Airflow as a Possible Transmission Route of Middle East Respiratory Syndrome at an Initial Outbreak Hospital in Korea


Abstract
:1. Introduction
2. Materials and Methods
2.1. Epidemiological Investigation of the Hospital
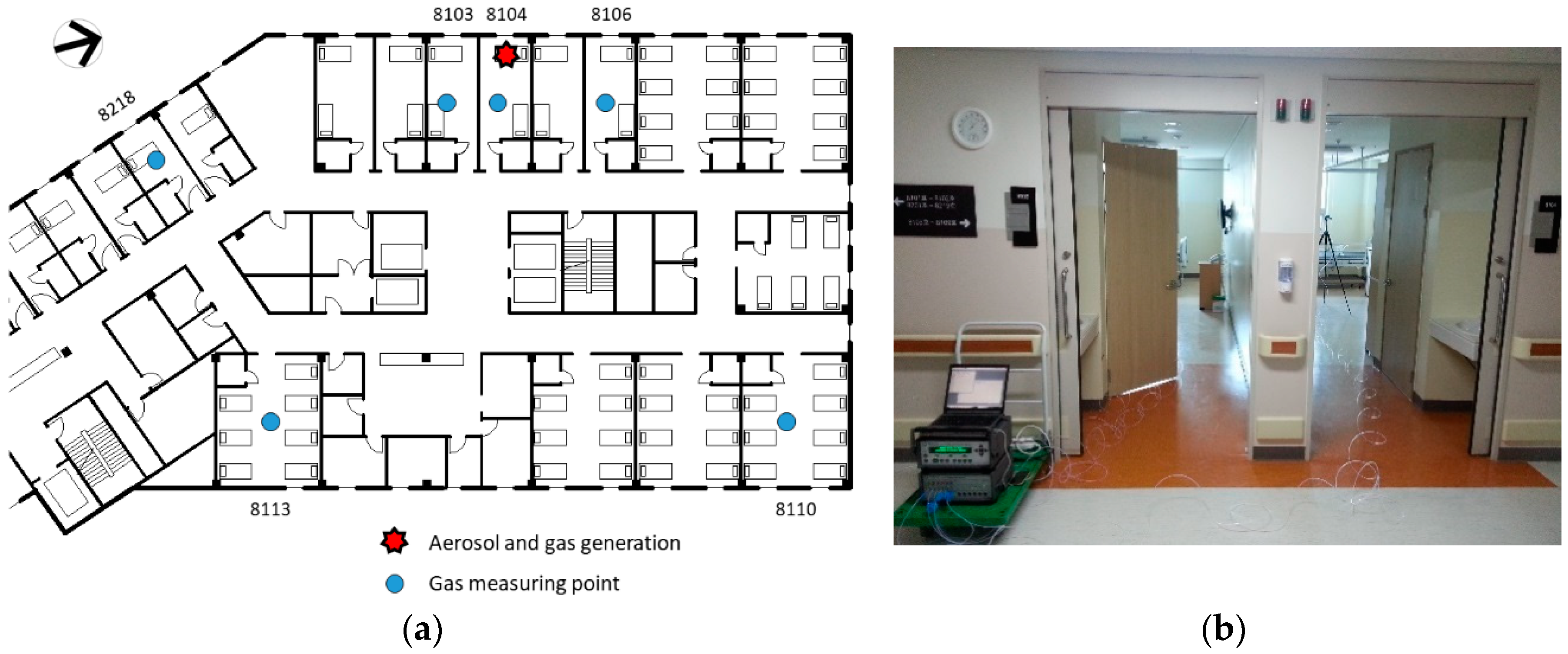
2.2. Tracer Experiments
3. Results
3.1. Epidemiological Investigation
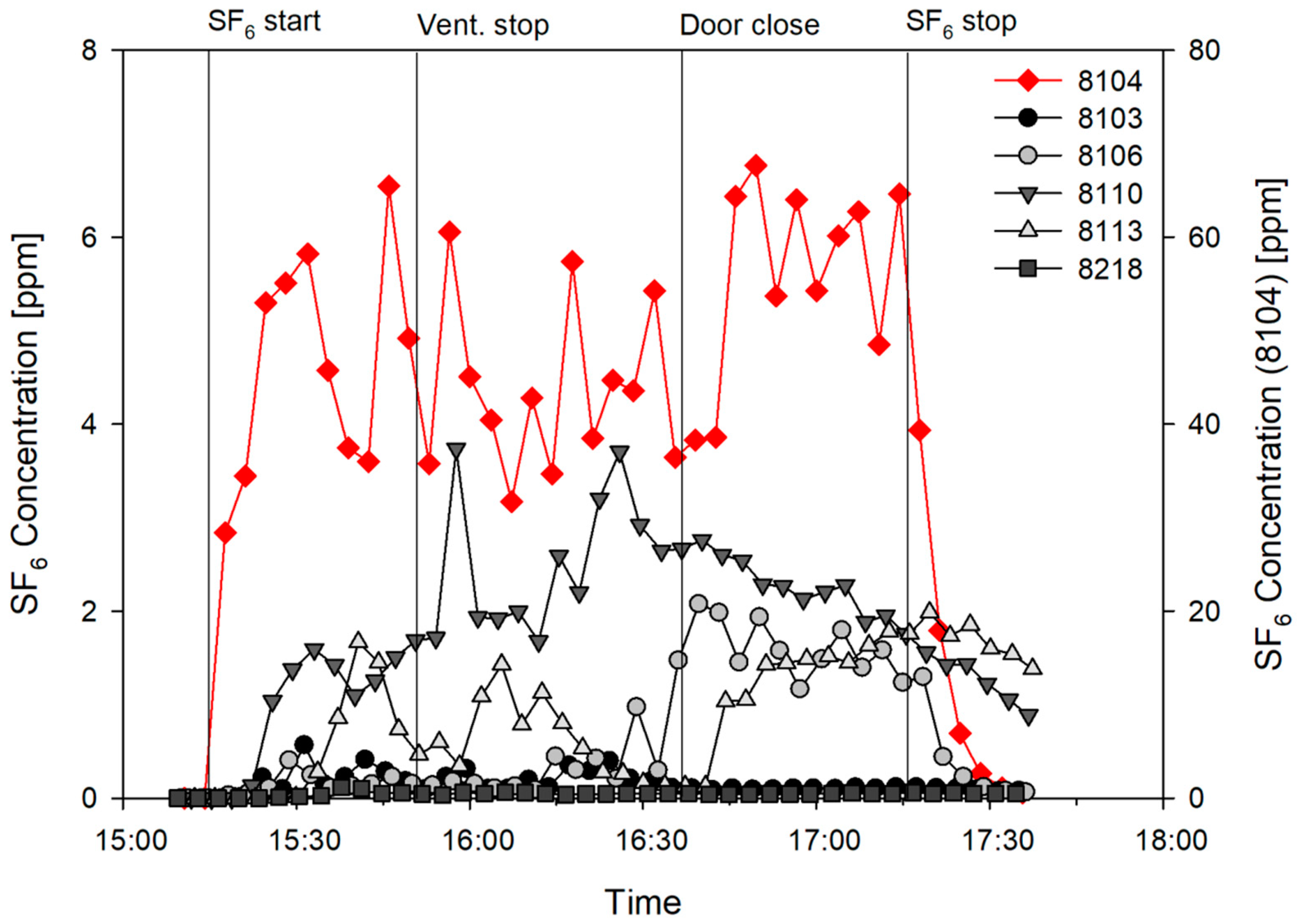
3.2. Tracer Experiments
