.M.; Baker, K.K.; Reyes-Salvail, F. Investigating measures of social context on 2 population-based health surveys, hawaii, 2010–2012. Prev. Chron. Dis. 2015, 12, E221. [Google Scholar]
- Friel, S. Climate change, food insecurity and chronic diseases: Sustainable and healthy policy opportunities for australia. N. S. W. Public Health Bull. 2010, 21, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Ashe, L.M.; Sonnino, R. At the crossroads: New paradigms of food security, public health nutrition and school food. Public Health Nutr. 2013, 16, 1020–1027. [Google Scholar] [CrossRef] [PubMed]
- Tarasuk, V. Implications of a Basic Income Guarantee for Household Food Insecurity. Northern Policy Institute, 2017. Available online: https://proof.utoronto.ca/wp-content/uploads/2017/06/Paper-Tarasuk-BIG-EN-17.06.13-1712.pdf (accessed on 22 November 2018).
- Lang, T.; Barling, D.; Caraher, M. Food, social policy and the environment: Towards a new model. Soc. Policy Adm. 2001, 35, 538–558. [Google Scholar] [CrossRef]
- Food and Agriculture Organisation. Declaration of the World Summit on Food Security 16–18 November; Food and Agriculture Organisation: Rome, Italiy, 2009. [Google Scholar]
- Carletto, C.; Zezza, A.; Banerjee, R. Towards better measurement of household food security: Harmonizing indicators and the role of household surveys. Glob. Food Secur. 2013, 2, 30–40. [Google Scholar] [CrossRef]
- Ecker, O.; Breisinger, C. The Food Security System: A New Conceptual Framework. International Food Policy Research Institute, 2012. Available online: http://ebrary.ifpri.org/cdm/ref/collection/p15738coll2/id/126837 (accessed on 22 November 2018).
- Rideout, K.; Seed, B.; Ostry, A. Putting food on the public health table: Making food security relevant to regional health authorities. Can. J. Public Health 2006, 97, 233–236. [Google Scholar] [PubMed]
- Bastian, A.; Coveney, J. Local evidenced-based policy options to improve food security in south australia: The use of local knowledge in policy development. Public Health Nutr. 2012, 15, 1497–1502. [Google Scholar] [CrossRef] [PubMed]
- Bell, E. Research for Health Policy; Oxford University Press: Oxford, UK, 2009. [Google Scholar]
- Caraher, M.; Coveney, J. Public health nutrition and food policy. Public Health Nutr. 2004, 7, 591–598. [Google Scholar] [CrossRef] [PubMed]
- Booth, S.; Smith, A. Food security and poverty in australia-challenges for dietitians. Aust. J. Nutr. Diet. 2001, 58, 150–156. [Google Scholar]
- Tarasuk, V. Health implications of food insecurity. Soc. Déterm. Health Can. Perspect. 2004, 187–200. [Google Scholar]
- Dinour, L.M.; Bergen, D.; Yeh, M.-C. The food insecurity–obesity paradox: A review of the literature and the role food stamps may play. J. Am. Diet. Assoc. 2007, 107, 1952–1961. [Google Scholar] [CrossRef] [PubMed]
- Franklin, B.; Jones, A.; Love, D.; Puckett, S.; Macklin, J.; White-Means, S. Exploring mediators of food insecurity and obesity: A review of recent literature. J. Commun. Health 2012, 37, 253–264. [Google Scholar] [CrossRef] [PubMed]
- HLPE, Nutrition and Food Systems. A Report by the High Level Panel of Experts on Food Security and Nutrition of the Committee on World Food Security; HLPE: Rome, Italy, 2017. [Google Scholar]
- Foley, W.; Ward, P.; Carter, P.; Coveney, J.; Tsourtos, G.; Taylor, A. An ecological analysis of factors associated with food insecurity in south australia, 2002–2007. Public Health Nutr. 2010, 13, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Quine, S.; Morrell, S. Food insecurity in community-dwelling older australians. Public Health Nutr. 2006, 9, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Russell, J.; Flood, V.; Yeatman, H.; Mitchell, P. Prevalence and risk factors of food insecurity among a cohort of older australians. J. Nutr. Health Aging 2014, 18, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Kleve, S.; Davidson, Z.; Gearon, E.; Booth, S.; Palermo, C. Are low-to-middle-income households experiencing food insecurity in victoria, australia? An examination of the victorian population health survey, 2006–2009. Aust. J. Prim. Health 2017, 23, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Marques, E.S.; Reichenheim, M.E.; de Moraes, C.L.; Antunes, M.M.L.; Salles-Costa, R. Household food insecurity: A systematic review of the measuring instruments used in epidemiological studies. Public Health Nutr. 2015, 18, 877–892. [Google Scholar] [CrossRef] [PubMed]
- McKechnie, R.; Turrell, G.; Giskes, K.; Gallegos, D. Single-item measure of food insecurity used in the national health survey may underestimate prevalence in australia. Aust. N. Z. J. Public Health 2018, 42, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Butcher, L.M.; O’Sullivan, T.A.; Ryan, M.M.; Lo, J.; Devine, A. Utilising a multi-item questionnaire to assess household food security in australia. Health Promot. J. Aust. 2018. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. Socio-Economic Indexes for Areas (Seifa) 2011; Australian Bureau of Statistics: Canberra, Australia, 2013.
