Lifestyle Health Behaviors of Nurses and Midwives: The ‘Fit for the Future’ Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Measures
2.3. Analysis
3. Results
3.1. Nurses’ Health-Related Behaviors
3.1.1. Diet
3.1.2. Physical Activity
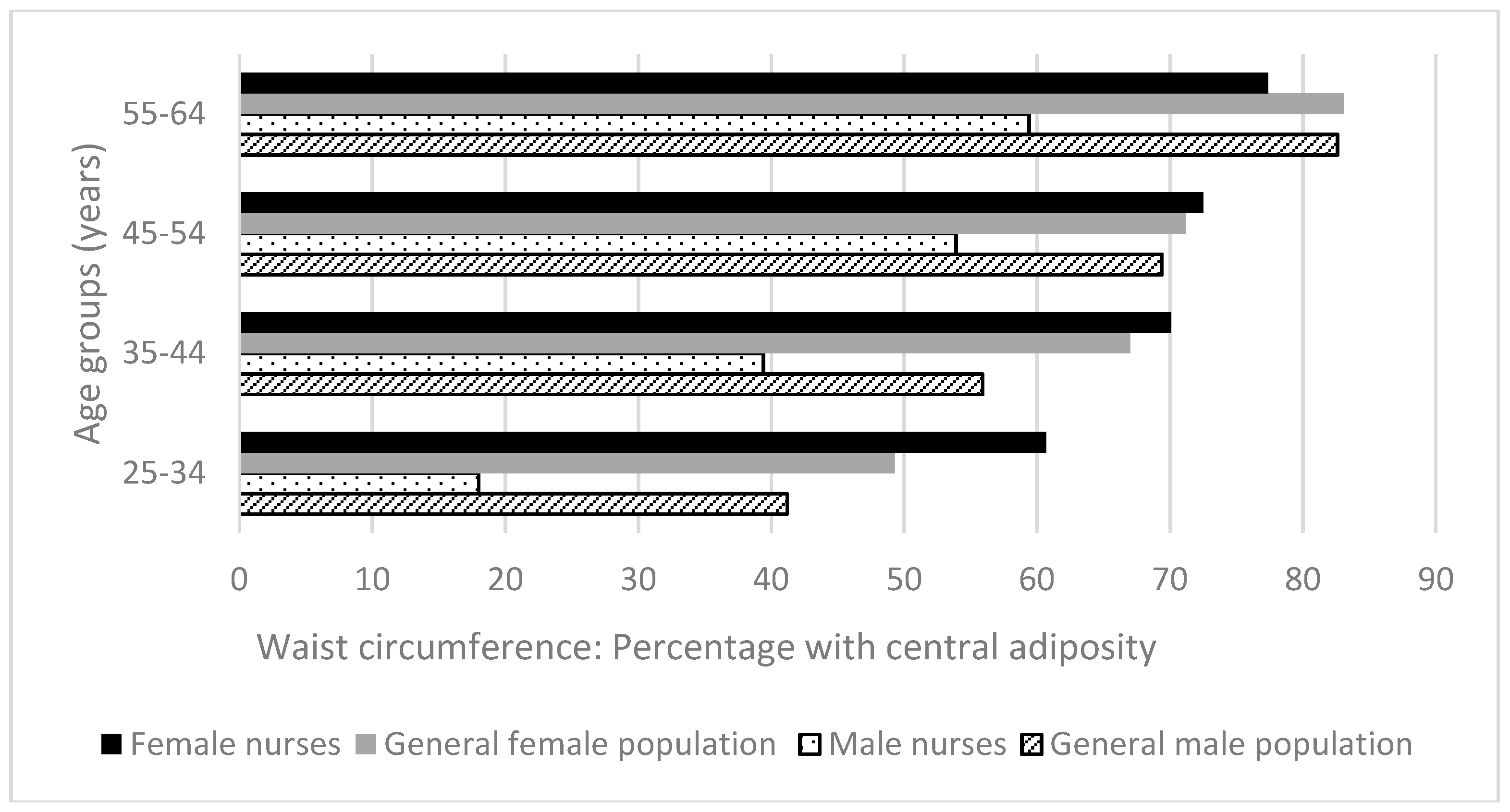
3.1.3. BMI and Waist Circumference
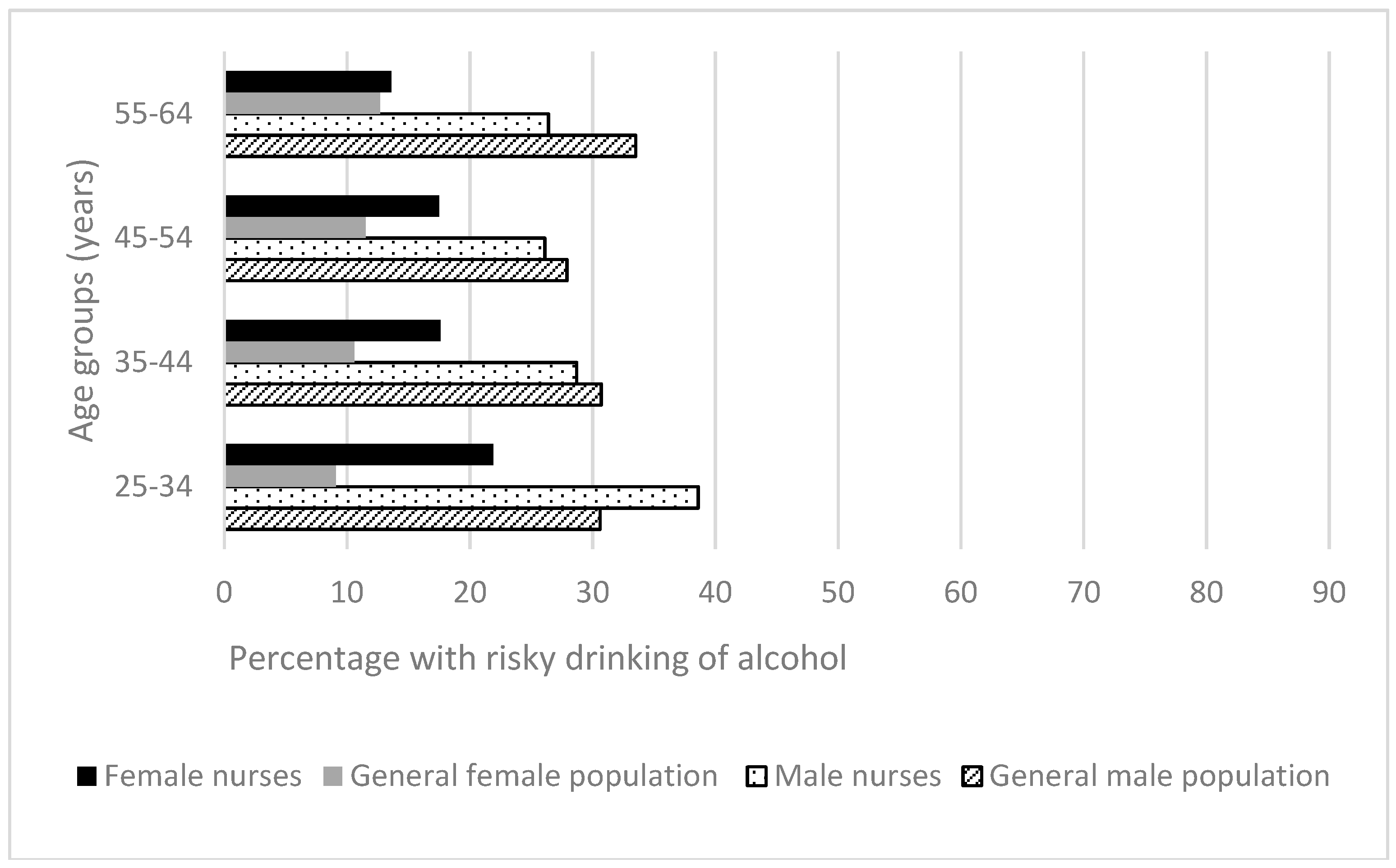
3.1.4. Risky Drinking
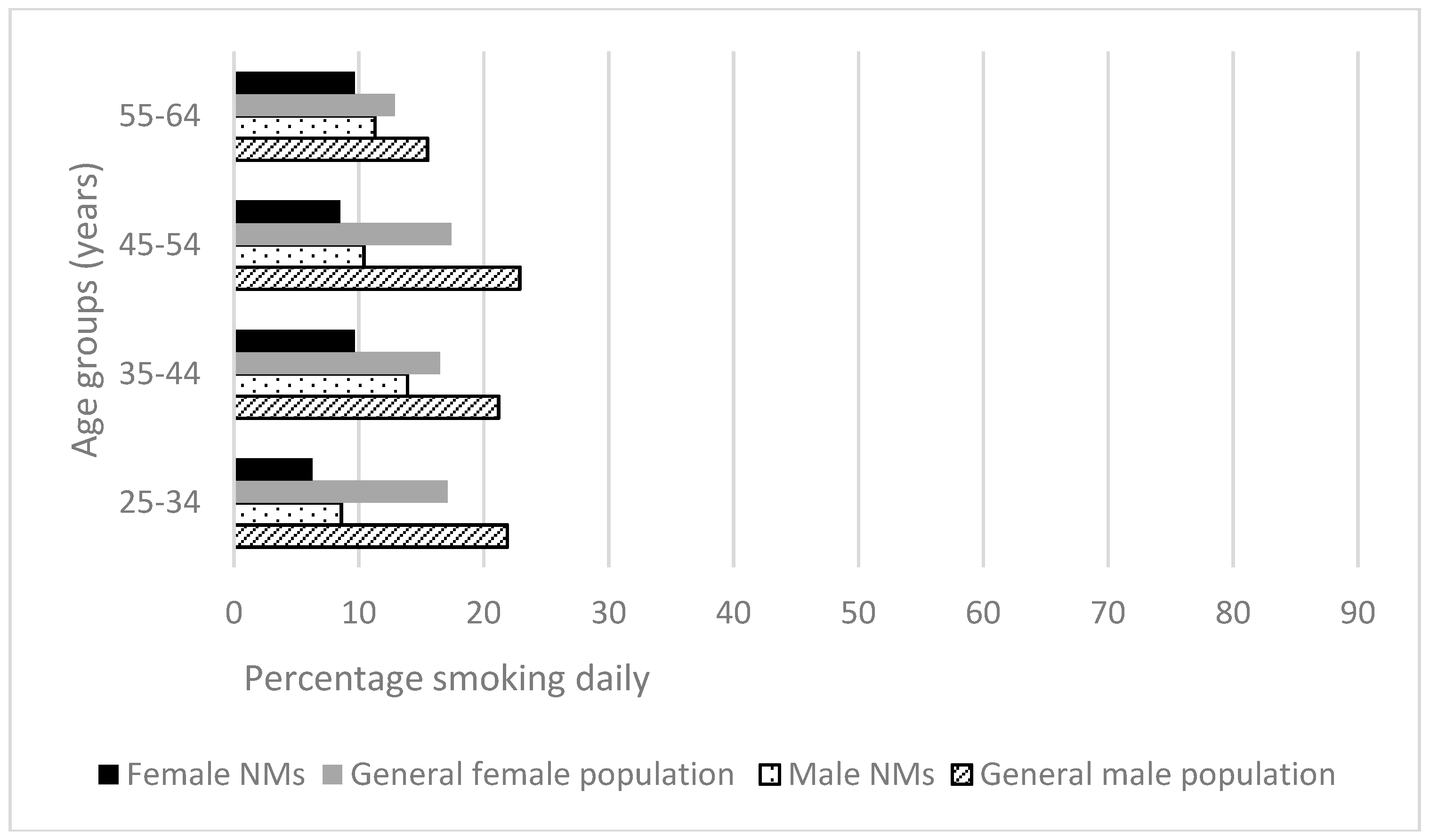
3.1.5. Smoking
3.2. Comparing Health-Related Behaviors of Nurses and the Australian General Population
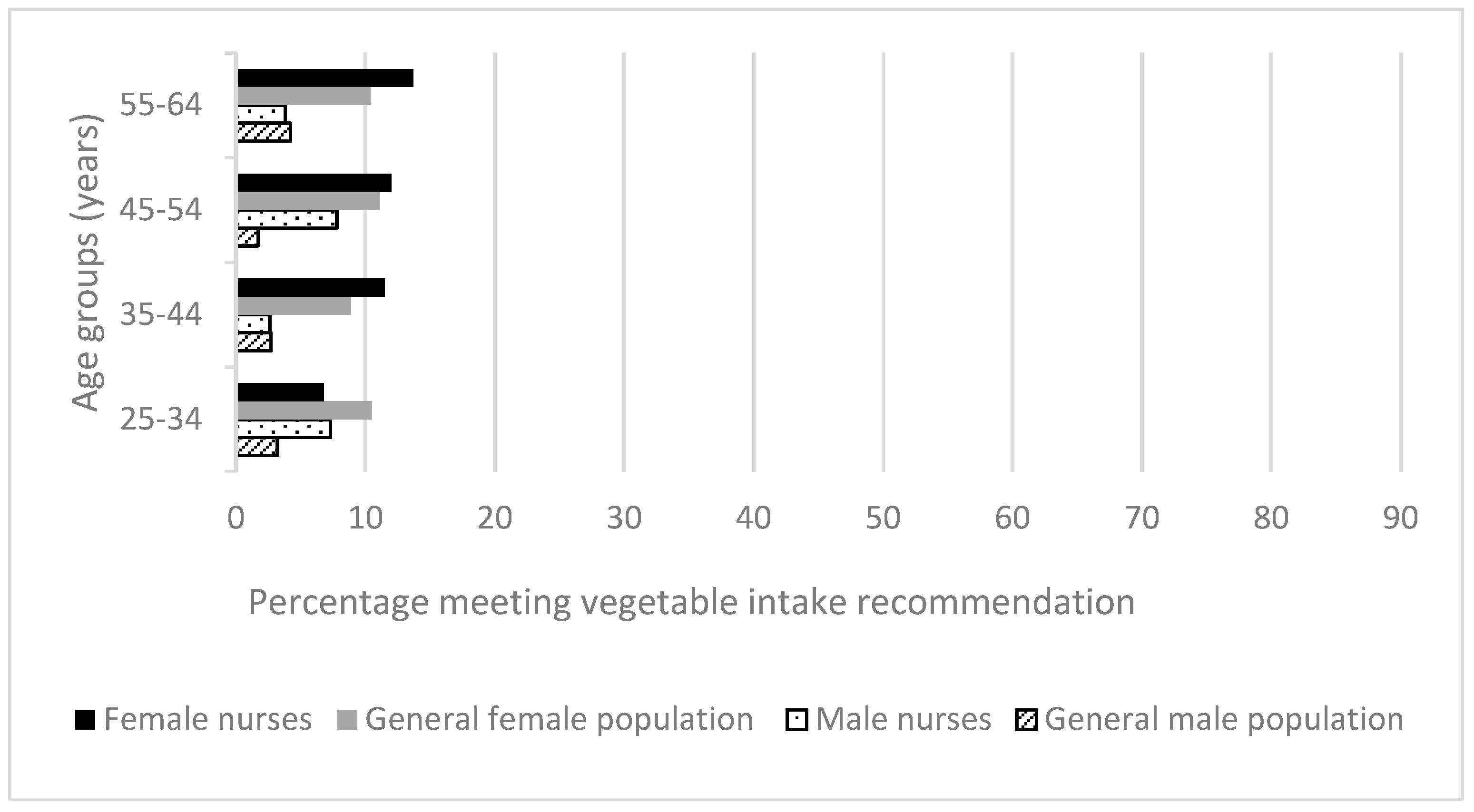
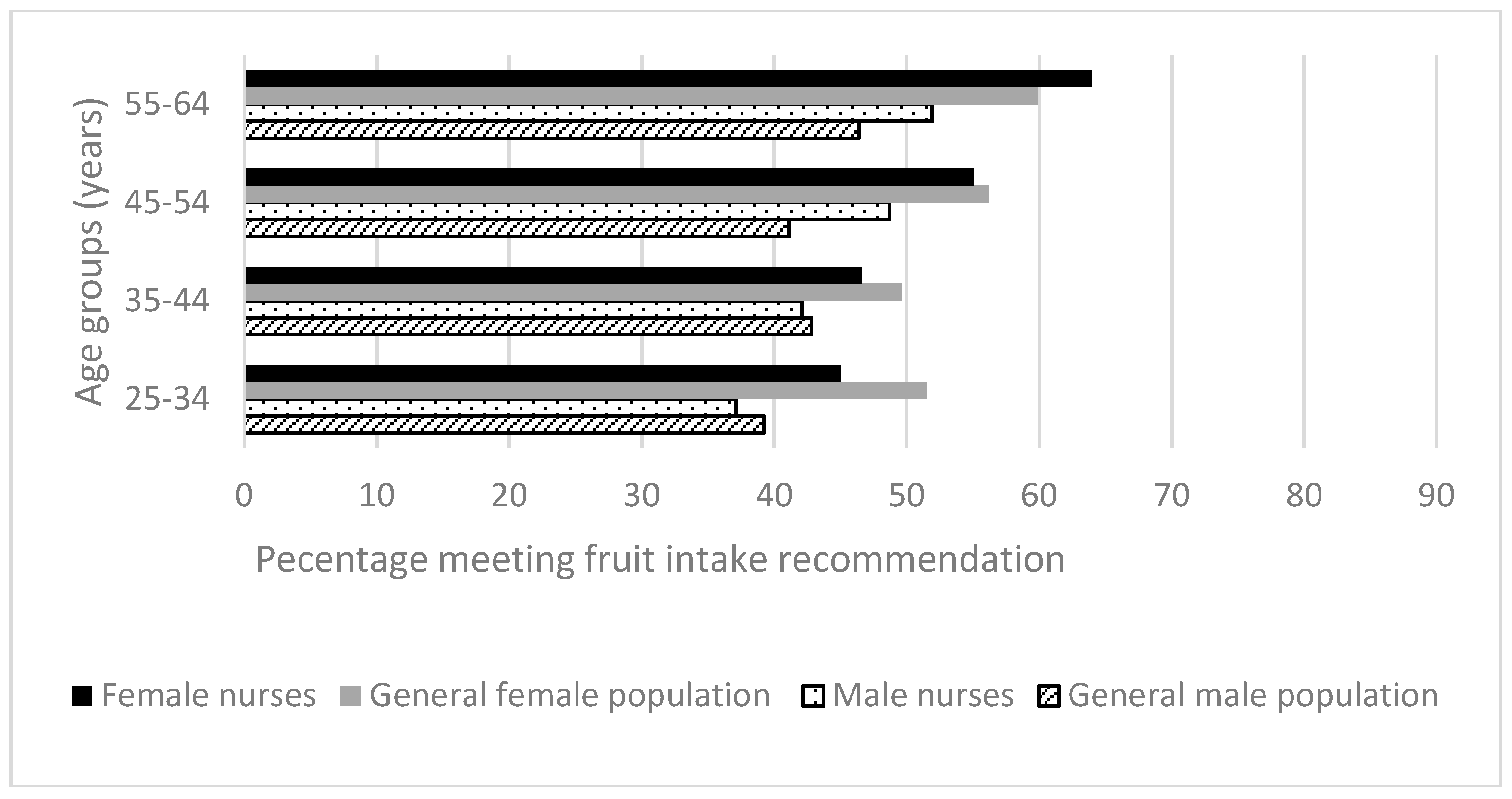
3.2.1. Diet
