2.1. Data Source and Sampling
The data used for this study come from the China Family Panel Studies (CFPS) for the years 2010 and 2014. The CFPS is a nationally representative, longitudinal social survey that was launched in 2010 and is conducted biennially by the Institute of Social Science Survey (ISSS) at Peking University, China. The survey design is based on the Panel Survey of Income Dynamics (PSID), the National Longitudinal Surveys of Youth (NLSY), and the Health and Retirement Study (HRS) in the United States. It focuses on a range of topics related to education outcomes, economics activities, migration, health, and family dynamics. The survey collects data at three levels: the individual-, family-, and community-levels.
The CFPS surveyed respondents in sampling units in 25 provinces (all provinces except Xinjiang, Tibet, Qinghai, Inner Mongolia, Ningxia, and Hainan), a sampling frame which represents 95% of the Chinese population. To generate nationally and provincially representative sample, the CFPS adopted a “Probability-Proportional-to-Size” (PPS) sampling strategy with multi-stage stratification and carried out a three-stage sampling process. The first stage was the Primary Sampling Unit, in which county-level units were randomly selected. In the second stage, village-level units (villages in rural areas and neighborhoods/communities in urban areas) were selected. In the third stage, households from the village-level units were selected according to the study’s systematic sampling protocol. All members of each household were interviewed, except those who were not at home at the time of the survey.
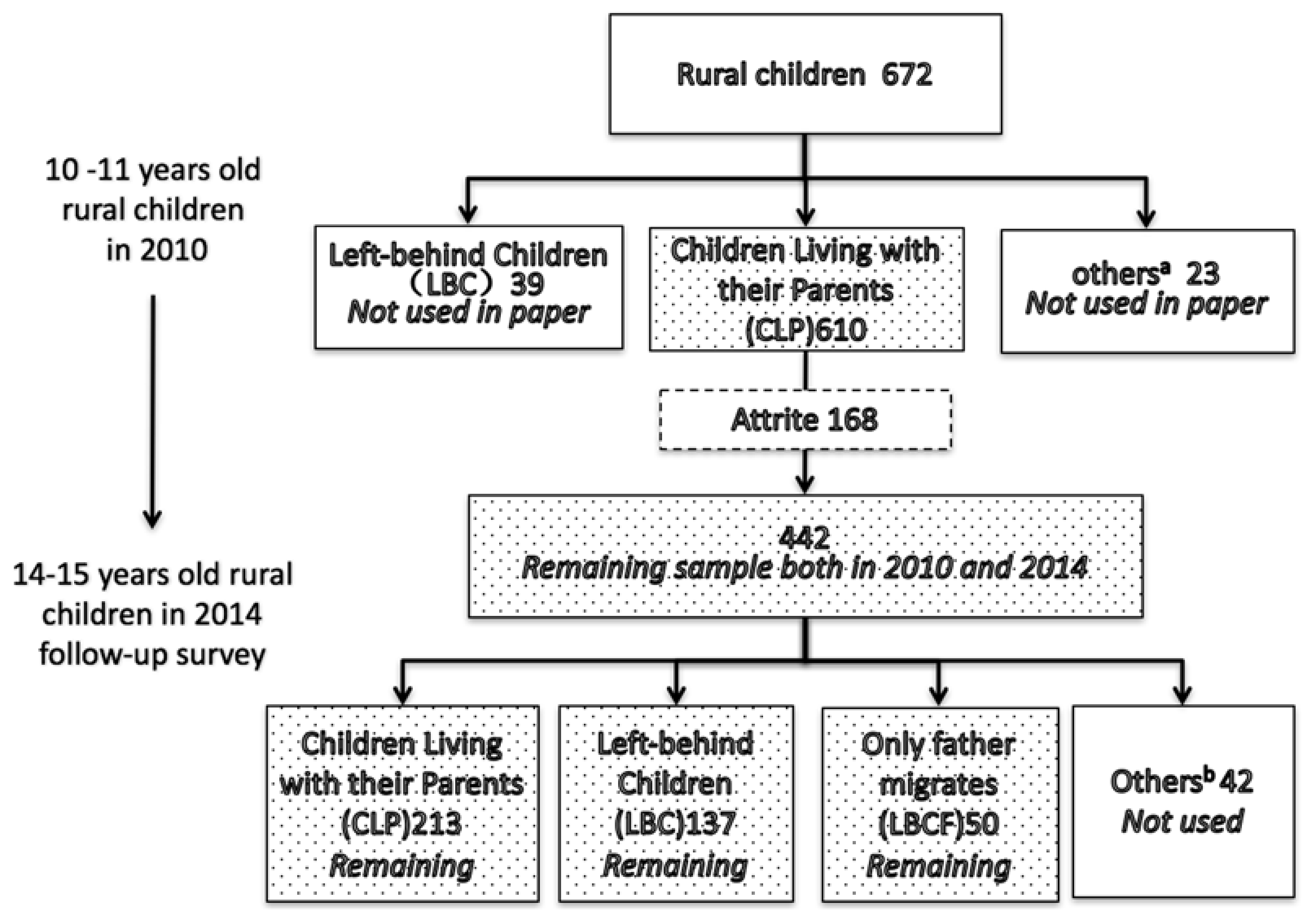
Following an initial baseline survey wave in 2010, ISSS conducted two follow-up surveys in 2012 and 2014. For the purposes of the survey, we examine the case of children who were 10 and 11-year-old at the time of the 2010 survey and 14 and 15-year-old, respectively, at the time of the 2014 survey. We limit our sample to children between the ages of 10 and 15 because children between these ages responded to the child questionnaire and were of the age to respond to the survey independently. In this study, we use the CFPS data from 2010 and 2014 to create a panel dataset that includes 442 children for both years, after excluding observations with missing information (
Figure 1). Because the 2010 and 2014 CFPS data both include the same depression scale (CES-D), this panel allows us to examine the depressive symptoms outcomes of children over these two periods. For the sake of our analysis, we exclude an additional 42 children whose parental migration status did not fit into one of our sample classifications. In the end, our sample is comprised of 400 children (we have added a balance test to identify whether there are systematic differences between the 168 children who dropped out and the 442 who remained in the sample. Just as
Appendix Table A3 shows, we generally did not find systematic differences between these two groups).
