In Hospital Stroke Mortality: Rates and Determinants in Southwestern Saudi Arabia

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Settings
2.2. Study Area
2.3. Data Collection
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Thrift, A.G.; Thayabaranathan, T.; Howard, G.; Howard, V.J.; Rothwell, P.M.; Feigin, V.L.; Norrving, B.; Donnan, G.A.; Cadilhac, D.A. Global stroke statistics. Int. J. Stroke 2017, 12, 13–32. [Google Scholar] [CrossRef] [PubMed]
- Koennecke, H.-C.; Belz, W.; Berfelde, D.; Endres, M.; Fitzek, S.; Hamilton, F.; Kreitsch, P.; Mackert, B.-M.; Nabavi, D.; Nolte, C. Factors influencing in-hospital mortality and morbidity in patients treated on a stroke unit. Neurology 2011, 77, 965–972. [Google Scholar] [CrossRef] [PubMed]
- Candelise, L.; Gattinoni, M.; Bersano, A.; Micieli, G.; Sterzi, R.; Morabito, A.; Group, T.P.S. Stroke-unit care for acute stroke patients: An observational follow-up study. Lancet 2007, 369, 299–305. [Google Scholar] [CrossRef]
- Rocha, M.S.G.; Almeida, A.C.F.; Abath Neto, O.; Porto, M.P.; Brucki, S.M.D. Impact of stroke unit in a public hospital on length of hospitalization and rate of early mortality of ischemic stroke patients. Arq. Neuro-Psiquiatr. 2013, 71, 774–779. [Google Scholar] [CrossRef] [PubMed]
- Borhani-Haghighi, A.; Safari, R.; Heydari, S.T.; Soleimani, F.; Sharifian, M.; Kashkuli, S.Y.; Khayatghuchani, M.N.; Azadi, M.; Shariat, A.; Safari, A. Hospital mortality associated with stroke in Southern Iran. Iran. J. Med. Sci. 2013, 38, 314–320. [Google Scholar] [PubMed]
- Matsui, H.; Fushimi, K.; Yasunaga, H. Variation in risk-standardized mortality of stroke among hospitals in Japan. PLoS ONE 2015, 10, e0139216. [Google Scholar] [CrossRef] [PubMed]
- Myint, P.K.; Bachmann, M.O.; Loke, Y.K.; Musgrave, S.D.; Price, G.M.; Hale, R.; Metcalf, A.K.; Turner, D.A.; Day, D.J.; Warburton, E.A. Important factors in predicting mortality outcome from stroke: Findings from the anglia stroke clinical network evaluation study. Age Ageing 2017, 46, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Nimptsch, U.; Mansky, T. Stroke unit care and trends of in-hospital mortality for stroke in Germany 2005–2010. Int. J. Stroke 2014, 9, 260–265. [Google Scholar] [CrossRef] [PubMed]
- Reeves, M.J.; Bushnell, C.D.; Howard, G.; Gargano, J.W.; Duncan, P.W.; Lynch, G.; Khatiwoda, A.; Lisabeth, L. Sex differences in stroke: Epidemiology, clinical presentation, medical care and outcomes. Lancet Neurol. 2008, 7, 915–926. [Google Scholar] [CrossRef]
- El-Hajj, M.; Salameh, P.; Rachidi, S.; Hosseini, H. The epidemiology of stroke in the Middle East. Eur. Stroke J. 2016, 1, 180–198. [Google Scholar] [CrossRef]
- Almekhlafi, M.A. Trends in one-year mortality for stroke in a tertiary academic center in Saudi Arabia: A 5-year retrospective analysis. Ann. Saudi Med. 2016, 36, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Barker-Collo, S.; Bennett, D.A.; Krishnamurthi, R.V.; Parmar, P.; Feigin, V.L.; Naghavi, M.; Forouzanfar, M.H.; Johnson, C.O.; Nguyen, G.; Mensah, G.A. Sex differences in stroke incidence, prevalence, mortality and disability-adjusted life years: Results from the global burden of disease study 2013. Neuroepidemiology 2015, 45, 203–214. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Abajobir, A.; Abate, K.; Abd-Allah, F.; Abdulle, A.; Abera, S.; Abyu, G.; Ahmed, M.; Ärnlöv, J.; Vos, T. Global, regional and national burden of neurological disorders during 1990–2015: A systematic analysis for the global burden of disease study 2015. Lancet Neurol. 2017, 16, 877–897. [Google Scholar] [CrossRef]
- Al Khathaami, A.M.; Algahtani, H.; Alwabel, A.; Alosherey, N.; Kojan, S.; Aljumah, M. The status of acute stroke care in Saudi Arabia: An urgent call for action! Int. J. Stroke 2011, 6, 75–76. [Google Scholar] [CrossRef] [PubMed]
- Statistical Yearbook of 2016. Issue Number: 52. Available online: https://www.stats.gov.sa/en/866-0 (accessed on 22 January 2018).
