Evaluating Health Co-Benefits of Climate Change Mitigation in Urban Mobility

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Mobility Scenarios
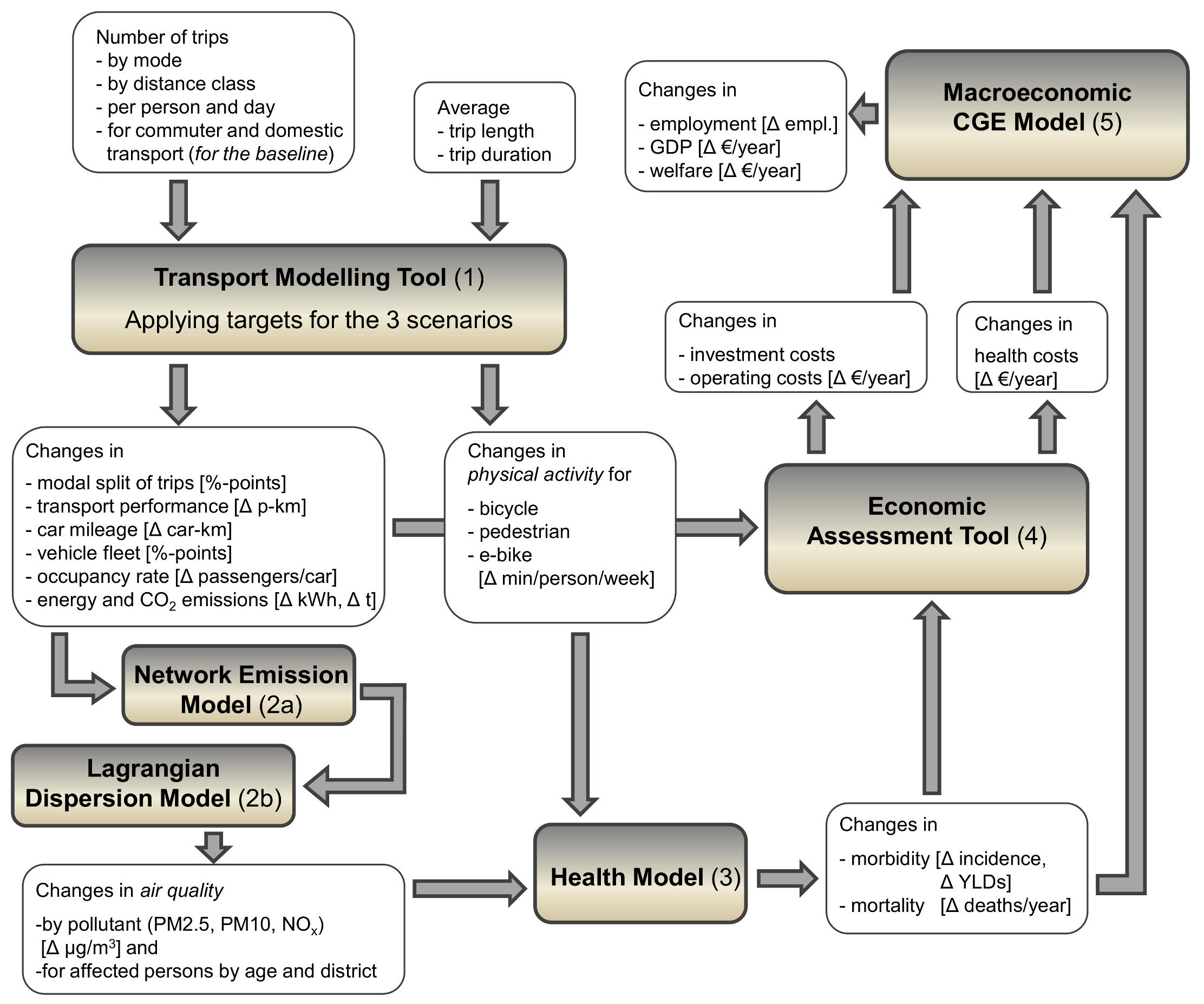
2.2. Modelling Changes in Transportation, Physical Activity and Air Pollution
- Number of trips by category of trip length and mode (#)
- Modal Share (%)
- Number of trips per person and day (#/d/p)
- Average trip length by transport mode (km)
- Average trip duration by transport mode (h)
2.3. Modelling Health Effects from Changes in Modal Shift
2.3.1. Physical Activity
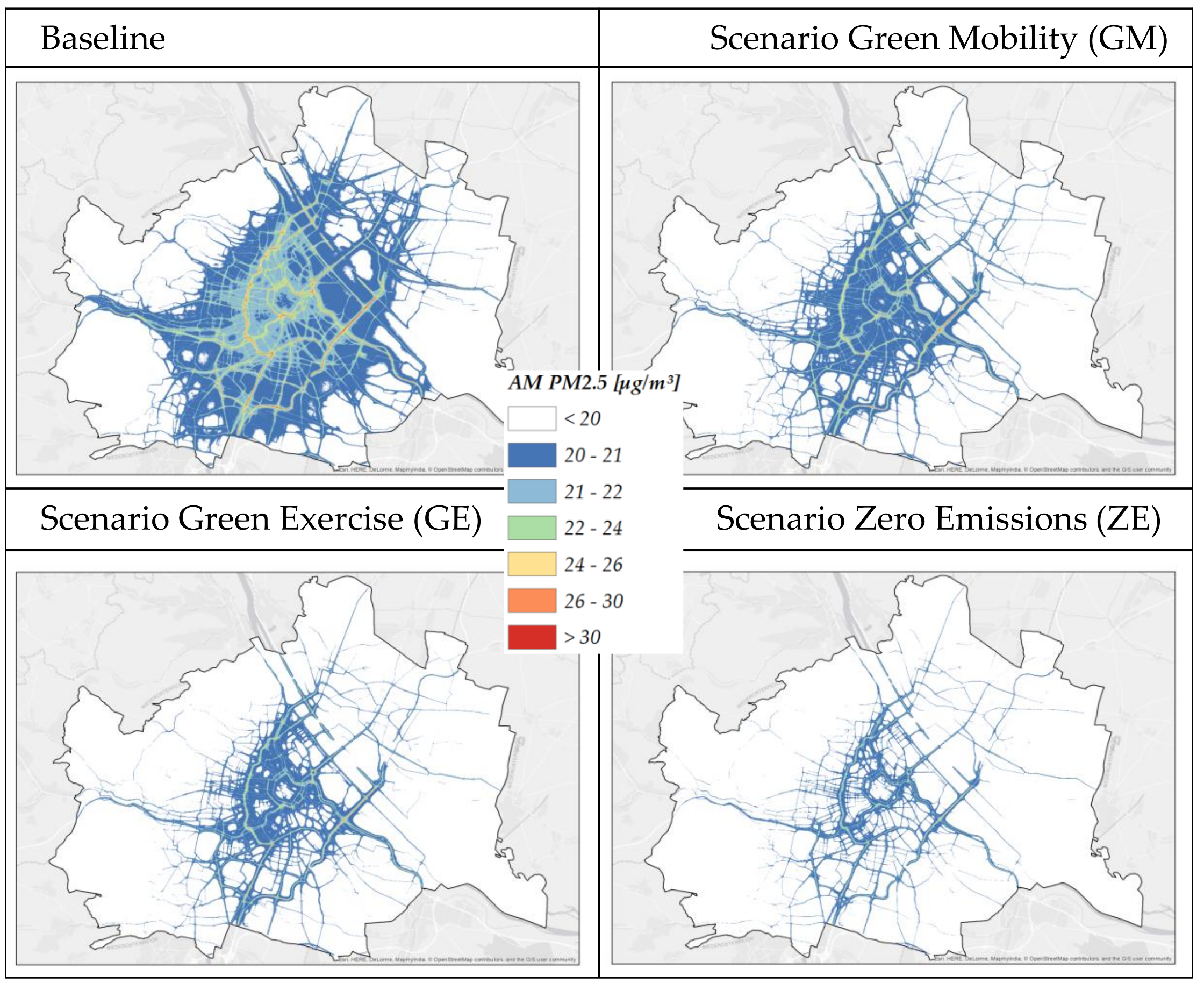
2.3.2. Air pollution
2.4. Economic Assessment
2.4.1. Investment Costs and Operating Costs
2.4.2. Health Costs and Benefits
2.5. The Macroeconomic Model
3. Results
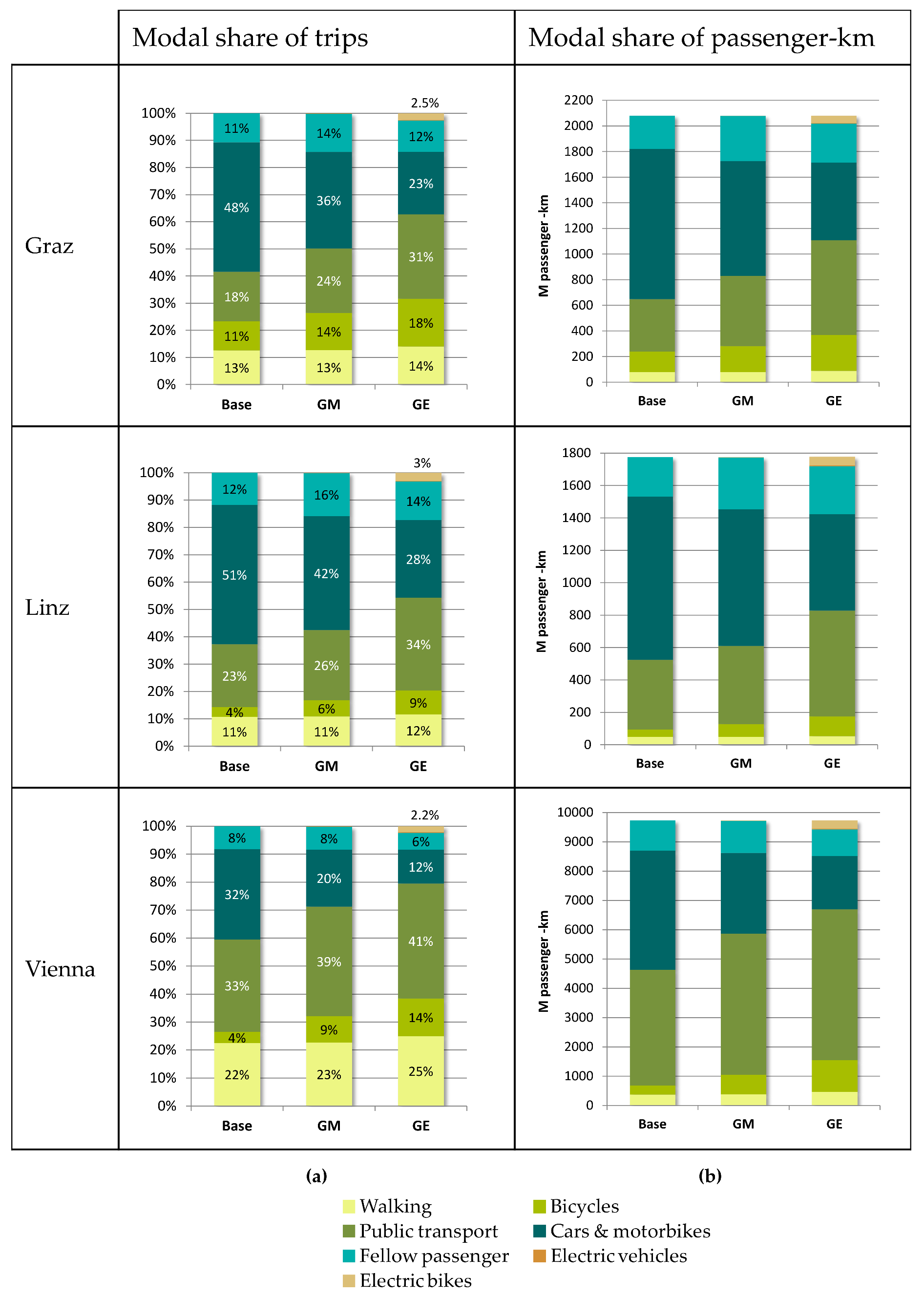
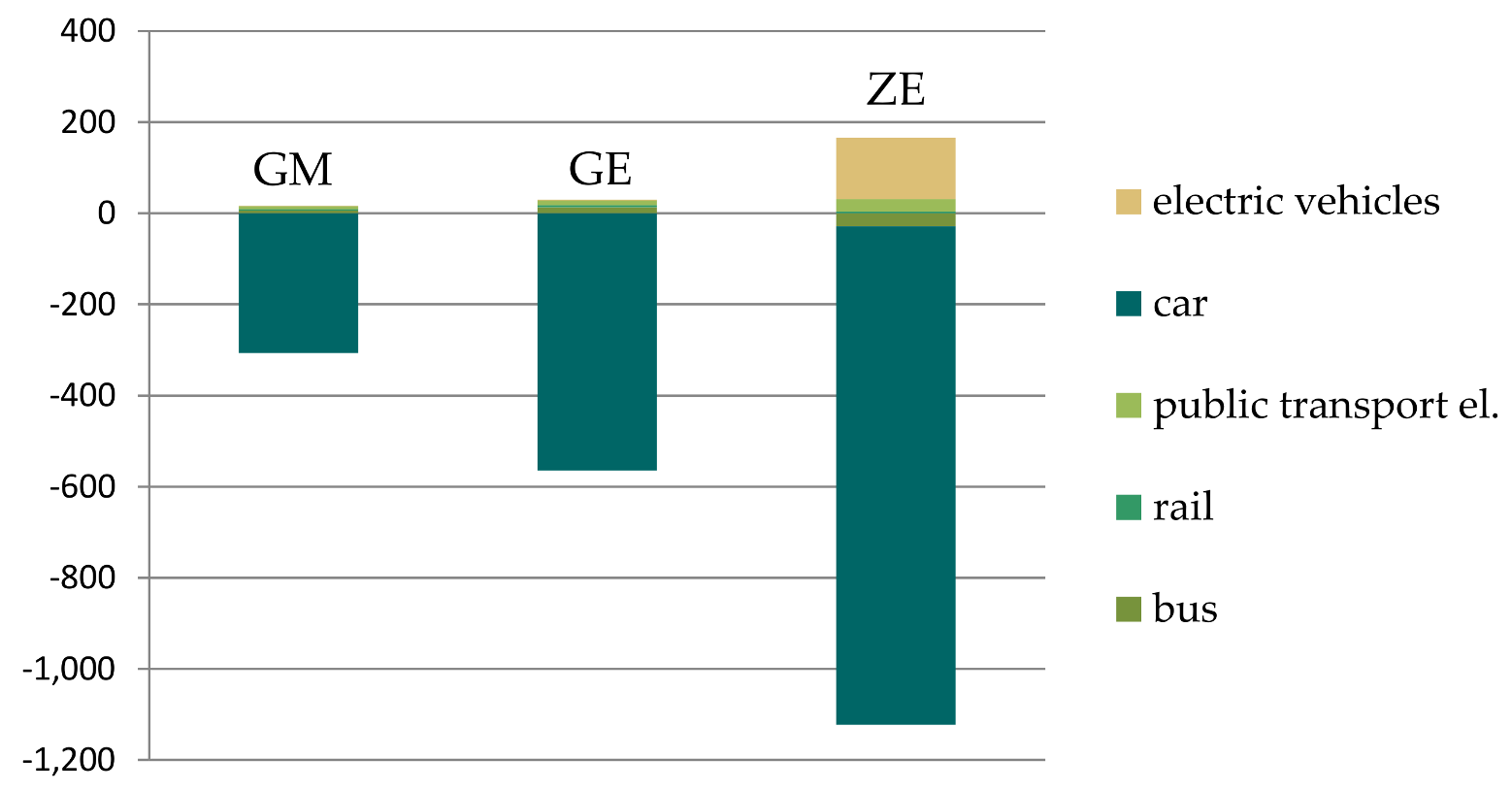
3.1. Transport and Environment
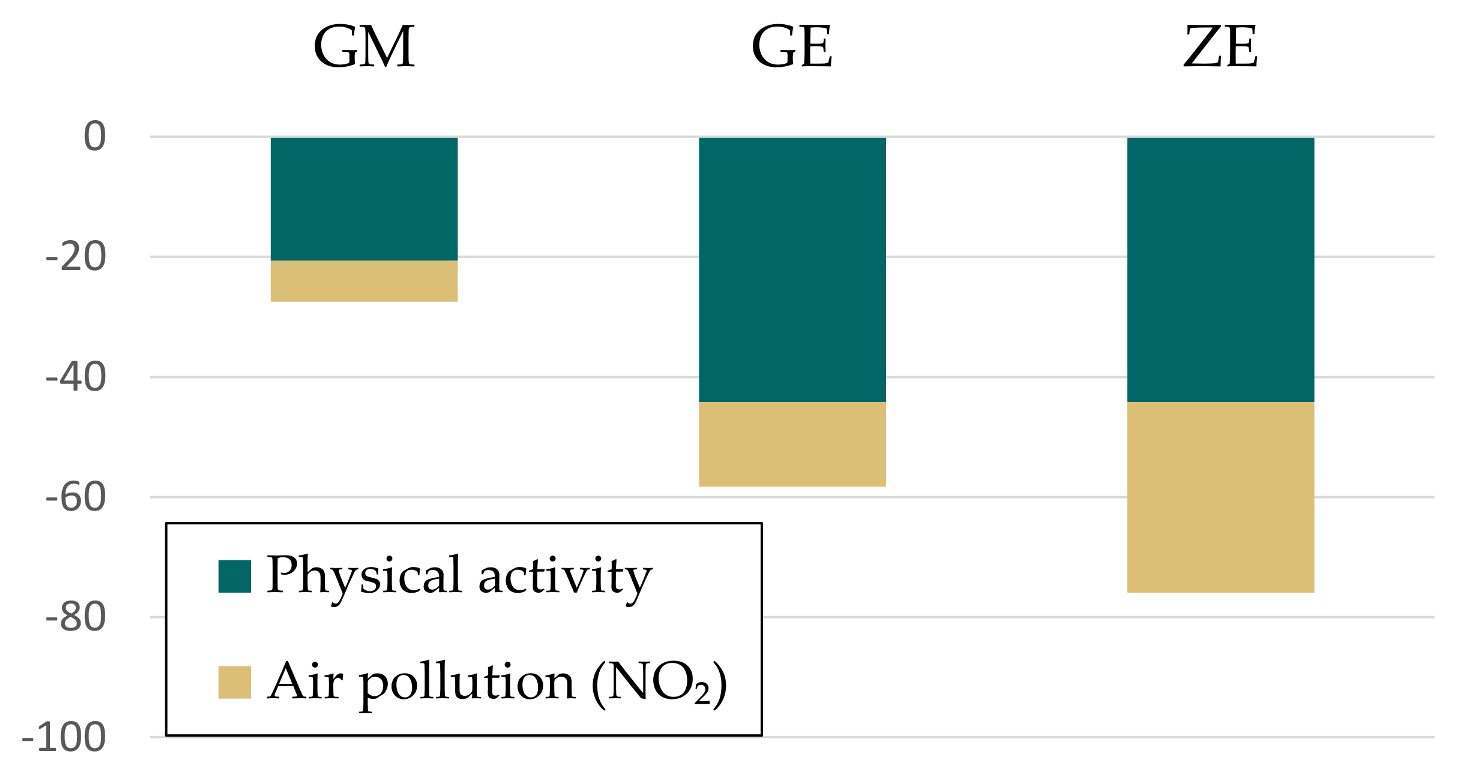
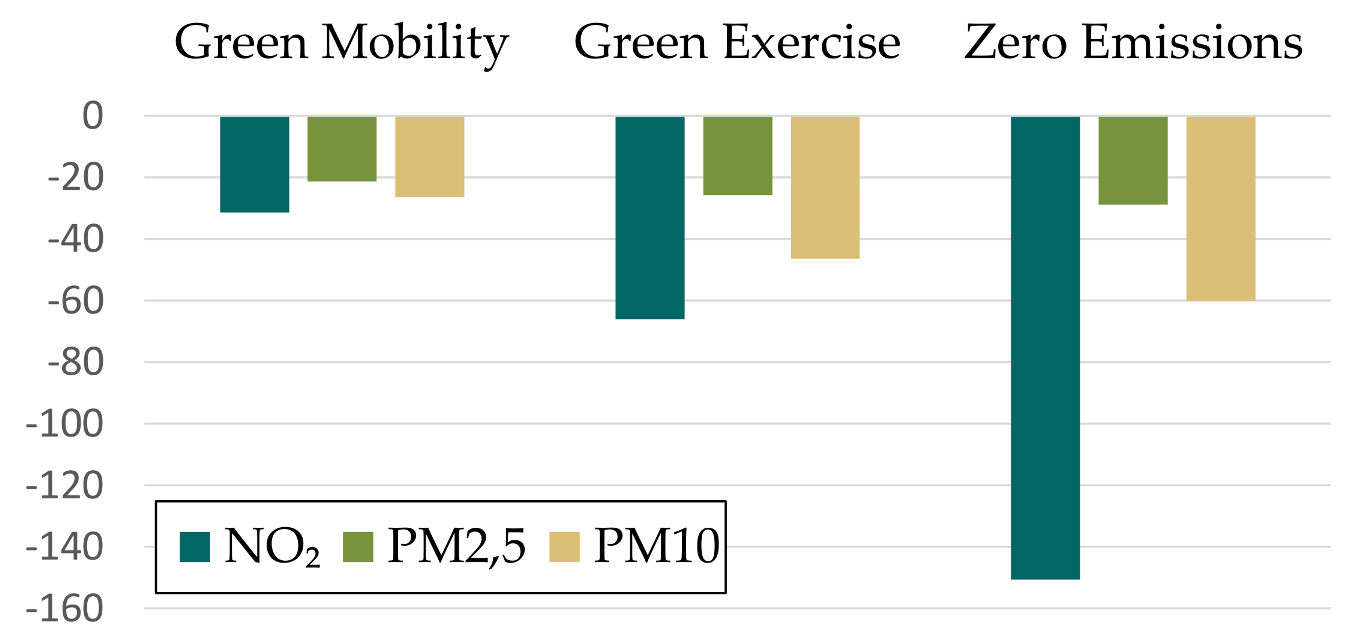
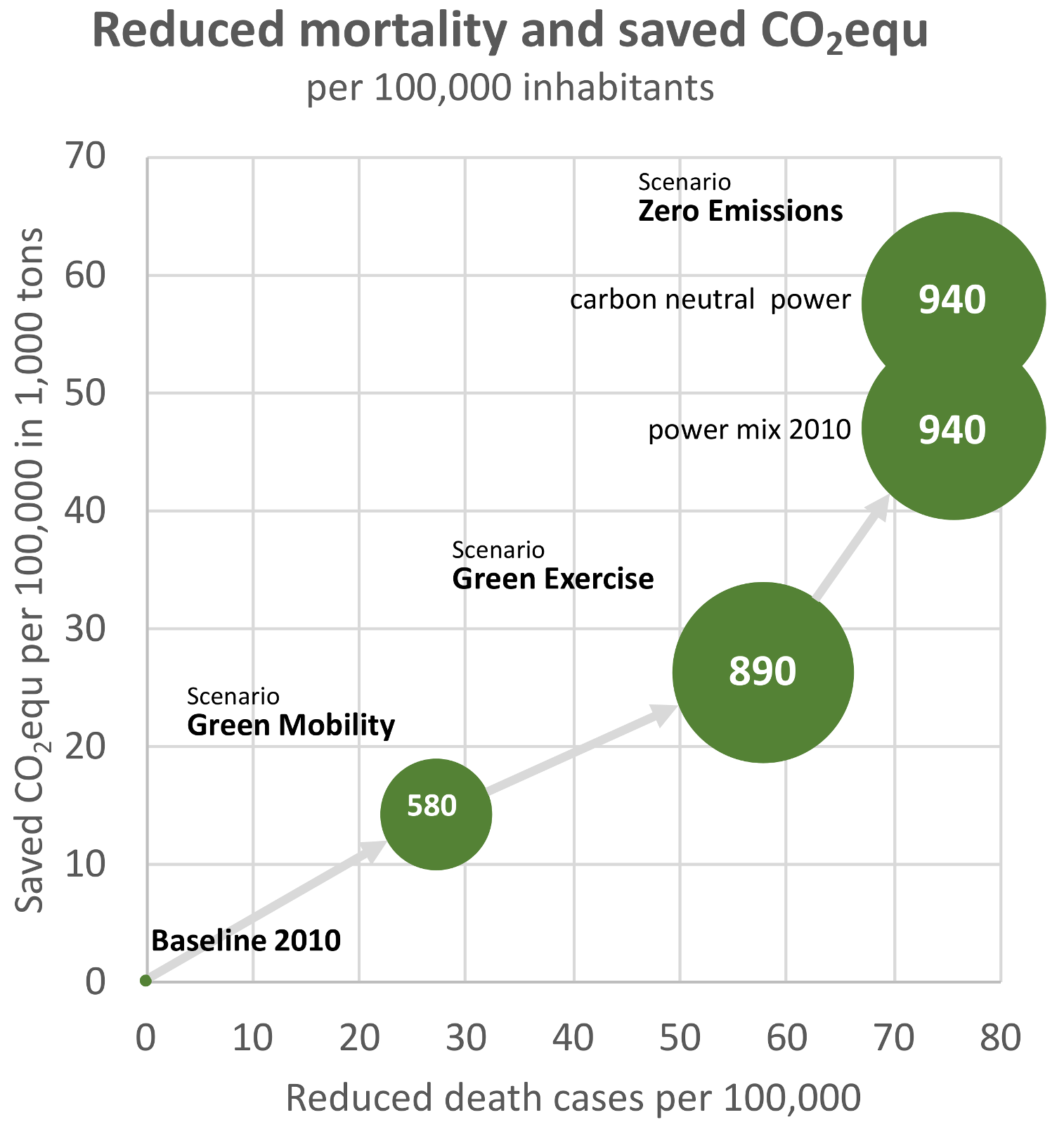
3.2. Health Effects
3.3. Economic Effects of Mitigation Measures and Co-Benefits
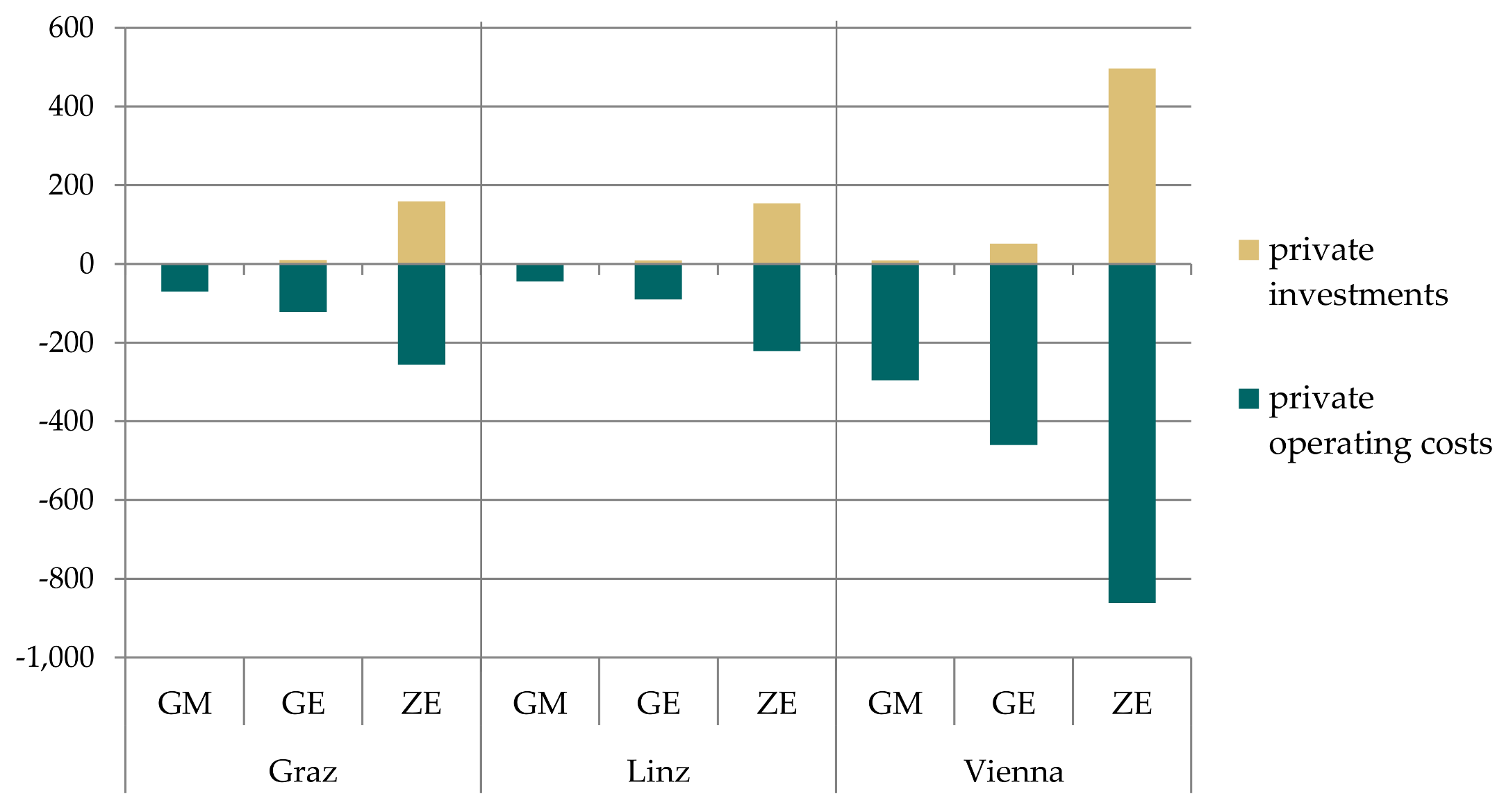
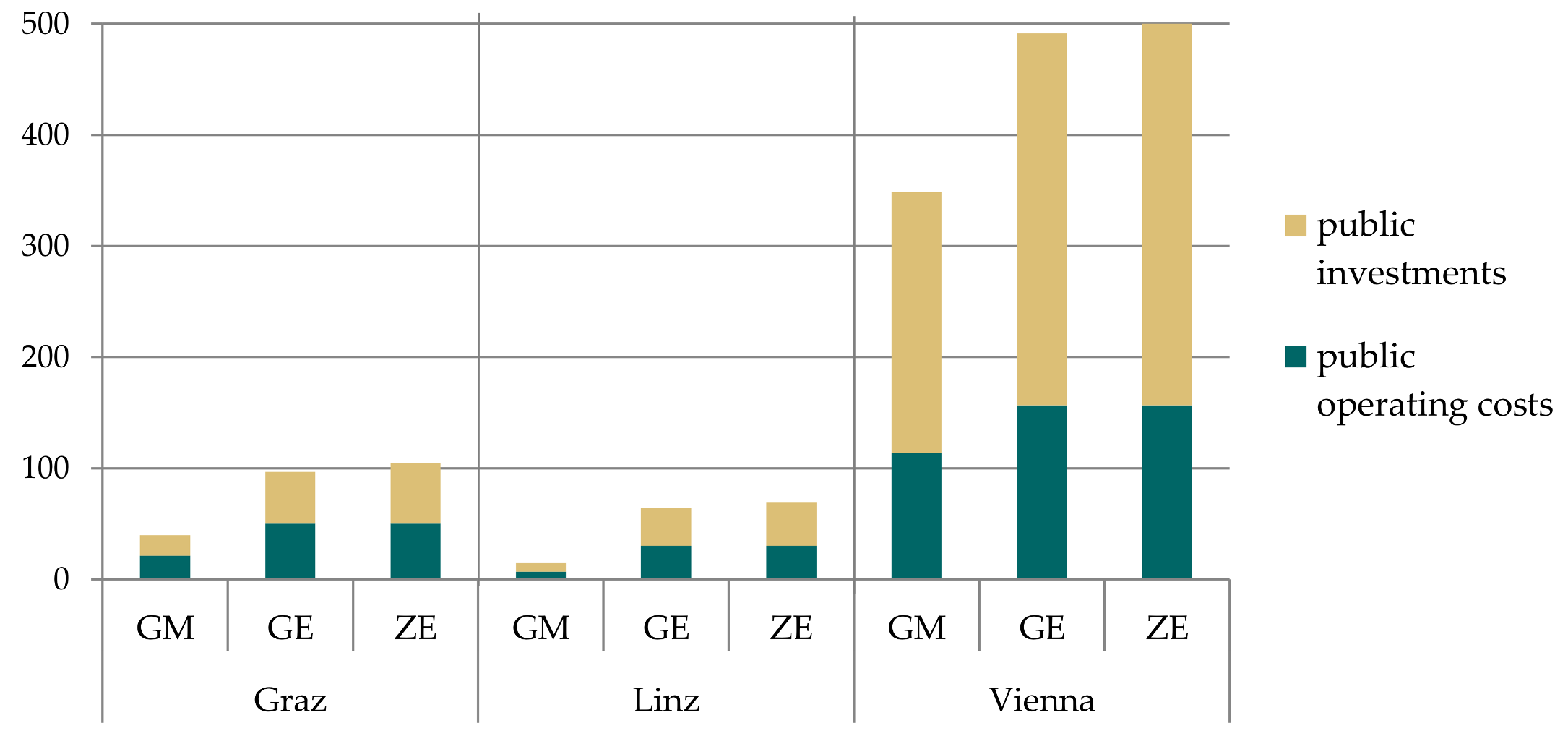
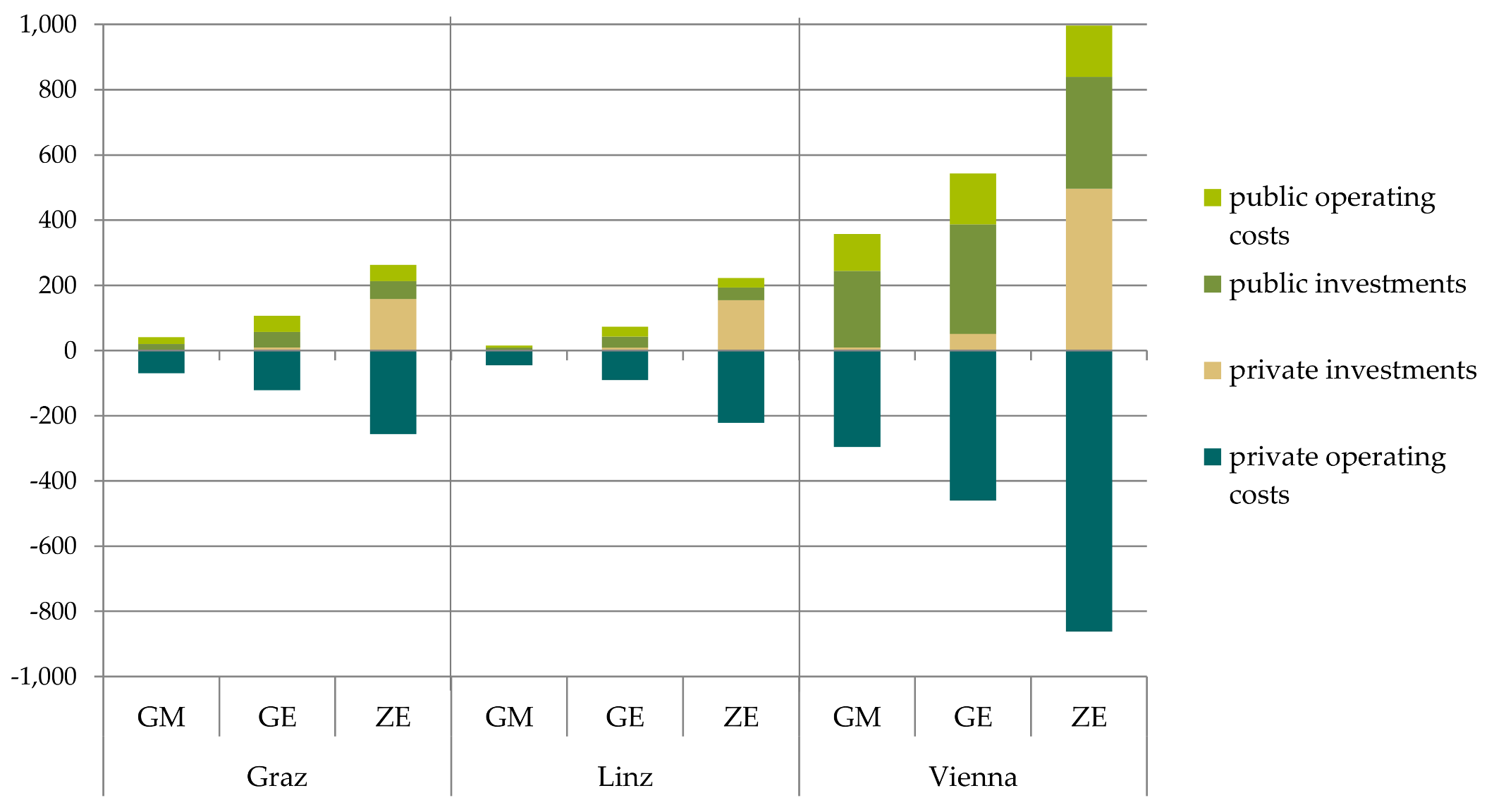
3.3.1. Changes in Implementation Costs, Operating Costs and Household Expenditures
3.3.2. Changes in Health Costs
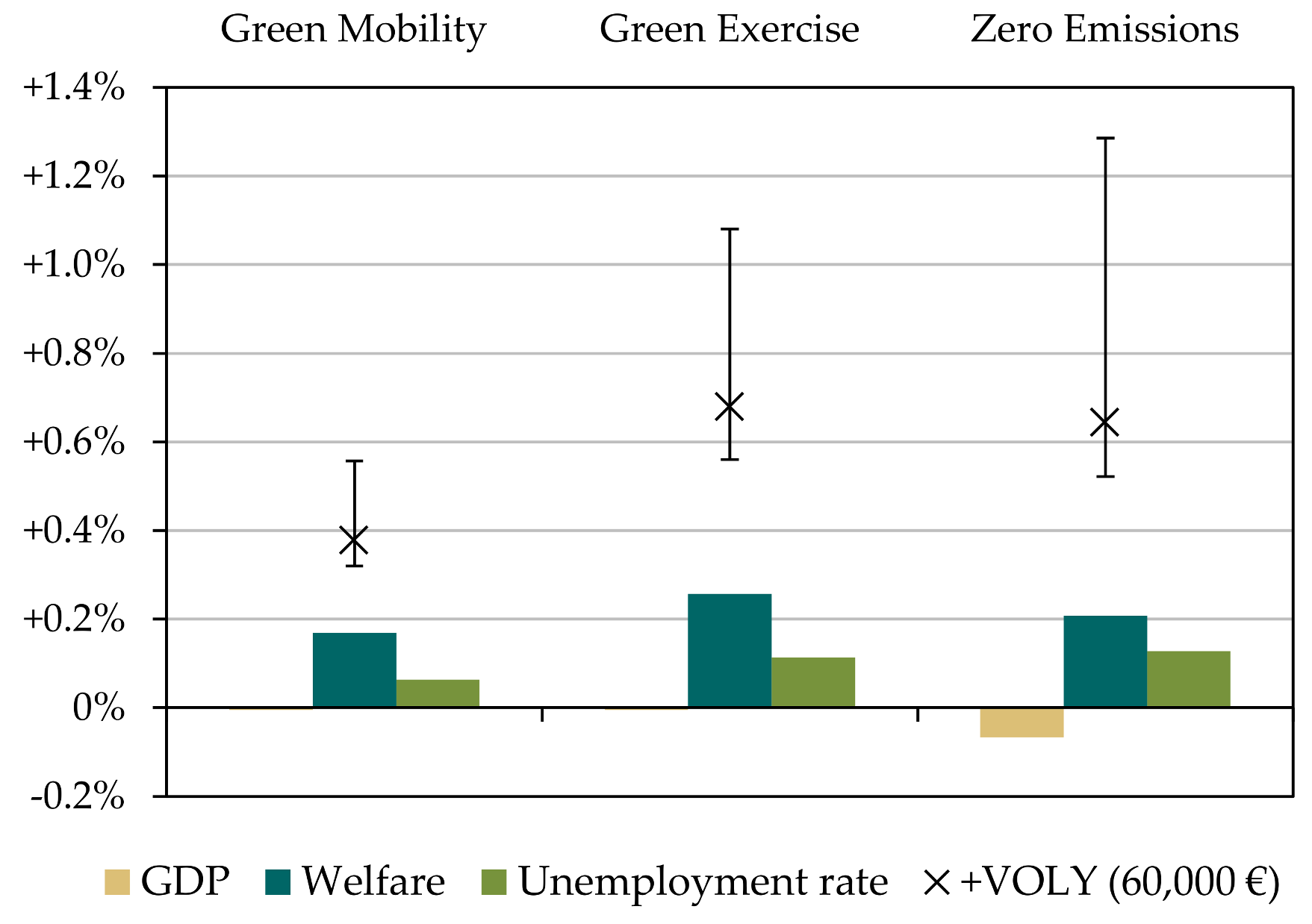
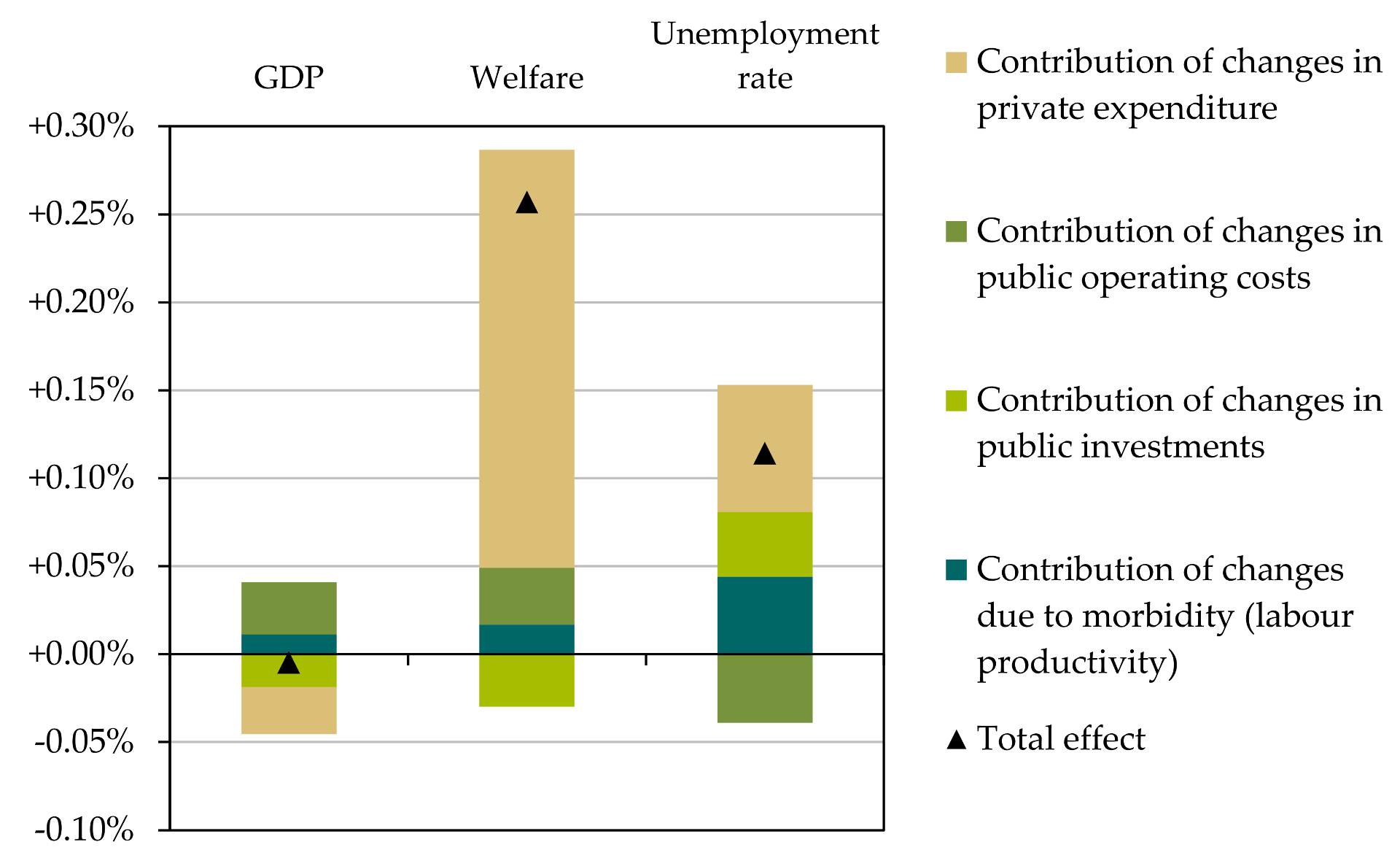
3.3.3. Macroeconomic Effects
3.4. Summary of Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| NACE Code | Activity/Industry | Model Code |
|---|---|---|
| V01 | Crop and animal production, hunting and related service activities | AGRI |
| V02 | Forestry and logging | FORE |
| V86 | Human health activities | HEAL |
| V87_88 | Residential care activities; Social work activities without accommodation | |