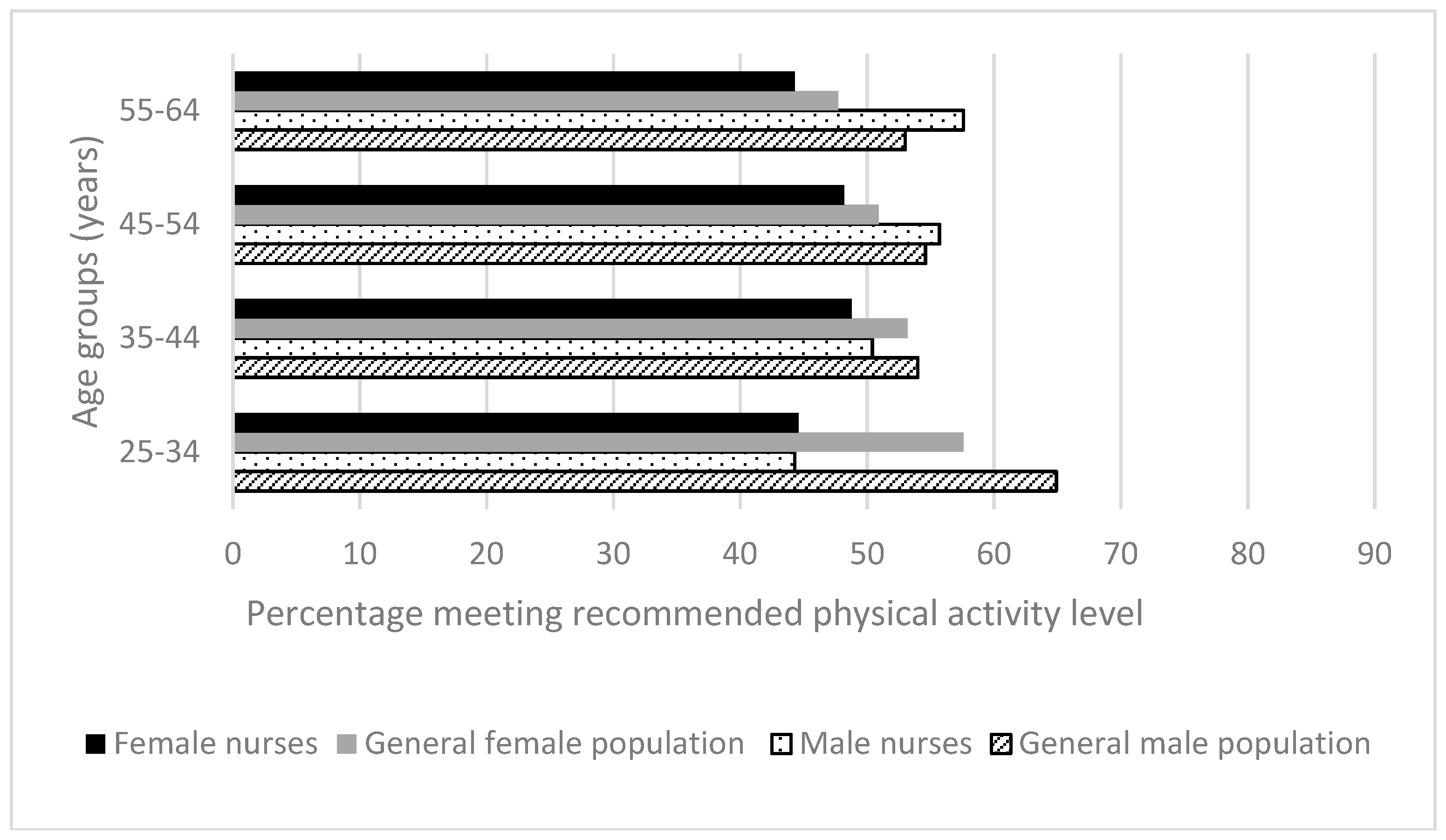
3.2.2. Physical Activity
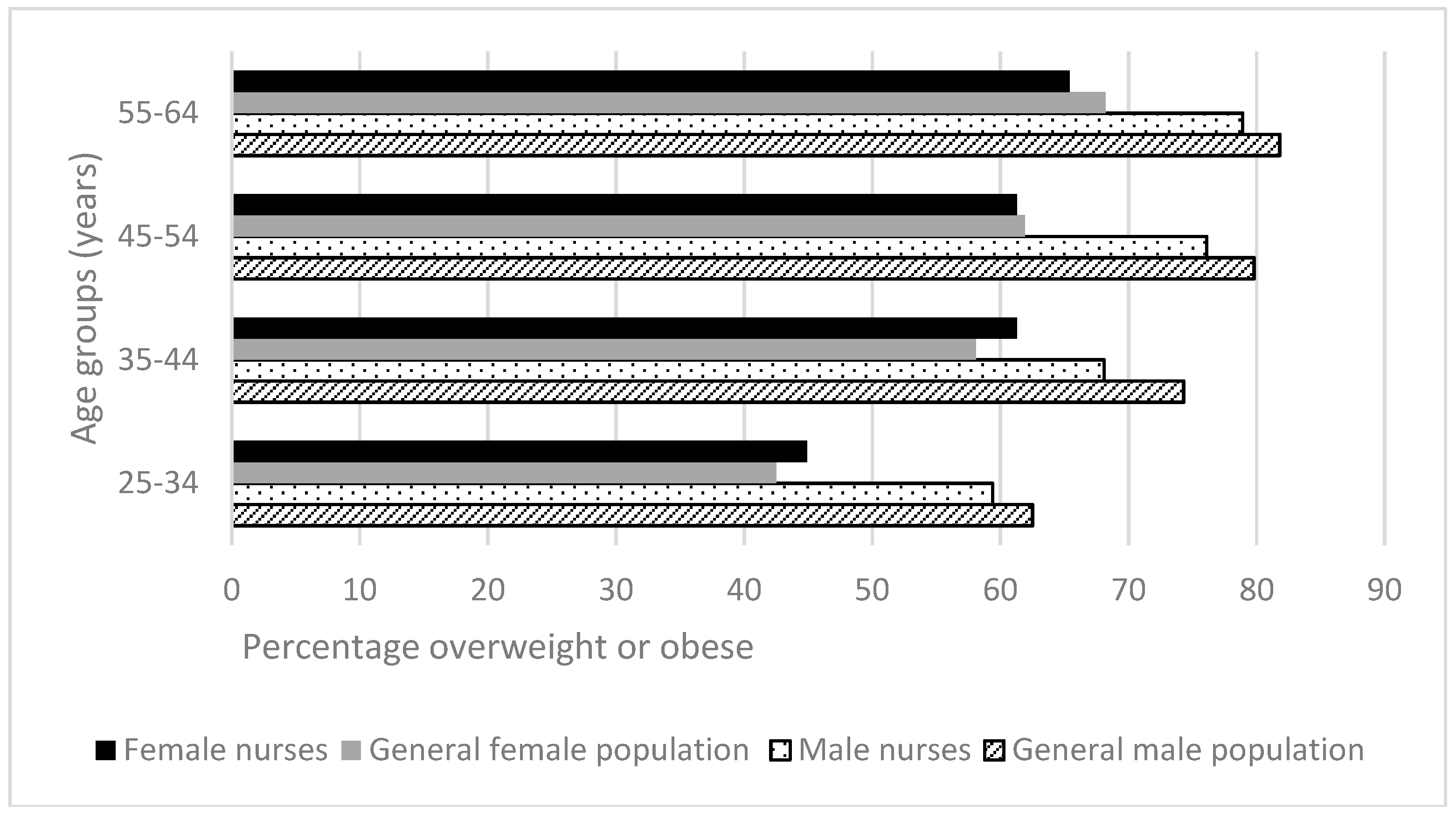
3.2.3. BMI and Waist Circumference
3.2.4. Risky Drinking
3.2.5. Daily Smoking
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- World Health Organisation. 10 Facts on Ageing and the Life Course; World Health Organisation: Geneva, Switzerland, 2013; Available online: http://www.who.int/features/factfiles/ageing/en/ (accessed on 11 December 2015).
- World Health Organisation. Ageing 2016; World Health Organisation: Geneva, Switzerland, 2016; Available online: http://www.who.int/topics/ageing/en/ (accessed on 2 January 2016).