- Okeng’o, K.; Chillo, P.; Gray, W.K.; Walker, R.W.; Matuja, W. Early mortality and associated factors among patients with stroke admitted to a large teaching hospital in Tanzania. J. Stroke Cerebrovasc. Dis. 2017, 26, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Ryglewicz, D.; Barañska-Gieruszczak, M.; Lechowicz, W.; Hier, D.B. High case-fatality rates in the warsaw stroke registry. J. Stroke Cerebrovasc. Dis. 1997, 6, 421–425. [Google Scholar] [CrossRef]
- Goulart, A.C.; Bensenor, I.M.; Fernandes, T.G.; Alencar, A.P.; Fedeli, L.M.; Lotufo, P.A. Early and one-year stroke case fatality in Sao Paulo, Brazil: Applying the world health organization’s stroke steps. J. Stroke Cerebrovasc. Dis. 2012, 21, 832–838. [Google Scholar] [CrossRef] [PubMed]
- Van Asch, C.J.; Luitse, M.J.; Rinkel, G.J.; van der Tweel, I.; Algra, A.; Klijn, C.J. Incidence, case fatality and functional outcome of intracerebral haemorrhage over time, according to age, sex and ethnic origin: A systematic review and meta-analysis. Lancet Neurol. 2010, 9, 167–176. [Google Scholar] [CrossRef]
- Kalėdienė, R.; Rastenytė, D. Trends and regional inequalities in mortality from stroke in the context of health care reform in Lithuania. Medicina 2016, 52, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Alhazzani, A.A.; Mahfouz, A.A.; Abolyazid, A.Y.; Awadalla, N.J.; Aftab, R.; Faraheen, A.; Khalil, S.N. Study