| V36 | Water collection, treatment and supply | WATE |
| V37_39 | Sewerage; Waste collection, treatment and disposal activities; materials recovery; Remediation activities and other waste management services | WAST |
| V35 | Electricity, gas, steam and air conditioning supply | ELEC |
| V19 | Manufacture of coke and refined petroleum products | COKE |
| V28 | Manufacture of machinery and equipment n.e.c.; Manufacture of electrical equipment | MACH |
| V29 | Manufacturing of cars | MACA |
| V30 | Manufacture of other transport equipment | MAVE |
| V41 | Construction of buildings | BUIL |
| V42 | Civil engineering | CIEN |
| V43 | Specialised construction activities | CONT |
| V68 | Real estate activities | REAL |
| V71 | Architectural and engineering activities; technical testing and analysis | ARCH |
| V45 | Wholesale and retail trade and repair services of motor vehicles and motorcycles | TRCA |
| V49 | Land transport and transport via pipelines | LTRA |
| V50 | Water transport | WTRA |
| V51 | Air transport | ATRA |
| V52_53 | Warehousing and support activities for transportation; Postal and courier activities | STRA |
| V10, V12 | Manufacture of food products; Manufacture of tobacco products | FOOD |
| V11 | Manufacture of beverages | BEVE |
| V16 | Manufacture of wood and of products of wood and cork, except furniture; manufacture of articles of straw and plaiting materials | WOOD |
| V17 | Manufacture of paper and paper products | PAPE |
| V20 | Manufacture of chemicals and chemical products | CHEM |
| V21 | Manufacture of basic pharmaceutical products and pharmaceutical preparations | PHAR |
| V22_23 | Manufacture of rubber and plastic products; Manufacture of other non-metallic mineral products | PLAS |
