Smartphone Applications for Mindfulness Interventions with Suicidality in Asian Older Adults: A Literature Review


Abstract
:1. Introduction
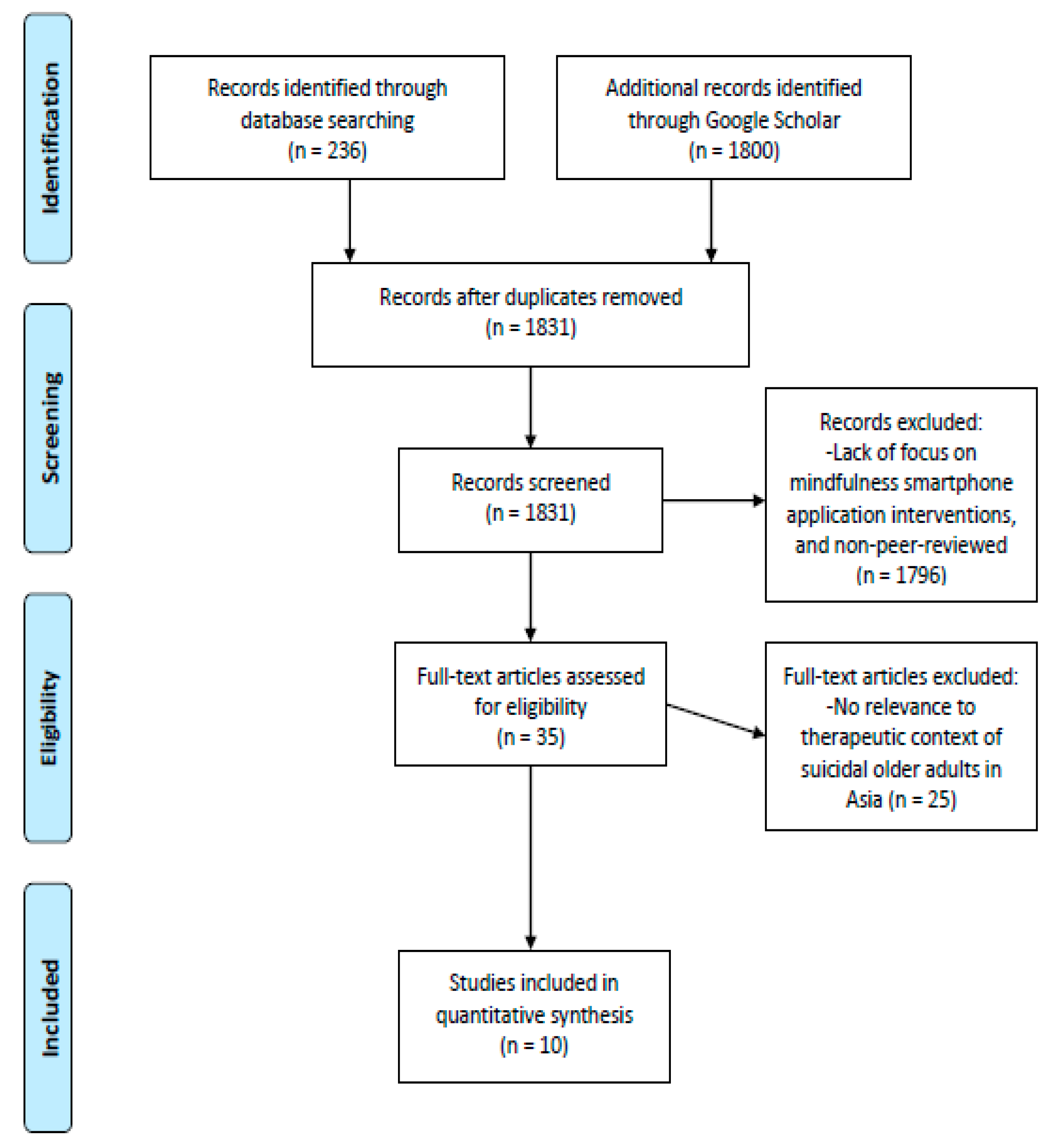
2. Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Cheng, A.; Lee, C. Suicide in Asia and Far East. In The International Handbook of Suicide and Attempted Suicide; Hawton, K., Van Heeringen, K., Eds.; John Wiley & Songs: West Sussex, UK, 2000; pp. 29–48. [Google Scholar]
- Lynch, M.; Howard, P.; El-Mallakh, E.; Matthews, J. Assessment and management of hospitalized suicidal patients. J. Psychosoc. Nurs. Ment. Health Serv. 2008, 46, 45–52. [Google Scholar] [PubMed]
- Cantor, C. Suicide in the Western world. In The International Handbook of Suicide and Attempted Suicide; Hawton, K., Van Heeringen, K., Eds.; John Wiley & Songs: West Sussex, UK, 2000; pp. 9–28. [Google Scholar]
- Liu, K.Y.; Yip, S.F. Mainland China. In Suicide in Asia: Causes and Prevention; Yip, P.S., Ed.; Hong Kong University Press: Hong Kong, China, 2008; pp. 31–49. [Google Scholar]
- Lo, W. Suicidal behaviour in Hong Kong. In Suicidal Behaviour in the Asia Pacific Region; Kok, L., Tseng, W., Eds.; Singapore University Press: Kent Ridge, Singapore, 1992; pp. 83–111. [Google Scholar]
- Maris, R.; Berman, A.; Silverman, M. Comprehensive Textbook of Suicidology; Guilford Press: New York, NY, USA, 2000. [Google Scholar]
- Peng, K.; Choo, A. Suicide and parasuicide in Singapore. Med. Sci. Law 1990, 30, 225–233. [Google Scholar] [CrossRef] [PubMed]
- Kua, E.; Tsoi, W. Suicide in the island of Singapore. Acta Psychiatr. Scand. 1985, 71, 227–229. [Google Scholar] [CrossRef] [PubMed]
- Morgan, A. Special issues of assessment and treatment of suicide risk in the elderly. In Suicide: Understanding and Responding; Jacobs, D., Browns, H., Eds.; International Universities Press: Madison, WI, USA, 1989; pp. 239–255. [Google Scholar]
- Pritchard, C. Suicide—The Ultimate Rejection? A Psycho-Social Study; Open University Press: Buckingham, UK, 1995. [Google Scholar]
- Stillion, J.; McDowell, E. Suicide across the Lifespan: Premature Exits; Taylor and Francis: Washington, DC, USA, 1996. [Google Scholar]
- Richman, J. Psychotherapy with suicidal older adults. In Treatment of Suicidal People; Leenaars, A., Maltsberger, J., Neimeyer, R., Eds.; Taylor and Francis: Washington, DC, USA, 1994; pp. 101–113. [Google Scholar]
- Chia, B.; Chia, A.; Tai, B. Suicide letters in Singapore. Arch. Suicide Res. 2008, 12, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Hawton, K. Why has suicide increased in young males? Crisis 1998, 19, 119–124. [Google Scholar] [CrossRef]
- Gunnell, D.; Frankel, S. Prevention of suicide: Aspirations and evidence. BMJ 1994, 308, 1227–1233. [Google Scholar] [CrossRef]
