Measuring Cortisol in the Classroom with School-Aged Children—A Systematic Review and Recommendations


Abstract
:1. Introduction
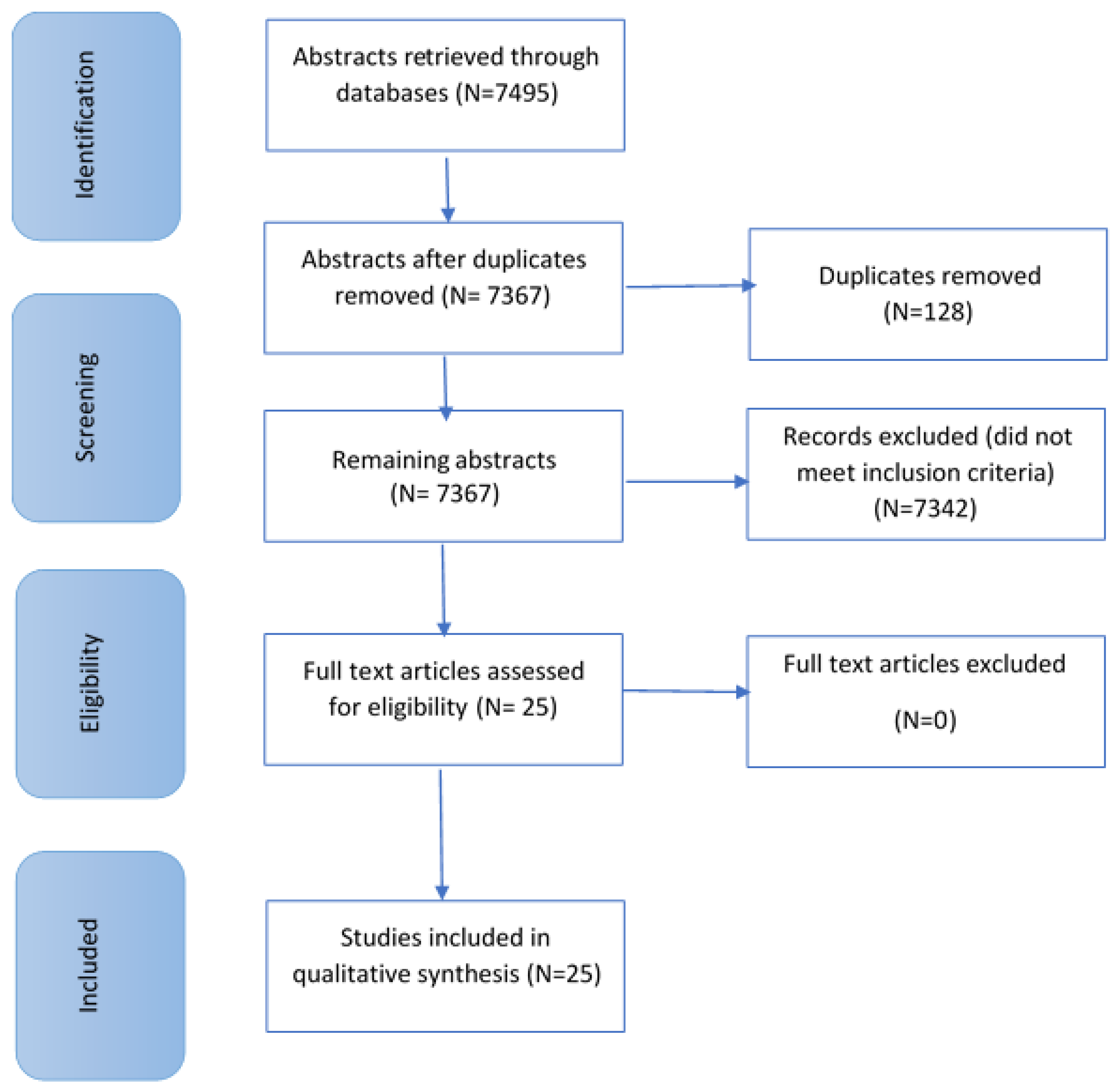
2. Materials and Methods
3. Results
3.1. Diurnal Measure of Cortisol
3.2. Measuring Intervention Effects on Cortisol Levels
3.3. Baseline Measure
3.4. Cortisol as an Acute Measure
4. Discussion
5. Recommendations for Future Research
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Palma, S.M.M.; Fernandes, D.R.M.; Muszkat, M.; Calil, H.M. The response to stress in Brazilian children and adolescents with attention deficit hyperactivity disorder. Psychiatry Res. 2012, 198, 477–481. [Google Scholar] [CrossRef] [PubMed]
- Palma, S.M.; Natale, A.M.P.; Maria Calil, H. A four-year follow-up controlled study of stress response and symptom persistence in Brazilian children and adolescents with attention deficit disorder and hyperactivity (ADHD). Psychiatry Res. 2015, 230, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Gabriels, R.L.; Agnew, J.A.; Pan, Z.; Holt, K.D.; Reynolds, A.; Laudenslager, M.L. Elevated repetitive behaviors are associated with lower diurnal salivary cortisol levels in autism spectrum disorder. Biol. Psychol. 2013, 93, 262–268. [Google Scholar] [CrossRef] [PubMed]
- Beetz, A.; Kotrschal, K.; Turner, D.C.; Hediger, K.; Uvnäs-Moberg, K.; Julius, H. The effect of a real dog, toy dog and friendly person on insecurely attached children during a stressful task: An exploratory study. Anthrozoös 2011, 24, 349–368. [Google Scholar] [CrossRef]
- Beetz, A.; Julius, H.; Turner, D.; Kotrschal, K. Effects of social support by a dog on stress modulation in male children with insecure attachment. Front. Psychol. 2012, 3, 352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schonert-Reichl, K.; Oberle, E.; Lawlor, M.S.; Abbott, D.; Thomson, K.; Oberlander, T.F.; Diamond, A. Enhancing cognitive and social-emotional development through a simple-to-administer mindfulness-based school program for elementary school children: A randomized controlled trial. Dev. Psychol. 2015, 51, 52–66. [Google Scholar] [CrossRef] [PubMed]
