Exercise Caution: Questions to Ask Adolescents Who May Exercise Too Hard


Abstract
:1. Introduction
The Present Study
2. Methods
2.1. Participants
2.2. Measures
2.3. Procedure
2.4. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. CE and Overall ED Symptom Burden
3.3. Associations between Individual Items and CE
3.3.1. Girls
3.3.2. Boys
4. Discussion
Strengths and Limitations
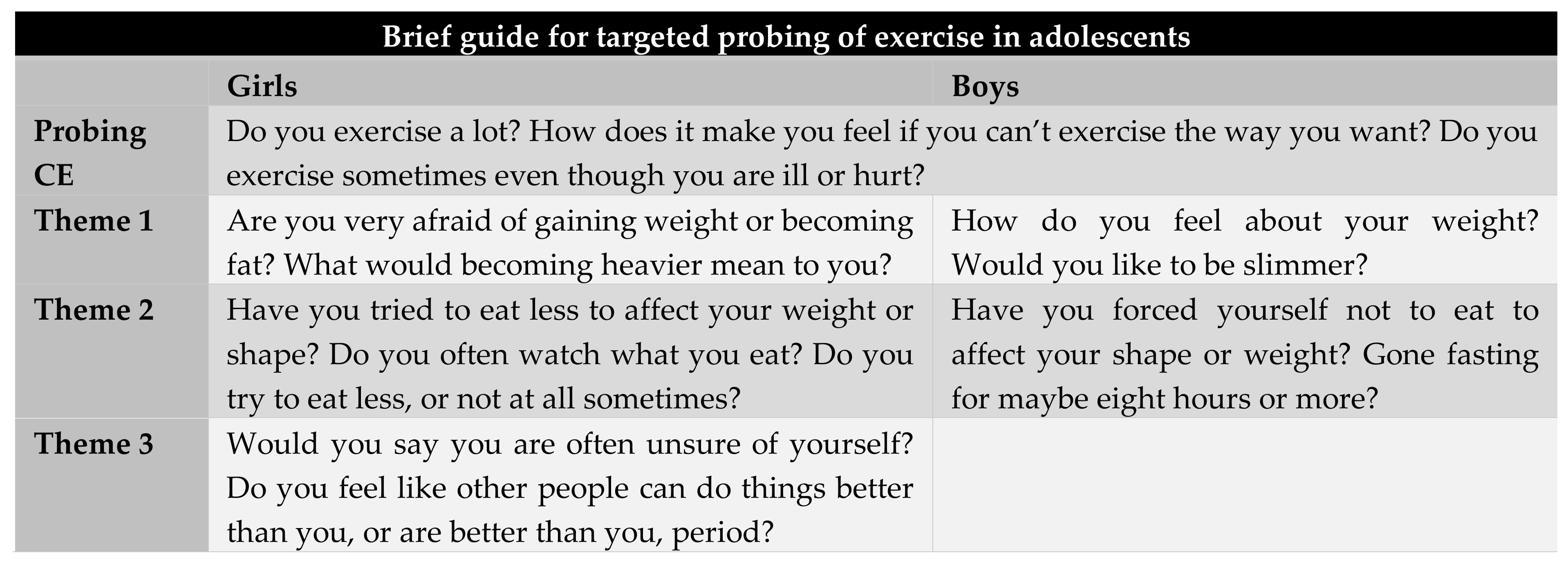
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Warburton, D.E.R.; Nicol, C.W.; Bredin, S.S.D. Health benefits of physical activity: The evidence. CMAJ 2006, 174, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Gisladottir, T.L.; Matthiasdottir, A.; Kristjandsdottir, H. The effect of adolescents’ sports clubs participation on self-reported mental and physical conditions and future expectations. J. Sports Sci. 2013, 31, 1139–1145. [Google Scholar] [CrossRef] [PubMed]
- Thorlindsson, T.; Vilhjalmson, R.; Valgeirsson, G. Sport participation and perceived health status: A study of adolecents. Soc. Sci. Med. 1990, 31, 551–556. [Google Scholar] [CrossRef]
- Allen, K.L.; Crosby, R.D.; Oddy, W.H.; Byrne, S.M. Eating disorder symptom trajectories in adolescence: Effects of time, participant sex, and early adolescent depressive symptoms. J. Eat. Disord. 2013, 1, 32. [Google Scholar] [CrossRef] [PubMed]
- Meyer, C.; Taranis, L.; Goodwin, H.; Haycraft, E. Compulsive exercise and eating disorders. Eur. Eat. Disord. Rev. 2011, 19, 174–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levallius, J.; Collin, C.; Birgegård, A. Now you see it, now you don’t: Compulsive exercise in adolescents with an eating disorder. J. Eat. Disord. 2017, 5, 9. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.; Kennedy, S.H.; Ravelski, E.; Dionne, M. The role of physical activity in the development and maintenance of eating disorders. Psychol. Med. 1994, 24, 957–967. [Google Scholar] [CrossRef] [PubMed]
- Kostrzewa, E.; Eijkemans, M.J.; Kas, M.J. The expression of excessive exercise co-segregates with the risk of developing an eating disorder in women. Psychiatry Res. 2013, 210, 1123–1128. [Google Scholar] [CrossRef] [PubMed]
- Davis, H.A.; Guller, L.; Smith, G.T. Developmental trajectories of compensatory exercise and fasting behavior across the middle school years. Appetite 2016, 107, 330–338. [Google Scholar] [CrossRef] [PubMed]
- Davis, H.A.; Guller, L.; Smith, G.T. Developmental Trajectories of Boys’ Driven Exercise and Fasting during the Middle School Years. J. Abnorm. Child Psychol. 2016b, 44, 1309–1319. [Google Scholar] [CrossRef] [PubMed]
- Wade, T.D.; O’Shea, A. DSM-5 unspecified feeding and eating disorders in adolescents: What do they look like and are they clinically significant? Int. J. Eat. Disord. 2015, 48, 367–374. [Google Scholar] [CrossRef] [PubMed]
- Stiles-Shields, E.C.; Goldschmidt, A.B.; Boepple, L.; Glunz, C.; Le Grange, D. Driven exercise among treatment-seeking youth with eating disorders. Eat. Behav. 2011, 12, 328–331. [Google Scholar] [CrossRef] [PubMed]
- Chamay-Weber, C.; Narring, F.; Michaud, P.A. Partial eating disorders among adolescents: A review. J. Adolesc. Health 2005, 37, 417–427. [Google Scholar] [CrossRef] [PubMed]