| V24 | Manufacture of basic metals | META |
| V25 | Manufacture of fabricated metal products, except machinery and equipment | MAME |
| V27 | Manufacture of electrical equipment; | MAEL |
| V13_14, V18, V26, V31_33 | Rest of manufacturing (Manufacture of textiles; Manufacture of wearing apparel; Printing and reproduction of recorded media; Manufacture of computer, electronic and optical products; Manufacture of furniture; Other manufacturing; Repair and installation of machinery and equipment) | RMAN |
| V15 | Manufacture of leather and related products | LEAT |
| V46_47 | Wholesale trade, except of motor vehicles and motorcycles; Retail trade, except of motor vehicles and motorcycles | TRAD |
| V64 | Financial service activities, except insurance and pension funding | FINA |
| V65 | Insurance, reinsurance and pension funding, except compulsory social security | INSU |
| V66 | Activities auxiliary to financial services and insurance activities | AFIN |
| V84 | Public administration and defence; compulsory social security | PUBL |
| V55_56 | Accommodation; Food and beverage service activities | ACCO |
| V79 | Travel agency, tour operator and other reservation service and related activities | TRAV |
| V90 | Creative, arts and entertainment activities | ENTE |
| V91 | Libraries, archives, museums and other cultural activities | CULT |
| V93 | Sports activities and amusement and recreation activities | SPOR |
| V03, V05_09 | Fishing and aquaculture; Mining of coal and lignite, Extraction of crude petroleum and natural gas, Mining of metal ores, Other mining and quarrying, Mining support service activities | REXT |
| V58 | Publishing activities | RECR |
| V59_60 | Motion picture, video and television programme production, sound recording and music publishing activities; Programming and broadcasting activities | |
