ETS Exposure and PAH Body Burden in Nonsmoking Italian Adults

 , , ,
, , ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
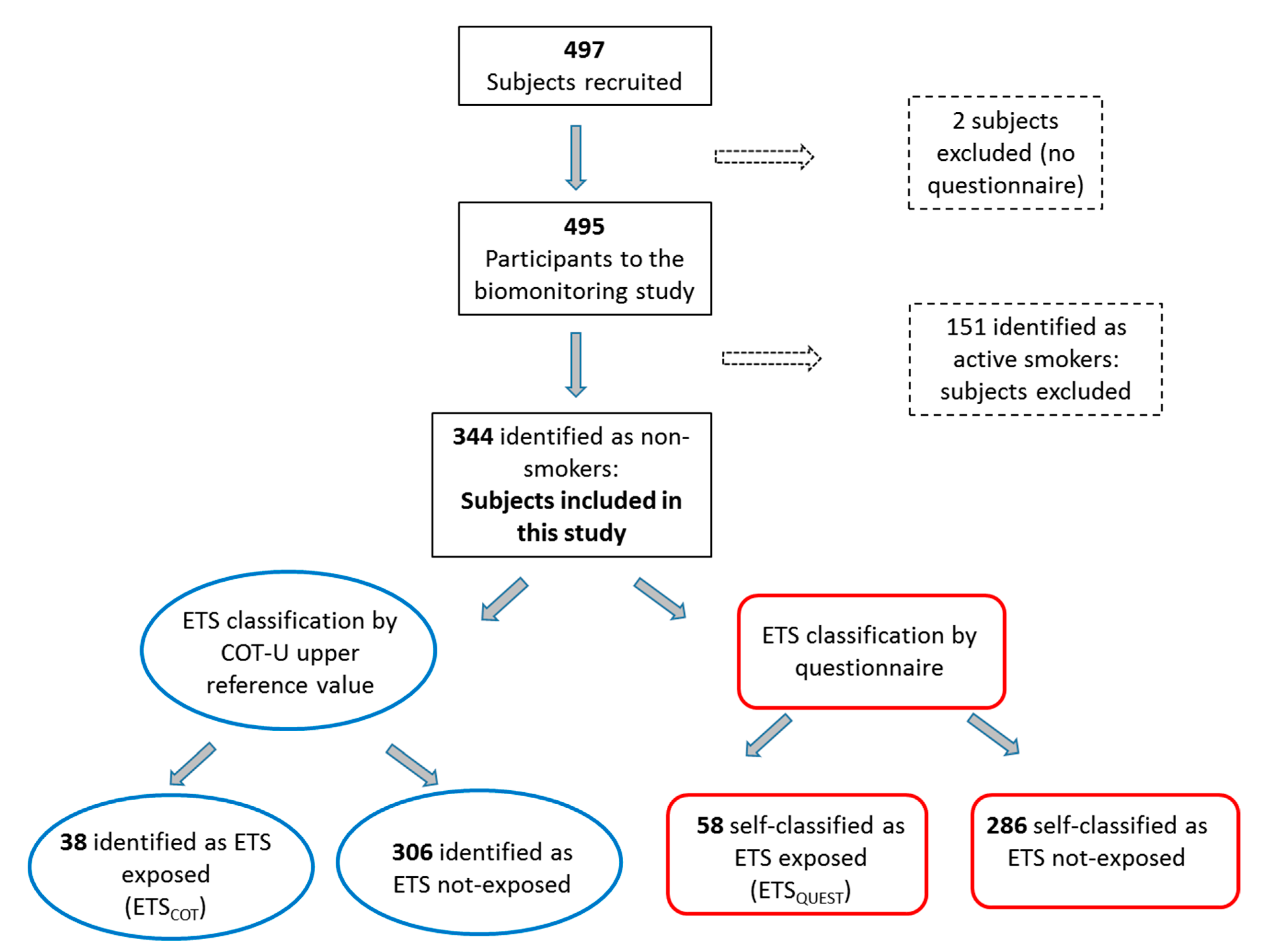
2.1. Study Population and Sample Collection
2.2. Questionnaire for Assessment of Active or Environmental Exposure to Tobacco Smoke
2.3. Quantification of COT-U Level
2.4. Urinary PAHs and 1-OHPYR Analysis
2.5. Urinary Creatinine
2.6. Statistical Analysis
3. Results
3.1. Study Population
3.2. ETS Exposure
3.3. PAH Exposure and ETS
3.4. Contribution of ETS to PAH Exposure
4. Discussion
4.1. Biomarkers of ETS and PAH Exposure
4.2. ETS and PAH Exposure
4.3. Role of ETS in Determining PAH Exposure
4.4. Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Matt, G.E.; Quintana, P.J.E.; Destaillats, H.; Gundel, L.A.; Sleiman, M.; Singer, B.C.; Jacob, I.P.; Benowitz, N.L.; Winickoff, J.P.; Rehan, V.; et al. Thirdhand tobacco smoke: Emerging evidence and arguments for a multidisciplinary research agenda. Environ. Health Perspect. 2011, 119, 1218–1226. [Google Scholar] [CrossRef] [PubMed]
- International Agency for Research on Cancer (IARC). IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Tobacco Smoke and Involuntary Smoking; World Health Organization: Lyon, France, 2004; Volume 83. [Google Scholar]
- Lodovici, M.; Akpan, V.; Evangelisti, C.; Dolara, P. Sidestream tobacco smoke as the main predictor of exposure to polycyclic aromatic hydrocarbons. J. Appl. Toxicol. 2004, 24, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y.S.; Trommel, J.S.; Yan, X.J.; Ashley, D.; Watson, C.H. Determination of 14 PAHs in mainstream smoke from domestic cigarettes. Environ. Sci. Technol. 2005, 39, 471–478. [Google Scholar] [CrossRef] [PubMed]
- International Agency for Research on Cancer (IARC). Some Non-Heterocyclic Polycyclic Aromatic Hydrocarbons and Some Related Exposures. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans; International Agency for Reaserch on Cancer (IARC): Lyon, France, 2010; Volume 92. [Google Scholar]
