Which Patients Are Prescribed Escitalopram?: Predictors for Escitalopram Prescriptions and Functional Outcomes among Patients with Acute Ischemic Stroke


Abstract
:1. Introduction
2. Materials and Methods
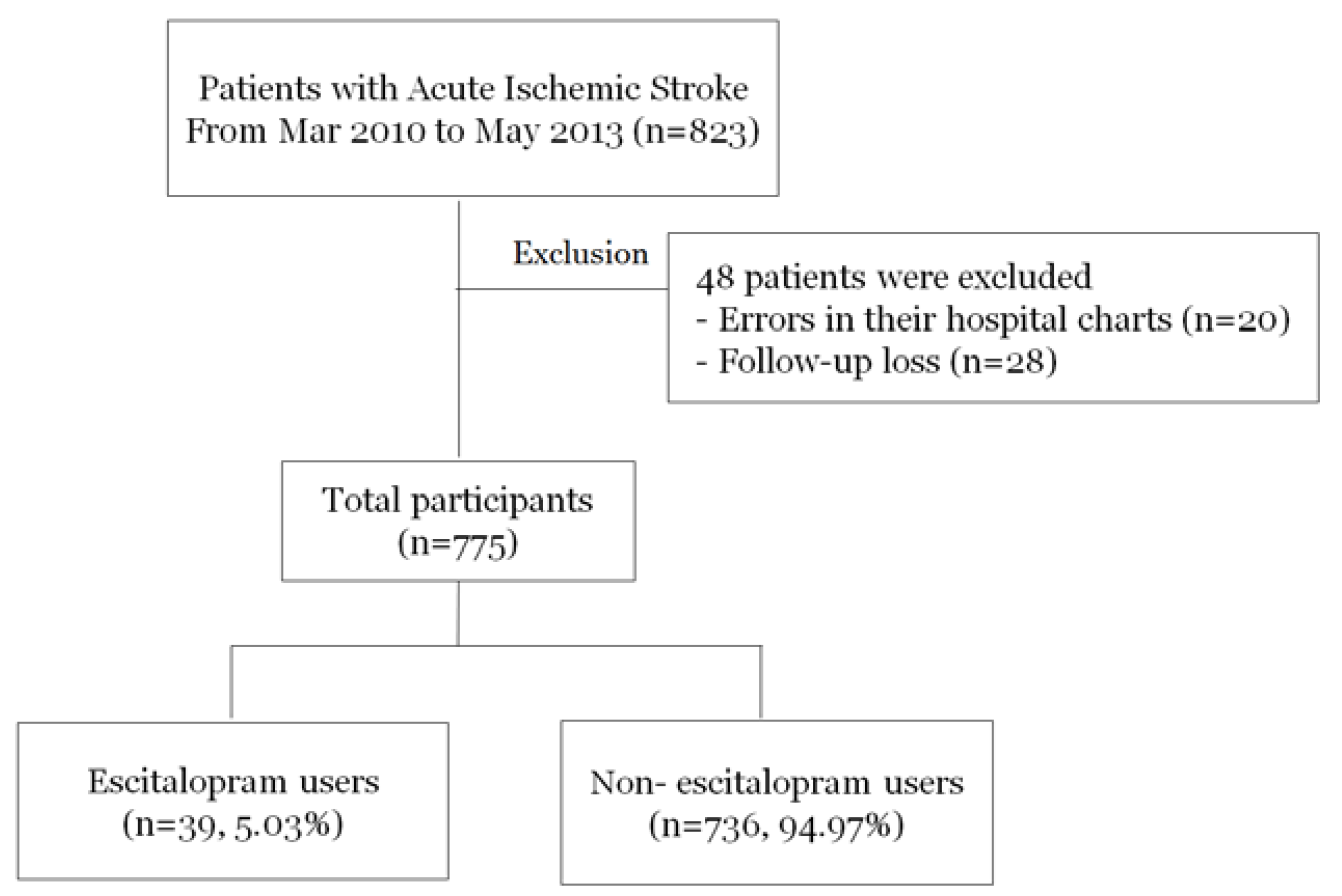
2.1. Study Population
2.2. Clinical Information
2.3. Statistical Analyses
3. Results
3.1. Analysis I: Predictors for Escitalopram Prescriptions
3.2. Analysis II: Escitalopram Prescriptions and Short-Term Functional Outcomes
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- OECD Indicators. Health at a Glance 2015. Available online: http://www.oecd.org/health/health-systems/health-at-a-glance-19991312.htm (accessed on 17 May 2018).
