Mood Regulation Focused CBT Based on Memory Reconsolidation, Reduced Suicidal Ideation and Depression in Youth in a Randomised Controlled Study


Abstract
:1. Introduction
2. Material and Methods
2.1. Setting
2.2. MR-CBT
2.3. Control Treatment
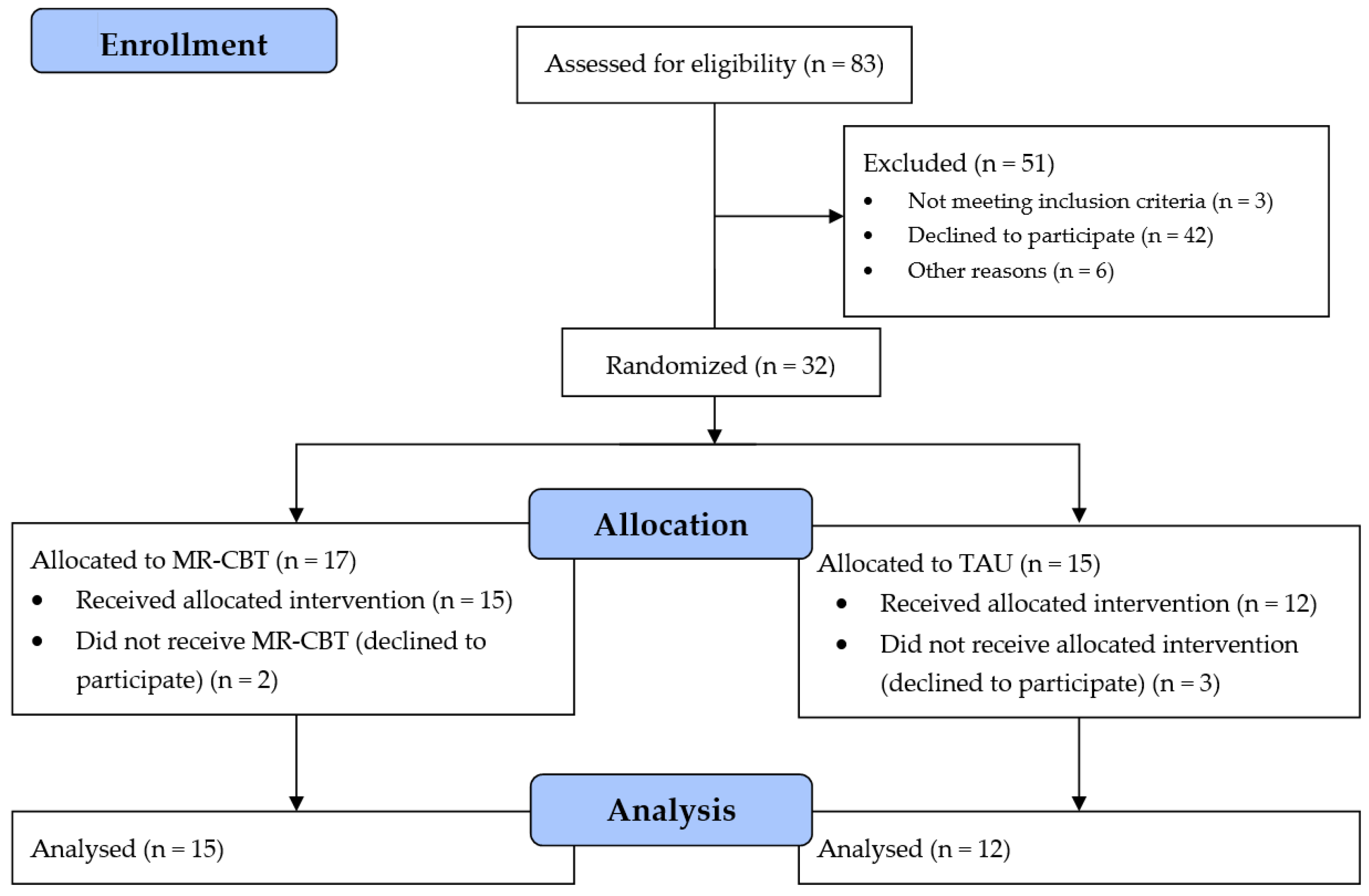
2.4. Randomisation
2.5. Medication
2.6. Primary Outcome Measures
2.7. Secondary Outcome Measure
2.8. Statistics
3. Results
4. Discussion
4.1. Suicidality
4.2. Depression
4.3. Wellbeing
4.4. Limitations
4.5. Mechanism of Change
4.6. Advantages
5. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- World Health Statistics 2017, Suicide Data. Available online: http://www.who.int/mental_health/prevention/suicide/suicideprevent/en/ (accessed on 7 March 2018).
