Activities of Daily Living and Determinant Factors among Older Adult Subjects with Lower Body Fracture after Discharge from Hospital: A Prospective Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Design
2.2. Selection and Sample Size of Subjects
2.3. Study Protocols
2.4. Statistical Analysis
3. Results
3.1. ADL: Frequency and Percentage of Independent or Dependent
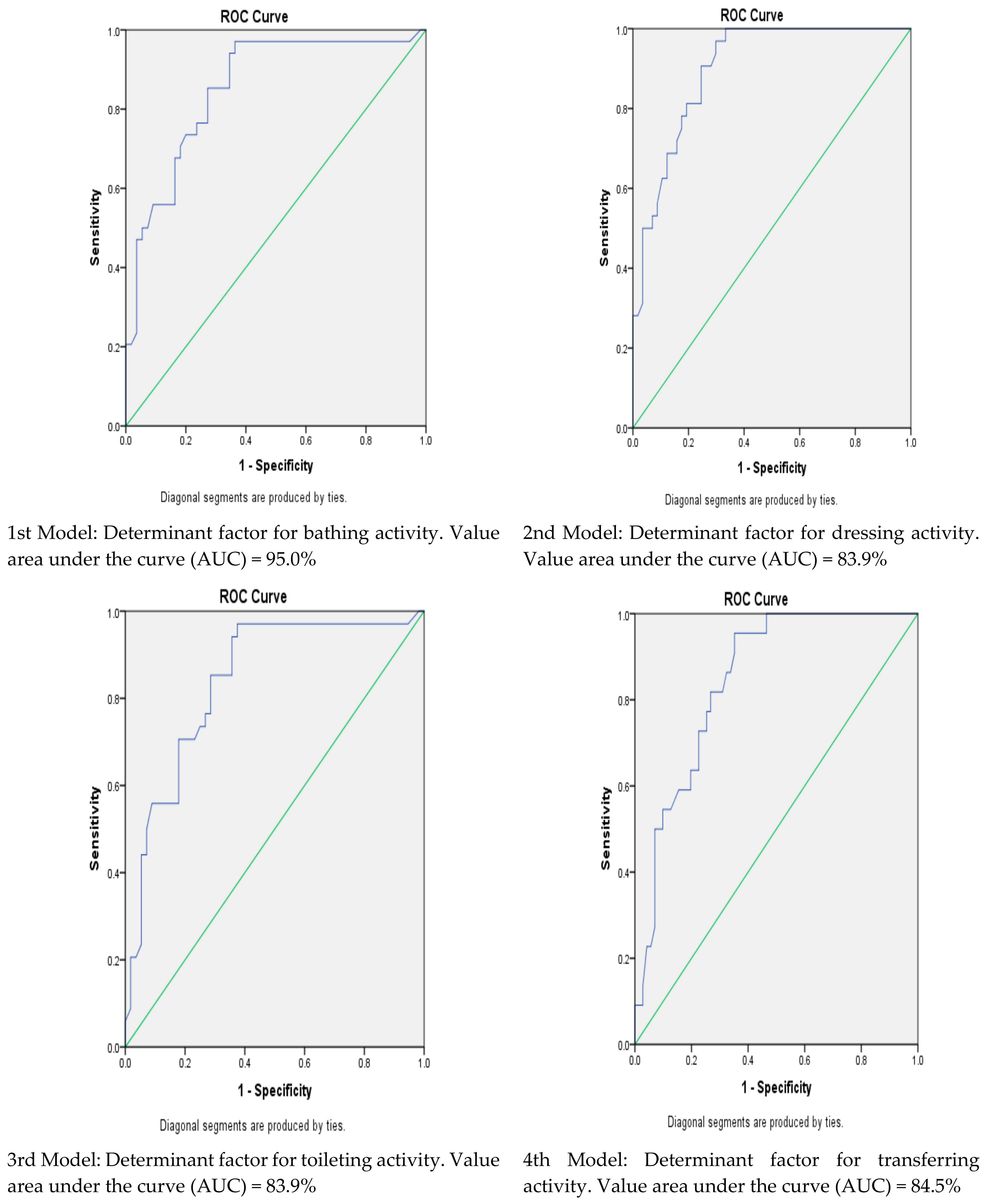
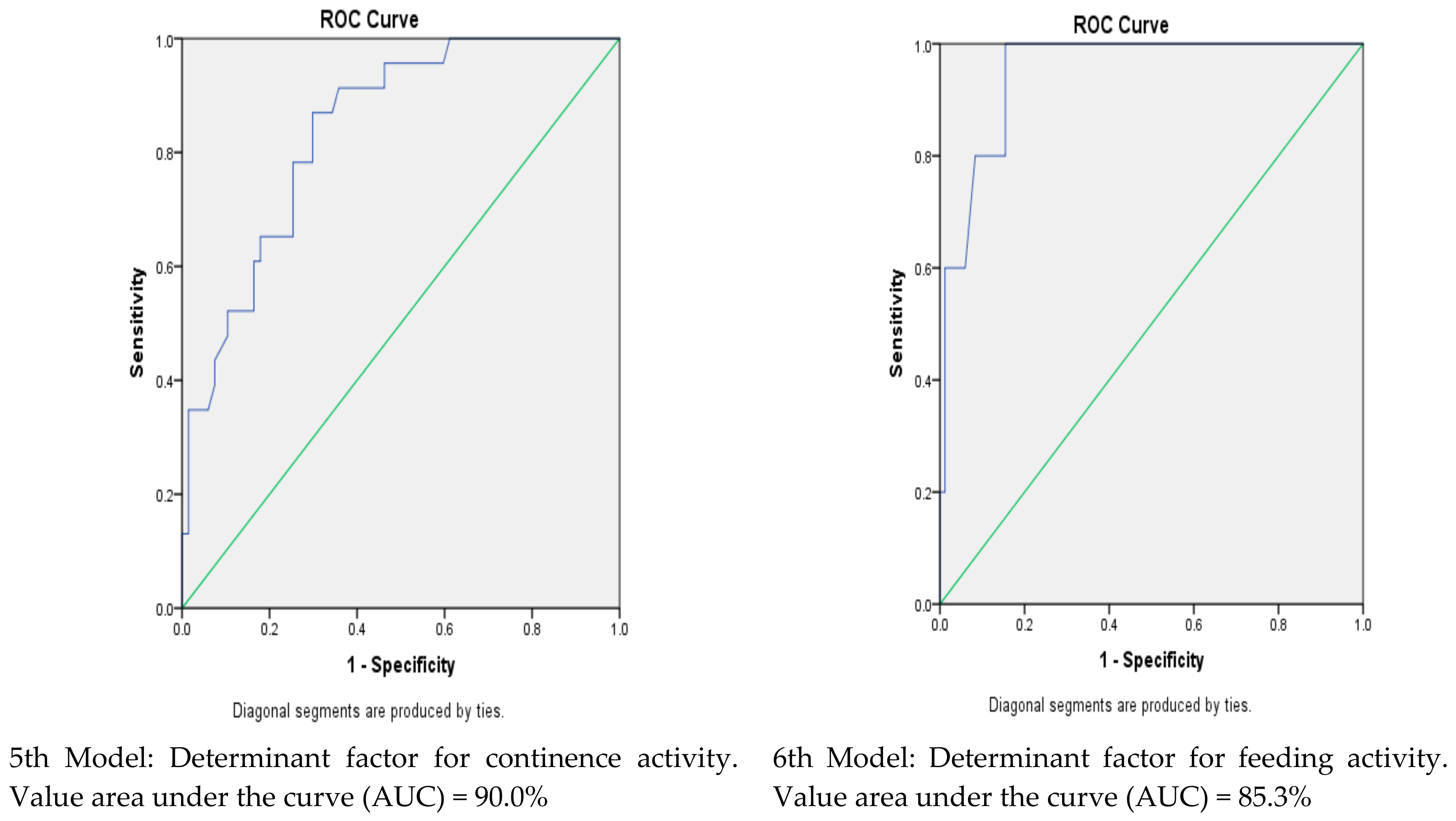
3.2. Determinant Factors Dependent for ADL at Post-Discharge Phase
3.3. Daily Life Activity Scores (ADLs) across All Three Phases of Study
3.4. ADL Score and Independent Variables (Age, Gender, Type of Fracture and Ability to Walk before Fracture)
4. Discussion
4.1. The scores of Daily Life Activity (ADL) Scale
4.2. Determinant Factors for Daily Life Activities at Post-Discharge Phase
4.3. Daily Life Activity Scores (ADLs) Across All Three Phases of Study
4.4. ADL Score and Independent Variables (Age, Gender, Type of Fracture and Ability to Walk before Fracture)