- Lim, G.Y.; Tam, W.W.; Lu, Y.; Ho, C.S.; Zhang, M.W.; Ho, R.C. Prevalence of depression in the community from 30 countries between 1994 and 2014. Sci. Rep. 2018, 8, 2861. [Google Scholar] [CrossRef] [PubMed]
- Alhazzani, A.A.; Mahfouz, A.A.; Abolyazid, A.Y.; Awadalla, N.J.; Aftab, R.; Faraheen, A.; Khalil, S.N. Study of stroke incidence in the aseer region, Southwestern Saudi Arabia. Int. J. Environ. Res. Public Health 2018, 15, 215. [Google Scholar] [CrossRef] [PubMed]
- Ho, R.C.; Ho, E.C.; Tai, B.C.; Ng, W.Y.; Chia, B.H. Elderly suicide with and without a history of suicidal behavior: Implications for suicide prevention and management. Arch. Suicide Res. Off. J. Int. Acad. Suicide Res. 2014, 18, 363–375. [Google Scholar] [CrossRef] [PubMed]
- Sharma, V.K.; Yeo, L.L.; Ho, R.C.; Rathakrishnan, R. Severe transient suicidality due to hemispheric hyperperfusion after successful acute stroke thrombolysis. J. Neuropsychiatry Clin. Neurosci. 2013, 25, E33–E34. [Google Scholar] [CrossRef] [PubMed]
- Chollet, F.; Acket, B.; Raposo, N.; Albucher, J.F.; Loubinoux, I.; Pariente, J. Use of antidepressant medications to improve outcomes after stroke. Curr. Neurol. Neurosci. Rep. 2013, 13, 318. [Google Scholar] [CrossRef] [PubMed]
- Dam, M.; Tonin, P.; De Boni, A.; Pizzolato, G.; Casson, S.; Ermani, M.; Freo, U.; Piron, L.; Battistin, L. Effects of fluoxetine and maprotiline on functional recovery in poststroke hemiplegic patients undergoing rehabilitation therapy. Stroke 1996, 27, 1211–1214. [Google Scholar] [CrossRef] [PubMed]
- Mak, K.K.; Kong, W.Y.; Mak, A.; Sharma, V.K.; Ho, R.C. Polymorphisms of the serotonin transporter gene and post-stroke depression: A meta-analysis. J. Neurol. Neurosur. Psychiatry 2013, 84, 322–328. [Google Scholar] [CrossRef] [PubMed]
- Zi, W.J.; Shuai, J. Cortisol as a prognostic marker of short-term outcome in Chinese patients with acute ischemic stroke. PLoS ONE 2013, 8, e72758. [Google Scholar] [CrossRef] [PubMed]
- Wijaya, C.S.; Lee, J.J.Z.; Husain, S.F.; Ho, C.S.H.; McIntyre, R.S.; Tam, W.W.; Ho, R.C.M. Differentiating medicated patients suffering from major depressive disorder from healthy controls by spot urine measurement of monoamines and steroid hormones. Int. J. Environ. Res. Public Health 2018, 15, e15050865. [Google Scholar] [CrossRef] [PubMed]
- Geng, H.H.; Wang, X.W.; Fu, R.L.; Jing, M.J.; Huang, L.L.; Zhang, Q.; Wang, X.X.; Wang, P.X. The relationship between c-reactive protein level and discharge outcome in patients with acute ischemic stroke. Int. J. Environ. Res. Public Health 2016, 13, 636. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Ho, C.S.; Liu, X.; Chua, A.N.; Wang, W.; McIntyre, R.S.; Ho, R.C. Chronic administration of fluoxetine and pro-inflammatory cytokine change in a rat model of depression. PLoS ONE 2017, 12, e0186700. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Yang, F.; Shi, H.; Yang, C.; Hu, H. What type of transitional care effectively reduced mortality and improved adl of stroke patients? A meta-analysis. Int. J. Environ. Res. Public Health 2017, 14, 510. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.M.; Stewart, R.; Kang, H.J.; Bae, K.Y.; Kim, S.W.; Shin, I.S.; Kim, J.T.; Park, M.S.; Cho, K.H.; Yoon, J.S. A prospective study of statin use and poststroke depression. J. Clin. Psychopharmacol. 2014, 34, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Puri, B.K.; Ho, R.; Hall, A. Revision Notes in Psychiatry; CRC Press: New York, NY, USA, 2014. [Google Scholar]