- Hayes, A.J.; Kortt, M.A.; Clarke, P.M.; Brandrup, J.D. Estimating equations to correct self-reported height and weight: Implications for prevalence of overweight and obesity in australia. Aust. N. Z. J. Public Health 2008, 32, 542–545. [Google Scholar] [CrossRef] [PubMed]
- Andrews, G.; Slade, T. Interpreting scores on the kessler psychological distress scale (k10). Aust. N. Z. J. Public Health 2001, 25, 494–497. [Google Scholar] [CrossRef] [PubMed]
- Gill, T.K.; Price, K.; Dal Grande, E.; Daly, A.; Taylor, A.W. Feeling angry about current health status: Using a population survey to determine the association with demographic, health and social factors. BMC Public Health 2016, 16, 588. [Google Scholar] [CrossRef] [PubMed]
- Burnham, K.P.; Anderson, D.R. Multimodel inference-understanding aic and bic in model selection. Sociol. Methods Res. 2004, 33, 261–304. [Google Scholar] [CrossRef]
- Raftery, A.E. Bayesian model selection in social research. Sociol. Methodol. 1995, 25, 111–163. [Google Scholar] [CrossRef]
- Little, R.J.; Rubin, D.B. Causal effects in clinical and epidemiological studies via potential outcomes: Concepts and analytical approaches. Annu. Rev. Public Health 2000, 21, 121–145. [Google Scholar] [CrossRef] [PubMed]
- StataCorp. Stata Statistical Software: Release 13; StataCorp LP: College Station, TX, USA, 2013. [Google Scholar]
- Ramsey, R.; Giskes, K.; Turrell, G.; Gallegos, D. Food insecurity among adults residing in disadvantaged urban areas: Potential health and dietary consequences. Public Health Nutr. 2012, 15, 227–237. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. 4727.0.55.005-Australian Aboriginal and Torres Strait Islander Health Survey: Nutrition Results-Food and Nutrients, 2012-13; Australian Bureau of Statistics: Canberra, Australia, 2015.
- Mackenbach, J.D.; Brage, S.; Forouhi, N.G.; Griffin, S.J.; Wareham, N.J.; Monsivais, P. Does the importance of dietary costs for fruit and vegetable intake vary by socioeconomic position? Br. J. Nutr. 2015, 114, 1464–1470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, S.; Moffitt, A.; Bellamy, J.; Carter, S.; McDowell, C.; Mollenhauer, J. When there not enough to eat: A national study of food insecurity among emergency relief clients. State Family Report 2012, 2, 137–161. [Google Scholar] [CrossRef]
- Landrigan, T.J.; Kerr, D.A.; Dhaliwal, S.S.; Savage, V.; Pollard, C.M. Removing the australian tax exemption on healthy food adds food stress to families vulnerable to poor nutrition. Aust. N. Z. J. Public Health 2017, 41, 591–597. [Google Scholar] [CrossRef] [PubMed]
- Lofters, A.; Slater, M.; Kirst, M.; Shankardass, K.; Quinonez, C. How do people attribute income-related inequalities in health? A cross-sectional study in ontario, canada. PLoS ONE 2014, 9, e85286. [Google Scholar] [CrossRef] [PubMed]
- Bocquier, A.; Vieux, F.; Lioret, S.; Dubuisson, C.; Caillavet, F.; Darmon, N. Socio-economic characteristics, living conditions and diet quality are associated with food insecurity in france. Public Health Nutr. 2015, 18, 2952–2961. [Google Scholar] [CrossRef] [PubMed]
- Stuff, J.E.; Casey, P.H.; Szeto, K.L.; Gossett, J.M.; Robbins, J.M.; Simpson, P.M.; Connell, C.; Bogle, M.L. Household food insecurity is associated with adult health status. J. Nutr. 2004, 134, 2330–2335. [Google Scholar] [CrossRef] [PubMed]