of stroke incidence in the aseer region, Southwestern Saudi Arabia. Int. J. Environ. Res. Public Health 2018, 15, 215. [Google Scholar] [CrossRef] [PubMed]
- Thrift, A.G.; Howard, G.; Cadilhac, D.A.; Howard, V.J.; Rothwell, P.M.; Thayabaranathan, T.; Feigin, V.L.; Norrving, B.; Donnan, G.A. Global stroke statistics: An update of mortality data from countries using a broad code of “cerebrovascular diseases”. Int. J. Stroke 2017, 12, 796–801. [Google Scholar] [CrossRef] [PubMed]
- Nkoke, C.; Lekoubou, A.; Balti, E.; Kengne, A.P. Stroke mortality and its determinants in a resource-limited setting: A prospective cohort study in Yaounde, Cameroon. J. Neurol. Sci. 2015, 358, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Nadiah, W.-A.; Amir, W.A.; Muzaimi, M.; Mustafa, M.; Naing, N.N. Determinants of mortality in first-ever stroke patients in the suburban Malaysia: A retrospective hospital-based study, 2005–2011. Iran. J. Public Health 2015, 44, 1291–1293. [Google Scholar]
- Edjoc, R.K.; Reid, R.D.; Sharma, M.; Fang, J. The prognostic effect of cigarette smoking on stroke severity, disability, length of stay in hospital and mortality in a cohort with cerebrovascular disease. J. Stroke Cerebrovasc. Dis. 2013, 22, e446–e454. