Systematic Literature Review of Attempted Suicide and Offspring

Abstract
:1. Introduction
1.1. Experiencing a Parental Suicide Attempt
1.2. Risk Is Associated with Parental Psychiatric Disorders
1.3. Risk Factors and Transmission of Parental Suicidal Behaviour
1.4. Review Questions
- (a)
- Do guidelines (advice for health care personnel in order to assure quality of the services) and routines (fixed program or regularly actions) exist to screen for and follow-up children of parents attempting suicide?
- (b)
- Are there interventional studies aimed at treating or following up children after a parent has attempted suicide?
2. Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Data Sources and Search Strategy
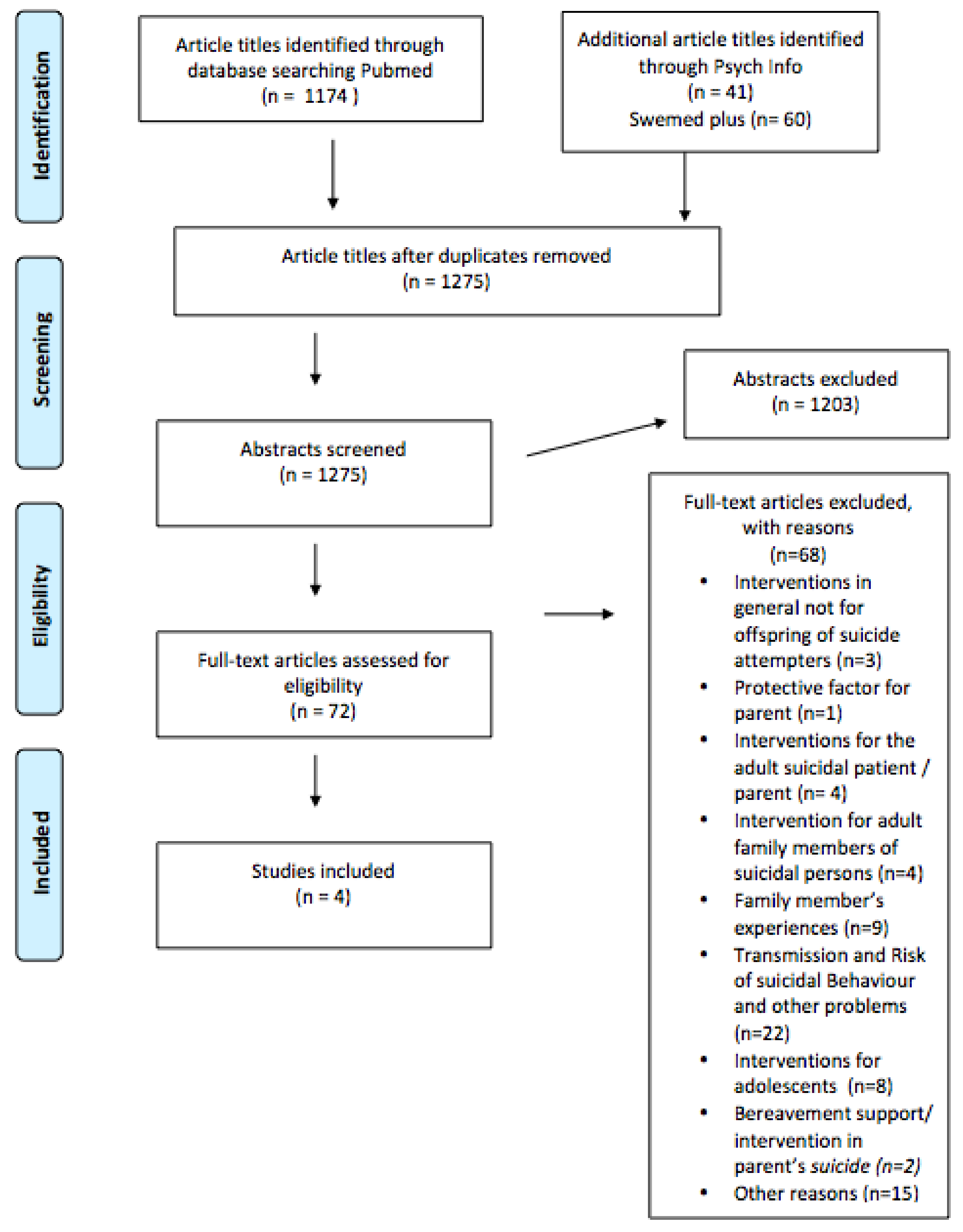
2.4. Study Selection
3. Results
4. Discussion
4.1. Summary of Evidence
4.2. Limitations
4.3. Consequences Practical Implications
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Cerel, J.; Frey, L.M.; Maple, M.; Kinner, D.G. Parents with suicidal behavior: Parenting is not always protective. J. Child Fam. Stud. 2016, 25, 2327–2336. [Google Scholar] [CrossRef]
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Koss, M.P.; Marks, J.S. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The adverse childhood experiences (ace) study. Am. J. Prev. Med. 1998, 14, 245–258. [Google Scholar] [CrossRef]
- Sun, F.K.; Long, A. A theory to guide families and carers of people who are at risk of suicide. J. Clin. Nurs. 2008, 17, 1939–1948. [Google Scholar] [CrossRef] [PubMed]
- Magne-Ingvar, U.; Ojehagen, A. One-year follow-up of significant others of suicide attempters. Soc. Psychiatry Psychiatr. Epidemiol. 1999, 34, 470–476. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, C.; McGowan, I.; O’Neill, S.; Kernohan, G. The burden of living with and caring for a suicidal family member. J. Ment. Health 2014, 23, 236–240. [Google Scholar] [CrossRef] [PubMed]
- Bjornaas, M.A.; Hovda, K.E.; Heyerdahl, F.; Skog, K.; Drottning, P.; Opdahl, A.; Jacobsen, D.; Ekeberg, O. Suicidal intention, psychosocial factors and referral to further treatment: A one-year cross-sectional study of self-poisoning. BMC Psychiatry 2010, 10, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hawton, K.; Saunders, K.; Topiwala, A.; Haw, C. Psychiatric disorders in patients presenting to hospital following self-harm: A systematic review. J. Affect. Disord. 2013, 151, 821–830. [Google Scholar] [CrossRef] [PubMed]
- Grimholt, T.K.; Jacobsen, D.; Haavet, O.R.; Sandvik, L.; Jorgensen, T.; Norheim, A.B.; Ekeberg, O. Effect of systematic follow-up by general practitioners after deliberate self-poisoning: A randomised controlled trial. PLoS ONE 2015, 10, e0143934. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, J.; Ellis, J.B. Family support and other social factors precipitating suicidal ideation. Int. J. Soc. Psychiatry 1995, 41, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Beardslee, W.R.; Versage, E.M.; Gladstone, T.R. Children of affectively ill parents: A review of the past 10 years. J. Am. Acad. Child Adolesc. Psychiatry 1998, 37, 1134–1141. [Google Scholar] [CrossRef] [PubMed]
- Klimes-Dougan, B.; Free, K.; Ronsaville, D.; Stilwell, J.; Welsh, C.J.; Radke-Yarrow, M. Suicidal ideation and attempts: A longitudinal investigation of children of depressed and well mothers. J. Am. Acad. Child Adolesc. Psychiatry 1999, 38, 651–659. [Google Scholar] [CrossRef] [PubMed]