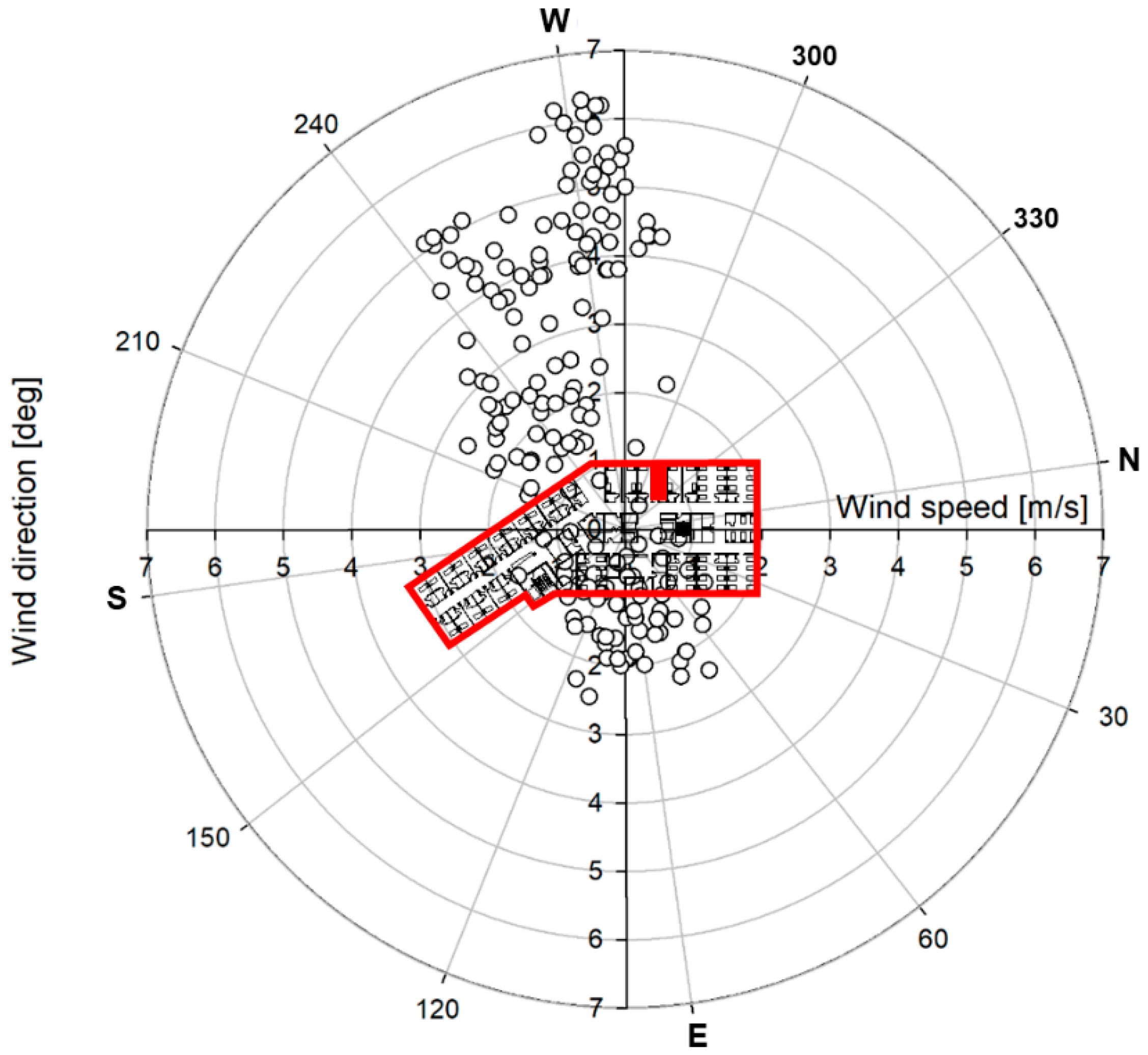
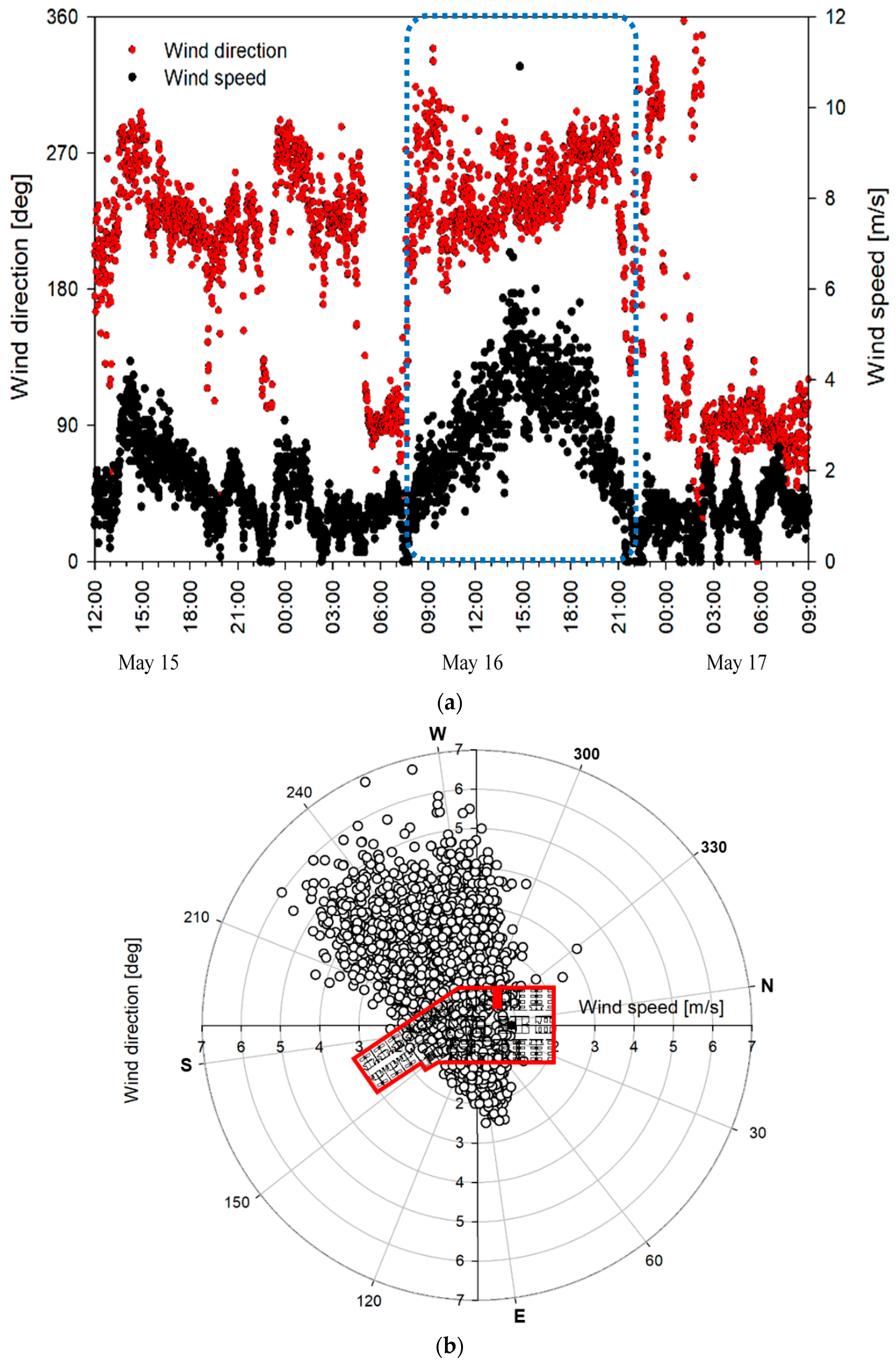
3.3. Airflow
4. Discussion
5. Conclusions
- The tracer gas from room 8104, in which the initial patient (super-spreader) was hospitalized, was confirmed to spread over long distances to patient rooms across the corridor. This indicates the significant effect of the outdoor wind entering through the window.
