Aluminum Adjuvant-Containing Vaccines in the Context of the Hygiene Hypothesis: A Risk Factor for Eosinophilia and Allergy in a Genetically Susceptible Subpopulation?

{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Aluminum Adjuvants, IL-5 and Eosinophils
3. The Immune Response to Aluminum Adjuvants vs. Helminth Infections, and the Hygiene Hypothesis and Emerging Microbiome Theory
3.1. Aluminum Adjuvants vs. Helminth Infections
3.2. The Hygiene Hypothesis and Emerging Microbiome Theory
3.3. An Alternative View
3.4. Aluminum Adjuvants and Immunotherapy
4. Susceptibility in a Subpopulation Genetically Predisposed to Allergic Diseases
4.1. Features of a Genetically Susceptible Subpopulation
4.2. Aluminum Adjuvants in a Genetically Susceptible Subpopulation
5. Differences between Mice and Humans
6. Conclusions
Author Contributions
Conflicts of Interest
References
- Global Advisory Committee on Vaccine Safety (GACVS). WHO secretariat. Global safety of vaccines: Strengthening systems for monitoring, management and the role of GACVS. Expert Rev. Vaccines 2009, 8, 705–716. [Google Scholar]
- Kelso, J.M. Update on vaccination guidelines for allergic children. Expert Rev. Vaccines 2009, 8, 1541–1546. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Recommended Immunization Schedules for Persons Aged 0 Through 18 Years, USA, 2016. Available online: http://www.cdc.gov/vaccines/schedules/downloads/child/0-18yrs-child-combined-schedule.pdf (accessed on 14 April 2017).
- Adachi, T.; Alam, R. The mechanism of IL-5 signal transduction. Am. J. Physiol. 1998, 275, C623–C633. [Google Scholar] [CrossRef] [PubMed]
- Takatsu, K.; Nakajima, H. IL-5 and eosinophilia. Curr. Opin. Immunol. 2008, 20, 288–294. [Google Scholar] [CrossRef] [PubMed]
- Rothenberg, M.E.; Hogan, S.P. The eosinophil. Annu. Rev. Immunol. 2006, 24, 147–174. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, H.; Takatsu, K. Role of cytokines in allergic inflammation. Int. Arch. Allergy Immunol. 2007, 142, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Ustun, S.; Turgay, N.; Delibas, S.B.; Ertabaklar, H. Interleukin (IL) 5 levels and eosinophilia in patients with intestinal parasitic diseases. World J. Gastroenterol. 2004, 10, 3643–3646. [Google Scholar] [CrossRef] [PubMed]
- Garofalo, R.; Kimpen, J.L.; Welliver, R.C.; Ogra, P.L. Eosinophil degranulation in the respiratory tract during naturally acquired respiratory syncytial virus infection. J. Pediatr. 1992, 120, 28–32. [Google Scholar] [CrossRef]
- Greenfeder, S.; Umland, S.P.; Cuss, F.M.; Chapman, R.W.; Egan, R.W. Th2 cytokines and asthma, the role of interleukin-5 in allergic eosinophilic disease. Respir. Res. 2001, 2, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Brewer, J.M.; Conacher, M.; Hunter, C.A.; Mohrs, M.; Brombacher, F.; Alexander, J. Aluminum Hydroxide Adjuvant Initiates Strong Antigen-Specific Th2 Responses in Absence of IL-4- or IL-13-Mediated Signaling. J. Immunol. 1999, 163, 6448–6454. [Google Scholar] [PubMed]
- Sokolovska, A.; Hem, S.L.; HogenEsch, H. Activation of dendritic cells and induction of CD4+ T cell differentiation by aluminum-containing adjuvants. Vaccine 2007, 25, 4575–4585. [Google Scholar] [CrossRef] [PubMed]
- Mckee, A.S.; Munks, M.W.; MacLeod, M.K.L.; Fleenor, C.J.; Rooijen, N.V.; Kapper, J.W.; Marrack, P. Alum Induces Innate Immune Responses through Macrophage and Mast Cell Sensors, but These Sensors Are Not Required for Alum to Act as an Adjuvant for Specific Immunity. J. Immunol. 2009, 183, 4403–4414. [Google Scholar] [CrossRef] [PubMed]
- Cain, D.W.; Sanders, S.E.; Cunningham, M.M.; Kelsoe, G. Disparate adjuvant properties among three formulations of “alum”. Vaccine 2013, 31, 653–660. [Google Scholar] [CrossRef] [PubMed]
- Rose, W.A.; Okragly, A.J.; Patel, C.N.; Benschop, R.J. IL-33 released by alum is responsible for early cytokine production and has adjuvant properties. Sci. Rep. 2015, 5, 13146. [Google Scholar] [CrossRef] [PubMed]
- Foster, P.S.; Hogan, S.P.; Ramsay, A.J.; Matthaei, K.I.; Young, I.G. Interleukin 5 Deficiency Abolishes Eosinophilia, Airways Hyperreactivity, and Lung Damage in a Mouse Asthma Model. J. Exp. Med. 1996, 183, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Cooper, P.D. The selective induction of different immune responses by vaccine adjuvants. In Strategies in Vaccine Design; Ada, G.L., Ed.; R.G. Lands Company: Austin, TX, USA, 1994; pp. 125–158. [Google Scholar]
- Mckee, A.; MacLeod, M.; White, J.; Crawford, F.; Kappler, J.; Marrack, P. Gr1+IL-4 producing innate cells are induced in response to Th2 stimuli and suppress Th1-dependent antibody responses. Int. Immunol. 2008, 20, 659–669. [Google Scholar] [CrossRef] [PubMed]
- Walls, R.S. Eosinophil Response to Alum Adjuvants. Involvement of T Cells in Non-Antigen-Dependent Mechanisms. Proc. Soc. Exp. Biol. Med. 1977, 156, 431–435. [Google Scholar] [CrossRef] [PubMed]
- Liesveld, J.; Reagan, P. Eosinophilia. Merck Manual 2014. Available online: http://www.merckmanuals.com/professional/hematology-and-oncology/eosinophilic-disorders/eosinophilia (accessed on 24 April 2017).