- Choi, H.; Perera, F.; Pac, A.; Wang, L.; Flak, E.; Mroz, E.; Jacek, R.; Chai-Onn, T.; Jedrychowski, W.; Masters, E.; et al. Estimating individual-level exposure to airborne polycyclic aromatic hydrocarbons throughout the gestational period based on personal, indoor, and outdoor monitoring. Environ. Health Perspect. 2008, 116, 1509–1518. [Google Scholar] [CrossRef] [PubMed]
- Edwards, S.C.; Jedrychowski, W.; Butscher, M.; Camann, D.; Kieltyka, A.; Mroz, E.; Flak, E.; Li, Z.; Wang, S.; Rauh, V.; et al. Prenatal exposure to airborne polycyclic aromatic hydrocarbons and Children’s intelligence at 5 years of age in a prospective cohort study in Poland. Environ. Health Perspect. 2010, 118, 1326–1331. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Cook, R.L.; Ilacqua, V.A.; Kan, H.; Talbott, E.O.; Kearney, G. Studying association between urinary metabolites of polycyclic aromatic hydrocarbons (PAHs) and cardiovascular diseases in the United States. Sci. Total Environ. 2010, 408, 4943–4948. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Liu, Y.; Sun, H.; Ma, J.; Xiao, L.; Cao, L.; Li, W.; Wang, B.; Yuan, J.; Chen, W. Associations of urinary polycyclic aromatic hydrocarbon metabolites with fractional exhaled nitric oxide and exhaled carbon monoxide: A cross-sectional study. Sci. Total Environ. 2018, 618, 542–550. [Google Scholar] [CrossRef] [PubMed]
- St Helen, G.; Goniewicz, M.L.; Dempsey, D.; Wilson, M.; Jacob, P.; Benowitz, N.L. Exposure and kinetics of polycyclic aromatic hydrocarbons (PAHs) in cigarette smokers. Chem. Res. Toxicol. 2012, 25, 952–964. [Google Scholar] [CrossRef] [PubMed]
- Suwan-ampai, P.; Navas-Acien, A.; Strickland, P.; Agnew, J. Involuntary tobacco smoke exposure and urinary levels of polycyclic aromatic hydrocarbons in the United States, 1999 to 2002. Cancer Epidemiol. Biomark. Prev. 2009, 18, 884–893. [Google Scholar] [CrossRef] [PubMed]
- Aquilina, N.J.; Delgado-Saborit, J.M.; Meddings, C.; Baker, S.; Harrison, R.M.; Jacob, P., III; Wilson, M.; Yu, L.; Duan, M.; Benowitz, N.L. Environmental and biological monitoring of exposure to PAHs and ETS in the general population. Environ. Int. 2010, 36, 763–771. [Google Scholar] [CrossRef] [PubMed]