- Rosner, B. Fundamentals of Biostatistics, 7th ed.; Brooks/Cole: Boston, MA, USA, 2011. [Google Scholar]
- Chollet, F.; Tardy, J.; Albucher, J.F.; Thalamas, C.; Berard, E.; Lamy, C.; Bejot, Y.; Deltour, S.; Jaillard, A.; Niclot, P.; et al. Fluoxetine for motor recovery after acute ischaemic stroke (flame): A randomised placebo-controlled trial. Lancet. Neurol. 2011, 10, 123–130. [Google Scholar] [CrossRef]
- Bae, K.Y.; Kim, S.W.; Kim, J.M.; Shin, I.S.; Yoon, J.S.; Jung, S.W.; Lee, M.S.; Yim, H.W.; Jun, T.Y. Antidepressant prescribing patterns in Korea: Results from the clinical research center for depression study. Psychiatry Investig. 2011, 8, 234–244. [Google Scholar] [CrossRef] [PubMed]
- Wahlgren, N.; Ahmed, N.; Davalos, A.; Ford, G.A.; Grond, M.; Hacke, W.; Hennerici, M.G.; Kaste, M.; Kuelkens, S.; Larrue, V.; et al. Thrombolysis with alteplase for acute ischaemic stroke in the safe implementation of thrombolysis in stroke-monitoring study (sits-most): An observational study. Lancet 2007, 369, 275–282. [Google Scholar] [CrossRef]
- Yoo, H.S.; Kim, Y.D.; Lee, H.S.; Song, D.; Song, T.J.; Kim, B.M.; Kim, D.J.; Kim, D.I.; Heo, J.H.; Nam, H.S. Repeated thrombolytic therapy in patients with recurrent acute ischemic stroke. J. Stroke 2013, 15, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Morris, P.L.; Robinson, R.G.; Andrzejewski, P.; Samuels, J.; Price, T.R. Association of depression with 10-year poststroke mortality. Am. J. Psychiatry 1993, 150, 124–129. [Google Scholar] [PubMed]
- Ellis, C.; Zhao, Y.; Egede, L.E. Depression and increased risk of death in adults with stroke. J. Psychosom. Res. 2010, 68, 545–551. [Google Scholar] [CrossRef] [PubMed]
- Hackett, M.L.; Yapa, C.; Parag, V.; Anderson, C.S. Frequency of depression after stroke: A systematic review of observational studies. Stroke 2005, 36, 1330–1340. [Google Scholar] [CrossRef] [PubMed]
- Drevets, W.C.; Price, J.L.; Furey, M.L. Brain structural and functional abnormalities in mood disorders: Implications for neurocircuitry models of depression. Brain Struct. Funct. 2008, 213, 93–118. [Google Scholar] [CrossRef] [PubMed]
- Raichle, M.E.; MacLeod, A.M.; Snyder, A.Z.; Powers, W.J.; Gusnard, D.A.; Shulman, G.L. A default mode of brain function. Proc. Natl. Acad. Sci. USA 2001, 98, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Sheline, Y.I.; Barch, D.M.; Price, J.L.; Rundle, M.M.; Vaishnavi, S.N.; Snyder, A.Z.; Mintun, M.A.; Wang, S.; Coalson, R.S.; Raichle, M.E. The default mode network and self-referential processes in depression. Proc. Natl. Acad. Sci. USA 2009, 106, 1942–1947. [Google Scholar] [CrossRef] [PubMed]
- Windle, V.; Corbett, D. Fluoxetine and recovery of motor function after focal ischemia in rats. Brain Res. 2005, 1044, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Lim, C.M.; Kim, S.W.; Park, J.Y.; Kim, C.; Yoon, S.H.; Lee, J.K. Fluoxetine affords robust neuroprotection in the postischemic brain via its anti-inflammatory effect. J. Neurosci. Res. 2009, 87, 1037–1045. [Google Scholar] [CrossRef] [PubMed]
- Acler, M.; Robol, E.; Fiaschi, A.; Manganotti, P. A double blind placebo rct to investigate the effects of serotonergic modulation on brain excitability and motor recovery in stroke patients. J. Neurol. 2009, 256, 1152–1158. [Google Scholar] [CrossRef] [PubMed]