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Turło, A.; Cywińska, A.; Czopowicz, M.; Witkowski, L.; Niedźwiedź, A.; Słowikowska, M.; Borowicz, H.; Jaśkiewicz, A.; Winnicka, A. The Effect of Different Types of Musculoskeletal Injuries on Blood Concentration of Serum Amyloid A in Thoroughbred Racehorses. PLoS ONE 2015, 10, e0140673. [Google Scholar] [CrossRef] [PubMed]
- Parmet, S.; Lynm, C.; Richard, M. Bone Fractures. JAMA 2004, 291, 2160. [Google Scholar] [CrossRef] [PubMed]
- Schuit, S.C.E.; van der Klift, M.; Weel, A.E.A.M.; de Laet, C.E.D.H.; Burger, H.; Seeman, E.; Hofman, A.; Uitterlinden, A.G.; van Leeuwen, J.P.T.M.; Polsa, H.A.P. Fracture incidence and association with bone mineral density in elderly men and women: The Rotterdam Study. Bone 2004, 34, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Harvey, N.; McCloskey, E.V. Gaps and Solutions in Bone Health—A Global Framework for Improvement. World Osteoporosis Day. 2016. Available online: http://share.iofbonehealth.org/WOD/2016/thematic-report/WOD16-report-WEB-EN.pdf (accessed on 23 April 2018).