- Stenager, K.; Qin, P. Individual and parental psychiatric history and risk for suicide among adolescents and young adults in denmark: A population-based study. Soc. Psychiatry Psychiatr. Epidemiol. 2008, 43, 920–926. [Google Scholar] [CrossRef] [PubMed]
- Weissman, M.M.; Fendrich, M.; Warner, V.; Wickramaratne, P. Incidence of psychiatric disorder in offspring at high and low risk for depression. J. Am. Acad. Child Adolesc. Psychiatry 1992, 31, 640–648. [Google Scholar] [CrossRef] [PubMed]
- King, C.A.; Kerr, D.C.; Passarelli, M.N.; Foster, C.E.; Merchant, C.R. One-year follow-up of suicidal adolescents: Parental history of mental health problems and time to post-hospitalization attempt. J. Youth Adolesc. 2010, 39, 219–232. [Google Scholar] [CrossRef] [PubMed]
- Camarena, B.; Fresan, A.; Sarmiento, E. Exploring personality features in patients with affective disorders and history of suicide attempts: A comparative study with their parents and control subjects. Depression Res. Treat. 2014, 2014, 291802. [Google Scholar] [CrossRef] [PubMed]
- Burke, A.K.; Galfalvy, H.; Everett, B.; Currier, D.; Zelazny, J.; Oquendo, M.A.; Melhem, N.M.; Kolko, D.; Harkavy-Friedman, J.M.; Birmaher, B.; et al. Effect of exposure to suicidal behavior on suicide attempt in a high-risk sample of offspring of depressed parents. J. Am. Acad. Child Adolesc. Psychiatry 2010, 49, 114–121. [Google Scholar] [PubMed]
- Geulayov, G.; Metcalfe, C.; Heron, J.; Kidger, J.; Gunnell, D. Parental suicide attempt and offspring self-harm and suicidal thoughts: Results from the avon longitudinal study of parents and children (alspac) birth cohort. J. Am. Acad. Child Adolesc. Psychiatry 2014, 53, 509–517. [Google Scholar] [CrossRef] [PubMed]
- Jeglic, E.L.; Sharp, I.R.; Chapman, J.E.; Brown, G.K.; Beck, A.T. History of family suicide behaviors and negative problem solving in multiple suicide attempters. Arch. Suicide Res. 2005, 9, 135–146. [Google Scholar] [CrossRef] [PubMed]
- Lieb, R.; Bronisch, T.; Hofler, M.; Schreier, A.; Wittchen, H.U. Maternal suicidality and risk of suicidality in offspring: Findings from a community study. Am. J. Psychiatry 2005, 162, 1665–1671. [Google Scholar] [CrossRef] [PubMed]
- Niederkrotenthaler, T.; Floderus, B.; Alexanderson, K.; Rasmussen, F.; Mittendorfer-Rutz, E. Exposure to parental mortality and markers of morbidity, and the risks of attempted and completed suicide in offspring: An analysis of sensitive life periods. J. Epidemiol. Community Health 2012, 66, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Mittendorfer-Rutz, E.; Rasmussen, F.; Wasserman, D. Familial clustering of suicidal behaviour and psychopathology in young suicide attempters. A register-based nested case control study. Soc. Psychiatry Psychiatr. Epidemiol. 2008, 43, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Geulayov, G.; Metcalfe, C.; Gunnell, D. Parental suicide attempt and offspring educational attainment during adolescence in the avon longitudinal study of parents and children (alspac) birth cohort. Psychol. Med. 2016, 46, 2097–2107. [Google Scholar] [CrossRef] [PubMed]