- El Husseini, N.; Goldstein, L.B.; Peterson, E.D.; Zhao, X.; Pan, W.; Olson, D.M.; Zimmer, L.O.; Williams, J.W., Jr.; Bushnell, C.; Laskowitz, D.T. Depression and antidepressant use after stroke and transient ischemic attack. Stroke 2012, 43, 1609–1616. [Google Scholar] [CrossRef] [PubMed]
- Teasell, R. Challenges in the implementation of evidence in stroke rehabilitation. Top. Stroke Rehabil. 2012, 19, 93–95. [Google Scholar] [CrossRef] [PubMed]
- Cipriani, A.; Furukawa, T.A.; Salanti, G.; Geddes, J.R.; Higgins, J.P.; Churchill, R.; Watanabe, N.; Nakagawa, A.; Omori, I.M.; McGuire, H.; et al. Comparative efficacy and acceptability of 12 new-generation antidepressants: A multiple-treatments meta-analysis. Lancet 2009, 373, 746–758. [Google Scholar] [CrossRef]
- Forbes, G.B.; Prochaska, E.; Weitkamp, L.R. Genetic factors in abdominal obesity, a risk factor for stroke. N. Engl. J. Med. 1988, 318, 1070. [Google Scholar] [PubMed]
- Quek, Y.H.; Tam, W.W.S.; Zhang, M.W.B.; Ho, R.C.M. Exploring the association between childhood and adolescent obesity and depression: A meta-analysis. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2017, 18, 742–754. [Google Scholar] [CrossRef] [PubMed]
- Ho, R.C.; Fu, E.H.; Chua, A.N.; Cheak, A.A.; Mak, A. Clinical and psychosocial factors associated with depression and anxiety in singaporean patients with rheumatoid arthritis. Int. J. Rheum. Dis. 2011, 14, 37–47. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic 1 | Non-Escitalopram User | Escitalopram User | p-Value 2 |
|---|---|---|---|
| No. (%) | 736 (94.97) | 39 (5.03) | |
| Age, years | 66.6 ± 13.0 | 71.4 ± 10.5 | 0.02 |
| Female gender, % | 284 (38.6) | 17 (43.6) | 0.53 |
| BMI at admission, kg/m2 | 23.74 ± 3.29 | 23.43 ± 3.15 | 0.55 |
| Dysphagia | 89 (12.1) | 19 (48.7) | <0.001 |
| Type of meals at 3 days after stroke onset | |||
| General diet | 606 (82.3) | 18 (46.2) | <0.001 |
| Tube feeding | 87 (11.8) | 19 (48.7) | |
| Fasting | 43 (5.8) | 2 (5.1) | |
| Cardiovascular risk factor | |||
| Prior ischemic stroke | 124 (16.8) | 5 (12.8) | 0.51 |
| Hypertension | 445 (60.5) | 24 (61.5) | 0.89 |
| Diabetes | 221 (30.0) | 11 (28.2) | 0.81 |
| Dyslipidemia | 225 (30.6) | 16 (41.0) | 0.17 |
| Smoking | 253 (34.4) | 12 (30.8) | 0.64 |
| Atrial fibrillation | 125 (17.0) | 8 (20.5) | 0.57 |
| Stroke subtype | <0.05 | ||
| Large artery atherosclerosis | 188 (28.4) | 11 (28.9) | |
| Small vessel occlusion | 157 (23.7) | 4 (10.5) | |
| Cardioembolic | 148 (22.4) | 16 (42.1) | |
| Undetermined | 113 (17.1) | 4 (10.5) | |
| Other determined | 56 (8.5) | 3 (7.9) | |
| Hospital stay, days | 9.7 ± 7.7 | 21.9 ± 14.9 | <0.001 |
| ICU stay, n (%) | 22 (3.0) | 5 (12.8) | 0.001 |
| Duration of ICU stay, days | 5.4 ± 6.7 | 12.4 ± 12.2 | <0.001 |
| Mechanical ventilation, n (%) | 23 (3.1) | 4 (10.3) | 0.02 |
| Duration of ventilator use, days | 7.4 ± 9.8 | 4.6 ± 4.6 | 0.58 |
| Infection, n (%) | 32 (4.3) | 11 (28.2) | <0.001 |
| Initial neurological severity, median (IQR) | 3 (1, 5) | 4 (1, 7) | 0.34 |
| NIHSS, 0–7 | 601 (81.7) | 32 (82.1) | 0.74 |
| NIHSS, 8–14 | 76 (10.3) | 5 (12.8) | |
| NIHSS, ≥15 | 59 (8.0) | 2 (5.1) | |
| Change in neurological severity | 0.36 | ||
| Much improved, NIHSS change > 3, n (%) | 205 (27.9) | 13 (33.3) | |
| Mild improved, 1 ≤ NIHSS change ≤ 3, n (%) | 158 (21.5) | 8 (20.5) | |
| Stable, NIHSS = 0, n (%) | 289 (39.3) | 17 (43.6) | |
