A Comparison of Mercury Exposure from Seafood Consumption and Dental Amalgam Fillings in People with and without Amyotrophic Lateral Sclerosis (ALS): An International Online Case-Control Study


Abstract
:1. Introduction
2. Methods
2.1. Setting
2.2. Ethics Approval
2.3. Frequency of Seafood Consumption
2.4. Favourite Seafoods
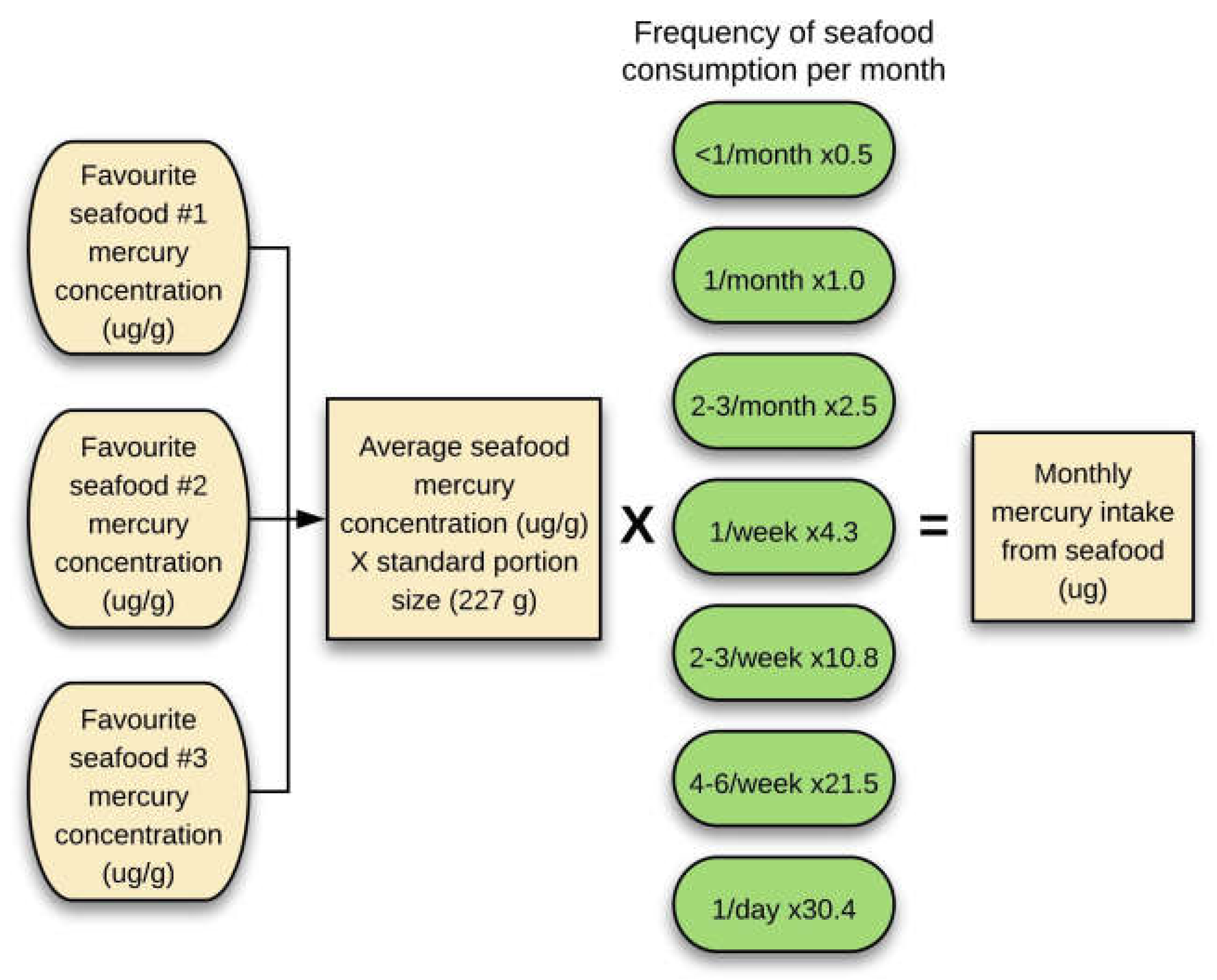
2.5. Estimation of Monthly Mercury Exposure from Seafood
2.6. Mercury-Containing Dental Fillings
2.7. Statistical Analyses
3. Results
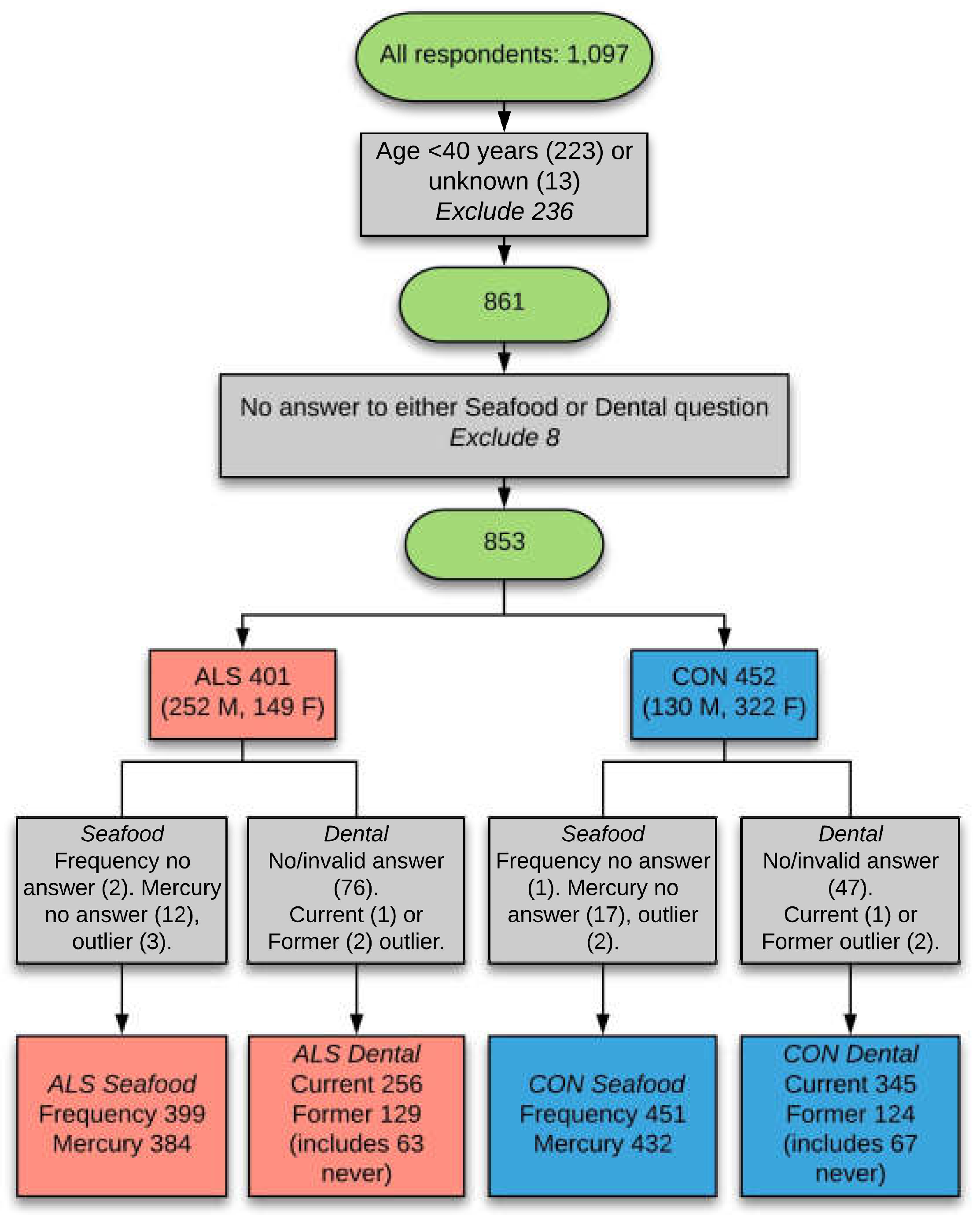
3.1. Cases and Controls
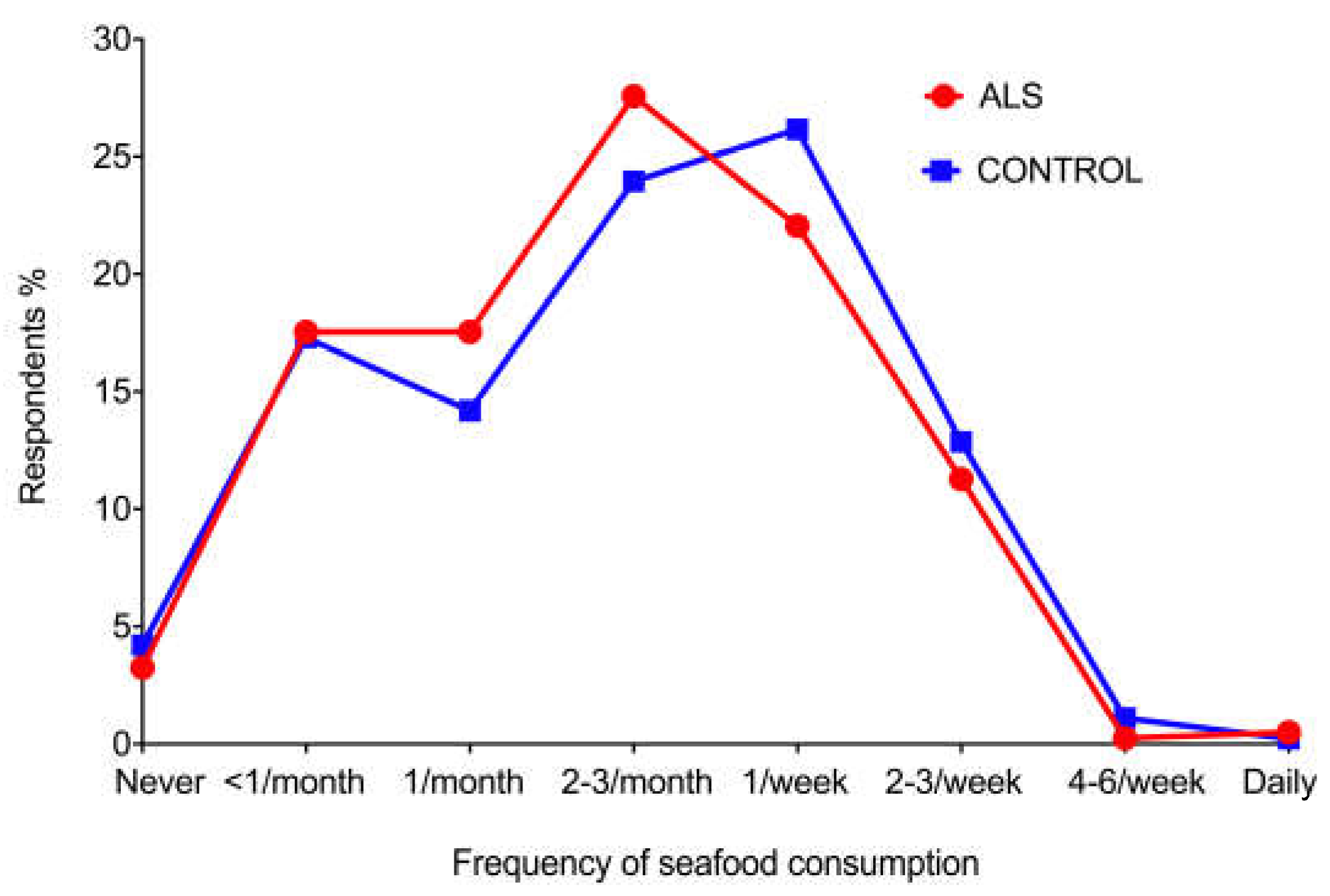
3.2. Frequency of Seafood Consumption
3.3. Favourite Seafoods
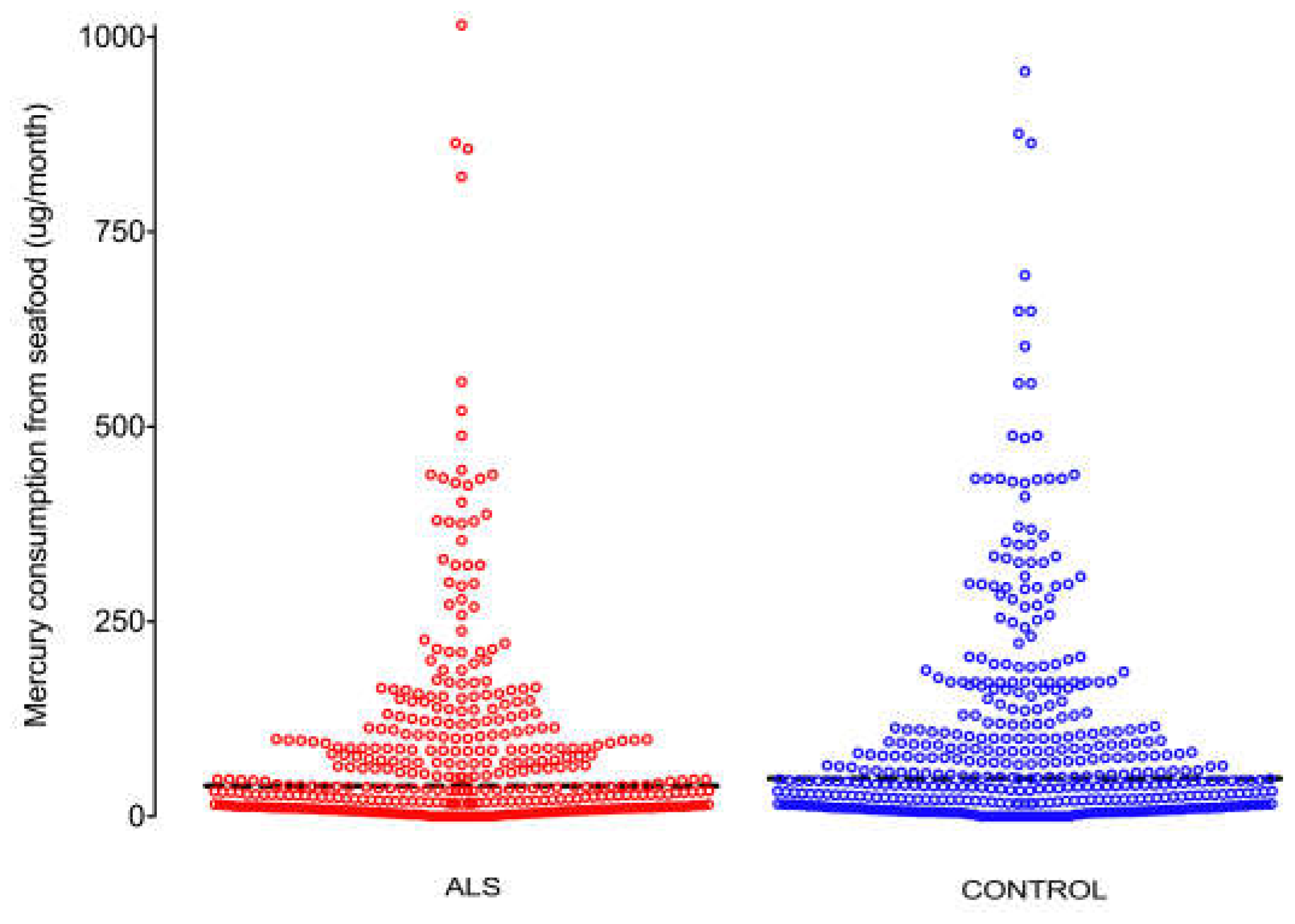
3.4. Mercury Consumption from Favourite Seafoods
3.5. Intra- and Inter-Country Comparisons of Mercury Consumption from Favourite Seafoods
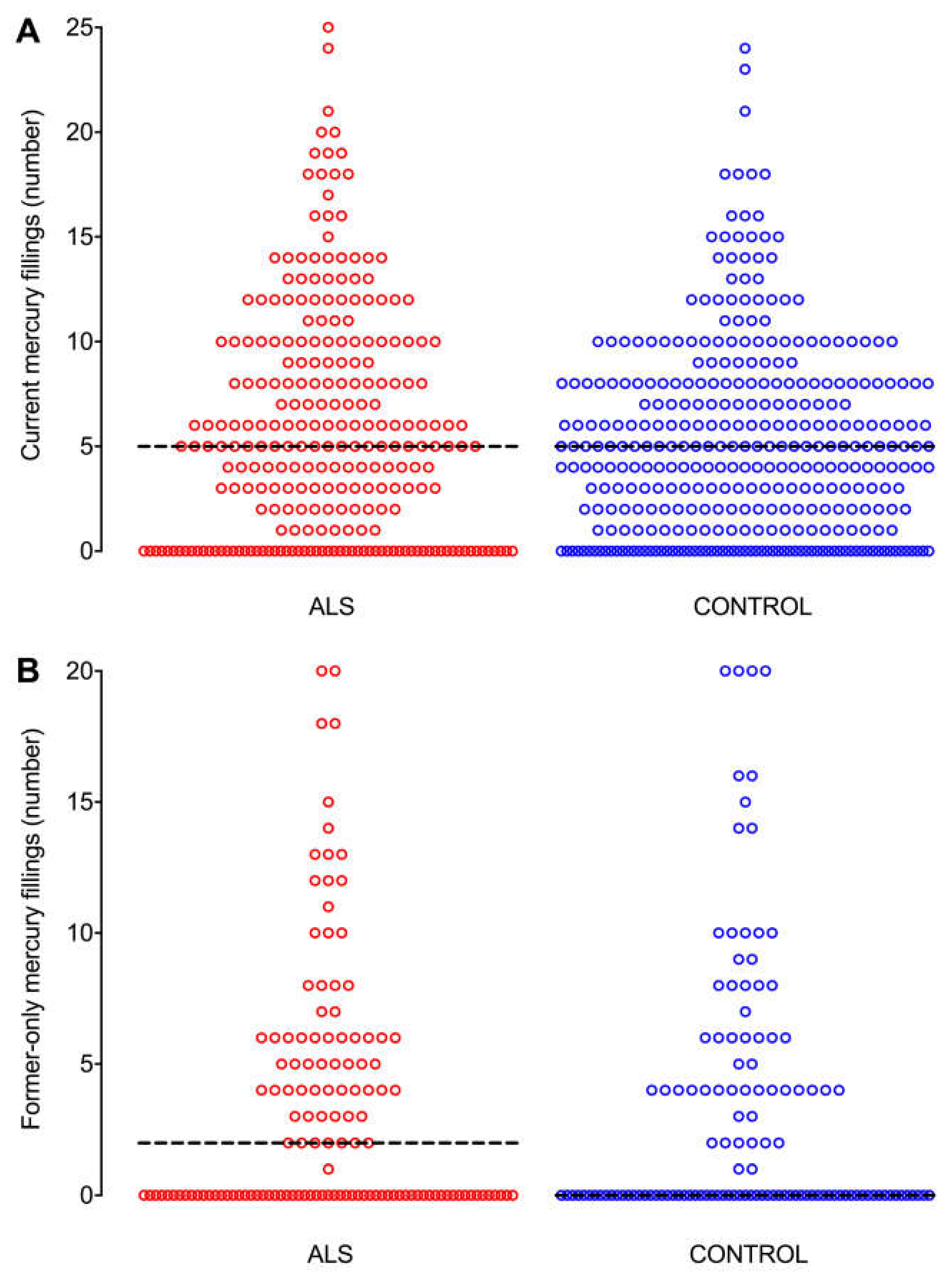
3.6. Mercury-Containing Dental Fillings
3.7. Intra- and Inter-Country Comparisons of Mercury-Containing Dental Fillings