- Kouro, T.; Takatsu, K. IL-5- and eosinophil-meditated inflammation: From discovery to therapy. Int. Immunol. 2009, 21, 1303–1309. [Google Scholar] [CrossRef] [PubMed]
- Kotsimbos, A.T.; Humbert, M.; Minshall, E.; Durham, S.; Pfister, R.; Menz, G. Upregulation of alpha GM-CSF-receptor in nonatopic asthma but not in atopic asthma. J. Allergy Clin. Immunol. 1997, 99, 666–672. [Google Scholar] [CrossRef]
- Amin, K.; Ludviksdottir, D.; Janson, C.; Nettelbladt, O.; Björnsson, E.; Roomans, G.M.; Boman, G.; Sevéus, L.; Venge, P. Inflammation and structural changes in the airways of patients with atopic and nonatopic asthma. BHR Group. Am. J. Respir. Crit. Care Med. 2000, 162, 2295–2301. [Google Scholar] [CrossRef] [PubMed]
- Uehara, M.; Izukura, R.; Sawai, T. Blood eosinophilia in atopic dermatitis. Clin. Exp. Dermatol. 1990, 15, 264–266. [Google Scholar] [CrossRef] [PubMed]
- Böttcher, M.F.; Bjurström, J.; Mai, X.M.; Nilsson, L.; Jenmaim, M.C. Allergen-induced cytokine secretion in atopic and non-atopic asthmatic children. Pediatr. Allergy Immunol. 2003, 14, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Turkeli, A.; Yilmaz, O.; Taneli, F.; Horasan, G.D.; Kanik, E.T.; Kizilkaya, M. IL-5, IL-8 and MMP -9 levels in exhaled breath condensate of atopic and nonatopic asthmatic children. Respir. Med. 2015, 109, 680–688. [Google Scholar] [CrossRef] [PubMed]
- Toma, T.; Mizuno, K.; Okamoto, H.; Kanegane, C.; Ohta, K.; Ikawa, Y.; Miura, M.; Kuroda, M.; Niida, Y.; Koizumi, S.; et al. Expansion of activated eosinophils in infants with severe atopic dermatitis. Pediatr. Int. 2005, 47, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Romagnani, S. The increased prevalence of allergy and the hygiene hypothesis: Missing immune deviation, reduced immune suppression, or both? Immunology 2004, 112, 352–363. [Google Scholar] [CrossRef] [PubMed]
- Riiser, A. The human microbiome, asthma, and allergy. Allergy Asthma Clin. Immunol. 2015, 11, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kool, M.; Willart, M.A.; van Nimwegen, M.; Bergen, I.; Pouliot, P.; Virchow, J.C.; Rogers, N.; Osorio, F.; Reis e Sousa, C.; Hammad, H.; et al. An Unexpected Role for Uric Acid as an Inducer of T Helper 2 Cell Immunity to Inhaled Antigens and Inflammatory Mediator of Allergic Asthma. Immunity 2011, 34, 527–540. [Google Scholar] [CrossRef] [PubMed]
- Kopf, M.; Brombacher, F.; Hodgkin, P.D.; Ramsay, A.J.; Milbourne, E.A.; Dai, W.J.; Ovington, K.S.; Behm, C.A.; Köhler, G.; Young, I.G.; et al. IL-5-deficient mice have a developmental defect in CD5+ B-1 cells and lack eosinophilia but have normal antibody and cytotoxic T cell responses. Immunity 1996, 4, 15–24. [Google Scholar] [CrossRef]
- Jordan, M.B.; Millis, D.M.; Kappler, J.; Marrack, P.; Cambier, J.C. Promotion of B cell immune responses via an alum-induced myeloid cell population. Science 2004, 304, 1808–1810. [Google Scholar] [CrossRef] [PubMed]
- Chu, V.T.; Berek, C. Immunization induces activation of bone marrow eosinophils required for plasma cell survival. Eur. J. Immunol. 2012, 42, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Kita, H. Eosinophils: Multifaceted biological properties and roles in health and disease. Immunol. Rev. 2011, 242, 161–177. [Google Scholar] [CrossRef] [PubMed]
- Wong, T.W.; Doyle, A.D.; Lee, J.J.; Jelinek, D.F. Eosinophils Regulate Peripheral B Cell Numbers in Both Mice and Humans. J. Immunol. 2014, 192, 3548–3558. [Google Scholar] [CrossRef] [PubMed]