- McManama O’Brien, K.H.; Salas-Wright, C.P.; Vaughn, M.G.; LeCloux, M. Childhood exposure to a parental suicide attempt and risk for substance use disorders. Addict. Behav. 2015, 46, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Hawton, K.; Roberts, J.; Goodwin, G. The risk of child abuse among mothers who attempt suicide. Br. J. Psychiatry 1985, 146, 486–489. [Google Scholar] [CrossRef] [PubMed]
- Heider, D.; Bernert, S.; Matschinger, H.; Haro, J.M.; Alonso, J.; Angermeyer, M.C. Parental bonding and suicidality in adulthood. Aust. N. Z. J. Psychiatry 2007, 41, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Ehnvall, A.; Parker, G.; Hadzi-Pavlovic, D.; Malhi, G. Perception of rejecting and neglectful parenting in childhood relates to lifetime suicide attempts for females—But not for males. Acta Psychiatr. Scand. 2008, 117, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Donath, C.; Graessel, E.; Baier, D.; Bleich, S.; Hillemacher, T. Is parenting style a predictor of suicide attempts in a representative sample of adolescents? BMC Pediatr. 2014, 14, 113. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Castroman, J.; Guillaume, S.; Olie, E.; Jaussent, I.; Baca-Garcia, E.; Courtet, P. The additive effect on suicidality of family history of suicidal behavior and early traumatic experiences. Arch. Suicide Res. 2015, 19, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Grimholt, T.K.; Bjornaas, M.A.; Jacobsen, D.; Dieserud, G.; Ekeberg, O. Treatment received, satisfaction with health care services, and psychiatric symptoms 3 months after hospitalization for self-poisoning. Ann. Gen. Psychiatry 2012, 11, 10. [Google Scholar] [CrossRef] [PubMed]
- Ferro, T.; Verdeli, H.; Pierre, F.; Weissman, M.M. Screening for depression in mothers bringing their offspring for evaluation or treatment of depression. Am. J. Psychiatry 2000, 157, 375–379. [Google Scholar] [CrossRef] [PubMed]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Group, P.-P. Preferred reporting items for systematic review and meta-analysis protocols (prisma-p) 2015: Elaboration and explanation. BMJ 2015, 349, g7647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, M.; Tiwari, A.; Fu, R.; Moe, E.; Buckley, D.I. A Framework to Facilitate the Use of Systematic Reviews and Meta-Analyses in the Design of Primary Research Studies; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2012. [Google Scholar]
- Mitchell, A.M.; Wesner, S.; Garand, L.; Gale, D.D.; Havill, A.; Brownson, L. A support group intervention for children bereaved by parental suicide. J. Child Adolesc. Psychiatr. Nurs. 2007, 20, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Sandler, I.; Tein, J.Y.; Wolchik, S.; Ayers, T.S. The effects of the family bereavement program to reduce suicide ideation and/or attempts of parentally bereaved children six and fifteen years later. Suicide Life Threat. Behav. 2016, 46, S32–S38. [Google Scholar] [CrossRef] [PubMed]
- Berk, M.S.; Asarnow, J.R. Assessment of suicidal youth in the emergency department. Suicide Life Threat. Behav. 2015, 45, 345–359. [Google Scholar] [CrossRef] [PubMed]
- Boeninger, D.K.; Masyn, K.E.; Conger, R.D. Testing alternative explanations for the associations between parenting and adolescent suicidal problems. J. Res. Adolesc. 2013, 23, 331–344. [Google Scholar] [CrossRef] [PubMed]