| V92 | Gambling and betting activities | |
| V69_70 | Legal and accounting activities; Activities of head offices, management consultancy activities | SCIE |
| V72 | Scientific research and development | |
| V74_75 | Other professional, scientific and technical activities; Veterinary activities | |
| V61 | Telecommunications | TELE |
| V62_63 | Computer programming, consultancy and related activities; Information service activities | |
| V77 | Rental and leasing activities | RSER |
| V78 | Employment activities | |
| V80_82 | Security and investigation activities; Services to buildings and landscape activities; Office administrative, office support and other business support activities | |
| V85 | Education | |
| V94 | Activities of membership organisations | |
| V96 | Other personal service activities | |
| V97_98 | Activities of households as employers of domestic personnel; Undifferentiated goods- and services-producing activities of private households for own use | |
| V99 | Activities of extraterritorial organisations and bodies | |
| V73 | Advertising and market research | ADVE |
| V95 | Repair of computers and personal and household goods | REPA |
References
- Mueller, N.; Rojas-Rueda, D.; Basagaña, X.; Cirach, M.; Cole-Hunter, T.; Dadvand, P.; Donaire-Gonzalez, D.; Foraster, M.; Gascon, M.; Martinez, D.; et al. Urban and Transport Planning Related Exposures and Mortality: A Health Impact Assessment for Cities. Environ. Health Perspect. 2016, 125. [Google Scholar] [CrossRef] [PubMed]