- Butzer, B.; Day, D.; Potts, A.; Ryan, C.; Coulombe, S.; Davies, B.; Weidknecht, K.; Ebert, M.; Flynn, L.; Khalsa, S.B.S. Effects of a classroom-based yoga intervention on cortisol and behaviour in second- and third-grade students: A pilot study. J. Evid.-Based Compliment. Altern. Med. 2015, 20, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Budde, H.; Pietrassyk-Kendziorra, S.; Bohm, S.; Voelcker-Rehage, C. Hormonal responses to physical and cognitive stress in a school setting. Neurosci. Lett. 2010, 474, 131–134. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, P.E.; Gustafsson, P.A.; Ivarsson, T.; Nelson, N. Diurnal cortisol levels and cortisol response in youths with Obsessive-Compulsive Disorder. Neuropsychobiology 2008, 57, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Kelly, S.J.; Young, R.; Sweeting, H.; Fischer, J.E.; West, P. Levels and confounders of morning cortisol collected from adolescents in a naturalistic (school) setting. Psychoneuroendocrinology 2008, 33, 1257–1268. [Google Scholar] [CrossRef] [PubMed]
- Sjörs, A.; Ljung, T.; Jonsdottir, I.H. Diurnal salivary cortisol in relation to perceived stress at home and at work in healthy men and women. Biol. Psychol. 2014, 99, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Freitag, C.M.; Hänig, S.; Palmason, H.; Meyer, J.; Wüst, S.; Seitz, C. Cortisol awakening response in healthy children and children with ADHD: Impact of comorbid disorders and psychosocial risk factors. Psychoneuroendocrinology 2009, 34, 1019–1028. [Google Scholar] [CrossRef]
- Ma, L.; Chen, Y.; Chen, H.; Liu, Y.; Wang, Y. The function of hypothalamus–pituitary–adrenal axis in children with ADHD. Brain Res. 2011, 1368, 159–162. [Google Scholar] [CrossRef] [PubMed]
- Lupien, S.J.; King, S.; Meaney, M.J.; McEwen, B.S. Can poverty get under your skin? Basal cortisol levels and cognitive function in children from low and high socioeconomic status. Dev. Psychopathol. 2001, 13, 653–676. [Google Scholar] [CrossRef]
- Clearfield, M.W.; Carter-Rodriguez, A.; Merali, A.; Shober, R. The effects of SES on infant and maternal diurnal salivary cortisol output. Infant Behav. Dev. 2014, 37, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Sajaniemi, N.; Suhonen, E.; Kontu, E.; Rantanen, P.; Lindholm, H.; Hyttinen, S.; Hirvonen, A. Children’s cortisol patterns and the quality of the early learning environment. Eur. Early Child. Educ. Res. J. 2011, 19, 45–62. [Google Scholar] [CrossRef]