| Deterioration, NIHSS < 0, n (%) | 84 (11.4) | 1 (2.6) | |
| Laboratory | |||
| White blood cell count | 7598 ± 2571 | 8032 ± 3236 | 0.31 |
| Hemoglobin, g/dL | 13.6 ± 1.9 | 12.8 ± 2.3 | 0.03 |
| Hematocrit, g/dL | 40.2 ± 5.5 | 38.2 ± 6.6 | 0.03 |
| Fasting blood sugar, mg/dL | 106.8 ± 34.7 | 118.0 ± 32.7 | <0.05 |
| HbA1c, % | 6.4 ± 1.2 | 6.4 ± 1.0 | 0.88 |
| Low density lipoprotein, mg/dL | 102.6 ± 38.8 | 98.9 ± 46.0 | 0.62 |
| Total cholesterol, mg/dL | 172.9 ± 41.9 | 177.3 ± 42.8 | 0.53 |
| Triglyceride, mg/dL | 115.7 ± 58.3 | 140.9 ± 83.8 | 0.07 |
| Prothrombin time | 1.01 ± 0.24 | 0.97 ± 0.13 | 0.33 |
| aPTT | 32.10 ± 12.21 | 30.87 ± 5.75 | 0.62 |
| Variables | OR | 95% CI | p-Value |
|---|---|---|---|
| Age, per 1 years | 1.03 | 0.99–1.07 | 0.11 |
| Female gender | 1.51 | 0.63–3.60 | 0.36 |
| Hospital duration, per 1 days | 1.07 | 1.04–1.10 | <0.001 |
| ICU stay | 1.75 | 0.50–6.11 | 0.38 |
| Mechanical ventilation | 5.15 | 1.53–17.40 | <0.01 |
| Infection | 2.75 | 0.94–7.99 | 0.06 |
| Type of meals at 3 days after stroke onset | |||
| General diet | reference | reference | reference |
| Tube feeding | 1.93 | 0.71–5.24 | 0.20 |
| Fasting | 1.29 | 0.25–6.58 | 0.76 |
| Initial neurological severity | |||
| NIHSS at admission, 0–7 | reference | reference | reference |
| NIHSS at admission, 8–14 | 1.56 | 0.53–4.58 | 0.42 |
| NIHSS at admission, ≥15 | 0.30 | 0.05–1.66 | 0.17 |
| Stroke subtype | |||
| Large artery atherosclerosis | reference | reference | reference |
| Small vessel occlusion | 0.63 | 0.18–2.17 | 0.46 |
| Cardioembolic | 0.94 | 0.35–2.49 | 0.90 |
| Undetermined | 0.53 | 0.15–1.93 | 0.34 |
| Other determined | 0.77 | 0.17–3.49 | 0.74 |
| Cardiovascular risk factor | |||
| Prior ischemic stroke | 0.85 | 0.29–2.53 | 0.77 |
| Hypertension | 0.79 | 0.34–1.80 | 0.57 |
| Diabetes | 0.88 | 0.38–2.08 | 0.78 |
| Dyslipidemia | 1.71 | 0.78–3.73 | 0.18 |
| Smoking | 0.98 | 0.40–2.45 | 0.97 |
| Atrial fibrillation | 1.78 | 0.67–4.65 | 0.24 |
| Variables | OR | 95% CI | p-Value |
|---|---|---|---|
| Age, per 1 years | 1.00 | 0.98–1.01 | 0.79 |
| Female gender | 0.94 | 0.57–1.53 | 0.79 |
| Initial neurological severity | |||
| NIHSS at admission, 0–7 | reference | reference | reference |
| NIHSS at admission, 8–14 | 8.55 | 4.93–14.81 | <0.001 |
| NIHSS at admission, ≥15 | 16.25 | 8.20–32.20 | <0.001 |
| Escitalopram use | 1.27 | 0.50–3.25 | 0.61 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Kim, Y. Which Patients Are Prescribed Escitalopram?: Predictors for Escitalopram Prescriptions and Functional Outcomes among Patients with Acute Ischemic Stroke. Int. J. Environ. Res. Public Health 2018, 15, 1085. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15061085
Kim J, Kim Y. Which Patients Are Prescribed Escitalopram?: Predictors for Escitalopram Prescriptions and Functional Outcomes among Patients with Acute Ischemic Stroke. International Journal of Environmental Research and Public Health. 2018; 15(6):1085. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15061085
Chicago/Turabian StyleKim, Jarim, and Yerim Kim. 2018. "Which Patients Are Prescribed Escitalopram?: Predictors for Escitalopram Prescriptions and Functional Outcomes among Patients with Acute Ischemic Stroke" International Journal of Environmental Research and Public Health 15, no. 6: 1085. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15061085