- Grover, P.L. Pathways involved in the metabolism and activation of polycyclic hydrocarbons. Xenobiotica 1986, 16, 915–931. [Google Scholar] [CrossRef] [PubMed]
- Ramesh, A.; Walker, S.A.; Hood, D.B.; Guillén, M.D.; Schneider, K.; Weyand, E.H. Bioavaibility and risk assement of orally ingested polycyclic aromatic hydrocarbons. Int. J. Toxicol. 2004, 23, 301–333. [Google Scholar] [CrossRef] [PubMed]
- Waidyanatha, S.; Zheng, Y.; Rappaport, S.M. Determination of polycyclic aromatic hydrocarbons in urine of coke oven workers by headspace solid phase microextraction and gas chromatography-mass spectrometry. Chem. Biol. Interact. 2003, 145, 165–174. [Google Scholar] [CrossRef]
- Campo, L.; Fustinoni, S.; Buratti, M.; Cirla, P.; Martinotti, I.; Foà, V. Unmetabolized polycyclic aromatic hydrocarbons in urine as biomarkers of low exposures in asphalt workers. J. Occup. Environ. Hyg. 2007, 4, 100–110. [Google Scholar] [CrossRef]
- Gatti, M.G.; Bechtold, P.; Campo, L.; Barbieri, G.; Quattrini, G.; Ranzi, A.; Sucato, S.; Olgiati, L.; Polledri, E.; Romolo, M.; et al. Human biomonitoring of polycyclic aromatic hydrocarbons and metals in the general population residing near the municipal solid waste incinerator of Modena, Italy. Chemosphere 2017, 186, 546–557. [Google Scholar] [CrossRef] [PubMed]
- Campo, L.; Polledri, E.; Bechtold, P.; Gatti, G.; Ranzi, A.; Lauriola, P.; Goldoni, C.A.; Bertazzi, P.A.; Fustinoni, S. Determinants of active and environmental exposure to tobacco smoke and upper reference value of urinary cotinine in not exposed individuals. Environ. Res. 2016, 148, 154–163. [Google Scholar] [CrossRef] [PubMed]
- AIA Study. Progetto A.I.A—Sorveglianza e biomonitoraggio di una coorte di modenesi residenti nell’area circostante l’impianto di incenerimento urbano. [Health Surveillance and Biomonitoring of a Cohort of Subjects Living in the Vicinity of an Urban Solid-Waste Incinerator]. Available online: http://www.Ausl.Mo.It/dsp/flex/cm/pages/serveblob.Php/l/it/idpagina/3472 (accessed on 29 June 2015).