- Wong, T.W.; Kita, H.; Hanson, C.A.; Walters, D.K.; Arendt, B.K.; Jelinek, D.F. Induction of malignant plasma cell proliferation by eosinophils. PLoS ONE 2013, 8, e70554. [Google Scholar] [CrossRef] [PubMed]
- Sabin, E.A.; Kopf, M.A.; Pearce, E.J. Schistosoma mansoni egg induced early IL-4 production is dependent upon IL-5 and eosinophils. J. Exp. Med. 1996, 184, 1871–1878. [Google Scholar] [CrossRef] [PubMed]
- Wynn, T.A.; Thompson, R.W.; Cheever, A.W.; Mentink-Kane, M.M. Immunopathogenesis of schistosomiasis. Immunol. Rev. 2004, 201, 156–167. [Google Scholar] [CrossRef] [PubMed]
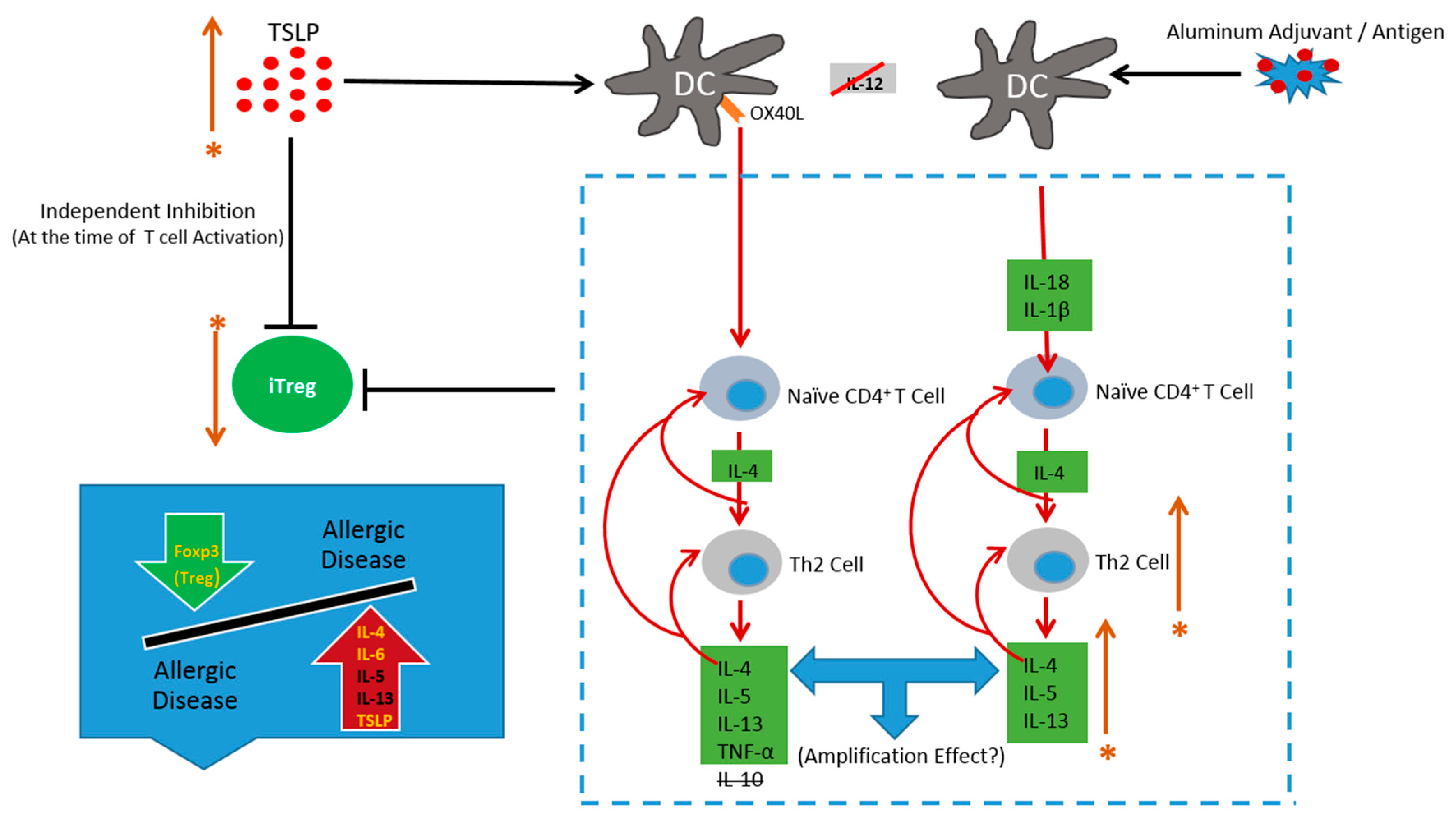
- Mori, A.; Oleszycka, E.; Sharp, F.A.; Coleman, M.; Ozasa, Y.; Singh, M.; O’Hagan, D.T.; Tajber, L.; Corrigan, O.I.; McNeela, E.A; et al. The vaccine adjuvant alum inhibits IL-12 by promoting PI3 kinase signaling while chitosan does not inhibit IL-12 and enhances Th1 and Th17 responses. Eur. J. Immunol. 2012, 42, 2709–2719. [Google Scholar] [CrossRef] [PubMed]
- Crater, S.E.; Platts-Mills, T.A. Searching for the cause of the increase in asthma. Curr. Opin. Pediatr. 1998, 10, 594–599. [Google Scholar] [CrossRef] [PubMed]
- Strachan, D.P. Hay fever, hygiene, and household size. Br. Med. J. 1989, 299, 1259–1260. [Google Scholar] [CrossRef]
- Lynch, N.R.; Lopez, R.I.; Di Prisco-Fuenmayor, M.C.; Hagel, I.; Medouze, L.; Viana, G.; Ortega, C.; Prato, G. Allergic reactivity and socio-economic level in a tropical environment. Clin. Allergy 1987, 17, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Hagel, I.; Lynch, N.R.; Di Prisco, M.C.; Lopez, R.I.; Garcia, N.M. Allergic reactivity of children of different socioeconomic levels in tropical populations. Int. Arch. Allergy Immunol. 1993, 101, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Yazdanbakhsh, M.; van den Biggelaar, A.; Maizels, R.M. Th2 responses without atopy: Immunoregulation in chronic helminth infections and reduced allergic disease. Trends Immunol. 2001, 22, 372–377. [Google Scholar] [CrossRef]
- Cooper, P.J. Can intestinal helminth infections (geohelminths) affect the development and expression of asthma and allergic disease? Clin. Exp. Immunol. 2002, 128, 398–404. [Google Scholar] [CrossRef] [PubMed]
- Andrade, Z.A.; Warren, K.S. Mild prolonged schistosomiasis in mice: Alterations in host response with time and the development of portal fibrosis. Trans. R. Soc. Trop. Med. Hyg. 1964, 58, 53–57. [Google Scholar] [CrossRef]
- Boros, D.L.; Pelley, R.P.; Warren, K.S. Spontaneous modulation of granulomatous hypersensitivity in Schistosomiasis mansoni. J. Immunol. 1975, 114, 1437–1441. [Google Scholar] [PubMed]
- Colley, D.G. Immune responses to a soluble schistosomal egg antigen preparation during chronic primary infection with Schistosoma mansoni. J. Immunol. 1975, 115, 150–156. [Google Scholar] [PubMed]
- Singh, K.P.; Gerard, H.C.; Hudson, A.P.; Reddy, T.R.; Boros, D.L. Retroviral Foxp3 gene transfer ameliorates liver granuloma pathology in Schistosoma mansoni infected mice. Immunology 2005, 114, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Hermelijn, H.S.; Everts, B.; Hartgers, F.C.; Yazdanbakhsh, M. Chronic Helminth Infections Protect Against Allergic Diseases by Active Regulatory Processes. Curr. Allergy Asthma Rep. 2010, 10, 3–12. [Google Scholar]
- Kitagaki, K.; Businga, T.R.; Racila, D.; Elliott, D.E.; Weinstock, J.V.; Kline, J.N. Intestinal Helminths Protect in a Murine Model of Asthma. J. Immunol. 2006, 177, 1628–1635. [Google Scholar] [CrossRef] [PubMed]
- Yazdanbakhsh, M.; Matricardi, P.M. Parasites and the Hygiene Hypothesis. Clin. Rev. Allergy Immunol. 2004, 26, 15–24. [Google Scholar] [CrossRef]