- Perez, L.; Trüeb, S.; Cowie, H.; Keuken, M.P.; Mudu, P.; Ragettli, M.S.; Sarigiannis, D.A.; Tobollik, M.; Tuomisto, J.; Vienneau, D.; et al. Transport-related measures to mitigate climate change in Basel, Switzerland: A health-effectiveness comparison study. Environ. Int. 2015, 85, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Woodcock, J.; Givoni, M.; Morgan, A.S. Health Impact Modelling of Active Travel Visions for England and Wales Using an Integrated Transport and Health Impact Modelling Tool (ITHIM). PLoS ONE 2013, 8, e51462. [Google Scholar] [CrossRef] [PubMed]
- Rojas-Rueda, D.; de Nazelle, A.; Tainio, M.; Nieuwenhuijsen, M.J. The health risks and benefits of cycling in urban environments compared with car use: Health impact assessment study. BMJ 2011, 343, d4521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haines, A.; McMichael, A.J.; Smith, K.R.; Roberts, I.; Woodcock, J.; Markandya, A.; Armstrong, B.G.; Campbell-Lendrum, D.; Dangour, A.D.; Davies, M.; et al. Public health benefits of strategies to reduce greenhouse-gas emissions: Overview and implications for policy makers. Lancet 2009, 374, 2104–2114. [Google Scholar] [CrossRef]
- Woodcock, J.; Edwards, P.; Tonne, C.; Armstrong, B.G.; Ashiru, O.; Banister, D.; Beevers, S.; Chalabi, Z.; Chowdhury, Z.; Cohen, A.; et al. Public health benefits of strategies to reduce greenhouse-gas emissions: Urban land transport. Lancet 2009, 374, 1930–1943. [Google Scholar] [CrossRef]
- IPCC Summary for Policymakers. Climate Change 2014: Mitigation of Climate Change. Contribution of Working Group III to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change; Edenhofer, O., Pichs-Madruga, R., Sokona, Y., Farahani, E., Kadner, S., Seyboth, K., Adler, A., Baum, I., Brunner, S., Eickemeier, P., et al., Eds.; Cambridge University Press: Cambridge, UK; New York, NY, USA, 2014. [Google Scholar]
- Umweltbundesamt Hintergrundinformation—Treibhausgas-Bilanz 2016; Umweltbundesamt: Wien, Austria, 2017.