- Smyth, N.; Hucklebridge, F.; Thorn, L.; Evans, P.; Clow, A. Salivary Cortisol as a Biomarker in Social Science Research. Soc. Personal. Psychol. Compass 2013, 7, 9–605. [Google Scholar] [CrossRef]
- Martinez-Aguayo, A.; Aglony, M.; Bancalari, R.; Avalos, C.; Bolte, L.; Garcia, H.; Loureiro, C.; Carvajal, C.; Campino, C.; Inostroza, A.; et al. Birth weight is inversely associated with blood pressure and serum aldosterone and cortisol levels in children. Clin. Endocrinol. 2012, 76, 713–718. [Google Scholar] [CrossRef] [PubMed]
- Spratt, E.G.; Nicholas, J.S.; Brady, T.; Carpenter, L.A.; Hatcher, C.R.; Meekins, K.A.; Furlanetto, R.W.; Charles, J.M. Enhanced Cortisol Response to Stress in Children in Autism. J. Autism Dev. Disord. 2012, 42, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Lupien, S.J.; Ouellet-Morin, I.; Trépanier, L.; Juster, R.P.; Marin, M.F.; Francois, N.; Sindi, S.; Wan, N.; Findlay, H.; Durand, N.; et al. The DeStress for success program: Effects of a stress education program on cortisol levels and depressive symptomatology in adolescents making the transition to high school. Neuroscience 2013, 249, 74–87. [Google Scholar] [CrossRef] [PubMed]
- Kirschbaum, C.; Hellhammer, D.H. Salivary cortisol in psychobiological research: An overview. Neuropsychobiology 1989, 22, 150–169. [Google Scholar] [CrossRef] [PubMed]
- Poll, E.; Kreitschmann-Andermahr, I.; Langejuergen, Y.; Stanzel, S.; Gilsbach, J.M.; Gressner, A.; Yaqmur, E. Saliva collection method affects predictability of serum cortisol. Clin. Chim. Acta 2007, 382, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Putnam, S.K.; Lopata, C.; Fox, J.D.; Thomeer, M.L.; Rodgers, J.D.; Volker, M.A.; Lee, G.K.; Neilans, E.G.; Werth, J. Comparison of saliva collection methods in children with high-functioning Autism Spectrum Disorders: Acceptability and Recovery of Cortisol. Child Psychiatry Hum. Dev. 2012, 43, 560–573. [Google Scholar] [CrossRef] [PubMed]
- Collection Methods: Passive Drool Using the Saliva Collection Aid. Available online: https://www.salimetrics.com/assets/documents/passive-drool-saliva-collection-instructions.pdf (accessed on 22 January 2018).
- Wan, N. Why We Use Passive Drool Collection Versus Absorbent Methods. Available online: https://humanstress.ca/Documents/pdf/SalivaLab/passivedrool_EN.pdf (accessed on 22 January 2018).