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Brown, I.A. Chronic mercurialism: A cause of the clinical syndrome of amyotrophic lateral sclerosis. AMA Arch. Neurol. Psychiatry 1954, 72, 674–681. [Google Scholar] [CrossRef] [PubMed]
- Adams, C.R.; Ziegler, D.K.; Lin, J.T. Mercury intoxication simulating amyotrophic lateral sclerosis. JAMA 1983, 250, 642–643. [Google Scholar] [CrossRef] [PubMed]
- Johnson, F.O.; Atchison, W.D. The role of environmental mercury, lead and pesticide exposure in development of amyotrophic lateral sclerosis. Neurotoxicology 2009, 30, 761–765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bjorklund, G.; Dadar, M.; Mutter, J.; Aaseth, J. The toxicology of mercury: Current research and emerging trends. Environ. Res. 2017, 159, 545–554. [Google Scholar] [CrossRef] [PubMed]
- Hardiman, O.; Al-Chalabi, A.; Chio, A.; Corr, E.M.; Logroscino, G.; Robberecht, W.; Shaw, P.J.; Simmons, Z.; van den Berg, L.H. Amyotrophic lateral sclerosis. Nat. Rev. Dis. Primers 2017, 3. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.W.; Hartmann, H.A. Electron microscopic histochemical study on the localization and distribution of mercury in the nervous system after mercury intoxication. Exp. Neurol. 1972, 35, 122–137. [Google Scholar] [CrossRef]
- Haase, G.; Rabouille, C. Golgi Fragmentation in ALS Motor Neurons. New Mechanisms Targeting Microtubules, Tethers, and Transport Vesicles. Front. Neurosci. 2015, 9, 448. [Google Scholar] [CrossRef] [PubMed]
- Arvidson, B. Inorganic mercury is transported from muscular nerve terminals to spinal and brainstem motoneurons. Muscle Nerve 1992, 15, 1089–1094. [Google Scholar] [CrossRef] [PubMed]
- Pamphlett, R.; Waley, P. Mercury in human spinal motor neurons. Acta Neuropathol. 1998, 96, 515–519. [Google Scholar] [CrossRef]
- Pamphlett, R.; Kum Jew, S. Age-Related Uptake of Heavy Metals in Human Spinal Interneurons. PLoS ONE 2016, 11, e0162260. [Google Scholar] [CrossRef]