- Macintyre, S. Deprivation amplification revisited; or, is it always true that poorer places have poorer access to resources for healthy diets and physical activity? Int. J. Behav. Nutr. Phys. Activ. 2007, 4, 32. [Google Scholar] [CrossRef] [Green Version]
- Rosenbaum, P.R.; Rubin, D.B. The central role of the propensity score in observational studies for causal effects. Biometrika 1983, 70, 41–55. [Google Scholar] [CrossRef] [Green Version]
- Habicht, J.P.; Victora, C.G.; Vaughan, J.P. Evaluation designs for adequacy, plausibility and probability of public health programme performance and impact. Int. J. Epidemiol. 1999, 28, 10–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daly, A.; Pollard, C.M.; Kerr, D.A.; Binns, C.W.; Phillips, M. Using short dietary questions to develop indicators of dietary behaviour for use in surveys exploring attitudinal and/or behavioural aspects of dietary choices. Nutrients 2015, 7, 6330–6345. [Google Scholar] [CrossRef] [PubMed]
- Caraher, M.; Furey, S. The Economics of Emergency Food Aid Provision: A Financial, Social and Cultural Perspective; Palgrave Macmillan: Basingstoke, UK, 2018. [Google Scholar]
- Steiner, J.F.; Stenmark, S.H.; Sterrett, A.T.; Paolino, A.R.; Stiefel, M.; Gozansky, W.S.; Zeng, C. Food insecurity in older adults in an integrated health care system. J. Am. Geriat. Soc. 2018, 66, 1017–1024. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, M.L.; Cafer, A. Understanding high incidence of severe obesity and very low food security in food pantry clients: Implications for social work. Soc. Work Public Health 2018, 33, 125–139. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Demographic Variables | Unwght % | Wght % | 95% CI | p |
|---|---|---|---|---|
| 18–24 | 7.8 | 8.0 | [6.5, 9.9] | |
| 25–34 | 5.1 | 4.9 | [3.8, 6.2] | |
| 35–44 | 3.6 | 3.2 | [2.6, 4.0] | |
| 45–54 | 2.8 | 2.4 | [1.9, 2.9] | |
| 55–64 | 2.0 | 1.6 | [1.3, 2.0] | <0.0001 |
| Tertiary education | 1.4 | 1.9 | [1.3, 2.6] | |
| Less than tertiary education | 3.8 | 4.7 | [4.1, 5.3] | <0.0001 |
| Employed | 2.2 | 2.9 | [2.5, 3.4] | |
| Unemployed | 11.4 | 12.6 | [9.0, 17.7] | |
| Home duties | 4.3 | 5.2 | [4.0, 6.7] | |
| Retired | 2.3 | 2.0 | [1.3, 3.0] | |
| Student | 7.5 | 7.1 | [4.8, 10.3] | |
| Unable to work | 17.3 | 17.6 | [13.2, 23.0] | <0.0001 |
| Annual household income: over AUD $40,000 | 1.7 | 2.4 | [2.0, 2.9] | |
| Annual household income: AUD $20,001–$40,000 | 7.0 | 9.6 | [7.6, 12.2] | |
| Annual household income: up to AUD $20,000 | 15.0 | 17.8 | [14.2, 22.2] | <0.0001 |
| Spend left over money or save some per pay | 1.1 | 1.7 | [1.4, 2.0] | |
| Just enough money to get by per pay | 10.6 | 12.5 | [10.7, 14.5] | |
| Not enough money to get by per pay | 17.5 | 19.0 | [15.1, 23.6] | <0.0001 |
| Not aboriginal | 3.1 | 3.8 | [3.4, 4.2] | |
| Aboriginal | 12.5 | 15.0 | [9.8, 22.1] | <0.0001 |
| Adults living with others | 2.8 | 3.7 | [3.3, 4.2] | |
| Adults living alone | 6.0 | 6.4 | [5.2, 7.8] | <0.0001 |
| Born outside Australia | 2.8 | 2.9 | [2.3, 3.7] | |
| Born in Australia | 3.5 | 4.4 | [3.9, 5.0] | 0.002 |
| Rents or pays mortgage | 4.1 | 4.6 | [4.3, 5.0] | |