- Johnell, O.; Kanis, J.A. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos. Int. 2006, 17, 1726–1733. [Google Scholar] [CrossRef] [PubMed]
- Moayyeri, A.; Luben, R.N.; Bingham, S.A.; Welch, A.A.; Wareham, N.J.; Khaw, K.T. Measured height loss predicts fractures in middle-aged and older men and women: The EPIC-Norfolk prospective population study. J. Bone Miner. Res. 2008, 23, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Clift, B. Fractures of the Lower Limb (include Foot). 2008. Available online: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/384502/fractures_lower_limb.pdf (accessed on 23 January 2014).
- Kaye, J.A.; Jick, H. Epidemiology of lower limb fractures in general practice in the United Kingdom. Inj. Prev. 2004, 10, 368–374. [Google Scholar] [CrossRef] [PubMed]
- Jones, G.; Nguyen, T.; Sambrook, P.N.; Kelly, P.J.; Gilbert, C.; Eisman, J.A. Symptomatic fracture incidence in elderly men and women: The Dubbo Osteoporosis Epidemiology Study (DOES). Osteoporos. Int. 1994, 4, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Melton, L.J.; Crowson, C.S.; O’Fallon, W.M. Fracture incidence in Olmsted County, Minnesota: Comparison of urban with rural rates and changes in urban rates over time. Osteoporos. Int. 1999, 9, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Miller, W. Survival and ambulation following hip fracture. J. Bone Jt. Surg. Am. 1978, 60, 930–934. [Google Scholar] [CrossRef]
- Cummings, S.R.; Kelsey, J.L.; Nevitt, M.C.; O’Dowd, K.J. Epidemiology of osteoporosis and osteoporotic fractures. Epidemiol. Rev. 1985, 7, 178–208. [Google Scholar] [CrossRef] [PubMed]
- Jensen, J.S.; Bagger, J. Long-term social prognosis after hip fractures. Acta Orthop. Scand. 1982, 53, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Cummings, S.R.; Melton, L.J. Epidemiology and outcomes of osteoporotic fractures. Lancet 2002, 359, 1761–1767. [Google Scholar] [CrossRef]
- Colón-Emeric, C.S.; Saag, K.G. Osteoporotic fractures in older adults. Best Pract. Res. Clin. Rheumatol. 2006, 20, 695–706. [Google Scholar] [CrossRef] [PubMed]
- Haentjens, P.; Lamraski, G.; Boonen, S. Costs and consequences of hip fracture occurrence in old age: An economic perspective. Disabil. Rehabil. 2005, 27, 1129–1141. [Google Scholar] [CrossRef] [PubMed]
- Wiktorowicz, M.E.; Goeree, R.; Papaioannou, A.; Adachi, J.D.; Papadimitropoulos, E. Economic implications of hip fracture: Health service use, institutional care and cost in Canada. Osteoporos. Int. 2001, 12, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Bouee, S.; Lafuma, A.; Fagnani, F.; Meunier, P.J.; Reginster, J.Y. Estimation of direct unit costs associated with non-vertebral osteoporotic fractures in five European countries. Rheumatol. Int. 2006, 26, 1063–1072. [Google Scholar] [CrossRef] [PubMed]
- Colon-Emeric, C.S. Postoperative management of hip fractures: Interventions associated with improved outcomes. BoneKEy Rep. 2012, 241. [Google Scholar] [CrossRef] [PubMed]
- Safa, A.; Alavi, N.M.; Abedzadeh-Kalahroudi, M. Predictive Factors of Dependency in Activities of Daily Living Following Limb Trauma in the Elderly. Trauma Mon. 2016, 21, e25091. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.; Boling, J.; Manson, M.; Owens, T.; Zura, R. Relation between prefracture characteristics and perioperative complications in the elderly adult patient with hip fracture. South. Med. J. 2012, 105, 306–310. [Google Scholar] [CrossRef] [PubMed]
- Vochteloo, A.J.H.; Moerman, S.; Tuinebreijer, W.E.; Maier, A.B.; de Vries, M.R.; Bloem, R.M.; Nelissen, R.G.; Pilot, P. More than half of hip fracture patients do not regain mobility in the first postoperative year. Geriatr. Gerontol. Int. 2013, 13, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Colon-Emeric, C.; Kuchibhatla, M.; Pieper, C.; Hawkes, W.; Fredman, L.; Magaziner, J.; Zimmerman, S.; Lyles, K.W. The contribution of hip fracture to risk of subsequent fractures: Data from two longitudinal studies. Osteoporos. Int. 2003, 14, 879–883. [Google Scholar] [CrossRef] [PubMed]
- Green, S.B. How many subjects does it take to do a regression analysis? Multivar. Behav. Res. 1991, 26, 499–510. [Google Scholar] [CrossRef] [PubMed]