- Pamphlett, R.; Kum Jew, S. Uptake of inorganic mercury by human locus ceruleus and corticomotor neurons: Implications for amyotrophic lateral sclerosis. Acta Neuropathol. Commun. 2013, 1, 13. [Google Scholar] [CrossRef] [PubMed]
- Pamphlett, R.; Kum Jew, S. Inorganic mercury in human astrocytes, oligodendrocytes, corticomotoneurons and the locus ceruleus: Implications for multiple sclerosis, neurodegenerative disorders and gliomas. Biometals 2018, 31, 807–819. [Google Scholar] [CrossRef] [PubMed]
- Eisen, A.; Kim, S.; Pant, B. Amyotrophic lateral sclerosis (ALS): A phylogenetic disease of the corticomotoneuron? Muscle Nerve 1992, 15, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Turner, M.R.; Kiernan, M.C. Does interneuronal dysfunction contribute to neurodegeneration in amyotrophic lateral sclerosis? Amyotroph. Lateral Scler. 2012, 13, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Philips, T.; Bento-Abreu, A.; Nonneman, A.; Haeck, W.; Staats, K.; Geelen, V.; Hersmus, N.; Kusters, B.; Van Den Bosch, L.; Van Damme, P.; et al. Oligodendrocyte dysfunction in the pathogenesis of amyotrophic lateral sclerosis. Brain 2013, 136, 471–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vinceti, M.; Bottecchi, I.; Fan, A.; Finkelstein, Y.; Mandrioli, J. Are environmental exposures to selenium, heavy metals, and pesticides risk factors for amyotrophic lateral sclerosis? Rev. Environ. Health 2012, 27, 19–41. [Google Scholar] [CrossRef] [PubMed]
- Vinceti, M.; Filippini, T.; Mandrioli, J.; Violi, F.; Bargellini, A.; Weuve, J.; Fini, N.; Grill, P.; Michalke, B. Lead, cadmium and mercury in cerebrospinal fluid and risk of amyotrophic lateral sclerosis: A case-control study. J. Trace Elem. Med. Biol. 2017, 43, 121–125. [Google Scholar] [CrossRef]
- Pamphlett, R.; Waley, P. Motor neuron uptake of low dose inorganic mercury. J. Neurol. Sci. 1996, 135, 63–67. [Google Scholar] [CrossRef]
- Mercury Levels in Commercial Fish and Shellfish (1990–2012). Available online: https://www.fda.gov /food/foodborneillnesscontaminants/metals/ucm115644.htm (accessed on 13 November 2018).
