1. Introduction
Sleeping and awakening are essential physiological processes that are necessary for human survival. Good sleep quality helps to maintain good wakefulness. However, more and more people complain about experiencing poor sleep quality. Estimated rates of insomnia vary between 6% and 48%, depending on the definition and sample or country [
1,
2,
3]. Recent studies have shown that poor sleep quality is associated with psychological problems [
4,
5,
6], physiological and chronic diseases [
7,
8,
9], and an increased risk of non-fatal and fatal occupational injuries [
10,
11]. These are a great burden to the individual and are a significant cost to society [
12,
13,
14]. Sleep problems are currently one of the leading health problems.
Many factors can influence sleep quality, including demographics, social support, health status, sleeping environment, and work and life-related stressors [
15]. The influence of work-related stress on the physical and mental health of populations from different occupations recently become of great interest. Some studies have demonstrated the relationship between insomnia and various types on occupational stress, such as job demand, job control, social support, job insecurity, organizational justice, intragroup conflict, job strain, effort–reward imbalance, employment level, and shift work [
16]. A group of Japanese scholars have published on the relationship between job stress and sleep quality, and the results suggest that job stress is indeed associated with sleep quality, and that it increases the risk of experiencing sleep problems [
17,
18,
19,
20,
21,
22,
23]. Studies from other countries have also found similar relationships between sleep and work-related stress [
24,
25,
26,
27,
28,
29,
30]. Furthermore, a number of studies have indicated that sleep deprivation can increase allostatic responses to psychosocial stress, but daytime sleepiness is associated with a reduced response to stress [
31,
32]. These results all suggest a strong link between sleep and work-related stress.
In addition to job stress, genetic factors may also increase the risk of sleep problems. Twin and family studies have indicated that circadian rhythms are not learned, but are the result, in part, of multiple heritable influences [
33,
34]. Over the years, researchers have been looking for genetic information pertaining to sleep. Animal and human studies have shown that sleep is associated with many neurotransmitters in the brain. Serotonin (5-hydroxytryptamine, 5-HT) is a key central nervous system neurotransmitter that regulates numerous physiological functions, including appetite, thermoregulation, pain perception and hormone secretion, etc. [
35]. Additionally, 5-HT has been shown to be related to the occurrence and maintenance of sleep [
36,
37,
38]. The various physiological functions of 5-HT are mediated via seven distinct receptor families (5-HT1–5-HT7). Studies have found that the 5-HT2A receptor is highly enriched in the medulla oblongata, dorsal raphe nucleus, hippocampus, cerebral cortex, and that these structures are relevant to sleep [
39]. Meanwhile, genetic association studies of the 5-HT2A gene have revealed a very strong linkage disequilibrium of the -1438G/A polymorphism with the T102C polymorphism [
40]. Relationships between the -1438G/A and/or T102C single nucleotide polymorphisms and risk of sleep problems have been found in obstructive sleep apnea (OSA) [
41], sleep bruxism [
42], and in some psychological problems, which accompany sleep disturbance [
43].
Previous studies have highlighted the roles of work-related stress and 5-HT receptor genes in sleep quality, respectively. However, the relationship between these three parameters has rarely been the focus of previous research. Therefore, we carried out a study to examine the independent and interactive effects of 5-HTR2A gene polymorphisms and job stress on sleep quality amongst physicians in the Urumqi of Xinjiang Province, China.
2. Materials and Methods
2.1. Subjects
This study was carried out between March 2015 and July 2016. All subjects gave their informed consent before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of Xinjiang Medical University (2015006). The study subjects were physicians working in six hospitals affiliated with Xinjiang Medical University in the Urumqi of Xinjiang Province, China. The six hospitals comprised of four general hospitals and two specialized hospital. For the study, we randomly selected two general hospitals and one specialized hospital. In total, 1836 physicians were working in these three hospitals. As a large number of blood samples and questionnaires needed to be collected, we applied computer-generated random numbers to the managers’ list of employees from each hospital to select 50% (918) of the participants. We conducted an interview, collecting sociodemographic data, job stress, and sleep quality status, and collected blood samples. The inclusion criteria were as follows: (1) physicians who have been working for >1 year and were aged between 20 and 60 years; and (2) voluntary consent to participate after being informed of the objective and significance of the study (i.e., informed consent) was obtained. The exclusion criteria were as follows: (1) a previous diagnosis of chronic and/or other diseases that may affect sleep quality; (2) use of any medication in the three months prior to the study which may affect the serotonergic system and/or sleep/wake cycle; (3) refusal to participate in the study or being stationed abroad; and (4) incomplete collection of relevant information and/or the absence of a blood sample. Subsequently, 504 physicians were included in the study. Each participant was compensated with RMB 30 Yuan for breakfast in this study.
