Relationship between Daytime Sleepiness and Health Utility in Patients after Cardiac Surgery: A Preliminary Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. ESS as an Index of Daytime Sleepiness
2.2. SF-6D as an Index of Health Utility
2.3. Statistical Analysis
3. Results
3.1. Clinical Characteristics of the Patients
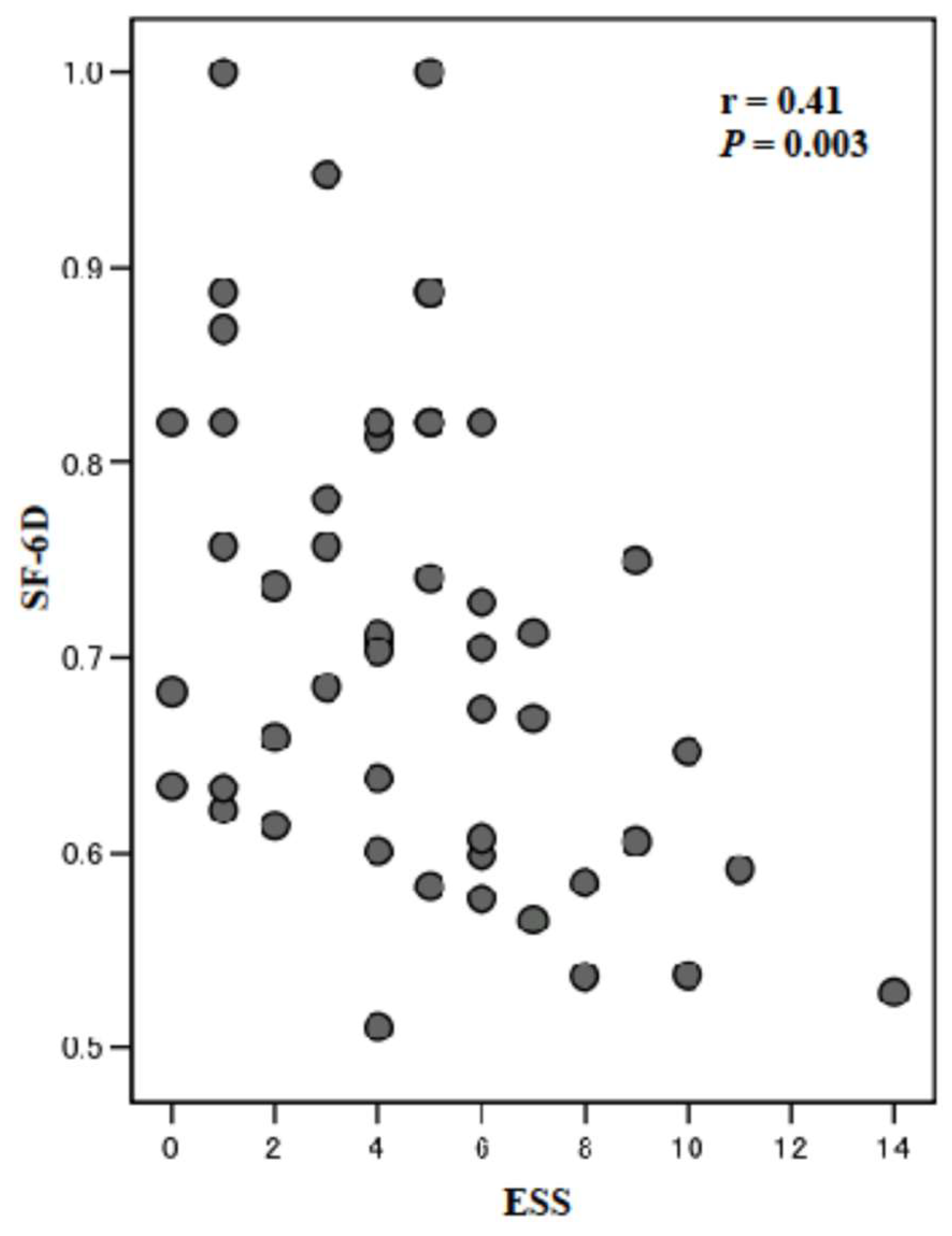
3.2. Sleep Quality and Health Utility at 5 Months after Cardiac Surgery
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Yilmaz, H.; Iskesen, I. Follow-up with objective and subjective tests of the sleep characteristics of patients after cardiac surgery. Circ. J. 2007, 71, 1506–1510. [Google Scholar] [CrossRef] [PubMed]
- Iskesen, I.; Kurdal, A.T.; Yilmaz, H.; Cerrahoglu, M.; Sirin, B.H. Sleep disturbances after cardiac surgery with or without elevated S100B levels. Acta Cardiol. 2009, 64, 741–746. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, H.; Iskesen, I. Objective and subjective characteristics of sleep after coronary artery bypass graft surgery in the early period: A prospective study with healthy subjects. Heart Surg. Forum 2007, 10, E16–E20. [Google Scholar] [CrossRef] [PubMed]
- Aksu, N.T.; Erdogan, A.; Ozgur, N. Effects of progressive muscle relaxation training on sleep and quality of life in patients with pulmonary resection. Sleep Breath 2017. [Google Scholar] [CrossRef] [PubMed]
- Redeker, N.S.; Hedges, C. Sleep during hospitalization and recovery after cardiac surgery. J. Cardiovasc. Nurs. 2002, 17, 56–68. [Google Scholar] [CrossRef] [PubMed]
- Ng, A.C.; Freedman, S.B. Sleep disordered breathing in chronic heart failure. Heart Fail. Rev. 2009, 14, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Johns, M.W. A new method for measuring daytime sleepiness: The Epworth sleepiness scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef]
- American Academy of Sleep Medicine Task Force. Sleep-related breathing disorders in adults: Recommendations for syndrome definition and measurement techniques in clinical research. Sleep 1999, 22, 667–689. [Google Scholar] [CrossRef]
- Jean-Louis, G.; Kripke, D.F.; Ancoli-Israel, S. Sleep and quality of well-being. Sleep 2000, 23, 1115–1121. [Google Scholar]
- Lopes, C.; Esteves, A.M.; Bittencourt, L.R.; Tufik, S.; Mello, M.T. Relationship between the quality of life and the severity of obstructive sleep apnea syndrome. Braz. J. Med. Biol. Res. 2008, 41, 908–913. [Google Scholar] [CrossRef] [Green Version]