- About Dental Amalgam Fillings. Available online: https://www.fda.gov/medicaldevices /productsandmedicalprocedures/dentalproducts/dentalamalgam/ucm171094.htm (accessed on 13 November 2018).
- Clarkson, T.W.; Magos, L. The toxicology of mercury and its chemical compounds. Crit. Rev. Toxicol. 2006, 36, 609–662. [Google Scholar] [CrossRef]
- Ho, D.T.; Russell, J.A. Mercury and motor neuron disease: Hooked on a hypothesis. Muscle Nerve 2018. [CrossRef]
- Andrew, A.S.; Chen, C.Y.; Caller, T.A.; Tandan, R.; Henegan, P.L.; Jackson, B.P.; Hall, B.P.; Bradley, W.G.; Stommel, E.W. Toenail mercury levels are associated with amyotrophic lateral sclerosis risk. Muscle Nerve 2018. [CrossRef] [PubMed]
- Mangelsdorf, I.; Walach, H.; Mutter, J. Healing of Amyotrophic Lateral Sclerosis: A Case Report. Complement. Med. Res. 2017, 24, 175–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parkin Kullmann, J.A.; Hayes, S.; Wang, M.X.; Pamphlett, R. Designing an Internationally Accessible Web-Based Questionnaire to Discover Risk Factors for Amyotrophic Lateral Sclerosis: A Case-Control Study. JMIR Res. Protoc. 2015, 4, e96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Padula, D.; Greenfield, H.; Cunningham, J.; Kiermeier, A.; McLeod, C. Australian seafood compositional profiles: A pilot study. Vitamin D and mercury content. Food Chem. 2016, 193, 106–111. [Google Scholar] [CrossRef]
- Guidance for Assessing Chemical Contaminant Data for Use in Fish Advisories, Volume 2, Risk Assessment and Fish Consumption Limits 2000. Available online: https://www.epa.gov/quality/guidance-assessing-chemical-contaminant-data-use-fish-advisories-volume-2-risk-assessment (accessed on 7 October 2018).
- Maier, A.; Holm, T.; Wicks, P.; Steinfurth, L.; Linke, P.; Munch, C.; Meyer, R.; Meyer, T. Online assessment of ALS functional rating scale compares well to in-clinic evaluation: A prospective trial. Amyotroph. Lateral Scler. 2012, 13, 210–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chio, A. ISIS Survey: An international study on the diagnostic process and its implications in amyotrophic lateral sclerosis. J. Neurol. 1999, 246 (Suppl. 3), III1-5. [Google Scholar] [CrossRef]
- Vimy, M.J.; Lorscheider, F.L. Serial measurements of intra-oral air mercury: Estimation of daily dose from dental amalgam. J. Dent. Res. 1985, 64, 1072–1075. [Google Scholar] [CrossRef]
- Methylmercury (MeHg). Available online: https://cfpub.epa.gov/ncea/iris2/ chemicallanding.cfm?substance_nmbr=73 (accessed on 2 October 2018).