- Zhang, M.W.; Tsang, T.; Cheow, E.; Ho, C.S.H.; Yeong, N.B.; Ho, R.C. Enabling psychiatrists to be mobile phone app developers: Insights into app development methodologies. JMIR mHealth uHealth 2014, 2, e53. [Google Scholar] [CrossRef]
- Zhang, M.; Cheow, E.; Ho, C.S.H.; Ng, B.Y.; Ho, R.; Cheok, C.C. Application of low-cost methodologies for mobile phone app development. JMIR mHealth uHealth 2014, 2, e55. [Google Scholar] [CrossRef]
- Zhang, M.W.; Ho, R.C. Moodle: The cost effective solution for internet cognitive behavioral therapy (I-CBT) interventions. Technol. Health Care 2017, 25, 163–165. [Google Scholar] [CrossRef]
- Aggarwal, N.K. Applying mobile technologies to mental health service delivery in South Asia. Asian J. Psychiatr. 2012, 5, 225–230. [Google Scholar] [CrossRef]
- Brian, R.M.; Ben-Zeev, D. Mobile health (mHealth) for mental health in Asia: Objectives, strategies, and limitations. Asian J. Psychiatr. 2014, 10, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Ho, C.; Fang, P.; Lu, Y.; Ho, R. Usage of social media and smartphone application in assessment of physical and psychological well-being of individuals in times of a major air pollution crisis. JMIR mHealth uHealth 2014, 2, e16. [Google Scholar] [CrossRef] [PubMed]
- Ho, R.C.; Zhang, M.W.; Ho, C.S.; Pan, F.; Lu, Y.; Sharma, V.K. Impact of 2013 south Asian haze crisis: Study of physical and psychological symptoms and perceived generousness of pollution level. BMC Psychiatry 2014, 14, 81. [Google Scholar] [CrossRef] [PubMed]
- Preziosa, A.; Grassi, A.; Gaggioli, A.; Riva, G. Therapeutic applications of the mobile phone. Br. J. Guid. Couns. 2009, 37, 313–325. [Google Scholar] [CrossRef] [Green Version]
- Kazemi, D.; Cochran, A.; Kelly, J.; Cornelius, J.; Belk, C. Integrating mHealth mobile applications to reduce high risk drinking among underage students. Health Educ. J. 2014, 23, 263–273. [Google Scholar] [CrossRef]
- Lu, H.; Frauendorfer, D.; Rabbi, M.; Mast, M.S.; Chittaranjan, G.T.; Campbell, A.T.; Gatica-Perez, D.; Choudhury, T. StressSense: Detecting stress in unconstrained acoustic environments using smartphones. In Proceedings of the 2012 ACM Conference on Ubiquitous Computing, Pittsburgh, PA, USA, 5–8 September 2012. [Google Scholar]
- Rachuri, K.; Musolesi, M.; Mascolo, C.; Rentfrow, P.J.; Longworth, C.; Aucinas, A. EmotionSense: A mobile phones based adaptive platform for experimental social psychology research. In Proceedings of the 2012 ACM Conference on Ubiquitous Computing, Copenhagen, Denmark, 26–29 September 2010. [Google Scholar]