| No mortgage or Government subsidized housing | 2.5 | 3.1 | [2.7, 3.4] | 0.0003 |
| SEIFA b Quintile 5 (least disadvantaged area) | 2.4 | 2.9 | [2.3, 3.6] | |
| SEIFA Quintiles 3,4 (less disadvantaged areas) | 3.4 | 4.5 | [3.9, 5.3] | |
| SEIFA Quintiles 1,2 (most disadvantages areas) | 4.0 | 5.2 | [4.2, 6.4] | <0.0001 |
| Has a health care card | 10.3 | 11.3 | [9.7, 13.2] | <0.0001 |
| Doesn’t have private health insurance | 7.0 | 8.3 | [7.2, 9.6] | <0.0001 |
| Has asthma | 5.7 | 6.3 | [4.7, 8.4] | 0.0011 |
| Some cardiovascular condition | 5.8 | 7.4 | [4.9, 11.0] | 0.0022 |
| Has cancer | 4.5 | 7.0 | [4.3, 11.3] | 0.0167 |
| Current mental health (depression/anxiety/other) | 9.1 | 9.7 | [8.3, 11.4] | <0.0001 |
| Health rated as fair/poor | 8.8 | 8.9 | [7.2, 11.0] | <0.0001 |
| Always or often feel a lack of control over health | 12.8 | 13.9 | [11.0, 17.3] | <0.0001 |
| Health rated worse than 12 months ago | 7.3 | 9.4 | [7.6, 11.6] | <0.0001 |
| High/very high Kessler 10 score | 14.1 | 14.8 | [12.4, 17.6] | <0.0001 |
| BMI 30 or more (in obese range) | 4.3 | 5.2 | [4.4, 6.1] | <0.0012 |
| Currently smoking | 7.1 | 8.5 | [7.0, 10.3] | <0.0001 |
| Does no leisure time physical activity | 4.4 | 5.5 | [4.0, 7.5] | 0.0447 |
| Spends four or more hours sitting in leisure time | 6.4 | 7.6 | [5.8, 9.8] | <0.0001 |
| Eats ‘fast food’ c three or more times a week | 9.1 | 11.9 | [8.3, 17.0] | <0.0001 |
| Uses full fat milk | 4.6 | 5.7 | [4.9, 6.7] | <0.0001 |
| Doesn’t eat any fruit | 6.3 | 6.4 | [4.5, 9.1] | |
| Eats less than two serves of fruit daily | 3.4 | 4.2 | [3.6, 4.9] | |
| Eats two or more serves of fruit daily | 2.7 | 3.3 | [2.8, 4.0] | 0.0030 |
| Doesn’t eat any vegetables | 15.0 | 14.9 | [6.5, 30.4] | |
| Eats less than five serves daily | 3.3 | 4.0 | [3.6, 4.5] | |
| Eats five or more serves daily | 2.3 | 2.6 | [1.7, 3.9] | <0.0012 |
| Main Effects | Odd Ratio (95% CI) | p |
|---|---|---|
| 35 over | Ref | |
| 18–34 years | 5.29 (3.65, 7.65) | 0.000 |
| Has tertiary education | Ref | |
| Does not have tertiary education | 1.87 (1.38, 2.54) | 0.000 |
| Not Aboriginal | Ref | |
| Aboriginal | 2.07 (1.34, 3.2) | 0.001 |
| Household income over $40,000 | Ref | |
| Household income $20,000 to $40,000 | 1.65 (1.29, 2.1) | 0.000 |
| Household income under $20,000 | 5.28 (3.91, 7.13) | 0.000 |
| Can save a bit of money | Ref | |
| Just enough money to get by | 1.08 (0.69, 1.71) | 0.730 |
| Not enough money to get by | 3.11 (2.17, 4.46) | 0.000 |
| Has private health insurance | Ref | |
| Has no private health insurance | 1.80 (1.46, 2.22) | 0.000 |
| Does not have doctor diagnosed mental health problem | Ref | |
| Has a doctor diagnosed mental health problem | 2.56 (1.96, 3.35) | 0.000 |
| Low or moderate Kessler 10 score | Ref | |
| High or very high Kessler 10 score | 1.65 (1.31, 2.06) | 0.000 |
| Health same or better than same time previous year | Ref | |
| Health worse or much worse than same time previous year | 1.70 (1.37, 2.09) | 0.000 |
| Does not smoke | Ref | |
| Smokes | 1.58 (1.29, 1.93) | 0.000 |
| Is not in Body Mass Index obese range | Ref | |
| Is in Body Mass Index obese range | 1.44 (1.18, 1.76) | 0.000 |
| Eats some vegetables daily | Ref | |
| Eats no vegetables daily | 2.40 (1.34, 4.3) | 0.003 |