- World Health Organisation. Global Burden of Disease; World Health Organisation: Geneva, Switzerland, 2015; Available online: http://www.who.int/healthinfo/global_burden_disease/GBD_report_2004update_full.pdf (accessed on 11 December 2015).
- Willcox, S. Chronic Diseases in Australia: The case for Changing Course; Melbourne Mitchell Institute for Health and Education Policy: Melbourne, Australia, 2014; Volume 65. [Google Scholar]
- McNab, J.; Schneider, C.H.; Leeder, S. Non-communicable diseases and implications for medical practice in Australia: A framework for analysis. Med. J. Aust. 2014, 201 (Suppl. S1), S29–S32. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. Chronic Diseases; Australian Institute of Health and Welfare: Canberra, Australia, 2016. Available online: http://www.aihw.gov.au/chronic-diseases/ (accessed on 20 September 2016).
- World Health Organization. Diet, Nutrition and the Prevention of Chronic Disease: Report of a Joint WHO/FAO Expert; World Health Organisation: Geneva, Switzerland, 2013; Available online: http://whqlibdoc.who.int/trs/who_trs_916.pdf (accessed on 2 December 2013).
- Xu, X.; Byles, J.E.; Shi, Z.; Hall, J.J. Evaluation of older Chinese people’s macronutrient intake status: Results from the China Health and Nutrition Survey. Br. J. Nutr. 2015, 113, 159–171. [Google Scholar] [CrossRef] [PubMed]
- Boeing, H.; Bechthold, A.; Bub, A.; Ellinger, S.; Haller, D.; Kroke, A.; Leschik-Bonnet, E.; Müller, M.J.; Oberritter, H.; Schulze, M.; et al. Critical review: Vegetables and fruit in the prevention of chronic diseases. Eur. J. Nutr. 2012, 51, 637–663. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. Risk Factors Contributing to Chronic Disease; Australian Institute of Health and Welfare: Canberra, Australia, 2016. Available online: http://www.aihw.gov.au/WorkArea/DownloadAsset.aspx?id=10737421546 (accessed on 10 October 2016).