- Umweltbundesamt Ueberschreitungen 2017. Available online: http://www.umweltbundesamt.at/umweltsituation/luft/luftguete_aktuell/ueberschreitungen/ueberschreitungen_2017/ (accessed on 23 January 2018).
- Quam, V.; Rocklöv, J.; Quam, M.; Lucas, R. Assessing Greenhouse Gas Emissions and Health Co-Benefits: A Structured Review of Lifestyle-Related Climate Change Mitigation Strategies. Int. J. Environ. Res. Public Health 2017, 14, 468. [Google Scholar] [CrossRef] [PubMed]
- Shaw, C.; Hales, S.; Howden-Chapman, P.; Edwards, R. Health co-benefits of climate change mitigation policies in the transport sector. Nat. Clim. Chang. 2014, 4, 427–433. [Google Scholar] [CrossRef]
- Xia, T.; Zhang, Y.; Crabb, S.; Shah, P. Cobenefits of Replacing Car Trips with Alternative Transportation: A Review of Evidence and Methodological Issues. J. Environ. Public Health 2013, 2013. [Google Scholar] [CrossRef] [PubMed]
- Grabow, M.L.; Spak, S.N.; Holloway, T.; Stone, B.; Mednick, A.C.; Patz, J.A. Air Quality and Exercise-Related Health Benefits from Reduced Car Travel in the Midwestern United States. Environ. Health Perspect. 2011, 120, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, G.; Macmillan, A.; Woodward, A. Moving urban trips from cars to bicycles: Impact on health and emissions. Aust. N. Z. J. Public Health 2011, 35, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Maizlish, N.; Woodcock, J.; Co, S.; Ostro, B.; Fanai, A.; Fairley, D. Health Cobenefits and Transportation-Related Reductions in Greenhouse Gas Emissions in the San Francisco Bay Area. Am. J. Public Health 2013, 103, 703. [Google Scholar] [CrossRef] [PubMed]
- Holm, A.L.; Glümer, C.; Diderichsen, F. Health Impact Assessment of increased cycling to place of work or education in Copenhagen. BMJ Open 2012, 2, e001135. [Google Scholar] [CrossRef] [PubMed]
- Remais, J.V.; Hess, J.J.; Ebi, K.L.; Markandya, A.; Balbus, J.M.; Wilkinson, P.; Haines, A.; Chalabi, Z. Estimating the Health Effects of Greenhouse Gas Mitigation Strategies: Addressing Parametric, Model, and Valuation Challenges. Environ. Health Perspect. 2014. [Google Scholar] [CrossRef]
- Rutter, H.; Cavill, N.; Kahlmeier, S.; Racioppi, F.; Oja, P. Health Economic Assessment Tool for Cycling (HEAT for cycling) User guide Version 2; WHO Regional Office for Europe: Copenhagen, Denmark, 2008. [Google Scholar]
- Doll, C.; Hartwig, J.; Senger, F. The Private and Public Economics of Sustainable Mobility Patterns. In Proceedings of the 13th WCTR Conference, Rio De Janeiro, Brazil, 15–18 July 2013. [Google Scholar]
- Keogh-Brown, M.; Jensen, H.T.; Smith, R.D.; Chalabi, Z.; Davies, M.; Dangour, A.; Edwards, P.; Garnett, T.; Givoni, M.; Griffiths, U.; et al. A whole-economy model of the health co-benefits of strategies to reduce greenhouse gas emissions in the UK. Lancet 2012, 380, S52. [Google Scholar] [CrossRef]
- Jensen, H.T.; Keogh-Brown, M.R.; Smith, R.D.; Chalabi, Z.; Dangour, A.D.; Davies, M.; Edwards, P.; Garnett, T.; Givoni, M.; Griffiths, U.; et al. The importance of health co-benefits in macroeconomic assessments of UK Greenhouse Gas emission reduction strategies. Clim. Chang. 2013, 121, 223–237. [Google Scholar] [CrossRef] [PubMed]
- Hiess, H. Masterplan Verkehr Wien 2003 Evaluierung 2013; Werkstattbericht; Stadt Wien: Wien, Austria, 2013. [Google Scholar]
- Fallast, K.; Moser, M.; Eder, E.; Tischler, G. Regionales Verkehrskonzept Graz und Graz-Umgebung; Das Land Steiermark: Graz, Austria, 2010. [Google Scholar]
- City of Graz Mobilitätsstrategie der Stadt Graz; City of Graz: Graz, Austria, 2012.
- Sammer, G.; Röschel, G.; Gruber, C. Gesamtverkehrskonzept für den Großraum Linz, Verkehrspolitische Leitlinien—Maßnahmenprogramm; Auftraggeber und Projektleitung: Linz/Graz/Wien, Austria, 2012. [Google Scholar]
- IPCC Climate Change 2014 Synthesis Report Summary for Policymakers. In Climate Change 2014: Impacts, Adaptation, and Vulnerability. Part A: Global and Sectoral Aspects. Contribution of Working Group II to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change; Edenhofer, O.; Pichs-Madruga, R.; Sokona, Y.; Farahani, E.; Kadner, S.; Seyboth, K.; Adler, A.; Baum, I.; Brunner, S.; Eickemeier, P.; et al. (Eds.) Cambridge University Press: Cambridge, UK; New York, NY, USA, 2014. [Google Scholar]
- Statistics Austria Economically Active Persons by Category and Distance. Available online: http://www.stat.at/web_en/statistics/PeopleSociety/population/population_censuses_register_based_census_register_based_labour_market_statistics/commuters/index.html (accessed on 4 March 2017).
- Rexeis, M.; Hausberger, S. Calculation of Vehicle Emissions in Road Networks with the model “NEMO.”. In Proceedings of the 85/I 14th Symposium Transport and Air Pollution, Graz, Austria, 1–3 June 2005; pp. 118–127. [Google Scholar]
- Oettl, D. Documentation of the Lagrangian Particle Model GRAL, Graz Lagrangian Model Vs. 13.3; Amt der Steiermärkischen Landesregierung, FA17C; Technische Umweltkontrolle: Graz, Austria, 2013. [Google Scholar]
- Bachler, G.; Karner, M.; Kurz, C.; Reifeltshammer, R.; Sturm, P. Modellierung von Verkehrsszenarien im Rahmen des ACRP—Projektes ClimbHealth; IVT I-05/16/Ku V&U I-14/13/630 V3.0; IVT-TUGRAZ: Graz, Austria, 2016. [Google Scholar]
- Arem, H.; Moore, S.C.; Patel, A.; Hartge, P.; Berrington de Gonzalez, A.; Visvanathan, K.; Campbell, P.T.; Freedman, M.; Weiderpass, E.; Adami, H.O.; et al. Leisure Time Physical Activity and Mortality: A Detailed Pooled Analysis of the Dose-Response Relationship. JAMA Intern. Med. 2015, 175, 959. [Google Scholar] [CrossRef] [PubMed]
- Kelly, P.; Kahlmeier, S.; Götschi, T.; Orsini, N.; Richards, J.; Roberts, N.; Scarborough, P.; Foster, C. Systematic review and meta-analysis of reduction in all-cause mortality from walking and cycling and shape of dose response relationship. Int. J. Behav. Nutr. Phys. Act. 2014, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woodcock, J.; Franco, O.H.; Orsini, N.; Roberts, I. Non-vigorous physical activity and all-cause mortality: Systematic review and meta-analysis of cohort studies. Int. J. Epidemiol. 2011, 40, 121–138. [Google Scholar] [CrossRef] [PubMed]
- Bull, F.C.; Armstrong, T.P.; Dixon, T.; Ham, S.; Neiman, A.; Pratt, M. Physical inactivity. In Comparative Quantification of Health Risks Global and Regional Burden of Disease Attributable to Selected Major Risk Factors; Ezzati, M., Lopez, A.D., Rodgers, A., Murray, C.J.L., Eds.; WHO: Geneva, Switzerland, 2004; Volume 1, pp. 729–881. [Google Scholar]
- Jetté, M.; Sidney, K.; Blümchen, G. Metabolic equivalents (METS) in exercise testing, exercise prescription, and evaluation of functional capacity. Clin. Cardiol. 1990, 13, 555–565. [Google Scholar] [CrossRef] [PubMed]
- Stare, J.; Maucort-Boulch, D. Odds Ratio, Hazard Ratio and Relative Risk. Metodoloski Zv. 2016, 13, 59–67. [Google Scholar]
- WHO ICD-10 International statistical classification of diseases and related health problems. Available online: http://www.who.int/classifications/icd/en/ (accessed on 26 January 2018).