- Beasley, R.; Crane, J.; Lai, C.K.; Pearce, N. Prevalence and etiology of asthma. J. Allergy Clin. Immunol. 2000, 105, S466–S472. [Google Scholar] [CrossRef]
- Holt, P.G. Primary Allergic Sensitization to Environmental Antigens: Perinatal T Cell Priming as a Determinant of Responder Phenotype in Adulthood. Pediatr. Allergy Immunol. 1996, 183, 1297–1301. [Google Scholar] [CrossRef]
- Romagnani, S. The Th1/Th2 paradigm. Curr. Opin. Immunol. 1997, 18, 263–266. [Google Scholar] [CrossRef]
- Yazdanbakhs, M.; Kremsner, P.G.; van Ree, R. Allergy, parasites, and the hygiene hypothesis. Science 2002, 296, 490–494. [Google Scholar] [CrossRef] [PubMed]
- Araujo, M.I.; Lopes, A.A.; Medeiros, M.; Cruz, A.A.; Sousa-Atta, L.; Sole, D.; Carvalho, E.M. Inverse association between skin response to aeroallergens and Schistosoma mansoni infection. Int. Arch. Allergy Immunol. 2000, 123, 145–148. [Google Scholar] [CrossRef] [PubMed]
- Van den Biggelaar, A.H.; van Ree, R.; Rodrigues, L.C.; Lell, B.; Deelder, A.M.; Kremsner, P.G.; Yazdanbakhsh, M. Decreased atopy in children infected with Schistosoma haematobium: A role for parasite-induced interleukin-10. Lancet 2000, 356, 1723–1727. [Google Scholar] [CrossRef]
- Nyan, O.A.; Walraven, G.E.; Banya, W.A.; Milligan, P.; Van Der Sande, M.; Ceesay, S.M.; Del Prete, G.; McAdam, K.P. Atopy, intestinal helminth infection and total serum IgE in rural and urban adult Gambian communities. Clin. Exp. Allergy 2001, 31, 1672–1678. [Google Scholar] [CrossRef] [PubMed]
- Masters, S.; Barrett-Connor, E. Parasites and asthma: Predictive or protective? Epidemiol. Rev. 1985, 7, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Elliott, D.E.; Urban, J.J.; Argo, C.K.; Weinstock, J.V. Does the failure to acquire helminthic parasites predispose to Crohn’s disease? FASEB J. 2000, 14, 1848–1855. [Google Scholar] [CrossRef] [PubMed]
- Edwards, L.J.; Constantinescu, C.S. A prospective study of conditions associated with multiple sclerosis in a cohort of 658 consecutive outpatients attending a multiple sclerosis clinic. Mult. Scler. 2004, 10, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Stene, L.C.; Nafstad, P. Relation between occurrence of type 1 diabetes and asthma. Lancet 2001, 357, 607–608. [Google Scholar] [CrossRef]
- Bach, J.F. The effect of infections on susceptibility to autoimmune and allergic diseases. N. Engl. J. Med. 2002, 347, 911–920. [Google Scholar] [CrossRef] [PubMed]
- Wills-Karp, M.; Santeliz, J.; Karp, C.L. The germless allergic disease: Revisiting the hygiene hypothesis. Nat. Rev. Immunol. 2001, 1, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Scrivener, S.; Yemaneberhan, H.; Zebeniqus, M.; Tilahun, D.; Girma, S.; Ali, S.; McElroy, P.; Custovic, A.; Woodcock, A.; Pritchard, D.; et al. Independent effects of intestinal parasite infection and domestic allergen exposure on risk of wheeze in Ethiopia: A nested case-control study. Lancet 2001, 358, 1493–1499. [Google Scholar] [CrossRef]
- Lozupone, C.A.; Stombaugh, J.I.; Gordon, J.I.; Jansson, J.K.; Knight, R. Diversity, stability and resilience of the human gut microbiota. Nature 2012, 489, 220–230. [Google Scholar] [CrossRef] [PubMed]
- Koenig, J.E.; Spor, A.; Scalfone, N.; Fricker, A.D.; Stombaugh, J.; Knight, R.; Angenent, L.T.; Ley, R.E. Succession of microbial consortia in the developing infant gut microbiome. Proc. Natl. Acad. Sci. USA 2011, 108, 4578–4585. [Google Scholar] [CrossRef] [PubMed]