- Cloutier, P.; Kennedy, A.; Maysenhoelder, H.; Glennie, E.J.; Cappelli, M.; Gray, C. Pediatric mental health concerns in the emergency department: Caregiver and youth perceptions and expectations. Pediatr. Emerg. Care 2010, 26, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Gabel, S.; Shindledecker, R. Parental substance abuse and suspected child abuse/maltreatment predict outcome in children’s inpatient treatment. J. Am. Acad. Child Adolesc. Psychiatry 1990, 29, 919–924. [Google Scholar] [CrossRef] [PubMed]
- Pineda, J.; Dadds, M.R. Family intervention for adolescents with suicidal behavior: A randomized controlled trial and mediation analysis. J. Am. Acad. Child Adolesc. Psychiatry 2013, 52, 851–862. [Google Scholar] [CrossRef] [PubMed]
- Saffer, B.Y.; Glenn, C.R.; David Klonsky, E. Clarifying the relationship of parental bonding to suicide ideation and attempts. Suicide Life Threat. Behav. 2015, 45, 518–528. [Google Scholar] [CrossRef] [PubMed]
- Shpigel, M.S.; Diamond, G.M.; Diamond, G.S. Changes in parenting behaviors, attachment, depressive symptoms, and suicidal ideation in attachment-based family therapy for depressive and suicidal adolescents. J. Marital Fam. Ther. 2012, 38, 271–283. [Google Scholar] [CrossRef] [PubMed]
- Spirito, A.; Wolff, J.C.; Seaboyer, L.M.; Hunt, J.; Esposito-Smythers, C.; Nugent, N.; Zlotnick, C.; Miller, I. Concurrent treatment for adolescent and parent depressed mood and suicidality: Feasibility, acceptability, and preliminary findings. J. Child Adolesc. Psychopharmacol. 2015, 25, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Dorpat, T.L.; Jackson, J.K.; Ripley, H.S. Broken homes and attempted and completed suicide. Arch. Gen. Psychiatry 1965, 12, 213–216. [Google Scholar] [CrossRef] [PubMed]
- Keitner, G.I.; Miller, I.W. Family functioning and major depression: An overview. Am. J. Psychiatry 1990, 147, 1128–1137. [Google Scholar] [PubMed]
- Melhem, N.M.; Brent, D.A.; Ziegler, M.; Iyengar, S.; Kolko, D.; Oquendo, M.; Birmaher, B.; Burke, A.; Zelazny, J.; Stanley, B.; et al. Familial pathways to early-onset suicidal behavior: Familial and individual antecedents of suicidal behavior. Am. J. Psychiatry 2007, 164, 1364–1370. [Google Scholar] [CrossRef] [PubMed]
- Rutz, E.M. Offspring of suicide attempters at greater risk of suicide events. Evid.-Based Ment. Health 2008, 11, 55. [Google Scholar] [CrossRef] [PubMed]
- Timmons, K.A.; Selby, E.A.; Lewinsohn, P.M.; Joiner, T.E. Parental displacement and adolescent suicidality: Exploring the role of failed belonging. J. Clin. Child Adolesc. Psychol. 2011, 40, 807–817. [Google Scholar] [CrossRef] [PubMed]
- Torjesen, I. Children whose parents attempted suicide are at raised risk of similar behaviour, study finds. BMJ 2015, 350, g7862. [Google Scholar] [CrossRef] [PubMed]
- Tuckman, J.; Youngman, W.F. Attempted suicide and family disorganization. J. Genet. Psychol. 1964, 105, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Valenstein, H.; Cronkite, R.C.; Moos, R.H.; Snipes, C.; Timko, C. Suicidal ideation in adult offspring of depressed and matched control parents: Childhood and concurrent predictors. J. Ment. Health 2012, 21, 459–468. [Google Scholar] [CrossRef] [PubMed]