- Banack, S.A.; Metcalf, J.S.; Bradley, W.G.; Cox, P.A. Detection of cyanobacterial neurotoxin beta-N-methylamino-l-alanine within shellfish in the diet of an ALS patient in Florida. Toxicon 2014, 90, 167–173. [Google Scholar] [CrossRef]
- Caller, T.A.; Field, N.C.; Chipman, J.W.; Shi, X.; Harris, B.T.; Stommel, E.W. Spatial clustering of amyotrophic lateral sclerosis and the potential role of BMAA. Amyotroph. Lateral Scler. 2012, 13, 25–32. [Google Scholar] [CrossRef]
- Andreoli, V.; Sprovieri, F. Genetic Aspects of Susceptibility to Mercury Toxicity: An Overview. Int. J. Environ. Res. Public Health 2017, 14. [Google Scholar] [CrossRef]
- Basu, N.; Goodrich, J.M.; Head, J. Ecogenetics of mercury: From genetic polymorphisms and epigenetics to risk assessment and decision-making. Environ. Toxicol. Chem. 2014, 33, 1248–1258. [Google Scholar] [CrossRef] [PubMed]
- Young, P.E.; Kum Jew, S.; Buckland, M.E.; Pamphlett, R.; Suter, C.M. Epigenetic differences between monozygotic twins discordant for amyotrophic lateral sclerosis (ALS) provide clues to disease pathogenesis. PLoS ONE 2017, 12, e0182638. [Google Scholar] [CrossRef] [PubMed]
- Yu, B.; Pamphlett, R. Environmental insults: Critical triggers for amyotrophic lateral sclerosis. Transl. Neurodegener. 2017, 6, 15. [Google Scholar] [CrossRef] [PubMed]
- Bailey, J.M.; Colon-Rodriguez, A.; Atchison, W.D. Evaluating a Gene-Environment Interaction in Amyotrophic Lateral Sclerosis: Methylmercury Exposure and Mutated SOD1. Curr. Environ. Health Rep. 2017, 4, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Pamphlett, R.; Bishop, D.P.; Kum Jew, S.; Doble, P.A. Age-related accumulation of toxic metals in the human locus ceruleus. PLoS ONE 2018, 13, e0203627. [Google Scholar] [CrossRef] [PubMed]
- Chio, A.; Mazzini, L.; D’Alfonso, S.; Corrado, L.; Canosa, A.; Moglia, C.; Manera, U.; Bersano, E.; Brunetti, M.; Barberis, M.; et al. The multistep hypothesis of ALS revisited: The role of genetic mutations. Neurology 2018, 91, e635–e642. [Google Scholar] [CrossRef] [PubMed]
- Andrade, V.M.; Aschner, M.; Marreilha Dos Santos, A.P. Neurotoxicity of Metal Mixtures. Adv. Neurobiol. 2017, 18, 227–265. [Google Scholar] [CrossRef]
- Bjorklund, G.; Aaseth, J.; Ajsuvakova, O.P.; Nikonorov, A.A.; Skalny, A.V.; Skalnaya, M.G.; Tinkov, A.A. Molecular interaction between mercury and selenium in neurotoxicity. Coordin. Chem. Rev. 2017, 332, 30–37. [Google Scholar] [CrossRef]
- Cardoso, B.R.; Roberts, B.R.; Bush, A.I.; Hare, D.J. Selenium, selenoproteins and neurodegenerative diseases. Metallomics 2015, 7, 1213–1228. [Google Scholar] [CrossRef] [Green Version]
- Sanchez-Diaz, G.; Escobar, F.; Badland, H.; Arias-Merino, G.; Posada de la Paz, M.; Alonso-Ferreira, V. Geographic Analysis of Motor Neuron Disease Mortality and Heavy Metals Released to Rivers in Spain. Int. J. Environ. Res. Public Health 2018, 15. [Google Scholar] [CrossRef]
- Mercury. Available online: https://www.cdc.gov/niosh/topics/mercury/default.html (accessed on 1 November 2018).
- Pamphlett, R.; Rikard-Bell, A. Different occupations associated with amyotrophic lateral sclerosis: Is diesel exhaust the link? PLoS ONE 2013, 8, e80993. [Google Scholar] [CrossRef] [PubMed]
- Gunnarsson, L.G.; Bodin, L. Amyotrophic Lateral Sclerosis and Occupational Exposures: A Systematic Literature Review and Meta-Analyses. Int. J. Environ. Res. Public Health 2018, 15. [Google Scholar] [CrossRef] [PubMed]
- Gresham, L.S.; Molgaard, C.A.; Golbeck, A.L.; Smith, R. Amyotrophic lateral sclerosis and occupational heavy metal exposure: A case-control study. Neuroepidemiology 1986, 5, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Gunnarsson, L.G.; Bodin, L.; Soderfeldt, B.; Axelson, O. A case-control study of motor neurone disease: Its relation to heritability, and occupational exposures, particularly to solvents. Br. J. Ind. Med. 1992, 49, 791–798. [Google Scholar] [CrossRef] [PubMed]
- McGuire, V.; Longstreth, W.T., Jr.; Nelson, L.M.; Koepsell, T.D.; Checkoway, H.; Morgan, M.S.; van Belle, G. Occupational exposures and amyotrophic lateral sclerosis. A population-based case-control study. Am. J. Epidemiol. 1997, 145, 1076–1088. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Su, F.C.; Callaghan, B.C.; Goutman, S.A.; Batterman, S.A.; Feldman, E.L. Environmental risk factors and amyotrophic lateral sclerosis (ALS): A case-control study of ALS in Michigan. PLoS ONE 2014, 9, e101186. [Google Scholar] [CrossRef]
- Andrew, A.S.; Caller, T.A.; Tandan, R.; Duell, E.J.; Henegan, P.L.; Field, N.C.; Bradley, W.G.; Stommel, E.W. Environmental and Occupational Exposures and Amyotrophic Lateral Sclerosis in New England. Neurodegener. Dis. 2017, 17, 110–116. [Google Scholar] [CrossRef] [Green Version]
- Lamborg, C.H.; Hammerschmidt, C.R.; Bowman, K.L.; Swarr, G.J.; Munson, K.M.; Ohnemus, D.C.; Lam, P.J.; Heimburger, L.E.; Rijkenberg, M.J.; Saito, M.A. A global ocean inventory of anthropogenic mercury based on water column measurements. Nature 2014, 512, 65–68. [Google Scholar] [CrossRef]
- Missing Mercury Pollution Is Enough for Mass Poisoning. Available online: https://www.newscientist.com/article/mg22329811-800-missing-mercury-pollution-is-enough-for-mass-poisoning/ (accessed on 1 November 2018).