- Duca, G.F.P.; Da Silva, M.C.; Hallal, P.C. Disability in relation to basic and instrumental activities of daily living among elderly subjects. Revista de Saúde Pública 2009, 43, 1–9. [Google Scholar]
- Sharkawi, M.A.; Zulfarina, S.M.; Aqilah-SN, S.M.Z.; Isa, N.M.; Sabarul, A.M.; Nazrun, A.S. Systematic Review on the Functional Status of Elderly Hip Fracture Patients using Katz Index of Activity of Daily Living (Katz ADL) Score. IMJM 2016, 15, 89–99. [Google Scholar]
- Yu, R.; Wong, M.; Chang, B.; Lai, X.; Lum, C.M.; Auyeung, T.W.; Lee, Y.; Tsoi, K.; Lee, R.; Woo, J. Trends in activities of daily living disability in a large sample of community-dwelling Chinese older adults in Hong Kong: An age-period-cohort analysis. BMJ Open 2016, 6, 1–9. [Google Scholar]
- Al Aqqad, S.H.; Chen, L.L.; Shafie, A.A.; Hassali, M.A.; Tangiisuran, B. The use of potentially inappropriate medications and changes in quality of life among older nursing home residents. Clin. Interv. Aging 2014, 9, 201–207. [Google Scholar] [PubMed]
- Wallace, M.; Shelkey, M. Katz Index of Independence in Activities of Daily Living (ADL). AJN 2008, 108, 67–71. [Google Scholar]
- Garcia, R.; Leme, M.D.; Garcez-Leme, L.E. Evolution of Brazilian Elderly with Hip Fracture Secondary to a Fall. CLINICS 2006, 61, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Reijneveld, S.A.; Spijker, J.; Dijkshoorn, H. Katz’ADL index assessed functional performance of Turkish, Moroccan, and Dutch elderly. J. Clin. Epidemiol. 2007, 60, 382–388. [Google Scholar] [CrossRef] [PubMed]
- Katz, S.; Down, T.D.; Cash, H.R.; Grotza, R.C. Progress in the Development of the Index of ADL. Gerontologist 1970, 10, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Zweig, M.H.; Campbell, G. Receiver-operating characteristic (ROC) plots: A fundamental evaluation tool in clinical medicine. Clin. Chem. 1993, 39, 561–577. [Google Scholar] [PubMed]
- Gold, D.A. An examination of instrumental activities of daily living assessment in older adults and mild cognitive impairment. J. Clin. Exp. Neuropsychol. 2012, 34, 11–34. [Google Scholar] [CrossRef] [PubMed]
- Wallace, M.; Shelkey, M. Katz Index of Independence in Activities of Daily Living. J. Gerontol. Nurs. 1999, 25, 8–9. [Google Scholar]
- Wallace, M.; Shelkey, M. Katz Index of Independence in Activities of Daily Living (ADL); The Hartford Institute for Geriatric Nursing, New York University, College of Nursing: New York, NY, USA, 2012. [Google Scholar]
- Wiener, J.M.; Hanley, R.J. Measuring the Activities of Daily Living among the Elderly: A Guide to National Surveys. 1989. Available online: https://aspe.hhs.gov/basic-report/measuring-activities-daily-living-among-elderly-guide-national-surveys (accessed on 25 December 2016).
- Puteh, S.E.B.W.; Bakar, I.M.A.; Borhanuddin, B.; Latiff, K.; Amin, R.M.; Sutan, R. A Prevalence Study of the Activities of Daily Living (ADL) Dependency among the Elderly in Four Districts in Selangor, Malaysia. J. Epidemiol. Prev. Med. 2015, 1, 1–8. [Google Scholar] [CrossRef]
- Tang, Z.; Wang, H.; Meng, C.; Wu, X.; Ericsson, K.; Winblad, B.; Pei, J. The prevalence of functional disability in activities of daily living and instrumental activities of daily living among elderly Beijing Chinese. Arch. Gerontol. Geriatr. 1999, 29, 115–125. [Google Scholar] [CrossRef]
- Matthews, C.A.; Whitehead, W.E.; Townsend, M.K.; Grodstein, F. Risk Factors for Urinary, Fecal or Dual Incontinence in the Nurses’ Health Study. Obstet. Gynecol. 2013, 122, 539–545. [Google Scholar] [CrossRef] [PubMed]
- Alavi, N.M.; Safa, A.; Abedzadeh-Kalahroudi, M. Dependency in Activities of Daily Living Following Limb Trauma in Elderly Referred to Shahid Beheshti Hospital, Kashan-Iran in 2013. Arch. Trauma Res. 2014, 3, e20608. [Google Scholar]
- Mossey, J.M.; Mutran, E.; Knott, K.; Craik, R. Determinants of Recovery 12 months after hip fracture: The importance of Psychosocial factors. Am. J. Public Health 1989, 79, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Kelsey, J.L.; Samelson, E.J. Variation in Risk Factors for Fractures at Different Sites. Curr. Osteoporos. Rep. 2009, 7, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Curry, L.C.; Hogstel, M.O.; Davis, G.C. Functional status in older women following hip fracture. J. Adv. Nurs. 2003, 42, 347–354. [Google Scholar] [CrossRef] [PubMed]