- Carissoli, C.; Villani, D.; Riva, G. Does a meditation protocol supported by a mobile application help people reduce stress? Suggestions from a controlled pragmatic trial. Cyberpsychol. Behav. Soc. Netw. 2015, 18, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Howells, A.; Ivtzan, I.; Eiroa-Orosa, F.J. Putting the ‘app’ in happiness: A randomised controlled trial of a smartphone-based mindfulness intervention to enhance wellbeing. J. Happiness Stud. 2016, 17, 163–185. [Google Scholar] [CrossRef]
- Ly, K.H.; Trüschel, A.; Jarl, L.; Magnusson, S.; Windahl, T.; Johansson, R.; Carlbring, P.; Andersson, G. Behavioural activation versus mindfulness-based guided self-help treatment administered through a smartphone application: A randomised controlled trial. BMJ Open 2014, 4, e003440. [Google Scholar] [CrossRef] [PubMed]
- Van Emmerik, A.A.P.; Berings, F.; Lancee, J. Efficacy of a mindfulness-based mobile application: A randomized waiting-list controlled trial. Mindfulness 2018, 9, 187–198. [Google Scholar] [CrossRef] [PubMed]
- Yang, E.; Schamber, E.; Meyer, R.M.L.; Gold, J.I. Happier healers: Randomized controlled trial of mobile mindfulness for stress management. J. Altern. Complement. Med. 2018, 24, 505–513. [Google Scholar] [CrossRef] [PubMed]
- Elliott, J.C.; Carey, K.B.; Bolles, J.R. Computer-based interventions for college drinking: A qualitative review. Addict. Behav. 2008, 33, 994–1005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donker, T.; Petrie, K.; Proudfoot, J.; Clarke, J.; Birch, M.; Christensen, H. Smartphones for smarter delivery of mental health programs: A systematic review. J. Med. Internet Res. 2013, 15, e247. [Google Scholar] [CrossRef] [PubMed]
- Wayne, N.; Ritvo, P. Smartphone-enabled health coach intervention for people with diabetes from a modest socioeconomic strata community: Single-arm longitudinal feasibility study. J. Med. Internet Res. 2014, 16, e149. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, E.; Greene, C.; Hoffman, J.; Nguyen, T.; Wald, L.; Schmidt, J.; Ruzek, J. Preliminary evaluation of PTSD Coach, a smartphone app for post-traumatic stress symptoms. Mil. Med. 2014, 179, 12–18. [Google Scholar] [CrossRef] [PubMed]
- McGrievy, G.; Tate, D. Tweets, apps, and pods: Results of the 6-month mobile pounds off digitally (Mobile POD) randomized weight-loss intervention among adults. J. Med. Internet Res. 2011, 13, e120. [Google Scholar] [CrossRef] [PubMed]
- Aguilera, A.; Muñoz, R.F. Text messaging as an adjunct to CBT in low-income populations: A usability and feasibility pilot study. Prof. Psychol. Res. Pract. 2011, 42, 472–478. [Google Scholar] [CrossRef] [PubMed]
- Durnham. DBT Coach and Diary [Mobile Application Software]. 2013. Available online: https://itunes.apple.com/au/app/dbt-diary-card-skills-coach/id479013889?mt=8 (accessed on 6 January 2017).