- Granger, D.A.; Kivlighan, K.T.; Fortunato, C.; Harmon, A.G.; Hibel, L.C.; Schwartz, E.B.; Whembolua, G.L. Integration of salivary biomarkers into developmental and behaviorally-oriented research: Problems and solutions for collecting specimens. Physiol. Behav. 2007, 92, 583–590. [Google Scholar] [CrossRef] [PubMed]
- Thorpe, K.J.; Pattinson, C.L.; Smith, S.S.; Straton, S.L. Mandatory naptimes in childcare do not reduce children’s cortisol levels. Sci. Rep. 2018, 8. [Google Scholar] [CrossRef] [PubMed]
- Smith, V.C.; Dougherty, L.R. Noisy Spit: Parental Noncompliance with Child Salivary Cortisol Sampling. Dev. Psychobiol. 2013, 647–656. [Google Scholar] [CrossRef] [PubMed]
- Kaitz, M.; Sabato, R.; SHalev, I.; Ebstein, R.; Mankuta, D. Children’s noncompliance during saliva collection predicts measures of salivary cortisol. Dev. Psychobiol. 2011, 54, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Von Polier, G.G.; Herpertz-Dahlmann, B.; Konrad, K.; Wiesler, K.; Rieke, J.; Heinzel-Gutenbrunner, M.; Bachmann, C.J.; Vloet, T.D. Reduced cortisol in boys with Early-Onset Conduct Disorder and Callous-Unemotional Traits. BioMed Res. Int. 2013, 2013, 349530. [Google Scholar] [CrossRef] [PubMed]
- Imeraj, L.; Antrop, I.; Roeyers, H.; Swanson, J.; Deschepper, E.; Bal, S.; Deboutte, D. Time-of-day effects in arousal: Disrupted diurnal cortisol profiles in children with ADHD. J. Child Psychol. Psychiatry 2012, 53, 782–789. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLOS Med. 2009, 6, 7. [Google Scholar] [CrossRef] [PubMed]
- Alghadir, A.H.; Gabr, S.A.; Al-Eisa, E. Effects of physical activity on trace elements and depression related biomarkers in children and adolescents. Biol. Trace Elem. Res. 2016, 172, 299–306. [Google Scholar] [CrossRef] [PubMed]
- Bevans, K.; Cerbone, A.; Overstreet, S. Relations between recurrent trauma exposure and recent life stress and salivary cortisol among children. Dev. Psychopathol. 2008, 20, 257–272. [Google Scholar] [CrossRef] [PubMed]
- Bunterm, T.; Wattanathorn, J.; Vangpoomyai, P.; Muchimapura, S. Impact of open inquiry in science education on working memory, saliva cortisol and problem solving skill. Procedia Soc. Behav. Sci. 2012, 46, 5387–5391. [Google Scholar] [CrossRef]
- Catherine, N.L.A.; Schonert-Reichl, K.A.; Hertzman, C.; Oberlander, T.F. Afternoon cortisol in elementary school classrooms: Associations with peer and teacher support and child behaviour. School Ment. Health 2012, 4, 181–192. [Google Scholar] [CrossRef]
- Fernald, L.C.; Grantham-McGregor, S.M.; Manandhar, D.S.; Costello, A. Salivary cortisol and heart rate in stunted and nonstunted Nepalese school children. Eur. J. Clin. Nutr. 2003, 57, 1458–1465. [Google Scholar] [CrossRef] [PubMed]
- Haines, M.M.; Stansfeld, S.A.; Job, R.F.S.; Berglund, B.; Head, J. Chronic aircraft noise exposure, stress responses, mental health and cognitive performance in school children. Psychol. Med. 2001, 31, 265–277. [Google Scholar] [CrossRef] [PubMed]
- Jager, K.; Schmidt, M.; Conzelmann, A.; Roebers, C.M. Cognitive and physiological effects of an acute physical activity intervention in elementary school children. Front. Psychol. 2014, 5, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Oskis, A.; Loveday, C.; Hucklebridge, F.; Thorn, L.; Clow, A. Diurnal patterns of salivary cortisol across the adolescent period in healthy females. Psychoneuroendocrinology 2009, 34, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Scherr, J.F.; Hahn, L.J.; Hooper, S.R.; Hatton, D.; Roberts, J.E. HPA axis function predicts development of working memory in boys with FXS. Brain Cognit. 2016, 102, 80–90. [Google Scholar] [CrossRef] [PubMed]