- Striegel-Moore, R.H.; Bulik, C.M. Risk factors for eating disorders. Am. Psychol. 2007, 62, 181–198. [Google Scholar] [CrossRef] [PubMed]
- Guarda, A.S. Treatment of anorexia nervosa: Insights and obstacles. Physiol. Behav. 2008, 94, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Lindstedt, K.; Neander, K.; Kjellin, L.; Gustafsson, S.A. Being me and being us—Adolescents’ experiences of treatment for eating disorders. J. Eat. Disord. 2015, 3, 9. [Google Scholar] [CrossRef] [PubMed]
- Mond, J.; Calogero, R. Compulsive exercise in eating disorder patients and in healthy women. Aust. N. Z. J. Psychiatry 2009, 43, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, H.; Haycraft, E.; Willis, A.M.; Meyer, C. Compulsive exercise: The role of personality, psychological morbidity, and disordered eating. Int. J. Eat. Disord. 2011, 44, 655–660. [Google Scholar] [CrossRef] [PubMed]
- White, J.; Halliwell, E. Examination of a sociocultural model of excessive exercise among male and female adolescents. Body Image 2010, 7, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, H.; Haycraft, E.; Meyer, C. Sociocultural risk factors for compulsive exercise: A prospective study of adolescents. Eur. Eat. Disord. Rev. 2014, 22, 360–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forsén Mantilla, E.; Bergsten, K.; Birgegård, A. Self-image and eating disorder symptoms in normal and clinical adolescents. Eat. Behav. 2014, 15, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Cash, T.F.; Grasso, K. The norms and stability of new measures of the multidimensional body image construct. Body Image 2005, 2, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Hewitt, E.L.; Flett, G.L. Perfectionism in the self and social contexts: Conceptualization, assessment, and association with psychopathology. J. Personal. Soc. Psychol. 1991, 60, 456–470. [Google Scholar] [CrossRef] [PubMed]
- Young, S.; Touyz, S.; Meyer, C.; Arcelus, J.; Rhodes, P.; Madden, S.; Pike, K.; Attia, E.; Crosby, R.D.; Wales, J.; et al. Validity of Exercise Measures in Adults with Anorexia Nervosa: The EDE, Compulsive Exercise Test and Other Self-Report Scales. Int. J. Eat. Disord. 2017, 50, 533–541. [Google Scholar] [CrossRef] [PubMed]
- Fairburn, C.G.; Beglin, S.J. Assessment of eating disorders: Interview or self-report questionnaire? Int. J. Eat. Disord. 1994, 16, 363–370. [Google Scholar] [PubMed]
- Forsén Mantilla, E.; Birgegård, A.; Clinton, D. Factor analysis of the adolescent version of the Eating Disorders Examination Questionnaire (EDE-Q): Results from Swedish general population and clinical samples. J. Eat. Disord. 2017, 5, 19. [Google Scholar] [CrossRef] [PubMed]
- Mond, J.; Hall, A.; Bentley, C.; Harrison, C.; Gratwick-Sarll, K.; Lewis, V. Eating-disordered behavior in adolescent boys: Eating disorder examination questionnaire norms. Int. J. Eat. Disord. 2013, 47, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Monell, E.; Levallius, J.; Forsén Mantilla, E.; Birgegård, A. Running on empty—A nationwide large-scale examination of compulsive exercise in eating disorders. J. Eat. Disord. In press.