- Rizvi, S.L.; Dimeff, L.A.; Skutch, J.; Carroll, D.; Linehan, M.M. A pilot study of the DBT coach: An interactive mobile phone application for individuals with borderline personality disorder and substance use disorder. Behav. Ther. 2011, 42, 589–600. [Google Scholar] [CrossRef] [PubMed]
- Choo, C.C.; Harris, K.M.; Chew, P.K.H.; Ho, R.C. Does ethnicity matter in risk and protective factors for suicide attempts and suicide lethality? PLoS ONE 2017, 12, e0175752. [Google Scholar] [CrossRef] [PubMed]
- Choo, C.C.; Chew, P.K.H.; Ho, R.C. Suicide precipitants differ across the lifespan but are not significant in predicting medically severe attempts. Int. J. Environ. Res. Public Health 2018, 15, 691. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.Y.S.; Mak, W.W.S.; Cheung, E.Y.L.; Ling, C.Y.M.; Lui, W.W.S.; Tang, W.K.; Wong, R.L.P.; Lo, H.H.M.; Mercer, S.; Ma, H.S.W. A randomized, controlled clinical trial: The effect of mindfulness-based cognitive therapy on generalized anxiety disorder among Chinese community patients: Protocol for a randomized trial. BMC Psychiatry 2011, 11, 187. [Google Scholar] [CrossRef]
- Chittaro, L.; Vianello, A. Evaluation of a mobile mindfulness app distributed through on-line stores: A 4-week study. Int. J. Hum. Comput. Stud. 2016, 86, 63–80. [Google Scholar] [CrossRef]
- Plaza, I.; Demarzo, M.M.P.; Herrera-Mercada, P.; García-Campayo, J. Mindfulness-based mobile applications: Literature review and analysis of current features. JMIR mHealth uHealth 2013, 1, e24. [Google Scholar] [CrossRef] [PubMed]
- Luoma, J.B.; Villatte, J.L. Mindfulness in the treatment of suicidal patients. Cogn. Behav. Pract. 2012, 19, 265–276. [Google Scholar] [CrossRef] [PubMed]
- McIndoo, C.C.; File, A.A.; Preddy, T.; Clark, C.G.; Hopko, D.R. Mindfulness-based therapy and behavioral activation: A randomized controlled trial with depressed college students. Behav. Res. Ther. 2016, 77, 118–128. [Google Scholar] [CrossRef]
- Thompson, M.; Gauntlett-Gilbert, J. Mindfulness with children and adolescents: Effective clinical application. Clin. Child Psychol. Psychiatry 2008, 13, 395–407. [Google Scholar] [CrossRef]
- Choo, C.; Diederich, J.; Song, I.; Ho, R. Cluster analysis reveals risk factors for repeated suicide attempts in a multi-ethnic Asian population. Asian J. Psychiatr. 2014, 8, 38–42. [Google Scholar] [CrossRef]
- Mani, M.; Kavanagh, D.J.; Hides, L.; Stoyanov, S.R. Review and evaluation of mindfulness-based iPhone apps. JMIR mHealth uHealth 2015, 3, e82. [Google Scholar] [CrossRef]
- Choo, C.C.; Harris, K.M.; Chew, P.K.H.; Ho, R.C. What predicts medical lethality of suicide attempts in Asian youths? Asian J. Psychiatr. 2017, 29, 136–141. [Google Scholar] [CrossRef]
- Plaza García, I.; Sánchez, C.M.; Espilez, Á.S.; García-Magariño, I.; Guillen, G.A.; García-Campayo, J. Development and initial evaluation of a mobile application to help with mindfulness training and practice. Int. J. Med. Inform. 2017, 105, 59–67. [Google Scholar] [CrossRef]
- Donovan, E.; Rodgers, R.F.; Cousineau, T.M.; McGowan, K.M.; Luk, S.; Yates, K.; Franko, D.L. Brief report: Feasibility of a mindfulness and self-compassion based mobile intervention for adolescents. J. Adolesc. 2016, 53, 217–221. [Google Scholar] [CrossRef]
- Cavanagh, K.; Strauss, C.; Forder, L.; Jones, F. Can mindfulness and acceptance be learnt by self-help? A systematic review and meta-analysis of mindfulness and acceptance-based self-help interventions. Clin. Psychol. Rev. 2014, 34, 118–129. [Google Scholar] [CrossRef] [PubMed]
- Cole-Lewis, H.; Kershaw, T. Text messaging as a tool for behavior change in disease prevention and management. Epidemiol. Rev. 2010, 32, 56–69. [Google Scholar] [CrossRef]
- Aguilera, A.; Muench, F. There’s an app for that: Information technology applications for cognitive behavioural pracitioners. Behav. Ther. 2012, 35, 65–73. [Google Scholar]
- Mohar, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e10000097. [Google Scholar] [CrossRef]
- Chittaro, L.; Vianello, A. Mobile mindfulness and user’s worry: A qualitative study of using a smartphone app for distancing from negative thoughts. Interact. Comput. 2016, 28, 695–717. [Google Scholar] [CrossRef]