- Yoo, Y.G.; Lee, D.J.; Lee, I.S.; Shin, N.; Park, J.Y.; Yoon, M.R.; Yu, B. The effects of mind subtraction meditation on depression, social anxiety, aggression, and salivary cortisol levels of elementary school children in South Korea. J. Pediatr. Nurs. 2016, 31, 185–197. [Google Scholar] [CrossRef] [PubMed]
- Young, R.; Sweeting, H.; West, P. Associations between DSM-IV diagnosis, psychiatric symptoms and morning cortisol levels in a community sample of adolescents. Soc. Psychiatry Psychiatr. Epidemiol. 2012, 47, 723–733. [Google Scholar] [CrossRef] [PubMed]
- Clements, A.D.; Parker, C.R. The relationship between salivary cortisol concentrations in frozen versus mailed samples. Psychoneuroendocrinology 1998, 23, 613–616. [Google Scholar] [CrossRef]
- Putnam, S.K.; Lopata, C.; Thomeer, M.L.; Volker, M.A.; Rodgers, J.D. Salivary cortisol levels and diurnal patterns in children with Autism Spectrum Disorder. J. Dev. Phys. Disabil. 2015, 27, 453–465. [Google Scholar] [CrossRef]
- Jacks, D.E.; Sowash, J.; Anning, J.; McGloughlin, T.; Andres, F. Effect of exercise at three exercise intensities on salivary cortisol. J. Strength Cond. Res. 2002, 16, 286–289. [Google Scholar] [PubMed]
- Stalder, T.; Kirschbaum, C.; Kudielka, B.M.; Adam, E.K.; Pruessner, J.C.; Wüst, S.; Dockray, S.; Smyth, N.; Evans, P.; Hellhammer, D.H.; et al. Assessment of the cortisol awakening response: Expert consensus guidelines. Psychoneuroendocrinology 2016, 63, 414–432. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Level | Levels of Evidence | Quantity of Articles |
|---|---|---|
| 1 | Systematic review of randomized trials or n-of-1 trials | 0 |
| 2 | Randomized trial or observational study with dramatic effect | 9 |
| 3 | Non-randomized controlled cohort/follow-up study | 16 |
| 4 | Case-series, case-control studies, or historically controlled studies | 0 |
| 5 | Mechanism based reasoning | 0 |
| First Author Year | Participants | Salivary Cortisol Collection | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| N | Male (% Only Where Stated) | Female (% Only Where Stated) | Age | Cohort Details | Control Group | Cortisol Measure | Method | Protocol | Time | Storage | |
| Alghadir 2016 [33] | 150 | 90 | 60 | 7–18 years | Typically Developing | N/A | Baseline comparison with other measures | Not known | Saliva collection after overnight fast | Morning: 9.00–11.30 | −80 °C |
| Beetz 2011 [4] | 31 | 31 | 0 | 7–12 years | Insecure/Disorganised Attachment | No | Acute | Salivette | Not known—researcher present when saliva sampling | Pre stress test, 7 min, 20 min, and 13 min later, post test | −20 °C |
| Beetz 2012 [5] | 47 | 47 | 0 | 7–11 years | Insecure/Disorganised Attachment | No | Acute | Salivette | Not known—researcher present when saliva sampling | Pre-stress test, 7 min, 20 min, and 13 min later, post test | −20 °C |
| Bevans 2008 [34] | 68 | 40% | 60% | 7–13 years | Typically Developing | N/A | Baseline comparison against measures | Salivette | Mouth rinsed with water 15 min prior to sampling | 1 a.m. sample 7.45–8.10 1 p.m. sample 2.15–3 p.m. | Stored in cooler, then university freezer −70 °C |
| Budde 2010 [8] | 53 | 27 | 26 | 9–10 years | Typically Developing | Yes | Acute | Salivette | First sample at 11.30 No food in last 2 h. Second sample approx. 12 p.m. | Pre- and post- exercise/movie watching | −20 °C |
| Bunterm 2012 [35] | 86 | 29 | 57 | 10th grade Thailand | Typically Developing | Yes | Intervention | Not known | Not known | Pre and post intervention 1 sample pre and post between 7.30–8.00 a.m. | Frozen and sent for lab analysis |