- Svensson, O.; Stromberg, L.; Ohlen, G.; Lindgren, U. Prediction of the outcome after hip fracture in elderly patients. J. Bone Jt. Surg. Br. 1996, 78, 115–118. [Google Scholar] [CrossRef]
- Mehul, R.S.; Gina, B.A.; Philip, W.; Joseph, D.Z.; Kenneth, J.K. Outcome after Hip fracture in individuals Ninety years of Age and Older. J. Orthop. Trauma 2001, 15, 34–39. [Google Scholar]
- Wollinsky, F.D.; Fitzgerald, J.F.; Stump, E.S. The Effect of Hip Fracture on Mortality, Hospitalization, and Functional Status: A Prospective Study. Am. J. Public Health 1997, 87, 398–403. [Google Scholar] [CrossRef]
- Alarcon, T.; Gonzalez-Montalvo, J.I.; Gotor, P.; Madero, R.; Otero, A. Activities of daily living after hip fracture: Profile and rate of recovery during 2 years of follow-up. Osteoporos. Int. 2011, 22, 1609–1613. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, G.I.; Hastie, C.L.; Morris, J.N.; Fries, B.E.; Ankri, J. Measuring change in activities of daily living in nursing home residents with moderate to severe cognitive impairment. BMC Geriatr. 2006, 6, 7. [Google Scholar] [CrossRef] [PubMed]
- Magaziner, J.; Hawkes, W.; Hebel, J.R.; Zimmerman, S.I.; Fox, K.M.; Dolan, M.; Felsenthal, G.; Kenzora, J. Recovery from hip fracture in eight areas of function. J. Gerontol. Med. Sci. 2000, 55, M498–M507. [Google Scholar] [CrossRef]
- Riemen, A.H.K.; Hutchison, J.D. The multidisciplinary management of hip fractures in older patients. Orthop. Trauma 2016, 30, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Karbakhshe, M.; Zargar, M.; Ershadi, Z.; Khaji, A. Mechanism and outcome of hip fracture: A multi-center study. Tehran Univ. Med. J. 2006, 64, 37–46. [Google Scholar]
- Mobaleghi, J.; NotashAidin, Y.; Notash Ali, Y.; Ahmadi Amoli, H.; Borna, L.; NotashAnaram, Y. Evaluation of trauma patterns and their related factors in Besat Hospital in Sanandaj in 2012. Sci. J. Kurdistan Univ. Med. Sci. 2014, 19, 99–107. [Google Scholar]
- Yu, B.; Chung, M.; Lee, G.; Lee, J. Mortality and Morbidity in Severely Traumatized Elderly Patients. Korean J. Crit. Care Med. 2014, 29, 88–92. [Google Scholar] [CrossRef]
- Kara, H.; Bayir, A.; Ak, A.; Akinci, M.; Tufekci, N.; Degirmenci, S. Trauma in elderly patients evaluated in a hospital emergency department in Konya, Turkey: A retrospective study. Clin. Interv. Aging 2014, 9, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Povoroznyuk, V.; Dedukh, N.; Makogonchuk, A. Effect of aging on fracture healing. Gerontologija 2014, 15, 97–102. [Google Scholar]
- Meyer, M.; Meyer, R., Jr. Altered expression of mitochondrial genes in response to fracture in old rats. Acta Orthop. 2006, 77, 944–951. [Google Scholar] [CrossRef] [PubMed]
- Nitti, V.W. The Prevalence of Urinary Incontinence. Rev. Urol. 2002, 3, S2–S6. [Google Scholar]
- Stenzelius, K.; Mattiasson, A.; Hallberg, I.R.; Westergren, A. Symptoms of urinary and faecal incontinence among men and women 75+ in relations to health complaints and quality of life. Neurourol. Urodyn. 2004, 23, 211–222. [Google Scholar] [CrossRef] [PubMed]
- Bertram, M.; Norman, R.; Kemp, L.; Vos, T. Review of the long-term disability associated with hip fractures. Inj. Prev. 2011, 17, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Flikweert, E.R.; Izaks, G.J.; Reininga, I.H.; Wendt, K.W.; Stevens, M. Evaluation of the effect of a comprehensive multidisciplinary care pathway for hip fractures: Design of a controlled study. BMC Musculoskelet. Disord. 2013, 14, 291. [Google Scholar] [CrossRef] [PubMed]
- Norton, R.; Butler, M.; Robinson, E.; Lee-Joe, T.; Campbell, A.J. Declines in physical functioning attributable to hip fracture among older people: A follow-up study of case–control participants. Disabil. Rehabil. 2000, 22, 345–351. [Google Scholar] [PubMed]
- Mariconda, M.; Costa, G.G.; Recano, P.; Orabona, G.; Gambacorta, M.; Misasi, M. Factors Predicting Mobility and the Change in Activities of Daily Living After Hip Fracture: A 1-Year Prospective Cohort Study. J. Orthop. Trauma 2016, 30, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Hu, G.; Hsu, C.; Hsieh, S.; Li, C. Assessment of Individual Activities of Daily Living and its Association with Self-Rated Health in Elderly People of Taiwan. Int. J. Gerontol. 2012, 6, 117–121. [Google Scholar] [CrossRef]