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Schooling, C.M.; Chan, W.M.; Lee, S.Y.; Leung, G.M.; Lam, T.H. Smoking and hemorrhagic stroke mortality in a prospective cohort study of older Chinese. Stroke 2013, 44, 2144–2149. [Google Scholar] [CrossRef] [PubMed]
- Levine, D.A.; Walter, J.M.; Karve, S.J.; Skolarus, L.E.; Levine, S.R.; Mulhorn, K.A. Smoking and mortality in stroke survivors: Can we eliminate the paradox? J. Stroke Cerebrovasc. Dis. 2014, 23, 1282–1290. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Yang, Y.; Jin, H.; Fan, C.; Lv, P.; Sun, W.; Peng, Q.; Zhao, M.; Jin, D.K.; Wang, J.; et al. Discrepant relationships between admission blood pressure and mortality in different stroke subtypes. J. Neurol. Sci. 2017, 383, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Ntaios, G.; Faouzi, M.; Ferrari, J.; Lang, W.; Vemmos, K.; Michel, P. An integer-based score to predict functional outcome in acute ischemic stroke the astral score. Neurology 2012, 78, 1916–1922. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.; Rudd, T.; Lewis, R.R.; Hunt, B.J. Mortality from pulmonary embolism after acute stroke: Can we do better? Age Ageing 2002, 31, 159–161. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | Males | Females | Total | ||||||
|---|---|---|---|---|---|---|---|---|---|
| No. Died | CFR (%) | 95% CI | No. Died | CFR (%) | 95% CI | No. Died | CFR (%) | 95% CI | |