- Yatsunenko, T.; Rey, F.E.; Manary, M.J.; Trehan, I.; Dominguez-Bello, M.G.; Contreras, M.; Magris, M.; Hidalgo, G.; Baldassano, R.N.; Anokhin, A.P.; et al. Human gut microbiome viewed across age and geography. Nature 2012, 486, 222–227. [Google Scholar] [CrossRef] [PubMed]
- McLoughlin, R.M.; Mills, K.H. Influence of gastrointestinal commensal bacteria on the immune responses that mediate allergy and asthma. J Allergy Clin. Immunol. 2011, 127, 1097–1107. [Google Scholar] [CrossRef] [PubMed]
- O’Mahony, C.; Scully, P.; O’Mahony, D.; Murphy, S.; O’Brien, F.; Lyons, A.; Sherlock, G.; John MacSharry, J.; Kiely, B.; Shanahan, F.; et al. Commensal-induced regulatory T cells mediate protection against pathogen-stimulated NF-kappaB activation. PLoS Pathog. 2008, 4, e1000112. [Google Scholar] [CrossRef]
- De Roock, S.; van Elk, M.; van Dijk, M.E.; Timmerman, H.M.; Rijkers, G.T.; Prakken, B.J.; Hoekstra, M.O.; de Kleer, I.M. Lactic acid bacteria differ in their ability to induce functional regulatory T cells in humans. Clin. Exp. Allergy J. Br. Soc. Allergy Clin. Immunol. 2010, 40, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Atarashi, K.; Tanoue, T.; Shima, T.; Imaoka, A.; Kuwahara, T.; Momose, Y.; Cheng, G.; Yamasaki, S.; Saito, T.; Ohba, Y.; et al. Induction of colonic regulatory T cells by indigenous Clostridium species. Science 2011, 331, 337–341. [Google Scholar] [CrossRef] [PubMed]
- Furusawa, Y.; Obata, Y.; Fukuda, S.; Endo, T.A.; Nakato, G.; Takahashi, D.; Nakanishi, Y.; Uetake, C.; Kato, K.; Kato, T.; et al. Commensal microbe-derived butyrate induces the differentiation of colonic regulatory T cells. Nature 2013, 504, 446–450. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.M.; Howitt, M.R.; Panikov, N.; Michaud, M.; Gallini, C.A.; Bohlooly-Y, M.; Glickman, J.N.; Garrett, W.S. The microbial metabolites, short-chain fatty acids, regulate colonic Treg cell homeostasis. Science 2013, 341, 569–573. [Google Scholar] [CrossRef] [PubMed]
- Maslowski, K.M.; Vieira, A.T.; Ng, A.; Kranich, J.; Sierro, F.; Yu, D.; Schilter, H.C.; Rolph, M.S.; Mackay, F.; Artis, D.; et al. Regulation of inflammatory responses by gut microbiota and chemoattractant receptor GPR43. Nature 2009, 461, 1282–1286. [Google Scholar] [CrossRef] [PubMed]
- Kalliomaki, M.; Kirjavainen, P.; Eerola, E.; Kero, P.; Salminen, S.; Isolauri, E. Distinct patterns of neonatal gut microflora in infants in whom atopy was and was not developing. J. Allergy Clin. Immunol. 2001, 107, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Penders, J.; Thijs, C.; Vink, C.; Stelma, F.F.; Snijders, B.; Kummeling, I.; van den Brandt, P.A.; Stobberingh, E.E. Factors influencing the composition of the intestinal microbiota in early infancy. Pediatrics 2006, 118, 511–521. [Google Scholar] [CrossRef] [PubMed]
- Terhune, T.D.; Deth, R.C. A role for impaired regulatory T cell function in adverse responses to aluminum adjuvant-containing vaccines in genetically susceptible individuals. Vaccine 2014, 32, 5149–5155. [Google Scholar] [CrossRef] [PubMed]
- Offit, P.A.; Hackett, C.J. Addressing parents’ concerns: Do vaccines cause allergic or autoimmune diseases? Pediatrics 2003, 111, 653–659. [Google Scholar] [CrossRef] [PubMed]
- Somerset, D.A.; Zheng, Y.; Kilby, M.D.; Sansom, D.M.; Drayson, M.T. Noramal human pregnancy is associated with an elevation in the immune suppressive CD25+ CD4+ regulatory T-cell subset. Immunology 2004, 112, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Zozulya, A.L.; Wiendl, H. The role of regulatory T cells in multiple sclerosis. Nat. Clin. Pract. Neurol. 2008, 4, 384–398. [Google Scholar] [CrossRef] [PubMed]