- Castellvi, P.; Lucas-Romero, E.; Miranda-Mendizábal, A.; Parés-Badell, O.; Almenara, J.; Alonso, I.; Blasco, M.J.; Cebrià, A.; Gabilondo, A.; Gili, M.; et al. Longitudinal association between self-injurious thoughts and behaviors and suicidal behavior in adolescents and young adults: A systematic review with meta-analysis. J. Affect. Disord. 2017, 215, 37–38. [Google Scholar] [CrossRef] [PubMed]
- Gold-Mellor, S.J.; Avshalom, C.; Harrington, H.; Hogan, S.; Nada-Raja, S.; Poulton, R.; Moffitt, T.E. Suicide attempt in young people: A signal for long-term health care and social needs. JAMA Psychiatry 2014, 7, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Ganz, D.; Braquehais, M.D.; Sher, L. Secondary prevention of suicide. PLoS Med. 2010, 7, e1000271. [Google Scholar] [CrossRef] [PubMed]
- Weisz, J.R.; Kuppens, S.; Ng, M.Y.; Eckshtain, D.; Ugueto, A.M.; Vaughn-Coaxum, R.; Jensen-Doss, A.; Hawley, K.M.; Krumholz Marchette, L.S.; Chu, B.C.; et al. What five decades of research tells us about the effects of youth psychological therapy: A multilevele meta-analysis and implications for science and practice. Am. Psychol. 2017, 72, 79–117. [Google Scholar] [CrossRef] [PubMed]
- Weisz, J.R. Building robust psychotherapies for children and adolescents. Perspect. Psychol. Sci. 2014, 9, 81–84. [Google Scholar] [CrossRef] [PubMed]
- Ougrin, D.; Tranah, T.; Stahl, D.; Moran, P.; Asarnow, J.R. Therapeutic interventions for suicide attempts and self-harm in adolescents: systematic review and meta-analysis. J. Am. Acad. Child Adolesc. Psychiatry 2015, 54, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Asarnow, J.R.; Hughes, J.L.; Babeva, K.N.; Sugar, C.A. Cognitive-behavioural family treatment for suicide attempt prevention: A randomized controlled trial. J. Am. Acad. Child. Adolesc. Psychiatry 2017, 56, 506–514. [Google Scholar] [CrossRef]
- Tanskanen, A.; Hintikka, J.; Honkalampi, K.; Haatainen, K.; Koivumaa-Honkanen, H.; Viinamäki, H. Impact of multiple traumatic experiences on the persistence of depressive symptoms—A population-based study. Nord. J. Psychiatry 2004, 58, 459–464. [Google Scholar] [CrossRef] [PubMed]
- Kumpulainen, K.; Räsänen, E.; Henttonen, I.; Almqvist, F.; Kresanov, K.; Linna, S.; Moilanen, I.; Piha, J.; Puura, K.; Tamminen, T. Bullying and pscyhiatric symptoms among elementary school-age children. Child Abuse Negl. 1998, 22, 705–717. [Google Scholar] [CrossRef]
- Darvez-Bornoz, J.M. Rape-related psychotraumatic syndromes. Eur. J. Obstet. Gynecol. reprod. Biol. 1997, 71, 59–65. [Google Scholar] [CrossRef]
- Díaz-Atienza, F.; Prados-Cuesta, M.; Ruz-Veguilla, M. Relación entre las conductas de intimidación, depresión e ideación suicida en adolescentes: Resultados preliminares. Rev. Psiquaitr. Psicol. Ninõ Adolsc. 2004, 4, 10–19. [Google Scholar]
- Reijntjes, A.; Kamphuis, J.H.; Prinzie, P.; Telch, M.J. Peer victimization and internalizing problems in children: A meta-analysis of longitudinal studies. Child Abuse Negl. 2010, 34, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Panagioti, M.; Gooding, P.A.; Triantafyllou, K.; Tarrier, N. Suicidality and posttraumatic stress disorder (PTSD) in adolescents: A systematic review and meta-analysis. Soc. Psychiatry Psychiatr. Epidemiol. 2015, 50, 523–537. [Google Scholar] [CrossRef] [PubMed]