| <40– | 10 | 14.3 | 7.1–24.7 | 4 | 6.8 | 2.2–15.5 | 14 | 10.9 | 6.1–17.5 |
| 40–49 | 3 | 3.9 | 1.0–10.4 | 4 | 8.5 | 2.4–20.4 | 7 | 5.7 | 2.3–11.4 |
| 50–59 | 11 | 9.0 | 4.8–15.1 | 5 | 8.6 | 2.9–19.0 | 16 | 8.9 | 5.2–14.0 |
| 60–69 | 8 | 5.4 | 2.6–10.1 | 7 | 8.9 | 3.6–17.4 | 15 | 6.6 | 3.8–10.7 |
| 70–79 | 14 | 8.4 | 4.7–13.7 | 4 | 3.9 | 1.1–9.6 | 18 | 6.7 | 4.0–10.3 |
| 80+ | 25 | 12.9 | 8.5–18.4 | 26 | 20.5 | 13.8–28.5 | 51 | 15.9 | 12.1–20.4 |
| Total | 71 | 9.1 | 7.3–11.3 | 50 | 10.6 | 7.9–13.7 | 121 | 9.7 | 8.1–11.5 |
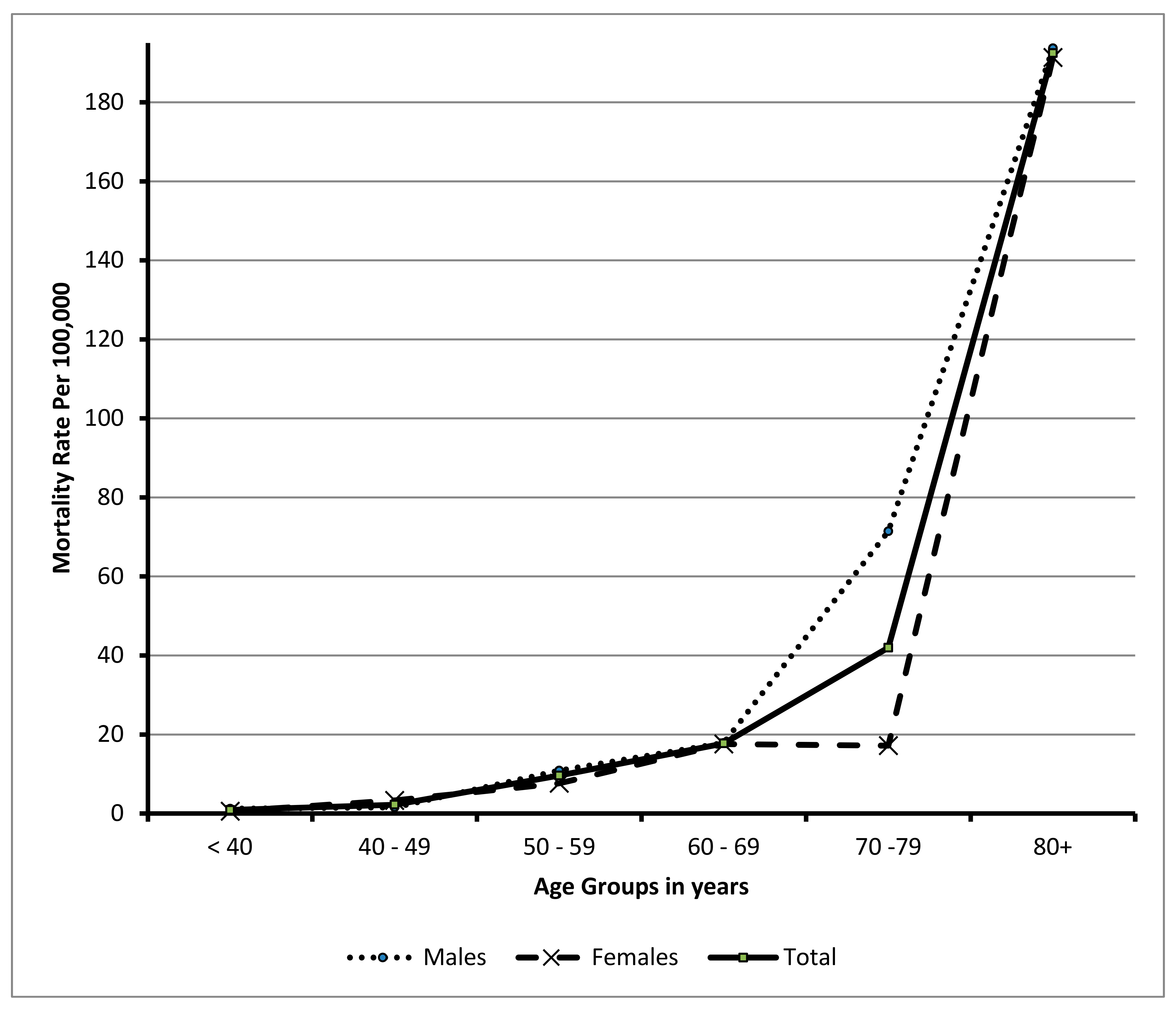
| Age Group | Males | Females | Total | |||
|---|---|---|---|---|---|---|
| Deaths/Pop. | Mortality Rate per 100,000 (95%CI) | Deaths/Pop. | Mortality Rate per 100,000 (95%CI) | Deaths/Pop. | Mortality Rate per 100,000 (95%CI) | |
| <40 | 10/813,170 | 1.230 (1.20–1.260) * | 4/719,814 | 0.560 (0.550–0.561) * | 14/1,532,984 | 0.910 (0.890–0.930) |
| 40–49 | 3/192,850 | 1.555 (1.500–1.610) * | 4/120,629 | 3.310 (3.220–3.420) * | 7/313,479 | 2.230 (2.180–2.290) |
| 50–59 | 11/101,192 | 10.870 (10.680–11.060) * | 5/65,405 | 7.644 (7.440–7.850) * | 16/166,597 | 9.604 (9.460–9.750) |
| 60–69 | 8/44,736 | 17.882 (17.530–18.240) | 7/39,806 | 17.585 (17.210–17.960) | 15/84,542 | 17.742 (17.490–18.000) |