- Statistics Austria Population by Demographic Characteristics. Available online: https://www.statistik.at/web_en/statistics/PeopleSociety/population/population_change_by_demographic_characteristics/index.html (accessed on 20 February 2018).
- Statistics Austria Causes of Deaths; STAT: Vienna, Austria, 2018.
- IHME—Institute for Health Metrics and Evaluation. Global Burden of Disease Study 2015 (GBD 2015) Results; IHME—Institute for Health Metrics and Evaluation: Seattle, WA, USA, 2016. [Google Scholar]
- Künzli, N.; Kaiser, R.; Medina, S.; Studnicka, M.; Chanel, O.; Filliger, P.; Herry, M.; Horak, F.; Puybonnieux-Texier, V.; Quénel, P.; et al. Public-health impact of outdoor and traffic-related air pollution: A European assessment. Lancet 2000, 356, 795–801. [Google Scholar] [CrossRef]
- Hoek, G.; Krishnan, R.M.; Beelen, R.; Peters, A.; Ostro, B.; Brunekreef, B.; Kaufman, J.D. Long-term air pollution exposure and cardio- respiratory mortality: A review. Environ. Health 2013, 12. [Google Scholar] [CrossRef] [PubMed]
- Raaschou-Nielsen, O.; Andersen, Z.J.; Beelen, R.; Samoli, E.; Stafoggia, M.; Weinmayr, G.; Hoffmann, B.; Fischer, P.; Nieuwenhuijsen, M.J.; Brunekreef, B.; et al. Air pollution and lung cancer incidence in 17 European cohorts: Prospective analyses from the European Study of Cohorts for Air Pollution Effects (ESCAPE). Lancet Oncol. 2013, 14, 813–822. [Google Scholar] [CrossRef]
- Faustini, A.; Rapp, R.; Forastiere, F. Nitrogen dioxide and mortality: Review and meta-analysis of long-term studies. Eur. Respir. J. 2014, 44, 744–753. [Google Scholar] [CrossRef] [PubMed]
- Cesaroni, G.; Forastiere, F.; Stafoggia, M.; Andersen, Z.J.; Badaloni, C.; Beelen, R.; Caracciolo, B.; de Faire, U.; Erbel, R.; Eriksen, K.T.; et al. Long term exposure to ambient air pollution and incidence of acute coronary events: Prospective cohort study and meta-analysis in 11 European cohorts from the ESCAPE Project. BMJ 2014, 348, f7412. [Google Scholar] [CrossRef] [PubMed]
- Vienneau, D.; Perez, L.; Schindler, C.; Lieb, C.; Sommer, H.; Probst-Hensch, N.; Künzli, N.; Röösli, M. Years of life lost and morbidity cases attributable to transportation noise and air pollution: A comparative health risk assessment for Switzerland in 2010. Int. J. Hyg. Environ. Health 2015, 218, 514–521. [Google Scholar] [CrossRef] [PubMed]
- Statistics Austria Cancer Incidence, Overview; STAT: Vienna, Austria, 2017.
- Federal Ministry of Labour. Social Affairs and Consumer Protection Stationäre Aufenthalte (KJ) 2007–2016; Federal Ministry of Labour: Vienna, Austria, 2017. [Google Scholar]
- Statistics Austria OENACE 2008—Structure. Available online: http://www.statistik.at/KDBWeb/kdb_VersionAuswahl.do?FAM=WZWEIG&NAV=DE&VersID=10438&EXT=J&KDBtoken=? (accessed on 21 February 2018).
- Statistics Austria Household Budget Survey 2009/2010; STAT: Vienna, Austria, 2011.
- Hausberger, S. Erstellung globaler Emissionsdaten für Österreichische Kfz von 1950 bis 2030; Technical University of Graz: Graz, Austria, 2010. [Google Scholar]
- Jo, C. Cost-of-illness studies: Concepts, scopes, and methods. Clin. Mol. Hepatol. 2014, 20, 327–337. [Google Scholar] [CrossRef] [PubMed]
- Walter, E.; Zehetmayr, S. Theoretische Implikationen zur gesundheitsökonomischen Evaluation mit Ausblick auf Österreich. Wien. Med. Wochenschr. 2006, 156, 622–627. [Google Scholar] [CrossRef] [PubMed]
- Haucke, F.; Holle, R.; Wichmann, H.E. Epidemiologische Erforschung und ökonomische Bewertung gesundheitlicher Umweltrisiken. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2009, 52, 1166–1178. [Google Scholar] [CrossRef] [PubMed]
- Le, C.; Lin, L.; Jun, D.; Jianhui, H.; Keying, Z.; Wenlong, C.; Ying, S.; Tao, W. The economic burden of type 2 diabetes mellitus in rural southwest China. Int. J. Cardiol. 2013, 165, 273–277. [Google Scholar] [CrossRef] [PubMed]
- Holland, M. Cost-Benefit Analysis of Final Policy Scenarios for the EU Clean Air Package—Version 2; EMRC: London, UK, 2014. [Google Scholar]
- Bickel, P.; Friedrich, R. ExternE: Externalities of Energy : Methodology 2005 Update; Office for Official Publications of the European Communities: Luxembourg, 2005. [Google Scholar]
- Desaigues, B.; Ami, D.; Bartczak, A.; Braun-Kohlová, M.; Chilton, S.; Czajkowski, M.; Farreras, V.; Hunt, A.; Hutchison, M.; Jeanrenaud, C.; et al. Economic valuation of air pollution mortality: A 9-country contingent valuation survey of value of a life year (VOLY). Ecol. Indic. 2011, 11, 902–910. [Google Scholar] [CrossRef]
- Statistics Austria Consumer Price Index (CPI 2005). Available online: http://www.statistik.at/web_en/statistics/Economy/Prices/consumer_price_index_cpi_hcpi/index.html (accessed on 27 March 2018).
- D 5.3.1/2 Methods and results of the HEIMTSA/INTARESE Common Case Study; University of Stuttgart: Stuttgart, Germany, 2011.
- Zsifkovits, J. Krankheitsausgabenrechnung für das Jahr 2008 (2012); Gesundheit Österreich: Vienna, Austria, 2012. [Google Scholar]
- Alt, R.; Binder, A.; Helmenstein, C.; Kleissner, A.; Krabb, P. Der volkswirtschaftliche Nutzen von Bewegung Volkswirtschaftlicher Nutzen von Bewegung, volkswirtschaftliche Kosten von Inaktivität und Potenziale von mehr Bewegung; SpEA SportsEconAustria: Wien, Austria, 2015. [Google Scholar]
- Brown, M.L.; Lipscomb, J.; Snyder, C. The Burden of Illness of Cancer: Economic Cost and Quality of Life. Annu. Rev. Public Health 2001, 22, 91–113. [Google Scholar] [CrossRef] [PubMed]
- Leoni, T. Fehlzeitenreport 2011. Krankheits- und unfallbedingte Fehlzeiten in Österreich. In Monographien; WIFO: Vienna, Austria, 2011. [Google Scholar]
- Pritchard, C.; Sculpher, M. Productivity Costs: Principles and Practice in Economic Evaluation; Off. of Health Economics: London, UK, 2000; ISBN 978-1-899040-76-6. [Google Scholar]
- Bachner, G. Assessing the economy-wide effects of climate change adaptation options of land transport systems in Austria. Reg. Environ. Chang. 2017. [Google Scholar] [CrossRef]
- Armington, P.S. A Theory of Demand for Products Distinguished by Place of Production (Une théorie de la demande de produits différenciés d’après leur origine) (Una teoría de la demanda de productos distinguiéndolos según el lugar de producción). Staff Pap. Int. Monet. Fund 1969, 16, 159–178. [Google Scholar] [CrossRef]
- Lofgren, H.; Haris, R.L.; Robinson, S. A Standard Computable General Equilibrium (CGE) Model in GAMS; International Food Policy Research Institute: Washington, DC, USA, 2002. [Google Scholar]
- WHO Health Statistics and Information Systems. Available online: http://www.who.int/healthinfo/global_burden_disease/metrics_daly/en/ (accessed on 26 January 2018).