- Laurie, J.; Blandford, A. Making time for mindfulness. Int. J. Med Inform. 2016, 96, 38–50. [Google Scholar] [CrossRef] [PubMed]
- Economides, M.; Martman, J.; Bell, M.J.; Sanderson, B. Improvements in stress, affect, and irritability following brief use of a mindfulness-based smartphone app: A randomized controlled trial. Mindfulness 2018, 9, 1584–1593. [Google Scholar] [CrossRef]
- Wolf, M.; Kraft, S.; Tschauner, K.; Bauer, S.; Becker, T.; Puschner, B. User activity in a mobile phone intervention to assist mindfulness exercises in people with depressive symptoms. Ment. Health Prev. 2016, 4, 57–62. [Google Scholar] [CrossRef]
- Kumar, S.; Mehrotra, S. Free mobile apps on depression for Indian users: A brief overview and critique. Asian J. Psychiatr. 2017, 28, 124–130. [Google Scholar] [CrossRef]
- Larsen, M.E.; Nicholas, J.; Christensen, H. A systematic assessment of smartphone tools for suicide prevention. PLoS ONE 2016, 11, e0152285. [Google Scholar] [CrossRef]
- Eysenbach, G.; CONSORT-EHEALTH Group. CONSORT-EHEALTH: Improving and standardizing evaluation reports of Web-based and mobile health interventions. J. Med. Internet Res. 2011, 13, e126. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author/Year | Study Design/Participants Characteristics/Grouping | Study Objectives | Results |
|---|---|---|---|
| Plaza Garcia, Sanchez, Espilez, Magarino, Guillen, and Garcia-Campayo (2017) [51] | Nonrandomized controlled trial 3977 users were involved in this study: 26 in the first trial during an 8-week usage period and 3951 in the second trial for 17 months (7.7% of the sample were below the age of 29 years) | The aim of the study was to examine a first prototype of a smartphone application with Spanish features for the training and practice of mindfulness. | In the first study, participants assessed the application and considered it a helping tool for mindfulness practice, and user-friendly. In the second study, weak associations were found between usage time and age, nationality, and educational level. The mindfulness level showed a weak positive correlation with the session accomplished (p = 0.051). Videos and information stood out as the most accessed resources. |
| Carissoli, Villani, and Riva (2015) [27] | Controlled pragmatic trial 56 Italian workers (Mage = 38.11, SDage = 6.92) were block-randomized to three conditions (self-help mindfulness, relaxing music, and wait list) | The aim of this study was to examine the efficacy of a 3-week mindfulness-inspired protocol, delivered by an Android application for smartphones, in reducing stress in the adult population. | No significant differences between groups on any of the perceived stress dimensions measured (p = 0.103–0.952). Participants in the mindfulness group reported significant reductions in hyperactivity and accelerated behaviors (p = 0.010). |
| Chittaro and Vianello (2016a) [43] | Mixed methods, longitudinal study 3979 participants downloaded the app but only 136 (Mage = 37.85, SDage = 11.30) completed all the questionnaires required. No grouping or specific demographical data. | The aim of this study was to assess the effectiveness of a mobile mindfulness app at increasing levels of mindfulness. | The results revealed that users with no or minimal experience with meditation significantly increased in their levels of mindfulness from the start and at the end of the 4-week study period (p < 0.001). Additionally, qualitative feedback indicated that the app was positively perceived as beautiful and its usage elicited positive feelings in the participants. |