| Eats fast foods less than three times a week | Ref | |
| Eats fast foods three or more times a week | 1.83 (1.11, 3.01) | 0.018 |
| Interaction terms | ||
| Has just enough money to get by # age 18–24 years | 0.56 (0.35, 0.91) | 0.019 |
| Has a mental health problem # age 18–24 years | 0.52 (0.31, 0.86) | 0.010 |
| Housing whether or not owned or rented # Not enough or just enough money to get by | 3.35 (2.41, 4.65) | 0.000 |
| Household income under $20,000 # Not enough or just enough money to get by | 3.05 (1.94, 4.80) | 0.000 |
| Outcome: ‘Running out of Food’ at Least Once in the Previous Twelve Months | Coef. | 95% | CI | Robust Std. Err | Z | p |
|---|---|---|---|---|---|---|
| Annual household income | ||||||
| Average effect when income <$20,000 | 0.038 | 0.013 | 0.063 | 0.013 | 3.02 | 0.003 |
| Probability if income is >$20,000 | 0.028 | 0.025 | 0.03 | 0.001 | 19.33 | <0.001 |
| Discretional income | ||||||
| Difference between spend left over vs. able to save | 0.023 | 0.014 | 0.033 | 0.005 | 4.85 | <0.001 |
| Difference between just enough vs. able to save | 0.056 | 0.046 | 0.067 | 0.005 | 10.48 | <0.001 |
| Difference between not enough vs. able to save | 0.066 | 0.048 | 0.083 | 0.009 | 7.38 | <0.001 |
| Average probability of outcome for those able to save | 0.012 | 0.009 | 0.014 | 0.001 | 9.05 | <0.001 |
| Obesity | ||||||
| Difference in probability when obese | 0.008 | 0.003 | 0.013 | 0.003 | 3.15 | 0.002 |
| Average probability of outcome if not obese | 0.029 | 0.026 | 0.032 | 0.002 | 17.88 | <0.001 |
| Outcome: | Coef. | 95% | CI | Robust Std. Err | Z | p |
|---|---|---|---|---|---|---|
| Eats fast food more than three times a week | ||||||
| Difference in probability of ‘running out of food’ vs. not | −0.007 | −0.013 | −0.0002 | 0.003 | −2.03 | 0.042 |
| Average probability of outcome when didn’t run out | 0.019 | <0.001 | 0.017 | 0.001 | 17.83 | <0.001 |
| Eats no vegetables | ||||||
| Difference in probability of fast food >2 times weekly | 0.029 | 0.007 | 0.051 | 0.011 | 2.61 | 0.009 |
| Average probability of FI when fast food <3 times weekly | 0.006 | 0.005 | 0.007 | 0.001 | 10.32 | <0.001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Daly, A.; Pollard, C.M.; Kerr, D.A.; Binns, C.W.; Caraher, M.; Phillips, M. Using Cross-Sectional Data to Identify and Quantify the Relative Importance of Factors Associated with and Leading to Food Insecurity. Int. J. Environ. Res. Public Health 2018, 15, 2620. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15122620
Daly A, Pollard CM, Kerr DA, Binns CW, Caraher M, Phillips M. Using Cross-Sectional Data to Identify and Quantify the Relative Importance of Factors Associated with and Leading to Food Insecurity. International Journal of Environmental Research and Public Health. 2018; 15(12):2620. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15122620
Chicago/Turabian StyleDaly, Alison, Christina M. Pollard, Deborah A. Kerr, Colin W. Binns, Martin Caraher, and Michael Phillips. 2018. "Using Cross-Sectional Data to Identify and Quantify the Relative Importance of Factors Associated with and Leading to Food Insecurity" International Journal of Environmental Research and Public Health 15, no. 12: 2620. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15122620