- Francis, J.N.; Till, S.J.; Durham, S.R. Induction of IL-10+CD4+CD25+ T cells by grass pollen immunotherapy. J. Allergy Clin. Immunol. 2003, 111, 125–161. [Google Scholar] [CrossRef]
- Tsai, Y.-G.; Chiou, Y.L.; Chien, J.W.; Wu, H.P.; Lin, C.Y. Induction of IL-10+CD4+CD25+ regulatory T cells with decreased NF-kB expression during immunotherapy. Pediatr. Allergy Immunol. 2010, 21, e166–e173. [Google Scholar] [CrossRef] [PubMed]
- Groß, F.; Metzner, G.; Behn, U. Mathematical modeling of allergy and specific immunotherapy: Th1 Th2–Treg interactions. J. Theor. Biol. 2010, 269, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Jutel, M.; Akdis, C.A. Immunological mechanisms of allergen-specific immunotherapy. Allergy 2011, 66, 725–732. [Google Scholar] [CrossRef] [PubMed]
- Barrios, C.; Brawand, P.; Berney, M.; Brandt, C.; Lambert, P.H.; Siegrist, C.A. Neonatal and early life immune responses to various forms of vaccine antigens qualitatively differ from adult responses: Predominance of a TH2-biased pattern which persists after adult boosting. Eur. J. Immunol. 1996, 26, 1489–1496. [Google Scholar] [CrossRef] [PubMed]
- Prescott, S.L.; Macaubas, C.; Holt, B.J.; Smallacombe, T.B.; Loh, R.; Sly, P.D.; Holt, P.G. Transplacental priming of the human immune system to environmental allergens: Universal skewing of initial T cell responses toward the TH2 cytokine profile. J. Immunol. 1998, 160, 4730–4737. [Google Scholar] [PubMed]
- Prescott, S.L.; Macaubas, C.; Smallacombe, T.; Holt, B.J.; Sly, P.D.; Loh, R.; Holt, P.G. Reciprocal age-related patterns of allergen-specific T-cell immunity in normal vs. atopic infants. Clin. Exp. Allergy 1998, 28, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Chougnet, C.; Kovacs, A.; Baker, R.; Mueller, B.U.; Luban, N.L.; Liewehr, D.J.; Steinberg, S.M.; Thomas, E.K.; Shearer, G.M. Influence of human immunodeficiency virus-infected maternal environment on development of infant interleukin-12 production. J. Infect. Dis. 2000, 181, 1590–1597. [Google Scholar] [CrossRef] [PubMed]
- Prince, B.T.; Erickson, K.A.; Szychlinski, C.; Schleimer, P.; Bryce, P.; Singh, A.M. The Differential Relationship between Regulatory T-Cells and Age in Children with Food Allergy. J. Allergy Clin. Immunol. 2015, 135, AB10. [Google Scholar] [CrossRef]
- Taams, L.S.; Vukmanovic-Stejic, M.; Smith, J.; Dunne, P.J.; Fletcher, J.M.; Plunkett, F.J.; Ebeling, S.B.; Lombardi, G.; Rustin, M.H.; Bijlsma, J.W.; et al. Antigen specific T cell suppression by human CD4+CD25+ regulatory T cells. Eur. J. Immunol. 2002, 32, 1621–1630. [Google Scholar] [CrossRef]
- Ling, E.M.; Smith, T.; Nguyen, X.D.; Pridgeon, C.; Dallman, M.; Arbery, J.; Carr, V.A.; Robinson, D.S. Relation of CD4+CD25+ regulatory T-cell suppression of allergen-driven T-cell activation to atopic status and expression of allergic disease. Lancet 2004, 363, 608–615. [Google Scholar] [CrossRef]
- Bellinghausen, I.; Klostermann, B.; Knop, J.; Saloga, J. Human CD4+CD25+ T cells derived from the majority of atopic donors are able to suppress TH1 and TH2 cytokine production. J. Allergy Clin. Immunol. 2003, 111, 862–868. [Google Scholar] [CrossRef] [PubMed]
- Hawrylowicz, C.M. Regulatory T cells and IL-10 in allergic inflammation. J. Exp. Med. 2005, 202, 1459–1463. [Google Scholar] [CrossRef] [PubMed]