- Brent, D.A.; Perper, J.A.; Moritz, G.; Liotus, L.; Schweers, J.; Balach, L.; Roth, C. Familial risk factors for adolescent suicide: A case-control study. Acta Psychiatr. Scand. 1994, 89, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Weich, S.; Patterson, J.; Shaw, R.; Stewart-Brown, S. Family relationships in childhood and common psychiatric disorders in later life: Systematic review of prospective studies. Br. J. Psychiatry 2009, 194, 392–398. [Google Scholar] [CrossRef] [PubMed]
- Goschin, S.; Briggs, J.; Blanco-Lutzen, S.; Cohen, L.J.; Galynker, I. Parental affectionless control and suicidality. J. Affect. Disord. 2013, 151, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Livingston, R. Children of people with somatization disorder. J. Am. Acad. Child Adolesc. Psychiatry 1993, 32, 536–544. [Google Scholar] [CrossRef] [PubMed]
- MacGregor, E.K.; Grunebaum, M.F.; Galfalvy, H.C.; Melhem, N.; Burke, A.K.; Brent, D.A.; Oquendo, M.A.; Mann, J.J. Depressed parents’ attachment: Effects on offspring suicidal behavior in a longitudinal family study. J. Clin. Psychiatry 2014, 75, 879–885. [Google Scholar] [CrossRef] [PubMed]
- Mackrill, T.; Hesse, M. Suicide behavior in parents with alcohol abuse problems and suicide behavior in their offspring-adult offspring and counselor perspectives. Nord. J. Psychiatry 2012, 66, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Abrahams, D.; Golden, J.S. Psychiatric consultations on a medical ward. Arch. Intern. Med. 1963, 112, 766–774. [Google Scholar] [CrossRef] [PubMed]
- Ai, A.L.; Weiss, S.I.; Fincham, F.D. Family factors contribute to general anxiety disorder and suicidal ideation among latina americans. Women’s Health Issues 2014, 24, e345–e352. [Google Scholar] [CrossRef] [PubMed]
- Barrero, S.A. Preventing suicide: A resource for the family. Ann. Gen. Psychiatry 2008, 7, 1. [Google Scholar] [CrossRef] [PubMed]
- Bridge, J.A.; Reynolds, B.; McBee-Strayer, S.M.; Sheftall, A.H.; Ackerman, J.; Stevens, J.; Mendoza, K.; Campo, J.V.; Brent, D.A. Impulsive aggression, delay discounting, and adolescent suicide attempts: Effects of current psychotropic medication use and family history of suicidal behavior. J. Child Adolesc. Psychopharmacol. 2015, 25, 114–123. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, J. Parasuicide and the family physician. Can. Fam. Physician 1979, 25, 1315–1318. [Google Scholar] [PubMed]
- Fowler, S.B.; Sweeney, J.B. Challenges in patient and family care following an unsuccessful suicide attempt. J. Neurosci. Nurs. 1996, 28, 234–237. [Google Scholar] [CrossRef] [PubMed]
- Greenley, J.R. The psychiatric patient’s family and length of hospitalization. J. Health Soc. Behav. 1972, 13, 25–37. [Google Scholar] [CrossRef] [PubMed]
- Hammerton, G.; Zammit, S.; Potter, R.; Thapar, A.; Collishaw, S. Validation of a composite of suicide items from the mood and feelings questionnaire (mfq) in offspring of recurrently depressed parents. Psychiatry Res. 2014, 216, 82–88. [Google Scholar] [CrossRef] [PubMed]
- O’Mara, R.M.; Hill, R.M.; Cunningham, R.M.; King, C.A. Adolescent and parent attitudes toward screening for suicide risk and mental health problems in the pediatric emergency department. Pediatr. Emerg. Care 2012, 28, 626–632. [Google Scholar] [CrossRef] [PubMed]