We also created three “types” of rural children: left-behind children (LBC), who have rural hukous and had resided in rural areas while both of their parents work and live outside of the household for at least 5 months out of the previous year; father-only migration children (LBCF), who have rural hukous and had resided in rural areas with their mother while only their father works and lives outside of the household for at least 5 months out of the previous year (only a small portion of our sample were “mother-only migration children” (2.84% of the sample), and for this reason we do not evaluate this group of children); and children living with both parents (CLP) in their rural communities.
Figure 1 shows that, among the 400 children in our sample who were living with their parents in 2010, at the time of the 2014 CFPS survey 213 children living with both parents, and are classified as
children living with parents (CLPs); 137 were living with neither parent, and are classified as
left-behind children (LBCs); and 50 were living with only their mother, and are classified as
father-only migrates children (LBCFs) (for our analysis, we exclude children from households where only the mother migrated (
n = 15) or with any other type of household migration status (
n = 27, total) due to their small sample size).
2.2. Measures
The depression scale used for the 2010 and 2014 CFPS data is the Center for Epidemiologic Studies Depression Scale (CES-D). This scale was developed by Radloff [
16] and has been used widely in the international literature [
17,
18]. The CES-D includes 20 items that are designed to evaluate four aspects of depression (somatic symptoms, depressed affect, positive affect, and interpersonal problems). If more than four responses are missing from a single observation, then it was dismissed. Due to changes in the scale between the time of the 2010 and 2014 CFPS surveys, some items in the CES-D scale did not match up between the two years. Specifically, six of the items in the scale matched between the two years, so we evaluate changes in depression status on these six items and dismiss the other 14 (see
Appendix Table A1). Due to the small group of value 1, we replace value 1 to 2, and then use 5 minus the score of each question to get the adjusted score, which range from 0 to 3. The higher score means the more severe of depressive symptoms.
2.3. Descriptive Analysis
As can be seen in
Table 1, 52.49% of children in our sample are male (row 3, column 2) and 11.76% are non-Han cultural minorities (row 7, column 2). In terms of the age distribution, 50.23% of respondents were 11 years old at the time of the 2010 CFPS survey, and 15 years old at the time of the 2014 CFPS survey (row 10, column 2). In 2010, the fraction of students that boarded at school was 12.67% (row 15, column 2), and this proportion increased to 53.17% by 2014 (row 15, column 5). We also found that the self-report health status of children worsened over our study period, as the share of children that reported “excellent” health fell from 75.34% in 2010 (row 17, column 2) down to 28.51% in 2014 (row 17, column 5).
In terms of individual-level characteristics, we find that there are significant differences between LBCs and CLPs in terms of school boarding status, household income, and self-reported health status in 2014 (
Table 2). Specifically, LBCs are more likely to board at school than CLPs, significant at the 5% level (Row 4, Column 4); LBCs have average household per capita incomes 301.73 yuan higher than CLPs, significant at the 1% level (Row 5, Column 4); and LBCs have measures of self-reported health 0.19 higher than CLPs, significant at the 5% level (Row 6, Column 4).
When examining the change in depression scores of our sample of 442 children, we find that the average depression score increases from 3.54 in 2010 (
Table 1, Row 1, Column 3) to 6.98 in 2014 (Row 1, Column 6) significantly at 1% level. To examine whether changes in parental migration status may have contributed to this increase in average depression scores, we compare the depression scores of CLPs to those of LBCs/LBCFs in 2010 and 2014 (
Figure 2).
We find that there is both insignificant difference between CLPs and LBCs in 2010, and between CLPs and LBCFs in 2010. However, there is a significant difference (at the 5% level) between CLPs and LBCs in 2014, but there is no significant difference between CLPs and LBCFs in the same year.

 ,
, 
{kind=link}
{kind=link}
{kind=link}