| 70–79 | 14/19,603 | 71.417 (70.78–72.05) * | 4/23,280 | 17.18 (16.70–17.67) * | 18/42,883 | 41.97 (38.0–53.0) |
| 80+ | 25/12,909 | 193.66(186.9–200.6) | 26/13,589 | 191.33 (184.7–198.0) | 51/26,498 | 192.46 (187.7–197.3) |
| Total | 71/1,184,460 | 38.491 (38.270–38.710) * | 50/982,523 | 5.10 (5.050–5.130) * | 121/2,166,983 | 5.584 (5.550–5.610) |
| Variables | Hazard Ratio (HR) | 95.0% CI | |
|---|---|---|---|
| Lower | Upper | ||
| Socio-Demographic: | |||
| Age: 70+ vs. < 70 years | 0.950 | 0.601 | 1.500 |
| Gender: Females vs. Males | 1.317 | 0.856 | 2.025 |
| Altitude: Low vs. High | 1.220 | 0.778 | 1.913 |
| Nationality: Non-Saudi vs. Saudi | 1.644 | 0.905 | 2.985 |
| History: | |||
| Family History of stroke: Yes vs. No | 0.646 | 0.277 | 1.511 |
| Diabetes Mellitus: Yes vs. No | 0.721 | 0.429 | 1.210 |
| Hypertension: Yes vs. No * | 1.776 | 1.056 | 2.988 |
| Hypercholesterolemia: Yes vs. No | 1.208 | 0.738 | 1.977 |
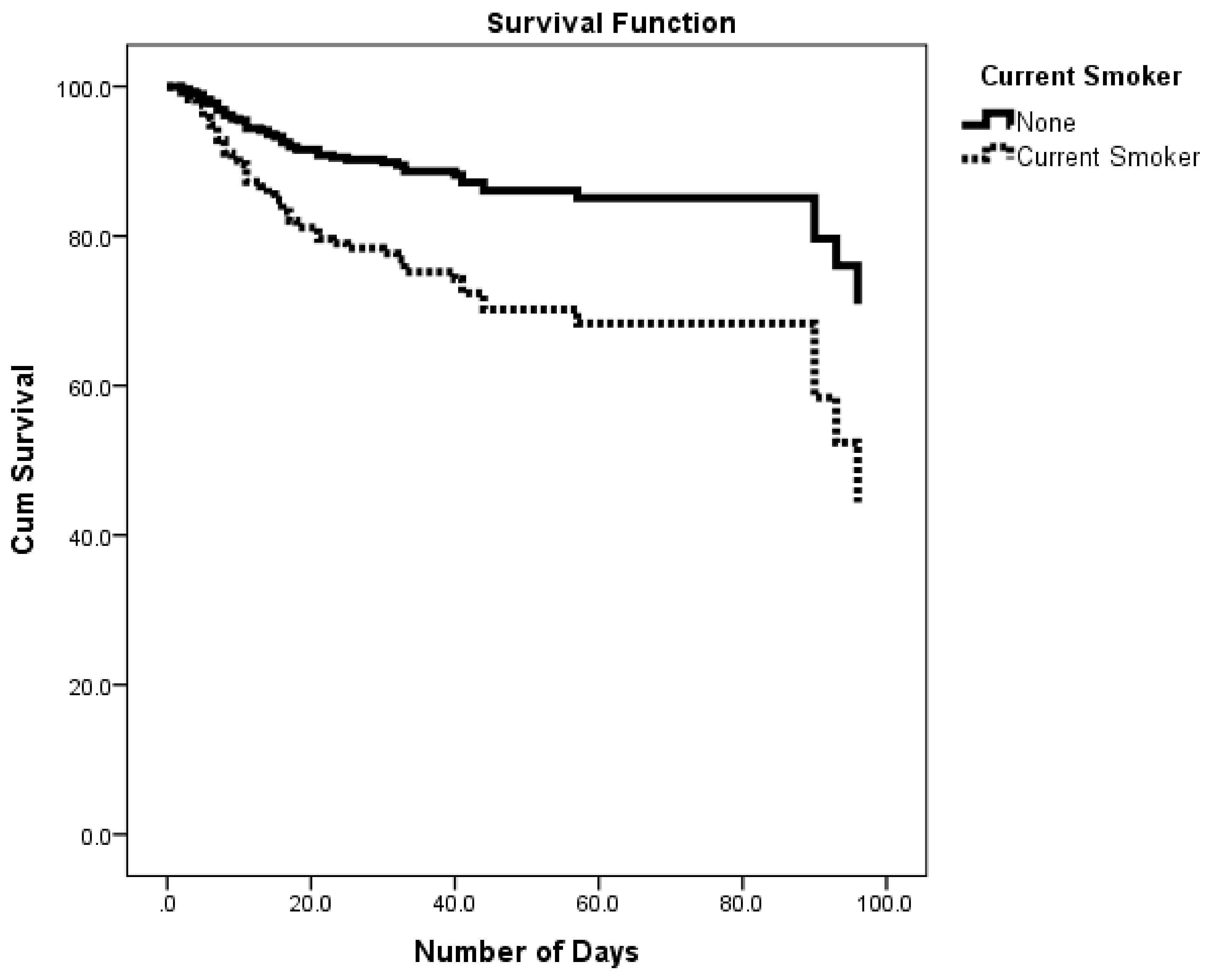
| Current Smoker: Yes vs. No * | 2.363 | 1.202 | 4.643 |
| Obesity: Yes vs. No | 1.322 | 0.884 | 1.977 |
| Atrial Fibrillation: Yes vs. No | 1.016 | 0.531 | 1.943 |
| Clinical Condition on Admission: | |||
| Level of consciousness: Drowsy or unconscious vs. alert * | 6.861 | 3.942 | 11.941 |
| Mobility: Immobile vs. mobile * | 2.605 | 1.559 | 4.352 |
| Hospital arrival time: 3 h+ vs. < 3 h | 1.319 | 0.827 | 2.104 |