- Onwumere, J.; Bebbington, P.; Kuipers, E. Family interventions in early psychosis: Specificity and effectiveness. Epidemiol. Psychiatr. Sci. 2011, 20, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Rice, F.; Lifford, K.J.; Thomas, H.V.; Thapar, A. Mental health and functional outcomes of maternal and adolescent reports of adolescent depressive symptoms. J. Am. Acad. Child Adolesc. Psychiatry 2007, 46, 1162–1170. [Google Scholar] [CrossRef] [PubMed]
- Skegg, K. Self-harm. Lancet 2005, 366, 1471–1483. [Google Scholar] [CrossRef]
- Buckle, R.C.; Linnane, J.; McConachy, N. Attempted suicide presenting at the alfred hospital, melbourne. Med. J. Aust. 1965, 1, 754–758. [Google Scholar] [PubMed]
- Shochet, B.R. Attempted suicide: Experience in a general hospital emergency service. Md. State Med. J. 1964, 13, 107–112. [Google Scholar] [PubMed]
- Waggoner, R.W., Jr.; Shearer, M. The child’s call for help. Mich. Med. 1968, 67, 846–851. [Google Scholar] [PubMed]
- Cerel, J.; Currier, G.W.; Conwell, Y. Consumer and family experiences in the emergency department following a suicide attempt. J. Psychiatr. Pract. 2006, 12, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Frey, L.M.; Hans, J.D.; Cerel, J. Suicide disclosure in suicide attempt survivors: Does family reaction moderate or mediate disclosure’s effect on depression? Suicide Life Threat. Behav. 2016, 46, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Sun, F.K.; Ko, C.J.; Chang, S.L.; Chiang, C.Y. Comparison study of postdischarge care provided to suicide patients by family members in east and south taiwan. J. Nurs. Res. 2012, 20, 53–65. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Williams, A.G.; McGee, R.E. Responding to a suicidal friend or family member: A qualitative study of college students. Death Stud. 2016, 40, 80–87. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, C.; McGowan, I.; Kernohan, G.; O’Neill, S. The unmet support needs of family members caring for a suicidal person. J. Ment. Health 2016, 25, 212–216. [Google Scholar] [CrossRef] [PubMed]
- Sun, F.K.; Long, A.; Huang, X.Y.; Chiang, C.Y. A grounded theory study of action/interaction strategies used when taiwanese families provide care for formerly suicidal patients. Public Health Nurs. 2009, 26, 543–552. [Google Scholar] [CrossRef] [PubMed]
- Mishara, B.L.; Houle, J.; Lavoie, B. Comparison of the effects of four suicide prevention programs for family and friends of high-risk suicidal men who do not seek help themselves. Suicide Life Threat. Behav. 2005, 35, 329–342. [Google Scholar] [CrossRef] [PubMed]
- Rajalin, M.; Wickholm-Pethrus, L.; Hursti, T.; Jokinen, J. Dialectical behavior therapy-based skills training for family members of suicide attempters. Arch. Suicide Res. 2009, 13, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Sun, F.K.; Chiang, C.Y.; Lin, Y.H.; Chen, T.B. Short-term effects of a suicide education intervention for family caregivers of people who are suicidal. J. Clin. Nurs. 2014, 23, 91–102. [Google Scholar] [CrossRef] [PubMed]
- Nosek, C.L. Managing a depressed and suicidal loved one at home: Impact on the family. J. Psychosoc. Nurs. Ment. Health Serv. 2008, 46, 36–44. [Google Scholar] [PubMed]
- Lansky, M.R. The subacute hospital treatment of the borderline patient: III. Management of suicidal crisis by family intervention. Hillside J. Clin. Psychiatry 1989, 11, 81–97. [Google Scholar] [PubMed]