| Butzer 2015 [7] | 36 | 20 | 16 | 2nd and 3rd grade | Typically Developing | Yes | Intervention | Passive drool | Instructions given prior to sampling | Pre- and post-stress test in week 1 and 10, after yoga session | Frozen, temp. not specified |
| Catherine 2012 [36] | 89 | 40 | 49 | 9–12 years | Typically Developing | N/A | Baseline Comparison against measures | Salivette | Recorded time of awakening and recent food intake before every sample | 9 a.m., 12 p.m. and 3 p.m. on 4 days | Samples centrifuged up to 3 h after collection |
| Fernald 2003 [37] | 130 | Not stated | Not stated | 8–10 years | Children with delayed physical growth and typically developing children | Yes | Acute | Salivette | Not known | Arrival, after digit span task, 10, 20,30 min after digit span task. 6th sample after school | Centrifuged, then stored at −20 °C |
| Gabriels 2013 [3] | 21 | 21 | 0 | 3–9 years | ASD | N/A | Diurnal | Color-coded Whatman filter paper | No eating, brushing teeth before collection, no drinking 15 min before collection. Collection demonstrated by RA. | Awakening, 30 min later, before lunch, 4 p.m. on three consecutive days | Stored in booklet and dried at room temperature |
| Gustafsson 2007 [9] | 23 + 336 | 10 | 13 | 9–17 years | OCD Typically Developing | Reference group—previous study | Acute | Salivette | Not known | Before and 30 min after stressor—time of day not specified | Centrifuged, then stored at −20 °C for 6 months |
| Haines 2001 [38] | 340 | 50% | 50% | 8–10 years | Typically Developing | N/A | Acute—measuring cognitive performance | Salivette | Screening: touching Salivette, food, medication, life-events, smoking, physical activity, mouth infection. | Morning | Not specified |
| Imeraj 2012 [31] | 66 | 52 | 14 | 6–12 years | ADHD Typically Developing | Yes | Diurnal | Salivette | No sour food, drink or brushing teeth 30 min prior to sampling | After awakening, 30 min later, noon, 4 p.m., 8 p.m. | Home keeping during collection. Then collected, centrifuged stored at −20 °C till analysis |
| Jager 2014 [39] | 104 | 45.2% | 54.8% | 6–8 years | Typically Developing | Yes | Acute—measuring intervention | Salivette | Not specified | School morning | −20 °C |
| Kelly 2008 [10] | 2995 | Not stated | Not stated | 15 years | Typically Developing | N/A | Diurnal | Salivette | Not known—researcher told teenagers when to put Salivette in mouth | Five min after start of questionnaire, 30 min later, about five min before end of session | −20 °C |
| Lupien 2001 [14] | 307 | Not stated | Not stated | 6–16 years | Typically Developing | N/A | Baseline comparison against measures | Salivette—filter paper | Instructions provided before sampling, demonstration of collection | Two samples pre and post assessment. Approx. 8 a.m., 9 a.m. | Paper clipped to drying device |
| Lupien 2013 [20] | 504 | 260 | 244 | 11–13 years | Typically Developing | Yes | Intervention | Passive drool | Provided with oral instructions | One sample at beginning and one at end of each session. Pre-intervention, post-intervention and at follow-up points | −20 °C |
| Oskis 2009 [40] | 61 | 0 | 61 | 9–18 years | Typically Developing | N/A | Diurnal | Passive drool straw | Participant information pack explaining collection. Only consuming water 30 min before sample, no exercise or brushing teeth. | CAR: awakening, 15, 30, 45 min after. 3, 6, 9, 12 h after awakening. On 2 school days. | −20 °C, home. Frozen straight away or after school. |
| Palma 2012 [1] | 76 | 62 | 14 | 8.7 years mean age | ADHD, Typically Developing | Yes | Acute | Passive drool, Salivette | Rinsing with filtered water prior sampling. No food/drink 30 min prior to sampling | 15 min before stress test, 20, 40, 60 min post stress test | Not known |