- Fustinoni, S.; Campo, L.; Polledri, E.; Mercadante, R.; Erspamer, L.; Ranzi, A.; Lauriola, P.; Goldoni, C.A.; Bertazzi, P. A validated method for urinary cotinine quantification used to classify active and environmental tobacco smoke exposure. Curr. Anal. Chem. 2013, 9, 447–456. [Google Scholar] [CrossRef]
- Campo, L.; Fustinoni, S.; Bertazzi, P. Quantification of carcinogenic 4- to 6-ring polycyclic aromatic hydrocarbons in human urine by solid-phase microextraction gas chromatography-isotope dilution mass spectrometry. Anal. Bioanal. Chem. 2011, 401, 625–634. [Google Scholar] [CrossRef] [PubMed]
- Kroll, M.H.; Chesler, R.; Hagengruber, C.; Blank, D.W.; Kestner, J.; Rawe, M. Automated determination of urinary creatinine without sample dilution: Theory and practice. Clin. Chem. 1986, 32, 446–452. [Google Scholar] [PubMed]
- World Health Organization (WHO). Biological Monitoring of Chemical Exposure in the Workplace; WHO: Geneva, Switzerland, 1996; Volume 1. [Google Scholar]
- Barr, D.B.; Wilder, L.C.; Caudill, S.P.; Gonzalez, A.J.; Needham, L.L.; Pirkle, J.L. Urinary creatinine concentrations in the U.S. population: Implications for urinary biologic monitoring measurements. Environ. Health Perspect. 2005, 113, 192–200. [Google Scholar] [CrossRef] [PubMed]
- BalbèŠ, M.; Martinez-Sanchez, J.M.; Sureda, X.; Fu, M.; Pérez-Ortuño, R.; Pascual, J.A.; Saltó, E.; Fernández, E. Cigarettes vs. E-cigarettes: Passive exposure at home measured by means of airborne marker and biomarkers. Environ. Res. 2014, 135, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Sanchez, J.M.; Sureda, X.; Fu, M.; Pérez-Ortuño, R.; Ballbè, M.; López, M.J.; Saltó, E.; Pascual, J.A. Fernández E. Secondhand smoke exposure at home: Assessment by biomarkers and airborne markers. Environ. Res. 2014, 133, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Levine, H.; Berman, T.; Goldsmith, R.; Göen, T.; Spungen, J.; Novack, L.; Amitai, Y.; Shohat, T.; Grotto, I. Exposure to tobacco smoke based on urinary cotinine levels among Israeli smoking and nonsmoking adults: A cross-sectional analysis of the first Israeli human biomonitoring study. BMC Public Health 2013, 13, 1241. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Lim, Y.; Lee, S.; Kim, C.; Hong, C.; Shin, D. Relationship between environmental tobacco smoke and urinary cotinine levels in passive smokers at their residence. J. Expo. Anal. Environ. Epidemiol. 2004, 14 (Suppl. 1), S65–S70. [Google Scholar] [CrossRef] [PubMed]
- Simoni, M.; Baldacci, S.; Puntoni, R.; Pistelli, F.; Farchi, S.; Lo Presti, E.; Pistelli, R.; Corbo, G.; Agabiti, N.; Basso, S.; et al. Plasma, salivary and urinary cotinine in non-smoker italian women exposed and unexposed to environmental tobacco smoking (SEASD study). Clin. Chem. Lab. Med. 2006, 44, 632–638. [Google Scholar] [CrossRef] [PubMed]
- SIVR. Società italiana valori di riferimento. Fourth list of reference values for elements, organic compounds and their metabolites (Quarta lista dei valori di riferimento per elementi, composti organici e loro metaboliti). Available online: www.valoridiriferimento.it (accessed on 20 December 2017).
- Ranzi, A.; Fustinoni, S.; Erspamer, L.; Campo, L.; Gatti, M.G.; Bechtold, P.; Bonassi, S.; Trenti, T.; Goldoni, C.A.; Bertazzi, P.A.; et al. Biomonitoring of the general population living near a modern solid waste incinerator: A pilot study in Modena, Italy. Environ. Int. 2013, 61, 88–97. [Google Scholar] [CrossRef] [PubMed]