2.2. Measures
2.2.1. Sleep Quality
Subjective sleep quality was assessed using the Pittsburgh Sleep Quality Index (PSQI). This scale was developed by Dr. Buysse, a psychiatrist at the University of Pittsburgh in 1989 [
44]. This scale is validated for evaluating sleep quality in patients with sleep and psychiatric disorders, as well as in healthy individuals. The scale is composed of 19 items within seven categories: (1) subjective sleep quality; (2) sleep latency; (3) sleep duration; (4) sleep efficiency; (5) sleep disturbances; (6) hypnotic use; and (7) daytime dysfunction. Each category is assigned a score from 0 to 3 using a four-point Likert scale, with the total score ranging from 0 to 21 points. A total score cut-off value of 5 points was used [
45]. A score ≥5 was classified as poor sleep quality, with higher scores reflecting poorer sleep quality. A score <5 was classified as good sleep quality.
2.2.2. Job Stress
Job stress was assessed using the Job Stress Survey (JSS). This scale was developed by Spielberger et al. in 1986 [
46]. It measures the intensity and frequency of stress factors to comprehensively evaluate the stress levels of subjects. The scales’ reliability and validity has been confirmed by other researchers [
47,
48]. The scale was introduced to China by Lian et al. [
49] after obtaining consent from Spielberger et al. The scale was then translated by experts at the Foreign Languages Department to ensure translational accuracy. Under the guidance of experts, relevant economic and cultural items were revised to make the scale more suitable for Chinese physicians. The scale has 60 items. The first 30 items are used to assess the intensity of stress factors, and each item is assigned a score from 1 to 9. The next 30 items are used to assess the number of days of stress experienced over the past 6 months, and again each item is assigned a score from 0 to 9 (with more than 9 days of stress given a score of 9+). The job stress index was the product of the overall intensity and frequency of job-related stress experienced, with higher scores associated with a high level of occupational stress. The quartile method was subsequently used to divide job stress into three categories: (1) low; (2) moderate; and (3) high levels of job stress.
2.3. Genotyping
Blood samples were collected into ethylene diamine tetraacetic acid tubes during the physicians’ physical examination. Genomic DNA (gDNA) was extracted using the Whole Blood Genome Extraction kit (Tiangen Biotech, Beijing, China) before cryopreservation at −20 °C until further use. The T102C and -1438G/A polymorphisms were genotyped using polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP). gDNA (100 ng) was used in each reaction mixture, with the final volume of each reaction mixture totaling 20 μL. gDNA was then amplified using the PCR instrument (MyCycler, Bio-Rad, Hercules, CA, USA). Ten μL of PCR product was then used in each enzyme-digested mixture, with the final volume of each enzyme-digested mixture totaling 30 μL. The fragments were resolved with electrophoresis on 2% agarose gels and visualized with UV light. The primers used and genotype information for T102C and -1438G/A are listed in
Table 1 and
Table 2.
2.4. Covariates
The demographic data collected (i.e., age and ethnicity), as well as job and lifestyle factors are considered to impact upon sleep quality. Therefore they could potentially effect the results of this study. The following variables were taken into account: (1) demographic: sex, age (<30, 30–40, 40–50, >50 years), ethnicity (Han and Minority), educational level (college degree and below, bachelor degree and above), marital status (married, unmarried); (2) job: monthly income (≤5000, >5000 yuan), professional title (elementary, intermediate, advanced), job tenure (<10, 10–20, >20 years); (3) lifestyles: smoking (yes or no), alcohol consumption (yes or no) and regular exercise (yes or no).
2.5. Quality Control
In an attempt to reduce investigator bias, all investigators were trained so that all investigations were conducted in a unified way. Participants were asked to complete the questionnaires independently and anonymously, within 5 min, after which all questionnaires were reviewed and coded by specialized investigators using EpiData version 3.1 (The EpiData Association, Odense, Denmark) to establish a database. 20% of entries were randomly compared against the original questionnaires to check the accuracy of the final database. The PSQI is considered the international gold standard, so the evaluation criteria is unified. Collection of blood samples was completed by a member of the medical team. All samples were stored at −20 °C in a freezer. All experimental instruments were calibrated to ensure standard operations prior to experimental work. The same manufacturer and batch number of each reagent was used throughout the experiment. This ensured that all experiments were standardized to optimize all procedures, and to avoid measurement bias.