- Izawa, K.P.; Watanabe, S.; Oka, K.; Hiraki, K.; Morio, Y.; Kasahara, Y.; Takeichi, N.; Tsukamoto, T.; Osada, N.; Omiya, K.; et al. Relation between sleep quality and physical activity in chronic heart failure patients. Recent Pat. Cardiovasc. Drug Discov. 2011, 6, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Hirano, Y.; Izawa, K.; Watanabe, S.; Yamada, S.; Oka, K.; Kasahara, Y.; Omiya, K. Physiological and health-related quality of life outcomes following cardiac rehabilitation after cardiac surgery. J. Jpn. Phys. Ther. Assoc. 2005, 8, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Hirschhorn, A.D.; Richards, D.A.; Mungovan, S.F.; Morris, N.R.; Adams, L. Does the mode of exercise influence recovery of functional capacity in the early postoperative period after coronary artery bypass graft surgery? A randomized controlled trial. Interact. Cardiovasc. Thorac. Surg. 2012, 15, 995–1003. [Google Scholar] [CrossRef] [PubMed]
- Anderson, L.; Thompson, D.R.; Oldridge, N.; Zwisler, A.D.; Rees, K.; Martin, N.; Taylor, R.S. Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst. Rev. 2016, D001800. [Google Scholar] [CrossRef]
- Izawa, K.; Hirano, Y.; Yamada, S.; Oka, K.; Omiya, K.; Iijima, S. Improvement in physiological outcomes and health-related quality of life following cardiac rehabilitation in patients with acute myocardial infarction. Circ. J. 2004, 68, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Hautala, A.J.; Kiviniemi, A.M.; Mäkikallio, T.; Koistinen, P.; Ryynänen, O.P.; Martikainen, J.A.; Seppänen, T.; Huikuri, H.V.; Tulppo, M.P. Economic evaluation of exercise-based cardiac rehabilitation in patients with a recent acute coronary syndrome. Scand. J. Med. Sci. Sports 2016. [Google Scholar] [CrossRef] [PubMed]
- Brazier, J.; Usherwood, T.; Harper, R.; Thomas, K. Deriving a preference-based single index from the UK SF-36 Health Survey. J. Clin. Epidemiol. 1998, 51, 1115–1128. [Google Scholar] [CrossRef]
- van Stel, H.F.; Buskens, E. Comparison of the SF-6D and the EQ-5D in patients with coronary heart disease. Health Qual. Life Outcomes 2006, 4, 20. [Google Scholar] [CrossRef]
- Brazier, J.; Roberts, J.; Deverill, M. The estimation of a preference-based measure of health from the SF-36. J. Health Econ. 2002, 21, 271–292. [Google Scholar] [CrossRef] [Green Version]
- Brazier, J.E.; Fukuhara, S.; Roberts, J.; Kharroubi, S.; Yamamoto, Y.; Ikeda, S.; Doherty, J.; Kurokawa, K. Estimating a preference-based index from the Japanese SF-36. J. Clin. Epidemiol. 2009, 62, 1323–1331. [Google Scholar] [CrossRef] [Green Version]
- Izawa, K.P.; Kasahara, Y.; Hiraki, K.; Hirano, Y.; Watanabe, S. Changes in health utility of patients after cardiac surgery. J. Yoga Phys. Ther. 2017, 7, 4. [Google Scholar]
- Takegami, M.; Sokejima, S.; Yamazaki, S.; Nakayama, T.; Fukuhara, S. An estimation of the prevalence of excessive daytime sleepiness based on age and sex distribution of epworth sleepiness scale scores: A population based survey. Nippon Koshu Eisei Zasshi 2005, 52, 137–145. (In Japanese) [Google Scholar] [PubMed]