- Shield, K.D.; Parry, C.; Rehm, J. Focus on: Chronic diseases and conditions related to alcohol use. Alcohol. Res. 2014, 35, 155–171. [Google Scholar]
- Cerhan, J.R.; Potter, J.D.; Gilmore, J.M.; Janney, C.A.; Kushi, L.H.; Lazovich, D.; Anderson, K.E.; Sellers, T.A.; Folsom, A.R. Adherence to the AICR cancer prevention recommendations and subsequent morbidity and mortality in the Iowa Women’s Health Study cohort. Cancer Epidemiol. Biomark. Prev. 2004, 13, 1114–1120. [Google Scholar]
- McCullough, M.L.; Patel, A.V.; Kushi, L.H.; Patel, R.; Willett, W.C.; Doyle, C.; Thun, M.J.; Gapstur, S.M. Following cancer prevention guidelines reduces risk of cancer, cardiovascular disease, and all-cause mortality. Cancer Epidemiol. Biomark. Prev. 2011, 20, 1089–1097. [Google Scholar] [CrossRef] [PubMed]
- Nursing and Midwifery Board of Australia. Revised Registration Standards and Standards for Practice Published Today; Nursing and Midwifery Board of Australia: Barton, Australian, 2016. Available online: http://www.nursingmidwiferyboard.gov.au/News/2016-02-01-revised-standards.aspx (accessed on 2 February 2017).
- Perry, L.; Gallagher, R.; Duffield, C.; Sibbritt, D.; Bichel-Findlay, J.; Nicholls, R. Does nurses’ health affect their intention to remain in their current position? J. Nurs. Manag. 2016, 24, 1088–1097. [Google Scholar] [CrossRef] [PubMed]
- Delaney, F.G. Nursing and health promotion: Conceptual concerns. J. Adv. Nurs. 1994, 20, 828–835. [Google Scholar] [CrossRef] [PubMed]
- Whitehead, D.; Wang, Y.; Wang, J.; Zhang, J.; Sun, Z.; Xie, C. Health promotion and health education practice: Nurses’ perceptions. J. Adv. Nurs. 2008, 61, 181–187. [Google Scholar] [CrossRef] [PubMed]
- International Council of Nursing. Delivering Quality, Serving Communitites: Nurses Leading Chronic Care; International Council of Nursing: Geneva, Switzerland, 2017; Available online: http://www.icn.ch/publications/2010-delivering-quality-serving-communities-nurses-leading-chronic-care/ (accessed on 10 January 2017).
- Kelly, M.; Wills, J.; Jester, R.; Speller, V. Should nurses be role models for healthy lifestyles? Results from a modified Delphi study. J. Adv. Nurs. 2016. [Google Scholar] [CrossRef] [PubMed]
- Nursing and Midwifery Council. Character and Health Decision-Making Guidance; Nursing and Midwifery Council: London, UK, 2017; Available online: https://www.nmc.org.uk/globalassets/sitedocuments/registration/character-and-health-decision-making-guidance.pdf (accessed on 10 January 2017).
- Perry, L.; Gallagher, R.; Duffield, C. The health and health behaviors of Australian metropolitan nurses: An exploratory study. BMC Nurs. 2015, 14, 45. [Google Scholar] [CrossRef] [PubMed]
- Perry, L.; Xu, X.; Duffield, C.; Gallagher, R.; Nicholls, R.; Sibbritt, D. Health, workforce characteristics, quality of life and intention to leave: The ‘Fit for the Future’ survey of Australian nurses and midwives. J. Adv. Nurs. 2017, 73, 2745–2756. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. Waist Circumference; Australian Bureau of Statistics: Canberra, Australia, 2013. Available online: http://www.abs.gov.au/ausstats/[email protected]/Lookup/4338.0main+features222011-13 (accessed on 12 October 2016).
- Australian Institute of Health and Welfare. National Drug Strategy Household Survey Detailed Report; Australian Institute of Health and Welfare: Canberra, Australia, 2016. Available online: http://www.aihw.gov.au/WorkArea/DownloadAsset.aspx?id=60129549848 (accessed on 12 December 2016).
- Australian Bureau of Statistics. National Health Survey: First Results, 2014–15; Australian Bureau of Statistics: Canberra, Australia, 2014. Available online: http://www.abs.gov.au/ausstats/[email protected]/Lookup/by%20Subject/4364.0.55.001~2014-15~Main%20Features~Waist%20circumference~23 (accessed on 12 November 2016).
- Australian Bureau of Statistics. Profiles of Health, Australia, 2011–13; Australian Bureau of Statistics: Canberra, Australia, 2011. Available online: http://www.abs.gov.au/ausstats/[email protected]/Lookup/by%20Subject/4338.0~2011-13~Main%20Features~Daily%20intake%20of%20fruit%20and%20vegetables~10009 (accessed on 12 November 2016).
- Australian Institute of Health and Welfare. Insufficient Physical Activity; Australian Institute of Health and Welfare: Canberra, Australia, 2016. Available online: http://www.aihw.gov.au/risk-factors/insufficient-physical-activity/ (accessed on 28 October 2016).
- Australian Bureau of Statistics. National Health Survey: First Results, 2014–15; Daily Intake of Fruit and Vegetables; Australian Bureau of Statistics: Canberra, Australia, 2016. Available online: http://www.abs.gov.au/ausstats/[email protected]/Lookup/by%20Subject/4364.0.55.001~2014-15~Main%20Features~Daily%20intake%20of%20fruit%20and%20vegetables~28 (accessed on 10 November 2016).
- Australian Bureau of Statistics. National Health Survey: First Results, 2014–15; Exercise; Australian Bureau of Statistics: Canberra, Australia, 2016. Available online: http://www.abs.gov.au/ausstats/[email protected]/Lookup/by%20Subject/4364.0.55.001~2014-15~Main%20Features~Exercise~29 (accessed on 28 October 2016).
- Australian Bureau of Statistics. National Health Survey: First Results, 2014–15; Somking; Australian Bureau of Statistics: Canberra, Australia, 2016. Available online: http://www.abs.gov.au/ausstats/[email protected]/Lookup/by%20Subject/4364.0.55.001~2014-15~Main%20Features~Smoking~24 (accessed on 12 December 2016).
- Greenhalgh, E.M.; Bayly, M.; Winstanley, M.H. Prevalence of Smoking—Adults; Cancer Council Victoria: Melbourne, Australia, 2016; Available online: http://www.tobaccoinaustralia.org.au/chapter-1-prevalence/1-3-prevalence-of-smoking-adults (accessed on 23 October 2016).