- Inagawa, T.; Hamagishi, T.; Takaso, Y.; Hitomi, Y.; Kambayashi, Y.; Hibino, Y.; Shibata, A.; Ngoc, N.T.M.; Okochi, J.; Hatta, K.; et al. Decreased activity of daily living produced by the combination of Alzheimer’s disease and lower limb fracture in elderly requiring nursing care. Environ. Health Prev. Med. 2013, 18, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Heikkinen, T.; Jalovaara, P. Four or Twelve Months Follow-Up in the Evaluation of functional Outcome After Hip fracture Surgery? Scand. J. Surg. 2005, 94, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Takayama, S.; Iki, M.; Kusaka, Y.; Takagi, H.; Tamaki, S. Factors that influence functional prognosis in elderly patients with hip fracture. Environ. Health Prev. Med. 2001, 6, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Koval, K.J.; Skovron, M.L.; Aharonoff, G.B.; Zuckerman, J.D. Predictors of functional recovery after hip fracture in the elderly. Clin. Orthop. Relat. Res. 1998, 348, 22–28. [Google Scholar] [CrossRef]
- Al-Ani, A.; Neander, G.; Samuelsson, B.; Blomfeldt, R.; Ekstrom, W.; Hedstrom, M. Risk factors for osteoporosis are common in young and middle-aged patients with femoral neck fractures regardless of trauma mechanism. Acta Orthop. 2013, 84, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Alegre-López, J.; Cordero-Guevara, J.; Alonso-Valdivielso, J.L.; Fernández-Melón, J. Factors associated with mortality and functional disability after hip fracture: An inception cohort study. Osteoporos. Int. 2005, 16, 729–736. [Google Scholar] [CrossRef] [PubMed]
- Orive, M.; Aguirre, U.; Garcia-Gutierrez, S.; Las Hayas, C.; Bilbao, A.; Gonzalez, N.; Zabala, J.; Navarro, G.; Quintana, J.M. Changes in health-related quality of life and activities of daily living after hip fracture because of a fall in elderly patients: A prospective cohort study. Int. J. Clin. Pract. 2015, 69, 491–500. [Google Scholar] [CrossRef] [PubMed]
- Sylliaas, H.; Thingstad, P.; Wyller, T.B.; Helbostad, J.; Sletvold, O.; Bergland, A. Prognostic factors for self-rated function and perceived health in patient living at home three months after a hip fracture. Disabil. Rehabil. 2012, 34, 1225–1231. [Google Scholar] [CrossRef] [PubMed]
- Dudkiewicz, I.; Burg, A.; Salai, M.; Hershkovitz, A.I. Gender differences among patients with proximal femur fractures during rehabilitation. Gend. Med. 2011, 8, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Samuelsson, B.; Hedström, M.I.; Ponzer, S.; Söderqvist, A.; Samnegård, E.; Thorngren, K.G.; Cederholm, T.; Sääf, M.; Dalen, N. Gender differences and cognitive aspects on functional outcome after hip fracture—A 2 years’ follow-up of 2134 patients. Age Ageing 2009, 38, 686–692. [Google Scholar] [CrossRef] [PubMed]
- Solarino, G.; Vicenti, G.; Picca, G.; Rifino, F.; Carrozzo, M.; Moretti, B. A review of gender differences in hip fracture anatomy, morbidity, mortality and function. Ital. J. Gend.-Specif. Med. 2016, 2, 55–59. [Google Scholar]
- Kempen, G.I.J.M.; Sanderman, R.; Scaf-Klomp, W.; Ormel, J. Gender differences in recovery from injuries to the extremities in older persons. A prospective study. Disabil. Rehabil. 2003, 25, 827–832. [Google Scholar] [CrossRef] [PubMed]
- Gill, T.M.; Murphy, T.E.; Gahbauer, E.A.; Allore, H.G. The course of disability before and after a serious fall injury. JAMA Intern. Med. 2013, 173, 1780–1786. [Google Scholar] [CrossRef] [PubMed]
- Vergara, I.; Vrotsou, K.; Orive, M.; Gonzalez, N.; Garcia, S.; Quintana, J.M. Factors related to functional prognosis in elderly patients after accidental hip fractures: A prospective cohort study. BMC Geriatr. 2014, 14, 124. [Google Scholar] [CrossRef] [PubMed]
- Ganezak, M.; Chrobrowski, K.; Korzen, M. Predictors of a Change and Correlation in Activities of Daily Living after Hip Fracture in Elderly Patients in a Community Hospital in Poland: A Six-Month Prospective Cohort Study. Int. J. Environ. Res. Public Health 2018, 15, 95. [Google Scholar] [CrossRef] [PubMed]