- Haaland, M. Family in crisis—Need for cross-professional team work. Sykepleien 1985, 72, 24–27. [Google Scholar] [PubMed]
- Richman, J. The family therapy of attempted suicide. Fam. Process 1979, 18, 131–142. [Google Scholar] [CrossRef] [PubMed]
- Swartz, H.A.; Zuckoff, A.; Frank, E.; Spielvogle, H.N.; Shear, M.K.; Fleming, M.A.; Scott, J. An open-label trial of enhanced brief interpersonal psychotherapy in depressed mothers whose children are receiving psychiatric treatment. Depression Anxiety 2006, 23, 398–404. [Google Scholar] [CrossRef] [PubMed]
- Woods, A.M.; Zimmerman, L.; Carlin, E.; Hill, A.; Kaslow, N.J. Motherhood, reasons for living, and suicidality among african american women. J. Fam. Psychol. 2013, 27, 600–606. [Google Scholar] [CrossRef] [PubMed]
- Reider, E.E.; Sims, B.E. Family-based preventive interventions: Can the onset of suicidal ideation and behavior be prevented? Suicide Life Threat. Behav. 2016, 46, S3–S7. [Google Scholar] [CrossRef] [PubMed]
- Brent, D. Prevention programs to augment family and child resilience can have lasting effects on suicidal risk. Suicide Life Threat. Behav. 2016, 46, S39–S47. [Google Scholar] [CrossRef] [PubMed]
- Au, A.C.; Lau, S.; Lee, M.T. Suicide ideation and depression: The moderation effects of family cohesion and social self-concept. Adolescence 2009, 44, 851–868. [Google Scholar] [PubMed]
- Diderich, H.M.; Fekkes, M.; Dechesne, M.; Buitendijk, S.E.; Oudesluys-Murphy, A.M. Detecting child abuse based on parental characteristics: Does the hague protocol cause parents to avoid the emergency department? Int. Emerg. Nurs. 2015, 23, 203–206. [Google Scholar] [CrossRef] [PubMed]
- Diderich, H.M.; Fekkes, M.; Verkerk, P.H.; Pannebakker, F.D.; Velderman, M.K.; Sorensen, P.J.; Baeten, P.; Oudesluys-Murphy, A.M. A new protocol for screening adults presenting with their own medical problems at the emergency department to identify children at high risk for maltreatment. Child Abus. Negl. 2013, 37, 1122–1131. [Google Scholar] [CrossRef] [PubMed]
- Diderich, H.; Pannebakker, F.; Dechesne, M.; Buitendijk, S.; Oudesluys-Murphy, A. Support and monitoring of families after child abuse detection based on parental characteristics at the emergency department. Child Care Health Dev. 2015, 41, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Hawton, K.; Witt, K.G.; Taylor Salisbury, T.L.; Arensman, E.; Gunnell, D.; Hazell, P.; Townsend, E.; van Heeringen, K. Psychosocial interventions for self-harm in adults. Cochrane Database Syst. Rev. 2016. [Google Scholar] [CrossRef] [PubMed]
- Hawton, K.; Witt, K.G.; Taylor Salisbury, T.L.; Arensman, E.; Gunnell, D.; Townsend, E.; van Heeringen, K.; Hazell, P. Interventions for self-harm in children and adolescents. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef] [PubMed]
- Conner, K.R.; Bossarte, R.M.; Lu, N.; Kaukeinen, K.; Chan, G.; Wyman, P.; Tu, X.M.; Goldston, D.B.; Houston, R.J.; Bucholz, K.K.; et al. Parent and child psychopathology and suicide attempts among children of parents with alcohol use disorder. Arch. Suicide Res. 2014, 18, 117–130. [Google Scholar] [CrossRef] [PubMed]
- Reupert, A.E.; Cuff, R.; Drost, L.; Foster, K.; van Doesum, K.T.; van Santvoort, F. Intervention programs for children whose parents have a mental illness: A review. Med. J. Aust. 2013, 199, S18–S22. [Google Scholar] [CrossRef] [PubMed]