| In-hospital compilations: | |||
| Deep Vein Thrombosis: Yes vs. No | 0.873 | 0.197 | 3.879 |
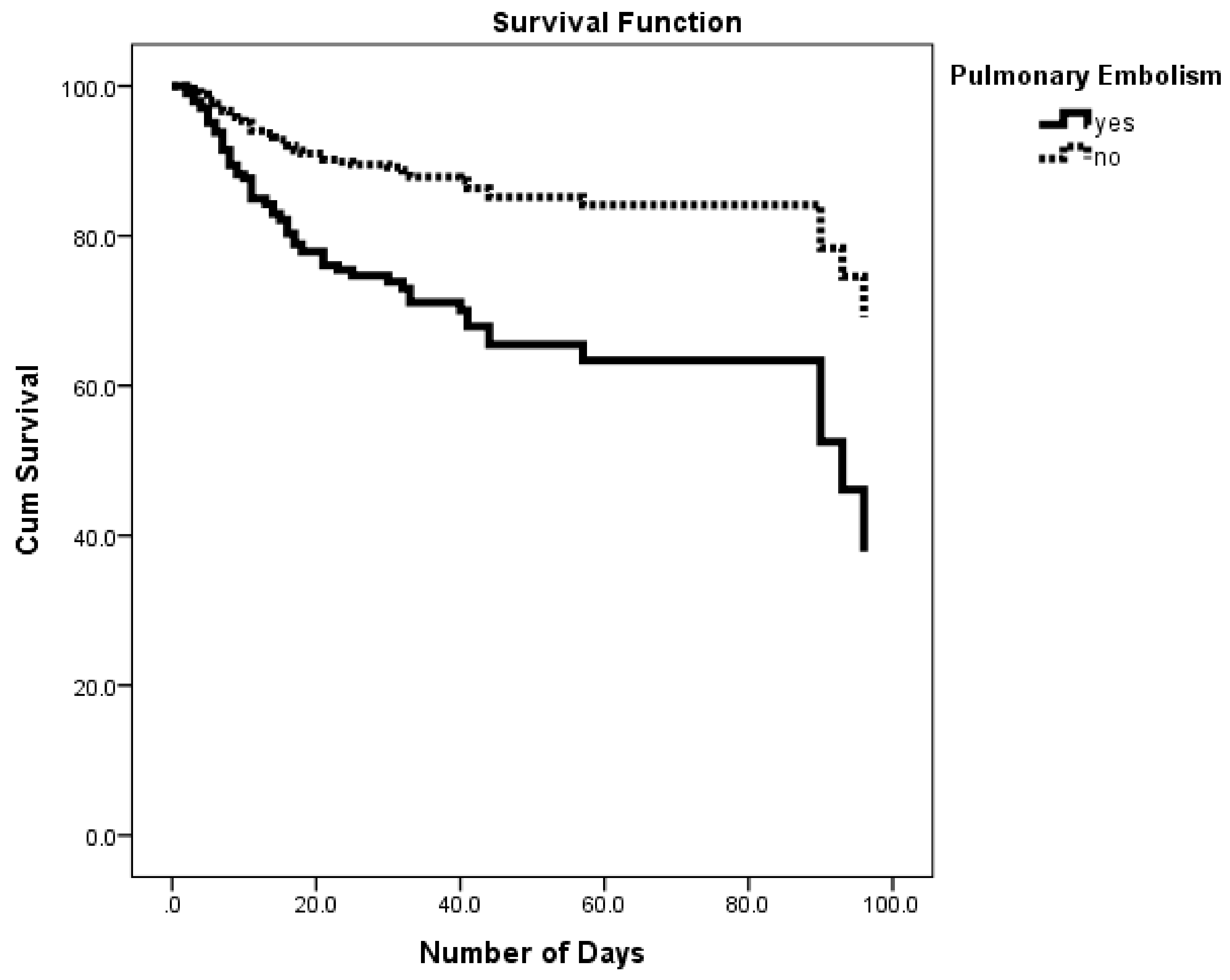
| Pulmonary Embolism: Yes vs. No * | 2.636 | 1.516 | 4.585 |
| Pneumonia: Yes vs. No | 0.700 | 0.447 | 1.096 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alhazzani, A.A.; Mahfouz, A.A.; Abolyazid, A.Y.; Awadalla, N.J.; Katramiz, K.; Faraheen, A.; Khalil, S.N.; Aftab, R. In Hospital Stroke Mortality: Rates and Determinants in Southwestern Saudi Arabia. Int. J. Environ. Res. Public Health 2018, 15, 927. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15050927
Alhazzani AA, Mahfouz AA, Abolyazid AY, Awadalla NJ, Katramiz K, Faraheen A, Khalil SN, Aftab R. In Hospital Stroke Mortality: Rates and Determinants in Southwestern Saudi Arabia. International Journal of Environmental Research and Public Health. 2018; 15(5):927. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15050927
Chicago/Turabian StyleAlhazzani, Adel A., Ahmed A. Mahfouz, Ahmed Y. Abolyazid, Nabil J. Awadalla, Khaled Katramiz, Aesha Faraheen, Shamsun Nahar Khalil, and Razia Aftab. 2018. "In Hospital Stroke Mortality: Rates and Determinants in Southwestern Saudi Arabia" International Journal of Environmental Research and Public Health 15, no. 5: 927. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15050927