- Jack, D.W.; Kinney, P.L. Health co-benefits of climate mitigation in urban areas. Curr. Opin. Environ. Sustain. 2010, 2, 172–177. [Google Scholar] [CrossRef]
- Bachner, G.; Bednar-Friedl, B.; Nabernegg, S.; Steininger, K.W. Macroeconomic Evaluation of Climate Change in Austria: A Comparison Across Impact Fields and Total Effects. In Economic Evaluation of Climate Change Impacts: Development of a Cross-Sectoral Framework and Results for Austria; Steininger, K.W., König, M., Bednar-Friedl, B., Kranzl, L., Loibl, W., Prettenthaler, F., Eds.; Springer: Berlin, Germany, 2015; pp. 415–440. [Google Scholar]
- De Nazelle, A.; Nieuwenhuijsen, M.J.; Antó, J.M.; Brauer, M.; Briggs, D.; Braun-Fahrlander, C.; Cavill, N.; Cooper, A.R.; Desqueyroux, H.; Fruin, S.; et al. Improving health through policies that promote active travel: A review of evidence to support integrated health impact assessment. Environ. Int. 2011, 37, 766–777. [Google Scholar] [CrossRef] [PubMed]
- Boniface, S.; Scantlebury, R.; Watkins, S.J.; Mindell, J.S. Health implications of transport: Evidence of effects of transport on social interactions. J. Transp. Health 2015, 2, 441–446. [Google Scholar] [CrossRef]
- Van Essen, H.; Schroten, A.; Otten, M.; Sutter, D.; Schreyer, C.; Zandonella, R.; Maibach, M.; Doll, C. External Costs of Transport in Europe Update Study 2008; CE Delft: Delft, The Netherlands, 2011. [Google Scholar]
- Rabl, A.; Spadaro, J.; Holland, M. How Much Is Clean Air Worth?: Calculating the Benefits of Pollution Control; Cambridge University Press: Cambridge, UK; New York, NY, USA, 2014. [Google Scholar]
- Markandya, A.; Sampedro, J.; Smith, S.J.; Van Dingenen, R.; Pizarro-Irizar, C.; Arto, I.; González-Eguino, M. Health co-benefits from air pollution and mitigation costs of the Paris Agreement: A modelling study. Lancet Planet. Health 2018, 2, e126–e133. [Google Scholar] [CrossRef]
- Bollen, J.; van der Zwaan, B.; Brink, C.; Eerens, H. Local air pollution and global climate change: A combined cost-benefit analysis. Resour. Energy Econ. 2009, 31, 161–181. [Google Scholar] [CrossRef]












| Shifted Trips [%] | Pedestrian | Bike | Public Transport | E-Car | E-Bike | |
|---|---|---|---|---|---|---|
| Domestic Transport | ||||||
| 0.01–0.99 km | 65 | 8% | 83% | 7% | 1% | 1% |
| 1.00–1.99 km | 50 | 5% | 85% | 8% | 1% | 1% |
| 2.00–2.99 km | 45 | 0% | 75% | 23% | 1% | 1% |
| 3.00–4.99 km | 35 | 0% | 55% | 43% | 1% | 1% |
| 5.00–9.99 km | 25 | 0% | 45% | 53% | 1% | 1% |
| Commuter Transport | ||||||
| 10.00–14.99 km | 20 | 5% | 93% | 1% | 1% | |
| >=15 km | 20 | 99% | 1% | 0% |
| City | Graz | Linz | Vienna | |||
|---|---|---|---|---|---|---|
| Scenario | GM | GE | GM | GE | GM | GE |
| Hazard Risk (HR) | 0.773 | 0.770 | 0.765 | 0.767 | 0.772 | 0.769 |
| Health endpoints | NO2 | PM2.5 | PM10 |
|---|---|---|---|
| Atraumatic mortality | 1.04 (1.02–1.06) [44] | 1.05 (1.01–1.09) [44] | 1.045 (1.029–1.060) ** [46] |
| Cardiovascular mortality | 1.13 (1.09–1.18) [44] | 1.20 (1.09–1.31) [44] | - |
| Respiratory mortality | 1.03 (1.02–1.03) [44] | 1.05 (1.01–1.09) [44] | - |
| Coronary events (HR) incidence (acute myocardial infarction) | - | 1.13 (0.98–1.30) [45] | 1.12 (1.01–1.25) [45] |
| Lung cancer (HR) incidence | - | 1.18 * (0.96–1.46) [43] | 1.22 (1.03–1.45) [43] |
| Cardiovascular hospital admissions (all ages) | - | - | 1.013 (1.007–1.019) [41] |
| Respiratory hospital admissions (all ages) | - | - | 1.013 (1.001–1.025) [41] |
| Disease | Mean Number of Days of Sick Leave per Year |
|---|---|
| Myocardial infarction | 37.5 |
| Lung cancer | 75.0 |
| Changes in mileage by city | Green Mobility | Green Exercise (Zero Emission) |
|---|---|---|
| Changes in car-km relative to the baseline (million km and %) | ||
| Vienna | −1306 (−32%) | −2241 (−55%) |
| Graz | −276 (−24%) | −564 (−48%) |
| Linz | −166 (−16%) | −416 (−41%) |
| Changes in bus-km relative to the baseline (%) | ||
| Vienna | 17.8% | 19.8% |
| Graz | 15.9% | 34.6% |
| Linz | 4.7% | 21.6% |
| Scenario | Pedestrian | Biker | E-Biker | |||
|---|---|---|---|---|---|---|
| Persons | Minutes | Persons | Minutes | Persons | Minutes | |
| Graz GM | 675 | +167 | 18,599 | +178 | 734 | +173 |
| Graz GE | 8666 | +217 | 37,673 | +206 | 3101 | +263 |
| Linz GM | 588 | +187 | 10,872 | +237 | 416 | +187 |
| Linz GE | 3954 | +227 | 20,398 | +233 | 1754 | +287 |
| Vienna GM | 5014 | +212 | 153,939 | +180 | 4702 | +160 |
| Vienna GE | 71,013 | +239 | 254,449 | +214 | 12,662 | +258 |
| Death Cases | Cause (activity, air quality) | Green Mobility | Green Exercise | Zero Emissions |
|---|---|---|---|---|
| Atraumatic Mortality | Physical Activity | −417 | −891 | −891 |
| NO2 | −88 | −185 | −421 | |
| PM2.5 | −48 | −58 | −65 | |
| PM10 | −41 | −70 | −91 | |
| Cardiovascular Diseases | NO2 | −135 | −284 | −647 |
| PM2.5 | −91 | −110 | −123 | |
| Respiratory Diseases | NO2 | −4 | −8 | −18 |
| PM2.5 | −3 | −3 | −4 |
| Changes in | Graz | Linz | Vienna | ||||||
|---|---|---|---|---|---|---|---|---|---|
| GM | GE | ZE | GM | GE | ZE | GM | GE | ZE | |
| Cardiovascular mortality NO2 | −26 | −48 | −99 | −1 | −14 | −50 | −107 | −222 | −498 |
| Respiratory mortality NO2 | −1 | −1 | −3 | 0 | −1 | −2 | −3 | −6 | −13 |
| Myocardial infarction Incidence PM10 | −4 (−0.07) | −8 (−0.1) | −10 (−0.1) | −3 (−0.02) | −6 (−0.05) | −7 (−0.08) | −20 (−0.3) | −34 (−0.5) | −43 (−0.7) |
| Lung cancer (HR) Incidence PM2.5 | −2 (−0.2) | −3 (−0.3) | −4 (−0.4) | −1 (−0.03) | −1 (−0.09) | −1 (−0.2) | −20 (−2.0) | −23 (−2.3) | −25 (−2.5) |
| Cardiovascular hospital admissions PM10 | −8 | −14 | −17 | −3 | −7 | −12 | −34 | −57 | −72 |
| Respiratory hospital admissions PM10 | −5 | −8 | −10 | −2 | −4 | −7 | −18 | −31 | −39 |
| Direct and indirect health costs and intangible costs | Green Mobility | Green Exercise | Zero Emissions |
|---|---|---|---|
| Changes due to improved air quality | |||
| Direct costs (in €1000) | |||
| Acute in-patient treatment including medicine | −2850 | −3940 | −4680 |
| Indirect costs | |||
| Morbidity (work absence in days) | −2740 | −3730 | −4350 |
| Morbidity (in 1000 €) | −280 | −380 | −440 |
| Mortality (number of persons) | −135 | −284 | −647 |
| Mortality (in 1000 €) | −4290 | −4400 | −4600 |
| Changes due to increased physical activity | |||
| Direct and indirect costs (in 1000 €) | −4350 | −9200 | −9200 |
| Mortality (number of persons) | −417 | −891 | −891 |
| Total changes of direct and indirect costs (air quality and increased physical activity) (in 1000 €) | −11,770 | −17,920 | −18,920 |
| Changes in intangible costs due to improved air quality and increased physical activity (in 1000 €) | |||
| VOLY (€43,000) | −352,700 | −715,600 | −738,500 |
| VOLY (€60,000) | −490,400 | −995,000 | −1,026,800 |
| VSL (€1,650,000) | −910,900 | −1,938,900 | −2,537,400 |
| Summary of co-benefits | Green Mobility | Green Exercise | Zero Emissions |
|---|---|---|---|
| Mortality (death cases) | |||
| Air Quality | −135 | −284 | −647 |
| Physical Activity | −417 | −891 | −891 |
| GHG emissions | |||
| (t CO2equ) | −289,680 | −534,260 | −956,500 |
| Direct and indirect health costs | |||
| (1000 € per year) | −11,800 | −18,000 | −19,000 |
| Intangible costs VSL | |||
| (1000 € per year) | −910,900 | −1,938,900 | −2,537,400 |
| Macroeconomic Effects [%] | |||
| GDP | −0.01% | −0.00% | −0.07% |
| Welfare | +0.2% | +0.3% | +0.2% |
| Employment | +0.1% | +0.1% | +0.1% |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wolkinger, B.; Haas, W.; Bachner, G.; Weisz, U.; Steininger, K.W.; Hutter, H.-P.; Delcour, J.; Griebler, R.; Mittelbach, B.; Maier, P.; et al. Evaluating Health Co-Benefits of Climate Change Mitigation in Urban Mobility. Int. J. Environ. Res. Public Health 2018, 15, 880. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15050880
Wolkinger B, Haas W, Bachner G, Weisz U, Steininger KW, Hutter H-P, Delcour J, Griebler R, Mittelbach B, Maier P, et al. Evaluating Health Co-Benefits of Climate Change Mitigation in Urban Mobility. International Journal of Environmental Research and Public Health. 2018; 15(5):880. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15050880
Chicago/Turabian StyleWolkinger, Brigitte, Willi Haas, Gabriel Bachner, Ulli Weisz, Karl W. Steininger, Hans-Peter Hutter, Jennifer Delcour, Robert Griebler, Bernhard Mittelbach, Philipp Maier, and et al. 2018. "Evaluating Health Co-Benefits of Climate Change Mitigation in Urban Mobility" International Journal of Environmental Research and Public Health 15, no. 5: 880. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15050880