- Dyer, S.M.; Crotty, M.; Fairhall, N.; Magaziner, J.; Beaupre, L.A.; Cameron, I.D.; Sherrington, C. A critical review of the long-term disability outcomes following hip fracture. BMC Geriatr. 2016, 16, 158. [Google Scholar] [CrossRef] [PubMed]
- Theander, E.; Jarnlo, G.; Ornstein, E.; Karlsson, M.K. Activities of daily living similarly in hospital-treated patients with a hip fracture or a vertebral fracture: A one-year prospective study in 151 patients. Scand. J. Public Health 2004, 32, 356–360. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, M.T. Factors affecting functional prognosis of patients with hip fracture. Eur. J. Phys. Rehabil. Med. 2011, 47, 257–264. [Google Scholar] [PubMed]
- Montalban-Quesada, S.; Garcia-Garcia, I.; Moreno-Lorenzo, C. Functional evolution in elderly individuals with hip fracture surgery. Revista da Escola de Enfermagem da USP 2012, 46, 1095–1100. [Google Scholar]
- Lin, P.C.; Chang, S.Y. Functional recovery among elderly people one year after hip fracture surgery. J. Nurs. Res. 2004, 12, 72–82. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, A.; Berggren, M.; Gustafson, Y.; Olofsson, B.; Lindelöf, N.; Stenvall, M. Effects of Geriatric Interdisciplinary Home Rehabilitation on Walking Ability and Length of Hospital Stay After Hip Fracture: A Randomized Controlled Trial. JAMDA 2016, 17, 464.e9–464.e15. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Demographic Profile | Ward Admission Phase n = 129 N (%) | Post Discharge Phase n = 89 N (%) |
|---|---|---|
| Age (mean ± SD) | 71.29 ± 10.94 | 69.62 ± 10.68 |
| Age group | ||
| 50–64 | 39 (30.2) | 32 (36.0) |
| 65–74 | 29 (22.5) | 19 (21.3) |
| 75–84 | 45 (34.9) | 32 (36.0) |
| >84 | 16 (12.4) | 6 (6.7) |
| Ethnic/Race | ||
| Malay | 48 (37.2) | 33 (37.1) |
| Chinese | 59 (45.7) | 45 (50.6) |
| Indian | 22 (17.1) | 11 (12.4) |
| Gender | ||
| Male | 50 (38.8) | 34 (38.2) |
| Female | 79 (61.2) | 55 (61.8) |
| Anatomy of fracture parts | ||
| Hip and femur | 84 (65.1) | 51 (57.3) |
| Knees and calves | 23 (17.8) | 18 (20.2) |
| Ankle and foot | 22 (17.1) | 20 (22.5) |
| Fracture type | ||
| Hip bone | 78 (60.5) | 46 (51.7) |
| Other than hip bone | 51 (39.5) | 43 (48.3) |
| Ability to walk before fracture | ||
| Without walking aid | 97 (75.2) | 22 (24.7) |
| With walking aid | 32 (24.8) | 67 (75.3) |
| Follow-Up Status | Frequency, N | Percentage (%) |
|---|---|---|
| Successful for follow-up visit | 89 | 69.0 |
| Died | 14 | 10.9 |
| Withdraw from the study | 15 | 11.6 |
| Uncontactable | 11 | 8.5 |
| ADL Scales | Pre-Fracture Phase n = 129 N (%) | Ward Admission Phase n = 129 N (%) | Post-Discharge Phase n = 89 N (%) |
|---|---|---|---|
| Bathing | |||
| Independent | 128 (99.2) | 2 (1.6) | 55 (61.8) |
| Dependent | 1 (0.8) | 127 (98.4) | 34 (38.2) |
| Dressing | |||
| Independent | 128 (99.2) | 14 (10.9) | 57 (64.0) |
| Dependent | 1 (0.8) | 115 (89.1) | 32 (36.0) |
| Transferring | |||
| Independent | 128 (99.2) | 12 (9.3) | 67 (75.3) |
| Dependent | 1 (0.8) | 117 (90.7) | 22 (24.7) |
| Toileting | |||
| Independent | 128 (99.2) | 3 (2.3) | 55 (61.8) |
| Dependent | 1 (0.8) | 126 (97.7) | 34 (38.2) |
| Continence | |||
| Independent | 113 (87.6) | 22 (17.1) | 66 (74.2) |
| Dependent | 16 (12.4) | 107 (82.9) | 23 (25.8) |
| Feeding | |||
| Independent | 129 (100.0) | 110 (85.3) | 84 (94.4) |
| Dependent | 0 (0.0) | 19 (14.7) | 5 (5.6) |
| (a) Logistic Regression for Bathing Activity | |||
|---|---|---|---|
| Determinant Factors | Logistic Regression | ||
| 95% CI | Odd Ratio (OR) | p-Value | |
| Age | 1.005 to 1.156 | 1.078 | 0.036 |
| Gender | |||
| Male | 0.538 to 5.792 | 1.765 | 0.349 |
| Female (R) | |||
| Type of fracture | |||
| Hip fracture | 0.693 to 9.196 | 2.524 | 0.160 |
| Non-hip fracture (R) | |||
| Ability to walk before the fracture | |||
| Walking aid | |||
| Without walking aid (R) | 1.688 to 20.383 | 5.866 | 0.005 |
| (b) Logistic Regression for Dressing Activity | |||
| Determinant Factors | Logistic Regression | ||
| 95% CI | Odd Ratio (OR) | p-Value | |
| Age | 1.037 to 1.227 | 11.233 | 0.001 |
| Gender | |||
| Male | 0.360 to 4.950 | 1.335 | 0.665 |
| Female (R) | |||
| Type of fracture | |||
| Hip fracture | 0.464 to 8.607 | 1.999 | 0.352 |