- Hickey, L.; Hawton, K.; Fagg, J.; Weitzel, H. Deliberate self-harm patients who leave the accident and emergency department without a psychiatric assessment: A neglected population at risk of suicide. J. Psychosom. Res. 2001, 50, 87–93. [Google Scholar] [CrossRef]


{kind=link}
| Country Year Reference | Design | Setting/Participants | n | Intervention | Outcome | Results |
|---|---|---|---|---|---|---|
| Netherland 2015 [90] | Case–control Study (before-after) & qualitative design Parents (n = 14) interviewed by telephone | Emergency department Parents admitted for -domestic violence -substance abuse or -suicide attempt or self-harm. | 14 | Referral made to the Reporting Center for Child Abuse and Neglect (RCCAN). | Does parents avoid medical care? | Parents don’t avoid medical care if referred No decline in the number of patients, included in the Protocol |
| Netherland 2015 [91] | Case Study | Emergency department referrals based on parental characteristics in which child abuse was confirmed after investigation by the RCCAN were analysed | 100 (99) | Consequences for the families three months after referral: Type of child abuse, reason for reporting, duration of problems prior to the ED referral, previous involvement of support services or other agencies, re-occurrence of the problems and outcome of the RCCAN monitoring l. | Existing support continued or intensified n = 31 Child Protection Services report made n = 24 New support organized n = 27 Support not necessary n = 17 Not followed up n = 31. | |
| Netherland 2013 [92] | Case-control Study (before-after) | Nine Emergency departments in 3 regions (one intervention region and 2 control regions). From January 2006 to November 2007 | Screening and Reporting to Centre for Child Abuse and Neglect (RCCAN) to assess family problems and offer voluntary community based support to parents. | Referrals to the Centre for Child Abuse and Neglect | Before implementation of the protocol (1 per 100,000) After implementation of the protocol (64 per 100,000). In the control region (1 per 100,000) and (3 per 100,000) (OR = 28.0 (95 CI 4.6–170.7)). | |
| United Kingdom 1985 [24] | Case-control Study | Mothers with children aged five years and under admitted to General hospital for attempted suicide | 114 | No | Child abuse | Risk of child abuse was identified in 29.8% of those who attempted suicide. |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lunde, I.; Myhre Reigstad, M.; Frisch Moe, K.; Grimholt, T.K. Systematic Literature Review of Attempted Suicide and Offspring. Int. J. Environ. Res. Public Health 2018, 15, 937. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15050937
Lunde I, Myhre Reigstad M, Frisch Moe K, Grimholt TK. Systematic Literature Review of Attempted Suicide and Offspring. International Journal of Environmental Research and Public Health. 2018; 15(5):937. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15050937
Chicago/Turabian StyleLunde, Ingeborg, Marte Myhre Reigstad, Kristin Frisch Moe, and Tine K. Grimholt. 2018. "Systematic Literature Review of Attempted Suicide and Offspring" International Journal of Environmental Research and Public Health 15, no. 5: 937. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15050937