2.6. Statistical Analysis
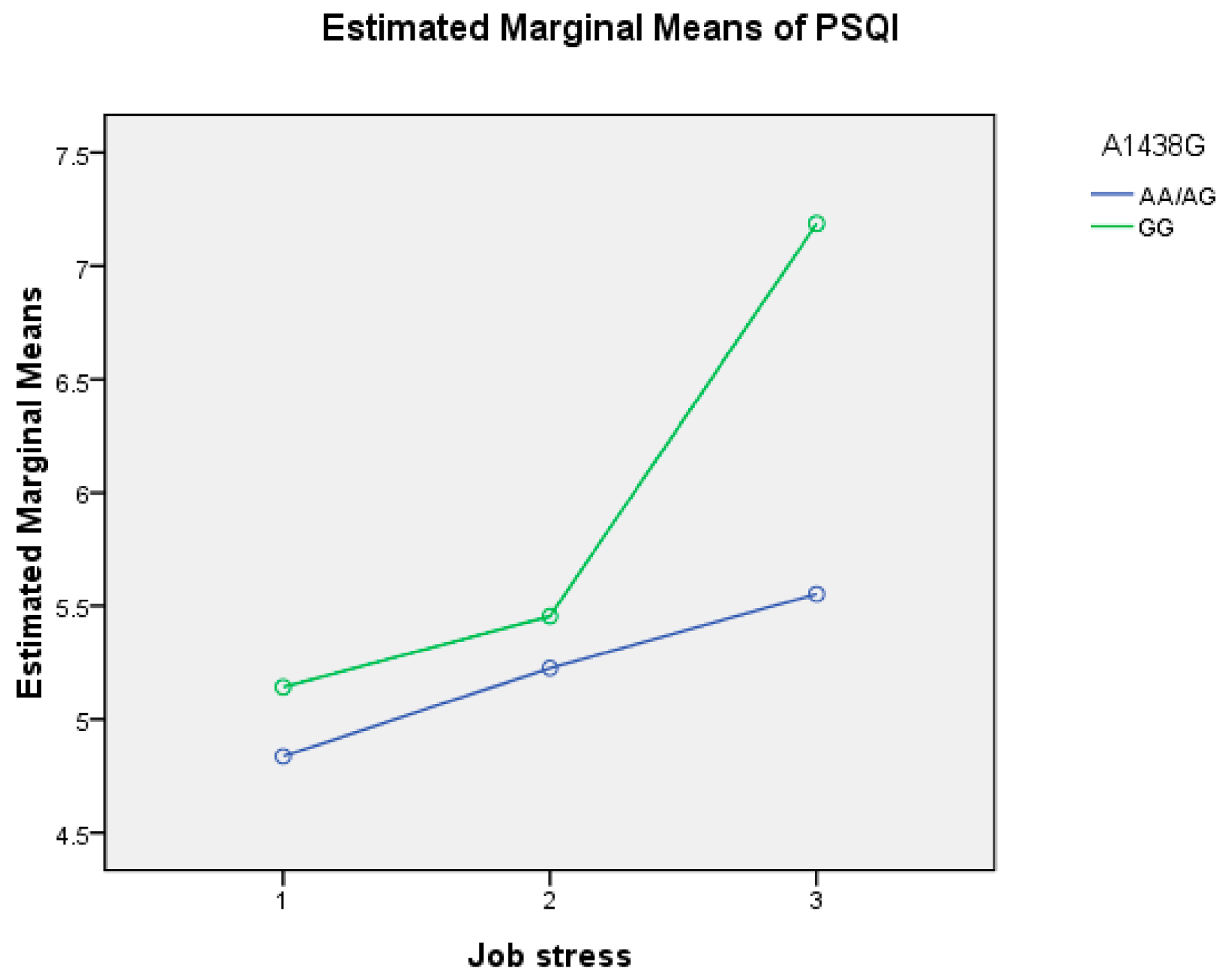
As PSQI scores were not normally distributed, they were analyzed using the Kruskal–Wallis test. If initial results showed significant differences, post hoc pairwise comparisons were analyzed using Mann–Whitney U tests and p-values were adjusted with Bonferroni’s correction. Chi-square (χ2) tests were used to analyze categorical variables [i.e., genotype and Hardy Weinberg Equilibrium (HWE)]. Odds ratios (OR) and 95% confidence intervals (CI) were used to determine the interaction between job-related stress levels and genotype associated with sleep quality using unconditional logistic regression. The interactions between job stress, genotype, and sleep quality were determined with general linear model and crossover analysis. The tests were two-tailed and the significance level was set at p < 0.05 or p < 0.01. The data were analyzed using SPSS 17.0 (IBM, Armonk, NY, USA).




{kind=link}