- The high concentration in room 8104 was probably spread to the corridor and rooms on the opposite side due to the strong airflow entering from the outside.
- The results indicate that cross ventilation by outdoor wind in central corridor inpatient ward could cause dispersion of infectious aerosols to indoor through airflow.
- Although there were limitations in confirming the infectivity of propagated airborne particles, the possibility of the spread of infections by airflow was presented for the analysis of relatively long-distance infection cases, for which the close-contact infection route by droplets could not be identified.
Author Contributions
Funding
Conflicts of Interest
References
- Park, H.Y.; Lee, E.J.; Ryu, Y.W.; Kim, Y.; Kim, H.; Lee, H.; Yi, S.J. Epidemiological investigation of MERS-CoV spread in a single hospital in South Korea, May to June 2015. Eurosurveillance 2015, 20, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Korea Center for Disease Control and Prevention. 2015 MERS White Paper; Korea Center for Disease Control and Prevention: Cheongju, Korea, 2016.
- Oh, M. The Korean Middle East respiratory syndrome coronavirus outbreak and our responsibility to the global scientific community. Infect. Chemother. 2016, 48, 145–146. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.-S.; Pebody, R.; Charlett, A.; de Angelis, D.; Birrell, P.; Kang, H.; Baguelin, M.; Choi, Y.H. Estimating and modelling the transmissibility of Middle East Respiratory Syndrome CoronaVirus during the 2015 outbreak in the Republic of Korea. Influenza Other Respir. Viruses 2017, 11, 434–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, J.Y. An Outbreak of Middle East Respiratory Syndrome Coronavirus Infection in South Korea. Yonsei Med. J. 2015, 56, 1174. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.-S.; Lee, C.; Kim, K.M.; Kim, S.W.; Lee, K.-J.; Ahn, J.; Ki, M. The first case of the 2015 Korean Middle East Respiratory Syndrome outbreak. Epidemiol. Health 2015, 37. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.M.; Ki, M.; Cho, S.; Sung, M.; Hong, J.K.; Cheong, H.-K.; Kim, J.-H.; Lee, S.-E.; Lee, C.; Lee, K.-J.; et al. Epidemiologic features of the first MERS outbreak in Korea: Focus on Pyeongtaek St. Mary’s Hospital. Epidemiol. Health 2015, 37. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.Y.; Kang, J.-M.; Ha, Y.E.; Park, G.E.; Lee, J.Y.; Ko, J.-H.; Lee, J.Y.; Kim, J.M.; Kang, C.-I.; Jo, I.J.; et al. MERS-CoV outbreak following a single patient exposure in an emergency room in South Korea: An epidemiological outbreak study. Lancet 2016, 388, 994–1001. [Google Scholar] [CrossRef]
- Nam, H.-S.; Park, J.W.; Ki, M.; Yeon, M.-Y.; Kim, J.; Kim, S.W. High fatality rates and associated factors in two hospital outbreaks of MERS in Daejeon, the Republic of Korea. Int. J. Infect. Dis. 2017, 58, 37–42. [Google Scholar] [CrossRef]