- Egan, S.J.; Bodill, K.; Watson, H.J.; Valentine, E.; Shu, C.; Hagger, M.S. Compulsive exercise as mediator between clinical perfectionism and eating pathology. Eat. Behav. 2017, 24, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Lichtenstein, M.B.; Christiansen, E.; Elkit, A.; Bilenberg, N.; Stoving, R.K. Exercise addiction: A study of ED symptoms, quality of life, personality traits and attachment styles. Psychiatry Res. 2014, 215, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Taranis, L.; Meyer, C. Perfectionism and compulsive exercise among female exercisers. Personal. Ind. Differ. 2010, 49, 3–7. [Google Scholar] [CrossRef]
- Benjamin, L.S. Structural Analysis of Social Behavior. Psychol. Rev. 1974, 81, 392–425. [Google Scholar] [CrossRef]
- Björck, C.; Clinton, D.; Sohlberg, S.; Norring, C. Negative self-image and outcome in eating disorders: Results at 3-year follow-up. Eat. Behav. 2007, 8, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Karlberg, J.; Luo, Z.C.; Albertsson-Wikland, K. Body mass index reference values (mean and SD) for Swedish children. Acta Paediatr. 2001, 90, 1427–1434. [Google Scholar] [CrossRef] [PubMed]
- Carter, J.C.; Stewart, D.A.; Fairburn, C.G. Eating disorder examination questionnaire: Norms for young adolescent girls. Behav. Res. Ther. 2001, 39, 625–632. [Google Scholar] [CrossRef]
- Carter, J.C.; Aime, A.A.; Mills, J.S. Assessment of bulimia nervosa: A comparison of interview and self-report questionnaire methods. Int. J. Eat. Disord. 2001, 30, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Welch, E.; Birgegård, A.; Parling, T.; Ghaderi, A. Eating disorder examination questionnaire and clinical impairment assessment questionnaire: General population and clinical norms for young adult women in Sweden. Behav. Res. Ther. 2011, 49, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, L.S. Scientific discipline can enhance clinical effectiveness. In Reconciling Empirical Knowledge and Clinical Experience. The Art and Science of Psychotherapy; Soldz, S., McCullough, L., Eds.; American Psychological Association: Washington, DC, USA, 2000; pp. 197–219. [Google Scholar]
- Critchfield, K.L.; Benjamin, L.S. Internalized representations of early interpersonal experience and adult relationships: A test of copy process theory in clinical and non-clinical settings. Psychiatry 2008, 71, 71–92. [Google Scholar] [CrossRef] [PubMed]
- Armelius, K. Reliabilitet Och Validitet för den Svenska Versionen av SASB-Självbildstestet; Umeå Universitet: Umeå, Sweden, 2001. [Google Scholar]
- Forsén Mantilla, E.; Birgegård, A. The enemy within: The association between self-image and eating disorder symptoms in helathy, non help-seking and clinical young women. J. Eat. Disord. 2015, 3, 30. [Google Scholar] [CrossRef] [PubMed]
- Ekeroth, K.; Birgegård, A. Evaluating reliable and clinically significant change in eating disorders: Comparisons to changes in DSM-IV diagnoses. Psychiatry Res. 2014, 216, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Machado, P.P.P.; Grilo, M.G.; Crosby, R.D. Replication of a modified factor structure for the eating disorder examination questionnaire: Extension to clinical eating disorder and non-clinical samples in Portugal. Eur. Eat. Disord. Rev. 2017, 26, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Meyer, C.; Plateau, C.R.; Taranis, L.; Brewin, N.; Wales, J.; Arcelus, J. The Compulsive Exercise Test: Confirmatory factor analysis and links with eating psychopathology among women with clinical eating disorders. J. Eat. Disord. 2016, 4, 22. [Google Scholar] [CrossRef] [PubMed]