- Pamphlett, R.; Jew, S.K. Heavy metals in locus ceruleus and motor neurons in motor neuron disease. Acta Neuropathol. Commun. 2013, 1, 81. [Google Scholar] [CrossRef]
- Parkin Kullmann, J.A.; Pamphlett, R. Does the index-to-ring finger length ratio (2D:4D) differ in amyotrophic lateral sclerosis (ALS)? Results from an international online case-control study. BMJ Open 2017, 7, e016924. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ALS | N (%) | Control | N (%) | |
|---|---|---|---|---|
| Country of residence | ||||
| United States | 180 (45%) | Australia | 339 (75%) | |
| Australia | 116 (29%) | United States | 49 (11%) | |
| Canada | 57 (14%) | Other * (<2% each) | 36 (8%) | |
| Other * (<2% each) | 37 (9%) | Spain | 14 (3%) | |
| Spain | 9 (2%) | New Zealand | 12 (3%) | |
| Ancestry | ||||
| Other (<6% each) | 184 (47%) | Other (<4% each) | 154 (34%) | |
| Australian | 60 (15%) | Australian | 131 (29%) | |
| English | 57 (15%) | English | 77 (17%) | |
| American | 37 (9%) | Irish | 41 (9%) | |
| German | 32 (8%) | British | 25 (6%) | |
| Irish | 23 (6%) | Scottish | 19 (4%) | |
| Cultural group | ||||
| American | 112 (29%) | Australian | 286 (64%) | |
| Australian | 98 (26%) | Other (<2% each) | 76 (17%) | |
| Other (<3% each) | 93 (24%) | American | 33 (7%) | |
| Canadian | 40 (10%) | English | 27 (6%) | |
| English | 28 (7%) | Spanish | 14 (3%) | |
| German | 13 (3%) | New Zealander | 11 (2%) | |
| Respondents N | Median Mercury Consumption µg/month | p | r | |
|---|---|---|---|---|
| Intra-country: Control vs. ALS | ||||
| USA control | 47 | 32 | 0.80 | 0.02 |
| USA ALS | 177 | 31 | ||
| Australia control | 324 | 51 | 0.27 | 0.05 |
| Australia ALS | 109 | 69 | ||
| Other countries control | 61 | 65 | 0.40 | 0.07 |
| Other countries ALS | 98 | 47 | ||
| Inter-country: USA vs. Australia | ||||
| USA control | 47 | 32 | 0.02 | 0.12 |
| Australia control | 324 | 51 | ||
| USA ALS | 177 | 31 | <0.001 | 0.21 |
| Australia ALS | 109 | 69 | ||
| Respondents N | Median No. of Current Fillings | p | r | |
|---|---|---|---|---|
| Intra-country: Control vs. ALS | ||||
| USA control | 30 | 4.5 | 0.49 | 0.06 |
| USA ALS | 103 | 5.0 | ||
| Australia control | 270 | 5.0 | 0.42 | 0.04 |
| Australia ALS | 84 | 4.5 | ||
| Other countries control | 45 | 5.0 | 0.76 | 0.03 |
| Other countries ALS | 69 | 5.0 | ||
| Inter-country: USA vs. Australia | ||||
| USA control | 30 | 4.5 | 0.93 | 0.005 |
| Australia control | 270 | 5.0 | ||
| USA ALS | 103 | 5.0 | 0.80 | 0.02 |
| Australia ALS | 84 | 4.5 | ||
© 2018 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parkin Kullmann, J.A.; Pamphlett, R. A Comparison of Mercury Exposure from Seafood Consumption and Dental Amalgam Fillings in People with and without Amyotrophic Lateral Sclerosis (ALS): An International Online Case-Control Study. Int. J. Environ. Res. Public Health 2018, 15, 2874. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15122874
Parkin Kullmann JA, Pamphlett R. A Comparison of Mercury Exposure from Seafood Consumption and Dental Amalgam Fillings in People with and without Amyotrophic Lateral Sclerosis (ALS): An International Online Case-Control Study. International Journal of Environmental Research and Public Health. 2018; 15(12):2874. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15122874
Chicago/Turabian StyleParkin Kullmann, Jane A., and Roger Pamphlett. 2018. "A Comparison of Mercury Exposure from Seafood Consumption and Dental Amalgam Fillings in People with and without Amyotrophic Lateral Sclerosis (ALS): An International Online Case-Control Study" International Journal of Environmental Research and Public Health 15, no. 12: 2874. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15122874