| Palma 2015 [2] | 59 | 45 | 14 | 10–18 years | ADHD Typically Developing | Yes | Acute | Salivette | Rinsing with filtered water prior sampling No food or drink 30 min prior to sampling | 15 min before stress test, 20, 40, 60 min post stress test | Not known |
| Scherr 2016 [41] | 105 | 105 | 0 | 7–13 years | Typically Developing and Fragile X syndrome | Yes | Baseline—first assessment Acute—final assessment | Salivette | No food or drink 30 min prior to saliva samples. | Pre and post assessment Time not specified | Not specified |
| Schonert---Reichl 2015 [6] | 99 | Not stated | Not stated | 9–11 years | Typically Developing | No | Intervention | Salivette | No food and physical activity min 30 min before sample collection. Researchers assisted collection. Children recorded time of awakening. | 9 a.m., 11.30 a.m. 2.30 p.m. | Shipped analysis after collection |
| von Polier 2013 [30] | 75 | 75 | 0 | 7–16 years | EO-CD CU traits Typically Developing | Yes | Diurnal | Salivette | Oral and written instructions for adults. Rinsed mouth pre- sampling. No smoking, eating, drinking caffeinated or alcoholic drinks, vigorous exercise or brushing teeth pre- first three samples. Journal for compliance. | Awakening, 30, 60 min after, 12 p.m.,15.20, 15.40, 19.00 | Frozen imme-diately −60 °C |
| Yoo 2016 [42] | 42 | 20 | 22 | 10 years mean age | Typically Developing | Yes | Measuring intervention effect | Passive drool | No stimulating food consumption 1 h before sampling. Rinsing mouth 10 min before collection. | School day 2–4 p.m. | −20 °C |
| Factor to Consider | Recommendation for Best Practice |
|---|---|
| Method of collection |
|
| Protocol for collection |
|
| Guidelines prior to collection | The following guidelines should be followed where possible:
|
| Collection training and compliance |
|
| Collection | Researchers to be present where suitable. If researchers cannot be present:
|
| Timing | Timing of sample collection must be respected as follows:
|
| Factors to record | Participants or parents/guardians to record the following through questionnaires or a diary where possible:
|
| Storage | Different storage procedures are possible, however the same procedure should be strictly followed throughout the entire study, including the storage timing in each condition (order from most to least recommended):
|
| Reporting outcome | Researchers must be transparent about the participant group characteristics and the cortisol collection procedure. The following must be stated clearly:
|
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dimolareva, M.; Gee, N.R.; Pfeffer, K.; Maréchal, L.; Pennington, K.; Meints, K. Measuring Cortisol in the Classroom with School-Aged Children—A Systematic Review and Recommendations. Int. J. Environ. Res. Public Health 2018, 15, 1025. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15051025
Dimolareva M, Gee NR, Pfeffer K, Maréchal L, Pennington K, Meints K. Measuring Cortisol in the Classroom with School-Aged Children—A Systematic Review and Recommendations. International Journal of Environmental Research and Public Health. 2018; 15(5):1025. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15051025
Chicago/Turabian StyleDimolareva, Mirena, Nancy R. Gee, Karen Pfeffer, Laëtitia Maréchal, Kyla Pennington, and Kerstin Meints. 2018. "Measuring Cortisol in the Classroom with School-Aged Children—A Systematic Review and Recommendations" International Journal of Environmental Research and Public Health 15, no. 5: 1025. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15051025