| Donovan et al. (2016) [52] | Mixed methods, nonrandomized controlled trial 20 participants (Mage = 16.9, SDage = 1.3) of ethnically diverse origins (7 African American, 3 Black Latino, 2 Hispanic, 2 Asian, 1 Native American, 1 Latino, and 4 Caucasian). | The aim of the study was to test the feasibility of a mindfulness and self-compassion based program for adolescents, delivered though mobile phones over a 30-day period. | Outcome measures included usage, satisfaction, and focus group findings. Usage data showed that participants used the app on the majority of the 30 days (M = 16.8, SD = 6.4, Range = 6–26). Satisfaction data indicated that they enjoyed using the program (92%), found it easy to navigate (72%) and understand (86%), and that the program helped them to focus on their feelings (71%) and learn new relaxation skills (64%). A total of 64% indicated they would be likely to continue using it. Qualitative data corroborated these findings but also provided suggestions for improvement (e.g., a more personalized experience). |
| Economides, Martman, Bell, and Sanderson (2018) [59] | Randomized controlled trial 69 participants randomized into headspace (n = 41, 75.6% White, 4.9% Hispanic, 2.4% African American, 9.8% Asian, 4.9% Mixed, and 2.4% others) and audiobook conditions (n = 28, 64.3% White, 3.6% Hispanic, 17.9% Asian, 7.14% Mixed, and 7.14% others) completed the study. | The study aimed to assess whether completing the first 10 introductory sessions of the mindfulness-based smartphone app Headspace positively impacted stress, affect, and irritability, relative to an active control (audiobook on mindfulness, which differed only on content). | The results suggested that there was no significant difference between both interventions, as they were equally effective at reducing stress associated with personal vulnerability (p = 0.09, d = 0.26); but only the mindfulness intervention had a significant positive impact on irritability (p < 0.05, d = 0.44), affect (p < 0.001, d = 0.47), and stress resulting from external pressure(p < 0.001, d = 0.45). |
| Hoswells, Iytzan, and Eiroa-Orosa (2016) [28] | Randomized controlled trial 121 participants (Mage = 40.7, SDage = 10.6) were assigned to the experimental (57) and control condition (64). The sample consisted pf 90.1% Caucasian, 1.7% Asian/Pacific Islander, 1.7% Hispanic, 5.0% other/multiracial, and 1.5% who declined to respond. | The objective of the study was to measure the efficacy of a mindfulness-based smartphone application designed to enhance wellbeing. | The findings on the mindfulness meditation application Headspace found that it was associated with a significantly increased positive affect (p = 0.003) and decreased depression (p = 0.05). No statistically significant difference in satisfaction with life or negative affect was found and might be attributable to the limited time duration of the research (intervention only lasted for 10 days) and there was only one post-intervention measurement. |
| Ly et al. (2014) [29] | Randomized controlled trial 81 participants (Mage = 36.0, SDage = 10.8) diagnosed with major depressive disorder were randomized into a behavioral activation treatment (n = 40) and mindfulness treatment (n = 41). No specific demographic information. | The aim of the study was to test the effects of two smartphone-delivered treatments, and to find out if the behavioral activation treatment was more effective than the mindfulness treatment. To evaluate the long-term effects, a 6-month follow-up after the start of the treatment was also included. | The results showed no significant interaction effect of group and time on any of the outcome measures either from pretreatment to post-treatment or from pretreatment to the 6-month follow-up. Subgroup analyses showed that the behavioral activation treatment was more effective than the mindfulness treatment among participants with higher initial severity of depression from pretreatment to the 6-month follow-up based on the PHQ-9 (p < 0.05, d = 0.47). Mindfulness treatment worked better among participants with lower initial severity from pretreatment to the 6-month follow-up based on the PHQ-9 (p < 0.01, d = 0.98) and BDI-II (p < 0.05, d = 1.21). |