- Egan, S.J.; Wade, T.D.; Shafran, R. Perfectionism as a transdiagnostic process: A clinical review. Clin. Psychol. Rev. 2011, 31, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Grandi, S.; Clementi, C.; Guidi, J.; Benassi, M.; Tossani, E. Personality characteristics and psychological distress assiciated with primary exercise dependence: An exploratory study. Psychiatry Res. 2011, 189, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Shafran, R.; Cooper, Z.; Fairburn, C.G. Clinical perfectionism: A cognitive behavioural analysis. Behav. Res. Ther. 2002, 40, 773–791. [Google Scholar] [CrossRef]
- Vartanian, L.R.; Hayward, L.E.; Smyth, J.M.; Paxton, S.J.; Touyz, S.W. Risk and resiliency factors related to body dissatisfaction and disordered eating: The identity disruption model. Int. J. Eat. Disord. 2018, 51. [Google Scholar] [CrossRef] [PubMed]
- Vartanian, L.R.; Porter, A.M. Weight stigma and eating behavior: A review of the literature. Appetite 2016, 102, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Sundgot-Borgen, J. Prevalence of Eating Disorders in Elite Female Athletes. Int. J. Sport Nutr. 1993, 3, 29–40. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Predictor Items | Girls | Boys |
|---|---|---|
| EDE-Q | ||
| Item 1. Restraint over eating | X | |
| Item 2. Dietary restraint | X | X |
| Item 10. Flat stomach | X | |
| Item 11. Preoccupation with weight/shape | X | |
| Item 12. Fear of weight gain | X | |
| Item 13. Feelings of fatness | X | X |
| Item 14. Desire to lose weight | X | X |
| Item 15. Feelings of guilt after eating | X | |
| Item 29. Importance of weight | X | |
| Item 30. Importance of shape | X | |
| Item 32. Dissatisfaction with weight | X | X |
| Item 33. Dissatisfaction with shape | X | X |
| Item 35. Discomfort seeing body | X | X |
| Item 36. Discomfort exposing body | X | X |
| SASB | ||
| Item 7. Self-accusation, blame and guilt, bad self | X | X |
| Item 24. Vengeful of self, self-punish | X | X |
| Item 25. Self-deception, forcefully diverting self | X | X |
| Item 35. Self-doubt, putting self down | X | X |
| Predictor Variables | B | S.E. | Wald’s Χ2 | df | p | Odds Ratio |
|---|---|---|---|---|---|---|
| Girls (n = 237) | ||||||
| Constant | −0.76 | 0.16 | 21.44 | 1 | <0.001 | 0.47 |
| EDE-Q item 12. Fear of weight gain | 0.72 | 0.19 | 14.07 | 1 | <0.001 | 2.05 |
| EDE-Q item 1. Restraint over eating | 0.46 | 0.19 | 5.70 | 1 | 0.017 | 1.58 |
| SASB item 35. Self-doubt, putting self down | 0.36 | 0.17 | 4.76 | 1 | 0.029 | 1.43 |
| Model test | Χ2 | |||||
| Overall model evaluation (Likelihood ratio test) | 63.87 | 3 | <0.001 | |||
| Boys (n = 246) | ||||||
| Constant | −1.48 | 0.18 | 70.20 | 1 | <0.001 | 0.23 |
| EDE-Q item 32. Dissatisfaction with weight | 0.47 | 0.14 | 10.53 | 1 | 0.001 | 1.60 |
| EDE-Q item 2. Dietary restraint | 0.37 | 0.13 | 7.65 | 1 | 0.006 | 1.45 |
| Model test | Χ2 | |||||
| Overall model evaluation (Likelihood ratio test) | 18.80 | 2 | <0.001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Forsén Mantilla, E.; Levallius, J.; Monell, E.; Birgegård, A. Exercise Caution: Questions to Ask Adolescents Who May Exercise Too Hard. Int. J. Environ. Res. Public Health 2018, 15, 797. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15040797
Forsén Mantilla E, Levallius J, Monell E, Birgegård A. Exercise Caution: Questions to Ask Adolescents Who May Exercise Too Hard. International Journal of Environmental Research and Public Health. 2018; 15(4):797. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15040797
Chicago/Turabian StyleForsén Mantilla, Emma, Johanna Levallius, Elin Monell, and Andreas Birgegård. 2018. "Exercise Caution: Questions to Ask Adolescents Who May Exercise Too Hard" International Journal of Environmental Research and Public Health 15, no. 4: 797. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15040797