- Dunn, V.; Goodyer, I.M. Longitudinal investigation into childhood-and adolesence-onset depression: Psychiatric outcome in early adulthood. Br. J. Psychiatry 2006, 188, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, L. Cognitive and affective development in adolescence. Trends Cogn. Sci. 2005, 9, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Sheeber, L.B.; Allen, N.B.; Leve, C.; Davis, B.; Shortt, J.W.; Katz, L.F. Dynamics of affective experience and behavior in depressed adolescents. J. Child Psychol. Psychiatry 2009, 50, 1419–1427. [Google Scholar] [CrossRef] [PubMed]
- Yap, B.H.; Allen, N.B.; Sheeber, L. Using an emotion regulation framework to understand the role of temperament and family processes in risk for adolescent depressive disorders. Clin. Child Fam. Psychol. Rev. 2007, 10, 180–196. [Google Scholar] [CrossRef] [PubMed]
- Larsen, R.J. Toward a science of mood regulation. Psychol. Inq. 2000, 11, 129–141. [Google Scholar] [CrossRef]
- Rojas, S.M.; Leen-Feldner, E.W.; Blumenthal, H.; Lewis, S.F.; Feldner, M.T. Risk for suicide among treatment seeking adolescents: the role of positive and negative affects intensity. Cogn. Ther. Res. 2015, 39, 100–109. [Google Scholar] [CrossRef]
- Köhler, C.A.; Carvalho, A.F.; Alves, G.S.; McIntyre, R.S.; Hyphantis, T.N.; Cammarota, M. Autobiographical memory disturbances in depression: A novel therapeutic target? Neural Plast. 2015, 2015, 759139. [Google Scholar] [CrossRef] [PubMed]
- Klonsky, E.D.; Kotov, R.; Bakst, S.; Rabinowitz, J.; Bromet, E.J. Hopelessness as a predictor of attempted suicide among first admission patients with psychosis: A 10-year cohort study. Suicide Life Threat. Behav. 2012, 42, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Nadel, L.; Hupbach, A.; Gomez, R.; Newman-Smith, K. Memory formation, consolidation and transformation. Neurosci. Biobehav. Rev. 2012, 36, 1640–1645. [Google Scholar] [CrossRef] [PubMed]
- Lane, R.D.; Ryan, L.; Nadel, L.; Greenberg, L. Memory reconsolidation, emotional arousal, and the process of change in psychotherapy: New insights from brain science. Behav. Brain. Sci. 2015, 38. [Google Scholar] [CrossRef] [PubMed]
- Ecker, B. Memory reconsolidation understood and misunderstood. Int. J. Neuropsychother. 2015, 3, 2–46. [Google Scholar] [CrossRef]
- Björkstrand, J.; Ågren, T.; Åhs, F.; Frick, A.; Larson, E.; Hjorth, O.; Fredriksson, M. Disrupting reconsolidation attenuates long-term fear memory in the human amygdala and facilitates approach behavior. Curr. Biol. 2016, 26, 2690–2695. [Google Scholar] [CrossRef] [PubMed]
- Steinfurth, E.C.; Kanen, J.K.; Raio, C.M.; Clem, R.L.; Huganir, R.L.; Phelps, E.A. Young and old Pavlovian fear memories can be modified with extinction training during reconsolidation in humans. Learn. Mem. 2014, 21, 338–341. [Google Scholar] [CrossRef] [PubMed]
- Högberg, G.; Nardo, D.; Hällström, T.; Pagani, M. Affective psychotherapy in post-traumatic reactions guided by affective neuroscience memory reconsolidation and play. Psychol. Res. Behav. Manag. 2011, 4, 87–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becker, T.; Kindt, M. Memory reconsolidation interference as an emerging treatment for emotional disorders: Strengths, limitations, challenges and opportunities. Annu. Rev. Clin. Psychol. 2017, 13, 99–121. [Google Scholar] [CrossRef] [PubMed]