- Akdis, M.; Verhagen, J.; Taylor, A.; Karamloo, F.; Karagiannidis, C.; Crameri, R.; Thunberg, S.; Deniz, G.; Valenta, R.; Fiebig, H.; et al. Immune responses in healthy and allergic individuals are characterized by a fine balance between allergen-specific T regulatory 1 and T helper 2 cells. J. Exp. Med. 2004, 199, 1567–1575. [Google Scholar] [CrossRef] [PubMed]
- Borish, L.; Aarons, A.; Rumbyrt, J.; Cvietusa, P.; Negri, J.; Wenzel, S. Interleukin-10 regulation in normal subjects and patients with asthma. J. Allergy Clin. Immunol. 1996, 97, 1288–1296. [Google Scholar] [CrossRef]
- Lim, S.; Crawley, E.; Woo, P.; Barnesn, P.J. Haplotype associated with low interleukin-10 production in patients with severe asthma. Lancet 1998, 352, 113. [Google Scholar] [CrossRef]
- Heaton, T.; Rowe, J.; Turner, S.; Aalberse, R.C.; de Klerk, N.; Suriyaarachchi, D.; Serralha, M.; Holt, B.J.; Hollams, E.; Yerkovich, S.; et al. An immunoepidemiological approach to asthma: Identification of in-vitro T-cell response patterns associated with different wheezing phenotypes in children. Lancet 2005, 365, 142–149. [Google Scholar] [CrossRef]
- Morelli, A.E.; Thomson, A.W. Dendritic cells: Regulators of alloimmunity and opportunities for tolerance induction. Immunol. Rev. 2003, 196, 125–146. [Google Scholar] [CrossRef] [PubMed]
- Wakkach, A.; Fournier, N.; Brun, V.; Breittmayer, J.P.; Cottrez, F.; Groux, H. Characterization of dendritic cells that induce tolerance and T regulatory 1 cell differentiation in vivo. Immunity 2003, 18, 605–617. [Google Scholar] [CrossRef]
- Bellinghausen, I.; Sudowe, S.; König, B.; Reske-Kunz, A.B.; Knop, J.; Saloga, J. Interleukin-10-Treated Dendritic Cells Do Not Inhibit Th2 Immune Responses in Ovalbumin/Alum-Sensitized Mice. Int. Arch. Allergy Immunol. 2005, 141, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Terhune, T.D.; Deth, R.C. How aluminum adjuvants could promote and enhance non-target IgE synthesis in a genetically-vulnerable sub-population. J. Immunotoxicol. 2012, 10, 210–222. [Google Scholar] [CrossRef] [PubMed]
- Kool, M.; Hammad, H.; Lambrecht, B.N. Cellular networks controlling Th2 polarization in allergy and immunity. F1000 Biol. Rep. 2012, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ulanova, M.; Tarkowski, A.; Hahn-Zoric, M.; Hanson, L.A. The Common Vaccine Adjuvant Aluminum Hydroxide Up-Regulates Accessory Properties of Human Monocytes via an Interleukin-4-Dependent Mechanism. Infect. Immun. 2001, 69, 1151–1159. [Google Scholar] [CrossRef] [PubMed]
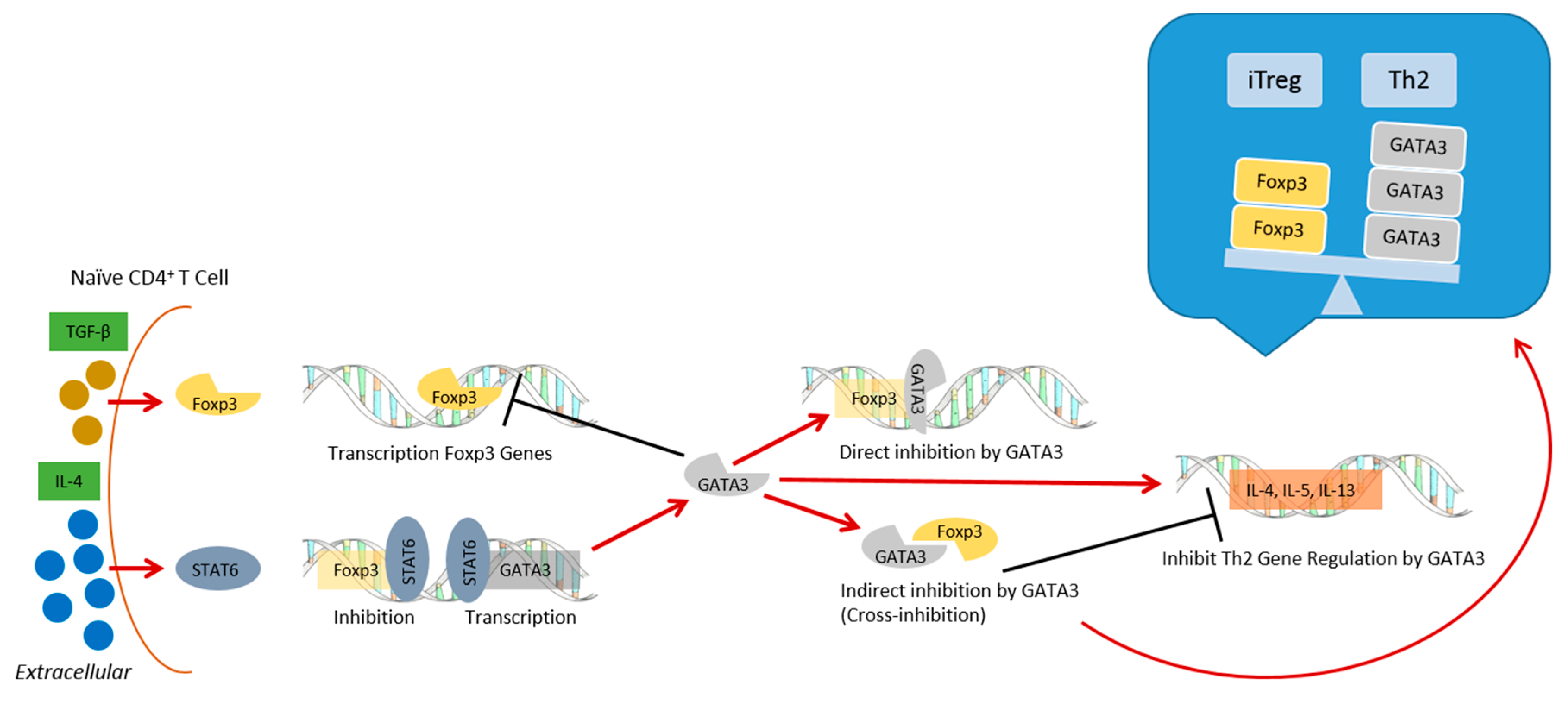
- Wei, J.; Duramad, O.; Perng, O.; Reiner, S.; Liu, Y.-J.; Qin, F.X.-F. Antagonistic nature of T helper 1/2 development programs in opposing peripheral induction of Foxp3+ regulatory T cells. Proc. Natl. Acad. Sci. USA 2007, 104, 18169–18174. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.H.; Cohn, L.; Ray, P.; Bottomly, K.; Ray, A. Transcription factor GATA-3 is differentially expressed in murine Th1 and Th2 cells and controls Th2-specificexpression of the interleukin-5 gene. J. Biol. Chem. 1997, 272, 21597–21603. [Google Scholar] [CrossRef] [PubMed]
- Zheng, W.; Flavell, R.A. The transcription factor GATA-3 is necessary and sufficient for Th2 cytokine gene expression in CD4 T cells. Cell 1997, 89, 587–596. [Google Scholar] [CrossRef]
- Takaki, H.; Ichiyama, K.; Koga, K.; Chinen, T.; Takaesu, G.; Sugiyama, Y.; Kato, S.; Yoshimura, A.; Kobayashi, T. STAT6 inhibits TGF-beta1 mediated Foxp3 induction through direct binding to the Foxp3 promoter, which is reverted by retinoic acid receptor. J. Biol. Chem. 2008, 283, 14955–14962. [Google Scholar] [CrossRef] [PubMed]