| Van Emmerik, Berings, and Lancee (2018) [30] | Randomized controlled trial 377 participants were randomized into either a mindfulness (n = 191, Mage = 45.63, SDage = 9.09, 4.2% male, 95.8% female) or waitlist control condition (n = 186, Mage = 43.78, SDage = 10.48, 3.8% male, 96.2% female) | The aim of the study was to evaluate the immediate and long-term efficacy of an MBI app (the VGZ Mindfulness Coach) in a wait-list controlled randomized trial, with mindfulness as a primary outcome variable and without any form of therapeutic guidance in addition to the self-help app. | The results revealed that compared to the waitlist control, the mindfulness intervention group, large (Cohen’s d = 0.77) and statistically significant increases of mindfulness after 8 weeks and small-to-medium increases of the Observing, Describing, Acting with awareness, Nonjudging, and Nonreactivity mindfulness facets as measured with the five facet mindfulness questionnaire (Cohen’s d = 0.66, 0.26, 0.49, 0.34, and 0.43, respectively) were reported. There were also large decreases of general psychiatric symptoms (GHQ-12; Cohen’s d = −0.68) and moderate increases of psychological, social, and environmental quality of life (WHOQOL-BREF; Cohen’s d = 0.38, 0.38, and 0.36, respectively). Except for social quality of life, these gains were maintained for at least 3 months. |
| Wolf, Kraft, Tschauner, Bauer, Becker, and Puschner, (2016) [60] | Randomized controlled trial 41 patients were randomized into either a text message mindfulness intervention (n = 21, Mage = 43.38, SDage = 12.65) or control group (n = 20, information about control group not provided). No other demographic data. | This study investigated the user activity in a text messaging intervention to assist mindfulness practice in patients with symptoms of depression. | The results revealed that women sent more messages than men (d = 0.73), and age was moderately correlated with the number of messages sent (r = 0.39). Prior text messaging experience was negatively associated with the activity of participants as more experienced participants sent fewer messages (r = −0.42). Participants who attended more mindfulness group sessions were also sending more messages (r = 0.40). Prior mindfulness experience also led to more messages being sent (d = 0.25). The number of messages sent was correlated with reductions in depressive symptoms (r = −0.46), preservative thinking (r = −0.36), and moderately associated with increases in self compassion(r = 0.45) and mindfulness (r = 0.23). |
| Yang, Schamber, Meyer, and Gold (2018) [31] | Randomized controlled trial 8 medical students (Mage = 25.11, Range 21–47; 63.6% female, 36.4% male; 25% Asian/Pacific Islander, 6.8% Black, 46.6% Caucasian, 5.7% Latino, 10.2% Mixed, and 5.7% others) were stratified by class year and randomized to either mindfulness intervention (n = 45) or control group (n = 43). | This study assessed whether 10–20 min of daily mindfulness meditation for 30 days, using a mobile phone application, could decrease perceived stress and improve wellbeing for medical students. | All participants completed the perceived stress scale (PSS), five-facet mindfulness questionnaire (FFMQ), and general wellbeing schedule (GWBS) at baseline, 30 days, and 60 days. There was a significant interaction between time and treatment group for perceived stress and wellbeing. Perceived stress significantly decreased for the intervention group (p < 0.05). General wellbeing significantly increased for the intervention group compared to the control group and the increase was sustained (p < 0.05). |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choo, C.C.; Kuek, J.H.L.; Burton, A.A.D. Smartphone Applications for Mindfulness Interventions with Suicidality in Asian Older Adults: A Literature Review. Int. J. Environ. Res. Public Health 2018, 15, 2810. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15122810
Choo CC, Kuek JHL, Burton AAD. Smartphone Applications for Mindfulness Interventions with Suicidality in Asian Older Adults: A Literature Review. International Journal of Environmental Research and Public Health. 2018; 15(12):2810. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15122810
Chicago/Turabian StyleChoo, Carol C., Jonathan H. L. Kuek, and André A. D. Burton. 2018. "Smartphone Applications for Mindfulness Interventions with Suicidality in Asian Older Adults: A Literature Review" International Journal of Environmental Research and Public Health 15, no. 12: 2810. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15122810