- Jepson, R.G.; Harris, F.M.; Platt, S.; Tannahill, C. The effectiveness of interventions to change six health behaviors: A review of reviews. BMC Public Health 2010, 10, 538. [Google Scholar] [CrossRef] [PubMed]
- Nicholls, R.; Perry, L.; Duffield, C.; Gallagher, R.; Pierce, H. Barriers and facilitators to healthy eating for nurses in the workplace: An integrative review. J. Adv. Nurs. 2017, 73, 1051–1065. [Google Scholar] [CrossRef] [PubMed]
- Perry, L.; Hoban, K.; Ryan, E. Food for thought: Nurses are what they eat? In Proceedings of the 4th Annual Worldwide Nursing Conference, Singapore, 18–19 July 2016. [Google Scholar]
- Greaves, C.J.; Sheppard, K.E.; Abraham, C.; Hardeman, W.; Roden, M.; Evans, P.H.; Schwarz, P.; IMAGE Study Group. Systematic review of reviews of intervention components associated with increased effectiveness in dietary and physical activity interventions. BMC Public Health 2011, 11, 119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ammerman, A.S.; Lindquist, C.H.; Lohr, K.N.; Hersey, J. The efficacy of behavioral interventions to modify dietary fat and fruit and vegetable intake: A review of the evidence. Prev. Med. 2002, 35, 25–41. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.W.; Perry, L. Lifestyle health promotion interventions for the nursing workforce: A systematic review. J. Clin. Nurs. 2012, 21, 2247–2261. [Google Scholar] [CrossRef] [PubMed]
- Kulie, T.; Slattengren, A.; Redmer, J.; Counts, H.; Eglash, A.; Schrager, S. Obesity and women’s health: An evidence-based review. J. Am. Board Fam. Med. 2011, 24, 75–85. [Google Scholar] [CrossRef] [PubMed]
- Bogossian, F.E.; Hepworth, J.; Leong, G.M.; Flaws, D.F.; Gibbons, K.S.; Benefer, C.A.; Turner, C.T. A cross-sectional analysis of patterns of obesity in a cohort of working nurses and midwives in Australia, New Zealand, and the United Kingdom. Int. J. Nurs. Stud. 2012, 49, 727–738. [Google Scholar] [CrossRef] [PubMed]
- Peplonska, B.; Bukowska, A.; Sobala, W. Rotating night shift work and physical activity of nurses and midwives in the cross-sectional study in Łódź, Poland. Chronobiol. Int. 2014, 31, 1152–1159. [Google Scholar] [CrossRef] [PubMed]
- Shaw, K.A.; Gennat, H.C.; O’Rourke, P.; Del Mar, C. Exercise for overweight or obesity. Cochrane Libr. 2006. [Google Scholar] [CrossRef] [PubMed]
- Orozco, L.J.; Buchleitner, A.M.; Gimenez-Perez, G.; Roqué I Figuls, M.; Richter, B.; Mauricio, D. Exercise or exercise and diet for preventing type 2 diabetes mellitus. Cochrane Libr. 2008. [Google Scholar] [CrossRef] [PubMed]
- Torquati, L.; Pavey, T.; Kolbe-Alexander, T.; Leveritt, M. Promoting Diet and Physical Activity in Nurses: A Systematic Review. Am. J. Health Promot. 2017, 31, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Berry, J.G.; Pidd, K.; Roche, A.M.; Harrison, J.E. Prevalence and patterns of alcohol use in the Australian workforce: Findings from the 2001 National Drug Strategy Household Survey. Addiction 2007, 102, 1399–1410. [Google Scholar] [CrossRef] [PubMed]
- Pidd, K.; Shtangey, V.; Roche, A.M. Alcohol Use in the Australian Workforce: Prevalence, Patterns, & Implications: Findings from a Secondary Analysis of 2004 NDSHS Data; NCETA: Adelaide, Australia, 2008. [Google Scholar]
- Government of South Australia. Alcohol and Other Drug Use among Nurses—Guideline for Respone in the Workplace; Government of South Australia: Adelaide, Australia, 2016. Available online: https://www.sahealth.sa.gov.au/wps/wcm/connect/379beb80417bae35ad91ef67a94f09f9/Alcohol+and+Other+Drug+Use+Among+Nurses+-+Guidelines+2001-DASSA-Oct2013.pdf?MOD=AJPERES&CACHEID=379beb80417bae35ad91ef67a94f09f9 (accessed on 12 November 2016).
- Sheard, M.; Huntington, A.; Gilmour, J. A study of alcohol consumption in a cohort of military nurses. J. Mil. Veterans Health 2014, 22, 25–33. [Google Scholar]
- Schluter, P.J.; Turner, C.; Benefer, C. Long working hours and alcohol risk among Australian and New Zealand nurses and midwives: A cross-sectional study. Int. J. Nurs. Stud. 2012, 49, 701–709. [Google Scholar] [CrossRef] [PubMed]
- Virtanen, M.; Jokela, M.; Nyberg, S.T.; Madsen, I.E.; Lallukka, T.; Ahola, K.; Alfredsson, L.; Batty, G.D.; Bjorner, J.B.; Borritz, M.; et al. Long working hours and alcohol use: Systematic review and meta-analysis of published studies and unpublished individual participant data. Br. Med. J. 2015, 350, g7772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayo Clinic. Job Burnout: How to Spot It and Take Action; Mayo Clinic: Rochester, MN, USA, 2016; Available online: http://www.mayoclinic.org/healthy-lifestyle/adult-health/in-depth/burnout/art-20046642 (accessed on 14 August 2016).
- Ferris, J.A.; Laslett, A.-M.; Livingston, M.; Room, R.; Wilkinson, C. The impacts of others’ drinking on mental health. Med. J. Aust. 2011, 195, S22. [Google Scholar] [PubMed]
- Nicholls, R.; Perry, L.; Gallagher, R.; Duffield, C. Building expert agreement on appropriate workplace health promotion interventions for nurses and midwives: A modified national Delphi consultation. J. Adv. Nurs. 2017, 73, 2587–2599. [Google Scholar]
- Australian Institute of Health and Welfare. Leading Types of Ill Health; Australian Institute of Health and Welfare: Canberra, Australia, 2016. Available online: http://www.aihw.gov.au/australias-health/2014/ill-health/#t2 (accessed on 10 October 2016).