- Mantel, P.Y.; Kuipers, H.; Boyman, O.; Rhyner, C.; Ouaked, N.; Rückert, B.; Karagiannidis, C.; Lambrecht, B.N.; Hendriks, R.W.; Crameri, R.; et al. GATA3-driven Th2 responses inhibit TGF-beta1-induced FOXP3 expression and the formation of regulatory T cells. PLoS Biol. 2007, 5, e329. [Google Scholar] [CrossRef] [PubMed]
- HogenEsch, H. Mechanism of immunopotentiation and safety of aluminum adjunvants. Front. Immunol. 2012, 3, 406. [Google Scholar] [PubMed]
- He, P.; Zou, Y.; Hu, Z. Advances in aluminum hydroxide-based adjuvant research and its mechanism. Hum. Vaccines Immunother. 2015, 11, 477–488. [Google Scholar] [CrossRef] [PubMed]
- Rowe, J.; Macaubas, C.; Monger, T.; Holt, B.; Harvey, J.; Poolman, J.T.; Loh, R.; Sly, P.D.; Holt, P.G. Heterogeneity in diphtheria-tetanus-acellular pertussis vaccine-specific cellular immunity during infancy: Relationship to variations in the kinetics of postnatal maturation of systemic Th1 function. J. Infect. Dis. 2001, 184, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Hoyt, A.; Heymann, P.; Schuyler, A.; Commins, S.; Platts-Mills, T. Changes in IgE Levels Following One-Year Immunizations in Two Children with Food Allergy. In Proceedings of the WAO Symposium on Food Allergy & the Microbiome, Miami, FL, USA, 5–6 December 2015. [Google Scholar]
- Sakaquchi, M.; Inouye, S. IgE sensitization to gelatin: The probable role of gelatin-containing diphtheria-tetanus-acellular pertussis (DTaP) vaccines. Vaccine 2000, 18, 2055–2058. [Google Scholar] [CrossRef]
- Lambercht, B.N.; Kool, M.; Willart, M.A.; Hammad, H. Mechanism of action of clinically approved adjuvants. Curr. Opin. Immunol. 2009, 21, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Haley, P.J. Species differences in the structure and function of the immune system. Toxicology 2003, 188, 49–71. [Google Scholar] [CrossRef]
- Lu, F.; HogenEsch, H. Kinetics of the inflammatory response following intramuscular injection of aluminum adjuvant. Vaccine 2013, 31, 3979–3986. [Google Scholar] [CrossRef] [PubMed]
- Snapper, C.M.; Finkelman, F.D. Immunoglobulin class switching. In Fundamental Immunology; Paul, W.E., Ed.; Lippincott-Raven: Philadelphia, PA, USA, 2003; p. 831. [Google Scholar]
- Del Prete, G.; De Carli, M.; Almerigogna, F.; Giudizi, M.G.; Biagiotti, R.; Romagnani, S. Human IL-10 is produced by both type 1 helper (Th1) and type 2 helper (Th2) T cell clones and inhibits their antigen-specific proliferation and cytokine production. J. Immunol. 1993, 150, 353–360. [Google Scholar] [PubMed]



© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Terhune, T.D.; Deth, R.C. Aluminum Adjuvant-Containing Vaccines in the Context of the Hygiene Hypothesis: A Risk Factor for Eosinophilia and Allergy in a Genetically Susceptible Subpopulation? Int. J. Environ. Res. Public Health 2018, 15, 901. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15050901
Terhune TD, Deth RC. Aluminum Adjuvant-Containing Vaccines in the Context of the Hygiene Hypothesis: A Risk Factor for Eosinophilia and Allergy in a Genetically Susceptible Subpopulation? International Journal of Environmental Research and Public Health. 2018; 15(5):901. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15050901
Chicago/Turabian StyleTerhune, Todd D., and Richard C. Deth. 2018. "Aluminum Adjuvant-Containing Vaccines in the Context of the Hygiene Hypothesis: A Risk Factor for Eosinophilia and Allergy in a Genetically Susceptible Subpopulation?" International Journal of Environmental Research and Public Health 15, no. 5: 901. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15050901