- Wolpe, J. Psychotherapy by Reciprocal Inhibition; Stanford University Press: Stanford, CA, USA, 1958. [Google Scholar]
- Angold, A.; Costello, E.J.; Messer, S.C.; Loeber, R.; VanKammen, W.; Loeber, A.S. Development of a short questionnaire for use in epidemiological studies of depression in children and adolescents. Int. J. Methods Psychiatr. Res. 1995, 5, 237–249. [Google Scholar]
- Högberg, G.; Hällström, T. Active multimodal psychotherapy in children and adolescents with suicidality: Description, evaluation and clinical profile. Clin. Child Psychol. Psychiatry 2008, 13, 435–448. [Google Scholar] [CrossRef] [PubMed]
- Posner, K.; Brown, G.K.; Stanley, B.; Brent, D.A.; Yershova, K.V.; Oquendo, M.A.; Currier, G.W.; Melvin, G.A.; Greenhill, L.; Shen, S.; et al. The Columbia-suicide Severity Rating Scale: Initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am. J. Psychiatry 2011, 168, 1266–1277. [Google Scholar] [CrossRef] [PubMed]
- Messer, S.C.; Angold, A.; Costello, E.J.; Loeber, R.; van Kammen, W.; Stouthamer-Loeber. Development of a short questionnaire for use in epidemiological studies of depression in children and adolescents: Factor composition and structure across development. Int. J. Methods Psychiatr. Res. 1995, 5, 251–262. [Google Scholar]
- Riso, L.P.; Thase, M.E.; Howland, R.H.; Friedman, E.S.; Simons, A.D.; Tu, X.M. A prospective test of criteria for response remission relapse recovery and recurrence in patients treated with cognitive behavior therapy. J. Affect. Disord. 1997, 43, 131–142. [Google Scholar] [CrossRef]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 Wellbeing Index: A systematic review of the Literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Allgaier, A.; Pietsch, K.; Frühe, B.; Prast, E.; Sigl-Glöckner, J.; Schulte-Körne, G. Depression in pediatric care: Is the WHO-five Wellbeing Index a valid screening instrument for children and adolescents? Gen. Hosp. Psychiatry 2012, 34, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Keilp, J.G.; Gorlyn, M.; Oquendo, M.A.; Brodsky, B.; Ellis, SP.; Stanley, B.; Mann, J. Aggressiveness, not impulsiveness of hostility, distinguishes suicide attempters with major depression. Psychol. Med. 2006, 36, 1779–1788. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, A.H.; Hames, J.L.; Ribeiro, J.D.; Silva, C.; Joiner, T.E.; Cougle, J.R. An examination of the relationship between anger and suicide risk through the lens of the interpersonal theory of suicide. J. Psychiatr. Res. 2014, 50, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Roberts, R.E.; Liu, Z.; Xian, M.; Tang, J.; Sun, J.; Yu, Y. Hostility, physical aggression and trait anger as predictors for suicidal behavior in Chinese Adolescents: A schoolbased study. PLoS ONE 2012, 7, e31044. [Google Scholar] [CrossRef] [PubMed]
- Wolff, J.C.; Davis, S.; Liu, R.T.; Cha, C.B.; Cheek, S.M.; Nestor, B.A.; Frazier, E.A.; Schaffer, M.M.; Spirito, A. Trajectories of suicidal ideation among adolescents following psychiatric hospitalization. J. Abnorm. Child Psychol. 2018, 46, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Orbach, I.; Mikulincer, M.; Blumenson, R.; Mester, R.; Stein, D. The subjective experience of problem irresolvability and suicidal behavior: dynamics and measurement. Suicide Life Threat. Behav. 1999, 29, 150–164. [Google Scholar] [PubMed]