- Takegami, M.; Suzukamo, Y.; Wakita, T.; Noguchi, H.; Chin, K.; Kadotani, H.; Inoue, Y.; Oka, Y.; Nakamura, T.; Green, J.; et al. Development of a Japanese version of the Epworth Sleepiness Scale (JESS) based on item response theory. Sleep Med. 2009, 10, 556–565. [Google Scholar] [CrossRef] [PubMed]
- Neumann, A.; Schoffer, O.; Norström, F.; Norberg, M.; Klug, S.J.; Lindholm, L. Health-related quality of life for pre-diabetic states and type 2 diabetes mellitus: A cross-sectional study in Västerbotten Sweden. Health Qual. Life Outcomes 2014, 12, 150. [Google Scholar] [CrossRef] [PubMed]
- Quercioli, C.; Messina, G.; Barbini, E.; Carriero, G.; Fanì, M.; Nante, N. Importance of sociodemographic and morbidity aspects in measuring health-related quality of life: Performances of three tools: Comparison of three questionnaire scores. Eur. J. Health Econ. 2009, 10, 389–397. [Google Scholar] [CrossRef] [PubMed]
- Pressler, A.; Christle, J.W.; Lechner, B.; Grabs, V.; Haller, B.; Hettich, I.; Jochheim, D.; Mehilli, J.; Lange, R.; Bleiziffer, S.; et al. Exercise training improves exercise capacity and quality of life after transcatheter aortic valve implantation: A randomized pilot trial. Am. Heart J. 2016, 182, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Lavie, C.J.; Milani, R.V. Effects of cardiac rehabilitation programs on exercise capacity, coronary risk factors, behavioral characteristics, and quality of life in a large elderly cohort. Am. J. Cardiol. 1995, 76, 177–179. [Google Scholar] [CrossRef]
- Pollmann, A.G.E.; Frederiksen, M.; Prescott, E. Cardiac Rehabilitation after Heart Valve Surgery: Improvement in Exercise Capacity and Morbidity. J. Cardiopulm. Rehabil. Prev. 2017, 37, 191–198. [Google Scholar] [CrossRef]
- Goel, K.; Pack, Q.R.; Lahr, B.; Greason, K.L.; Lopez-Jimenez, F.; Squires, R.W.; Zhang, Z.; Thomas, R.J. Cardiac rehabilitation is associated with reduced long-term mortality in patients undergoing combined heart valve and CABG surgery. Eur. J. Prev. Cardiol. 2015, 22, 159–168. [Google Scholar] [CrossRef]
- Dehbarez, N.T.; Lynggaard, V.; May, O.; Søgaard, R. Learning and coping strategies versus standard education in cardiac rehabilitation: A cost-utility analysis alongside a randomised controlled trial. BMC Health Serv. Res. 2015, 15, 422. [Google Scholar] [CrossRef]
- Campbell, M.J. Statistics at Square Two, 2nd ed.; BMJ Books: London, UK, 2006. [Google Scholar]
- Schaefer, K.M.; Swavely, D.; Rothenberger, C.; Hess, S.; Williston, D. Sleep disturbances post coronary artery bypass surgery. Prog. Cardiovasc. Nurs. 1996, 11, 5–14. [Google Scholar] [PubMed]
- Tack, B.B.; Gilliss, C.L. Nurse-monitored cardiac recovery: A description of the first 8 weeks. Heart Lung 1990, 19 Pt 1, 491–499. [Google Scholar]
- King, K.B.; Parrinello, K.A. Patient perceptions of recovery from coronary artery bypass grafting after discharge from the hospital. Heart Lung 1988, 17 Pt 1, 708–715. [Google Scholar]