- Australain Institute of Health and Welfare. Cardiovascular Disease 2016 Data Tables; Australian Institute of Health and Welfare: Canberra, Australia, 2016. Available online: http://www.aihw.gov.au/chronic-diseases/data/#cardio (accessed on 1 March 2017).
- DeCola, P.; Benton, D.; Peterson, C.; Matebeni, D. Nurses’ potential to lead in non-communicable disease global crisis. Int. Nurs. Rev. 2012, 59, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Miller, S.K.; Alpert, P.T.; Cross, C.L. Overweight and obesity in nurses, advanced practice nurses, and nurse educators. J. Am. Acad. Nurse Pract. 2008, 20, 259–265. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | N | % |
|---|---|---|
| Age groups | ||
| 18–24 | 143 | 3.2 |
| 25–34 | 577 | 12.9 |
| 35–44 | 808 | 18.1 |
| 45–54 | 1400 | 31.4 |
| 55–64 | 1382 | 31.0 |
| 65 years and above | 152 | 3.4 |
| Gender | ||
| Males | 4421 | 90.6 |
| Females | 458 | 9.4 |
| Education level | ||
| Certificate/diploma | 1245 | 27.8 |
| Bachelor and above | 3227 | 72.2 |
| Work location | ||
| Metropolitan areas | 3313 | 66.5 |
| Inner regional areas | 1354 | 27.2 |
| Outer regional and beyond | 314 | 6.3 |
| Work role | ||
| Foundational | 3560 | 71.7 |
| Advanced practice | 380 | 7.7 |
| Domain-specific (manager, educator, researcher, etc.) | 773 | 15.6 |
| Work setting | ||
| Hospital | 3005 | 59.6 |
| Aged care/rehabilitation or disability | 686 | 13.6 |
| Community centre/general practice/outpatients | 896 | 17.8 |
| Others | 454 | 9.0 |
| Working hours | ||
| <40 | 2990 | 60.2 |
| ≥40 | 1975 | 39.8 |
| Odds Ratio (95% CI) | p Value | |
| Age Groups (years) | Vegetable Intake | |
| 25–34 | 1 | |
| 35–44 | 1.55 (1.04; 2.31) | 0.03 |
| 45–54 | 1.79 (1.25; 2.58) | 0.002 |
| 55–64 | 2.03 (1.41; 2.91) | <0.001 |
| Gender | ||
| Female | 1 | |
| Male | 0.42 (0.26; 0.64) | <0.001 |
| Age Groups (years) | Fruit Intake | |
| 25–34 | 1 | |
| 35–44 | 1.08 (0.87; 1.34) | 0.46 |
| 45–54 | 1.52 (1.25; 1.85) | <0.001 |
| 55–64 | 2.18 (1.79; 2.65) | <0.001 |
| Gender | ||
| Female | 1 | |
| Male | 0.68 (0.56; 0.84) | <0.001 |
| Age Groups (years) | Physical Activity Level | |
| 25–34 | 1 | |
| 35–44 | 1.20 (0.97; 1.49) | 0.09 |
| 45–54 | 1.19 (0.98; 1.44) | 0.09 |
| 55–64 | 1.03 (0.85; 1.26) | 0.75 |
| Gender | ||
| Female | 1 | |
| Male | 1.28 (1.05; 1.58) | <0.02 |
| Age Groups (years) | Risky Drinking | |
| 25–34 | 1 | |
| 35–44 | 0.76 (0.59; 0.99) | 0.04 |
| 45–54 | 0.71 (0.56; 0.90) | 0.004 |
| 55–64 | 0.54 (0.43; 0.69) | <0.001 |
| Gender | ||
| Female | 1 | |
| Male | 2.03 (1.61; 2.56) | <0.001 |
| Age Groups (years) | Daily Smoking | |
| 25–34 | 1 | |
| 35–44 | 1.62 (1.09; 2.42) | 0.02 |
| 45–54 | 1.34 (0.92; 1.96) | 0.13 |
| 55–64 | 1.54 (1.06; 2.23) | 0.03 |
| Gender | ||
| Female | 1 | |
| Male | 1.32 (0.95; 1.83) | 0.09 |
| Age Groups (years) | BMI | |
| 25–34 | 1 | |
| 35–44 | 1.88 (1.50; 2.35) | <0.001 |
| 45–54 | 1.91 (1.55; 2.33) | <0.001 |
| 55–64 | 2.25 (1.83; 2.76) | <0.001 |
| Gender | ||
| Female | 1 | |
| Male | 1.64 (1.31; 2.06) | <0.001 |
| Age Groups (years) | Waist Circumference | |
| 25–34 | 1 | |
| 35–44 | 1.59 (1.23; 2.07) | <0.001 |
| 45–54 | 2.04 (1.61; 2.59) | <0.001 |
| 55–64 | 2.68 (2.10; 3.40) | <0.001 |
| Gender | ||
| Female | 1 | |
| Male | 0.31 (0.25; 0.39) | <0.001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perry, L.; Xu, X.; Gallagher, R.; Nicholls, R.; Sibbritt, D.; Duffield, C. Lifestyle Health Behaviors of Nurses and Midwives: The ‘Fit for the Future’ Study. Int. J. Environ. Res. Public Health 2018, 15, 945. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15050945
Perry L, Xu X, Gallagher R, Nicholls R, Sibbritt D, Duffield C. Lifestyle Health Behaviors of Nurses and Midwives: The ‘Fit for the Future’ Study. International Journal of Environmental Research and Public Health. 2018; 15(5):945. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15050945
Chicago/Turabian StylePerry, Lin, Xiaoyue Xu, Robyn Gallagher, Rachel Nicholls, David Sibbritt, and Christine Duffield. 2018. "Lifestyle Health Behaviors of Nurses and Midwives: The ‘Fit for the Future’ Study" International Journal of Environmental Research and Public Health 15, no. 5: 945. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15050945