- Park, J.W.; Lee, K.J.; Lee, K.H.; Lee, S.H.; Cho, J.R.; Mo, J.W.; Choi, S.Y.; Kwon, G.Y.; Shin, J.-Y.; Hong, J.Y.; et al. Hospital Outbreaks of Middle East Respiratory Syndrome, Daejeon, South Korea, 2015. Emerg. Infect. Dis. 2017, 23, 898–905. [Google Scholar] [CrossRef] [Green Version]
- Wong, G.; Liu, W.; Liu, Y.; Zhou, B.; Bi, Y.; Gao, G.F. MERS, SARS, and Ebola: The Role of Super-Spreaders in Infectious Disease. Cell Host Microbe 2015, 18, 398–401. [Google Scholar] [CrossRef]
- Mackay, I.M.; Arden, K.E. MERS coronavirus: Diagnostics, epidemiology and transmission. Virol. J. 2015, 12, 222. [Google Scholar] [CrossRef] [PubMed]
- Xiao, S.; Li, Y.; Sung, M.; Wei, J.; Yang, Z. A study of the probable transmission routes of MERS-CoV during the first hospital outbreak in the Republic of Korea. Indoor Air 2018, 28, 51–63. [Google Scholar] [CrossRef] [PubMed]
- Oh, M.; Park, W.B.; Park, S.-W.; Choe, P.G.; Bang, J.H.; Song, K.-H.; Kim, E.S.; Kim, H.B.; Kim, N.J. Middle East respiratory syndrome: What we learned from the 2015 outbreak in the Republic of Korea. Korean J. Intern. Med. 2018, 33, 233–246. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Cumulative Number of Reported Probable Cases of Severe Acute Respiratory Syndrome (SARS); WHO: Geneva, Switzerland, 2004. [Google Scholar]
- Booth, T.F.; Kournikakis, B.; Bastien, N.; Ho, J.; Kobasa, D.; Stadnyk, L.; Li, Y.; Spence, M.; Paton, S.; Henry, B.; et al. Detection of Airborne Severe Acute Respiratory Syndrome (SARS) Coronavirus and Environmental Contamination in SARS Outbreak Units. J. Infect. Dis. 2005, 191, 1472–1477. [Google Scholar] [CrossRef] [Green Version]
- Yu, I.T.; Li, Y.; Wong, T.W.; Tam, W.; Chan, A.T.; Lee, J.H.; Leung, D.Y.; Ho, T. Evidence of airborne transmission of the severe acute respiratory syndrome virus. N. Engl. J. Med. 2004, 350, 1731–1739. [Google Scholar] [CrossRef] [PubMed]
- Yu, I.T.S.; Wong, T.W.; Chiu, Y.L.; Lee, N.; Li, Y. Temporal-Spatial Analysis of Severe Acute Respiratory Syndrome among Hospital Inpatients. Clin. Infect. Dis. 2005, 40, 1237–1243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qian, H.; Li, Y.; Nielsen, P.V.; Huang, X. Spatial distribution of infection risk of SARS transmission in a hospital ward. Build. Environ. 2009, 44, 1651–1658. [Google Scholar] [CrossRef]
- Lee, C.; Ki, M. Strengthening epidemiologic investigation of infectious diseases in Korea: Lessons from the Middle East Respiratory Syndrome outbreak. Epidemiol. Health 2015, 37. [Google Scholar] [CrossRef]
- Song, Y.; Yang, J.-S.; Cheong, H.-K.; Yoon, H.J.; Nam, H.-S.; Lee, S.Y.; Park, W.; Park, S.; Choi, B.Y.; Kim, S.S.; et al. Asymptomatic infection of Middle East respiratory syndrome coronavirus using serologic survey in Korea. Epidemiol. Health 2018, 40. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Interim Infection Prevention and Control Recommendations for Hospitalized Patients with Middle East Respiratory Syndrome Coronavirus. 2015. Available online: https://www.cdc.gov/coronavirus/mers/infection-prevention-control.html (accessed on 23 November 2018).