- Krogsbøll, L.T.; Hrobjartsson, A.; Gøtzsche, P.C. Spontaneous improvement in randomized clinical trials: Meta-analysis of three-armed trials comparing no treatment, placebo and active intervention. BMC Med. Res. Methodol. 2009, 9, 1–10. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Mental Health. Development and Definitions of the RDoC Domains and Constructs. Available online: http://www.nimh.nih.gov/research-priorities/rdoc/development-and-definitions-of-the-rdoc-domains-and-constructs (accessed on 7 March 2018).
- Insel, T.; Cuthbert, B.; Garvey, M.; Heinssen, R.; Pine, D.S.; Quinn, K.; Sanislow, C.; Wang, P. Research domain criteria (RDoC): Toward a new classification framework for research on mental disorders. Am. J. Psychiatry 2010, 167, 748–751. [Google Scholar] [CrossRef] [PubMed]
- Fredrickson, B.L.; Losada, M.F. Positive affect and the complex dynamics of human flourishing. Am. Psychol. 2005, 60, 678–686. [Google Scholar] [CrossRef] [PubMed]
- Diener, E.; Diener, C. Subjective wellbeing: The science of happiness and a proposal for a national index. Am. Psychol. 2000, 55, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Hayes, S.C.; Hofman, S.G. The third wave of cognitive behavioral therapy and the rise of process-based care. World Psychiatry 2017, 16, 245–246. [Google Scholar] [CrossRef] [PubMed]
- Goldston, D.B.; Erkanli, A.; Daniel, S.S.; Heilbron, N.; Weller, B.E.; Doyle, O. Developmental trajectories of suicidal thoughts and behaviors from adolescence through adulthood. J. Am. Acad. Child Adolesc. Psychiatry 2016, 55, 400–407. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| MR-CBT | TAU | ||||||
|---|---|---|---|---|---|---|---|
| Effect variable | Baseline | End of treatment | p within sample * | Baseline | End of treatment | p within sample * | p comparing treatments # |
| SMFQ | 16.9 (11–23) (n = 15) | 6.7 (1–17) (n = 15) | <0.01 | 16.4 (8–26) (n = 12) | 8.8 (2–21) (n = 8) | <0.01 | 0.2 |
| WHO-5 | 28(4–68) (n = 14) | 63(24–92) (n = 14) | <0.01 | 32(4–60) (n = 7) | 69(48–76) (n = 5) | <0.05 | 0.6 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Högberg, G.; Hällström, T. Mood Regulation Focused CBT Based on Memory Reconsolidation, Reduced Suicidal Ideation and Depression in Youth in a Randomised Controlled Study. Int. J. Environ. Res. Public Health 2018, 15, 921. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15050921
Högberg G, Hällström T. Mood Regulation Focused CBT Based on Memory Reconsolidation, Reduced Suicidal Ideation and Depression in Youth in a Randomised Controlled Study. International Journal of Environmental Research and Public Health. 2018; 15(5):921. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15050921
Chicago/Turabian StyleHögberg, Göran, and Tore Hällström. 2018. "Mood Regulation Focused CBT Based on Memory Reconsolidation, Reduced Suicidal Ideation and Depression in Youth in a Randomised Controlled Study" International Journal of Environmental Research and Public Health 15, no. 5: 921. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15050921