| Non-hip fracture (R) | |||
| Ability to walk before the fracture | |||
| Walking aid | |||
| Without walking aid (R) | 2.801 to 45.047 | 11.233 | 0.001 |
| (c) Logistic Regression for Transferring Activity | |||
| Determinant Factors | Logistic Regression | ||
| 95% CI | Odd Ratio (OR) | p-Value | |
| Age | 0.999 to 1.176 | 1.084 | 0.053 |
| Gender | |||
| Male | 0.539 to 8.035 | 2.082 | 0.287 |
| Female (R) | |||
| Type of fracture | |||
| Hip fracture | |||
| Non-hip fracture (R) | 0.558 to 13.089 | 2.702 | 0.217 |
| Ability to walk before the fracture | |||
| Walking aid | |||
| Without walking aid (R) | 1.147 to 11.843 | 3.684 | 0.029 |
| (d) Logistic Regression for Toileting Activity | |||
| Determinant Factors | Logistic Regression | ||
| 95% CI | Odd Ratio (OR) | p-Value | |
| Age | 1.022 to 1.149 | 1.073 | 0.043 |
| Gender | |||
| Male | 0.506 to 5.123 | 1.610 | 0.420 |
| Female (R) | |||
| Type of fracture | |||
| Hip fracture | |||
| Non-hip fracture (R) | 0.678 to 8.554 | 2.408 | 0.174 |
| Ability to walk before the fracture | |||
| Walking aid | |||
| Without walking aid (R) | 1.420 to 15.032 | 4.620 | 0.011 |
| (e) Logistic Regression for Continence Activity | |||
| Determinant Factors | Logistic Regression | ||
| 95% CI | Odd Ratio (OR) | p-Value | |
| Age | 1.024 to 1.220 | 1.118 | 0.013 |
| Gender | |||
| Male | 1.050 to 18.046 | 4.354 | 0.043 |
| Female (R) | |||
| Type of fracture | |||
| Hip fracture | 0.249 to 4.876 | 1.102 | 1.102 |
| Non-hip fracture (R) | |||
| Ability to walk before the fracture | |||
| Walking aid | |||
| Without walking aid (R) | 0.705 to 7.596 | 2.313 | 0.167 |
| (f) Logistic Regression for Feeding Activity | |||
| Determinant Factors | Logistic Regression | ||
| 95% CI | Odd Ratio (OR) | p-Value | |
| Age | 1.057 to 1.841 | 1.395 | 0.019 |
| Gender | |||
| Male | |||
| Female (R) | 0.044 to 9.734 | 0.657 | 0.760 |
| Type of fracture | |||
| Hip fracture | |||
| Non-hip fracture (R) | 0.013 to 9.863 | 0.363 | 0.548 |
| Ability to walk before the fracture | |||
| Walking aid | |||
| Without walking aid (R) | 0.840 to 199.860 | 12.955 | 0.067 |
| ADL Score | Pre-Fracture Phase n = 129 | Ward Phase n = 129 | Post-Discharge Phase n = 89 |
|---|---|---|---|
| Minimum | 3 | 0 | 0 |
| Maximum | 6 | 6 | 6 |
| Mean | 5.85 | 1.28 | 4.33 |
| Phases | ADL Score Median (IQR) | p-Value |
|---|---|---|
| Pre-fracture phase, n = 129 | 6 (0) | 0.000 |
| Ward phase, n = 129 | 1 (0) | |
| Post-discharge phase, n = 89 | 6 (4) |
| Independent Variables | Median (IQR) | p-Value |
|---|---|---|
| Age | ||
| 50–64 | 6 (0) | |
| >65 | 3 (5) | 0.000 |
| Gender | ||
| Male | 6(1) | |
| Female | 6 (5) | 0.021 |
| Fracture type | ||
| Hip fracture | 3 (5) | |
| Non-hip fracture | 6 (0) | 0.000 |
| Ability to walk before fracture | ||
| Using walking aid | 2 (3) | |
| Not using walking aid | 6 (2) | 0.000 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ibrahim, N.I.; Ahmad, M.S.; Zulfarina, M.S.; Zaris, S.N.A.S.M.; Mohamed, I.N.; Mohamed, N.; Mokhtar, S.A.; Shuid, A.N. Activities of Daily Living and Determinant Factors among Older Adult Subjects with Lower Body Fracture after Discharge from Hospital: A Prospective Study. Int. J. Environ. Res. Public Health 2018, 15, 1002. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15051002
Ibrahim NI, Ahmad MS, Zulfarina MS, Zaris SNASM, Mohamed IN, Mohamed N, Mokhtar SA, Shuid AN. Activities of Daily Living and Determinant Factors among Older Adult Subjects with Lower Body Fracture after Discharge from Hospital: A Prospective Study. International Journal of Environmental Research and Public Health. 2018; 15(5):1002. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15051002
Chicago/Turabian StyleIbrahim, Nurul Izzah, Mohd Sharkawi Ahmad, Mohamed S Zulfarina, Sharifah Nurul Aqilah Sayed Mohd Zaris, Isa Naina Mohamed, Norazlina Mohamed, Sabarul Afian Mokhtar, and Ahmad Nazrun Shuid. 2018. "Activities of Daily Living and Determinant Factors among Older Adult Subjects with Lower Body Fracture after Discharge from Hospital: A Prospective Study" International Journal of Environmental Research and Public Health 15, no. 5: 1002. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15051002