- Duguid, J.P. The size and the duration of air-carriage of respiratory droplets and droplet-nuclei. Epidemiol. Infect. 1946, 44, 471–479. [Google Scholar] [CrossRef]
- Xie, X.; Li, Y.; Chwang, A.T.Y.; Ho, P.L.; Seto, W.H. How far droplets can move in indoor environments—Revisiting the Wells evaporation–falling curve. Indoor Air 2007, 17, 211–225. [Google Scholar] [CrossRef] [PubMed]
- Seo, Y.B.; Heo, J.Y.; Song, M.-S.; Lee, J.; Kim, E.-H.; Park, S.-J.; Kwon, H.; mi Kim, S.; Kim, Y.; Si, Y.-J.; Lee, I.-W.; et al. Environmental Contamination and Viral Shedding in MERS Patients during MERS-CoV Outbreak in South Korea. Clin. Infect. Dis. 2015, 62, 755–760. [Google Scholar] [CrossRef]
- Kim, S.-H.; Chang, S.Y.; Sung, M.; Park, J.H.; Bin Kim, H.; Lee, H.; Choi, J.-P.; Choi, W.S.; Min, J.-Y. Extensive Viable Middle East Respiratory Syndrome (MERS) Coronavirus Contamination in Air and Surrounding Environment in MERS Isolation Wards. Clin. Infect. Dis. 2016, 63, 363–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Huang, X.; Yu, I.T.S.; Wong, T.W.; Qian, H. Role of air distribution in SARS transmission during the largest nosocomial outbreak in Hong Kong. Indoor Air 2005, 15, 83–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). Natural Ventilation for Infection Control in Health-Care Settings; WHO Guidelines; WHO: Geneva, Switzerland, 2009. [Google Scholar]
- Hambraeus, A.; Sanderson, H.F. The control by ventilation of airborne bacterial transfer between hospital patients and its assessment by means of a particle tracer. Epidemiol. Infect. 1972, 70, 299–312. [Google Scholar]
- Wiley, A.M.; Ha’Eri, G.B. Routes of Infection: A Study of Using “Tracer Particles” in the Orthopedic Operating Room. Clin. Orthop. Relat. Res. 1979, 139, 150–155. [Google Scholar] [CrossRef]
- Wu, Y.; Tung, T.C.W.; Niu, J. On-site measurement of tracer gas transmission between horizontal adjacent flats in residential building and cross-infection risk assessment. Build. Environ. 2016, 99, 13–21. [Google Scholar] [CrossRef]
- Gilkeson, C.A.; Camargo-Valero, M.A.; Pickin, L.E.; Noakes, C.J. Measurement of ventilation and airborne infection risk in large naturally ventilated hospital wards. Build. Environ. 2013, 65, 35–48. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Room Number | 8104 | 8103 | 8106 | 8110 | 8113 | 8218 |
|---|---|---|---|---|---|---|
| Average | 49.5 | 0.18 | 0.71 | 2.09 | 0.63 | 0.048 |
| (100%) | (0.36%) | (1.43%) | (4.22%) | (1.27%) | (0.10%) | |
| Maximum | 67.7 | 0.56 | 2.07 | 3.74 | 1.67 | 0.12 |
| (137%) | (1.13%) | (4.18%) | (7.56%) | (3.37%) | (0.24%) | |
| Infected case | 5/5 | 1/3 | 0/1 | 2/6 | 1/9 | 0/1 |
| Distance from 8104 | 0 m | 1 m | 6.3 m | 28 m | 24 m | 18 m |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sung, M.; Jo, S.; Lee, S.-E.; Ki, M.; Choi, B.Y.; Hong, J. Airflow as a Possible Transmission Route of Middle East Respiratory Syndrome at an Initial Outbreak Hospital in Korea. Int. J. Environ. Res. Public Health 2018, 15, 2757. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15122757
Sung M, Jo S, Lee S-E, Ki M, Choi BY, Hong J. Airflow as a Possible Transmission Route of Middle East Respiratory Syndrome at an Initial Outbreak Hospital in Korea. International Journal of Environmental Research and Public Health. 2018; 15(12):2757. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15122757
Chicago/Turabian StyleSung, Minki, Seongmin Jo, Sang-Eun Lee, Moran Ki, Bo Youl Choi, and JinKwan Hong. 2018. "Airflow as a Possible Transmission Route of Middle East Respiratory Syndrome at an Initial Outbreak Hospital in Korea" International Journal of Environmental Research and Public Health 15, no. 12: 2757. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15122757