- Magni, G.; Unger, H.P.; Valfrè, C.; Polesel, E.; Cesari, F.; Rizzardo, R.; Paruzzolo, P.; Gallucci, V. Psychosocial outcome one year after heart surgery. A prospective study. Arch. Intern. Med. 1987, 147, 473–477. [Google Scholar] [CrossRef] [PubMed]
- Lukkarinen, H. Quality of life in coronary artery disease. Nurs. Res. 1998, 47, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Uchôa, C.H.G.; Danzi-Soares, N.J.; Nunes, F.S.; de Souza, A.A.L.; Nerbass, F.B.; Pedrosa, R.P.; César, L.A.M.; Lorenzi-Filho, G.; Drager, L.F. Impact of OSA on cardiovascular events after coronary artery bypass surgery. Chest 2015, 147, 1352–1360. [Google Scholar] [CrossRef]
- Darchia, N.; Oniani, N.; Sakhelashvili, I.; Supatashvili, M.; Basishvili, T.; Eliozishvili, M.; Maisuradze, L.; Cervena, K. Relationship between Sleep Disorders and Health Related Quality of Life-Results from the Georgia SOMNUS Study. Int. J. Environ. Res. Public Health 2018, 15, 1588. [Google Scholar] [CrossRef]


{kind=link}
| Clinical Characteristics | Middle-Aged Group | Older-Aged Group | t or χ2 Value * | p Value |
|---|---|---|---|---|
| No. of patients | 29 | 22 | ||
| Age (yrs) | 56.3 ± 7.1 | 70.9 ± 3.6 | −8.61 | <0.001 |
| Sex (male) | 23 | 18 | 0.02 * | 0.58 |
| BMI (kg/m2) | 23.4 ± 2.4 | 22.7 ± 3.0 | 0.88 | 0.38 |
| LVEF (%) | 52.8 ± 11.0 | 57.3 ± 12.1 | −1.04 | 0.31 |
| Etiology (%) | ||||
| CABG | 62.1 | 71.4 | 0.47 * | 0.35 |
| VR/VP | 37.9 | 28.6 | - | - |
| Medications (%) | ||||
| Beta-blockers | 43.7 | 45.5 | 0.00 * | 0.61 |
| ACEI/ARB | 31.2 | 54.5 | 1.46 * | 0.20 |
| Diuretic | 62.5 | 81.8 | 2.73 * | 0.11 |
| Middle-Aged Group | Older-Aged Group | t Value | p Value | |
|---|---|---|---|---|
| ESS | 5.14 ± 2.96 | 4.05 ± 3.23 | 1.24 | 0.22 |
| SF-6D | 0.72 ± 0.14 | 0.71 ± 0.10 | 0.31 | 0.76 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Izawa, K.P.; Kasahara, Y.; Hiraki, K.; Hirano, Y.; Oka, K.; Watanabe, S. Relationship between Daytime Sleepiness and Health Utility in Patients after Cardiac Surgery: A Preliminary Study. Int. J. Environ. Res. Public Health 2018, 15, 2716. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15122716
Izawa KP, Kasahara Y, Hiraki K, Hirano Y, Oka K, Watanabe S. Relationship between Daytime Sleepiness and Health Utility in Patients after Cardiac Surgery: A Preliminary Study. International Journal of Environmental Research and Public Health. 2018; 15(12):2716. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15122716
Chicago/Turabian StyleIzawa, Kazuhiro P., Yusuke Kasahara, Koji Hiraki, Yasuyuki Hirano, Koichiro Oka, and Satoshi Watanabe. 2018. "Relationship between Daytime Sleepiness and Health Utility in Patients after Cardiac Surgery: A Preliminary Study" International Journal of Environmental Research and Public Health 15, no. 12: 2716. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15122716