- De Craemer, S.; Croes, K.; van Larebeke, N.; Sioen, I.; Schoeters, G.; Loots, I.; Nawrot, T.; Nelen, V.; Campo, L.; Fustinoni, S.; et al. Investigating unmetabolized polycyclic aromatic hydrocarbons in adolescents' urine as biomarkers of environmental exposure. Chemosphere 2016, 155, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Campo, L.; Fustinoni, S.; Consonni, D.; Pavanello, S.; Kapka, L.; Siwinska, E.; Mielzyňska, D.; Bertazzi, P. Urinary carcinogenic 4-6 ring polycyclic aromatic hydrocarbons in coke oven workers and in subjects belonging to the general population: Role of occupational and environmental exposure. Int. J. Hyg. Environ. Health 2014, 217, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Merlo, F.; Andreassen, A.; Weston, A.; Pan, C.F.; Haugen, A.; Valerio, F.; Reggiardo, G.; Fontana, V.; Garte, S.; Puntoni, R.; et al. Urinary excretion of 1-hydroxypyrene as a marker for exposure to urban air levels of polyciclic aromatic hydrocarbons. Cancer Epidemiol. Biomarkers Prev. 1998, 7, 147–155. [Google Scholar] [PubMed]
- Bartolomé, M.; Ramos, J.J.; Cutanda, F.; Huetos, O.; Esteban, M.; Ruiz-Moraga, M.; Calvo, E.; Pérez-Gómez, B.; González, O.; Castaño, A.; et al. Urinary polycyclic aromatic hydrocarbon metabolites levels in a representative sample of the Spanish adult population: The BIOAMBIENT.ES project. Chemosphere 2015, 135, 436–446. [Google Scholar] [CrossRef] [PubMed]
- Chetiyanukornkul, T.; Toriba, A.; Kizu, R.; Hayakawa, K. Urinary 2-hydroxyfluorene and 1-hydroxypyrene levels in nonsmokers in japan and Thailand. Polycycl. Aromat. Compd. 2004, 24, 467–474. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | All Subjects N (%) | ETS Exposure by Questionnaire N (%) | ETS Exposure by COT-U N (%) | |||||
|---|---|---|---|---|---|---|---|---|
| No-ETS Exposure | ETS Exposure (ETSQUEST) | p * | No-ETS Exposure | ETS Exposure (ETSCOT) | p * | |||
| 344 | 286 (83) | 58 (17) | - | 306 (89) | 38 (11) | - | ||
| Age (years) Mean (minimum-maximum) | 45 (18–69) | 46 (18–69) | 40 (18–68) | 0.004 | 45 (18–69) | 42 (18–68) | 0.122 | |
| Age (class) N (%) | 18–34 | 96 (28) | 70 (2) | 26 (45) | 0.004 χ | 81 (26) | 15 (39) | 0.240 χ |
| 35–49 | 111 (32) | 99 (35) | 12 (21) | 101 (33) | 10 (26) | |||
| 50–69 | 137 (40) | 117 (41) | 20 (34) | 124 (41) | 13 (34) | |||
| Gender N (%) | Male | 161 (47) | 138 (48) | 23 (40) | 0.191 χ | 163 (53) | 20 (53) | 0.941 χ |
| Female | 183 (53) | 148 (52) | 35 (60) | 143 (47) | 18 (47) | |||
| Education N (%) | Primary school | 13 (9) | 9 (3) | 4 (7) | 0.077 χ | 10 (3) | 3 (8) | 0.361 χ |
| Secondary school | 82 (24) | 63 (22) | 19 (33) | 71 (23) | 11 (29) | |||
| High school | 144 (42) | 122 (43) | 22 (38) | 131 (43) | 13 (34) | |||
| Graduated | 103 (30) | 90 (31) | 13 (22) | 93 (30) | 10 (26) | |||
| Income (€/month) N (%) | No income | 3 (1) | 3 (1) | 0 (0) | 0.452 χ | 3 (1) | 0 | 0.700 χ |
| <1000 | 24 (7) | 20 (7) | 4 (7) | 22 (7) | 2 (5) | |||
| 1001–2000 | 94 (27) | 75 (26) | 19 (33) | 80 (26) | 14 (37) | |||
| 2001–3000 | 99 (29) | 78 (27) | 21 (36) | 91 (30) | 8 (21) | |||
| 3001–5000 | 76 (22) | 68 (24) | 8 (14) | 68 (22) | 8 (21) | |||
| >5000 | 23 (7) | 21 (7) | 2 (3) | 21 (7) | 2 (5) | |||
| Don’t know/missing | 25 (7) | 18 (6) | 4 (7) | 21 (7) | 4 (10 | |||
| Ethnicity | European whites | 324 (94) | 271 (95) | 53 (91) | 0.311 χ | 289 (94) | 35 (92) | 0.416 χ |
| Non-European whites | 8 (2) | 7 (2) | 1 (2) | 7 (2) | 1 (3) | |||
| African blacks | 5 (1) | 4 (1) | 1 (2) | 5 (2) | 0 (0) | |||
| Others | 7 (2) | 4 1) | 3 (5) | 5 (2) | 2 (5) | |||
| ETS duration (h/day) Mean (minimum-maximum) | - | - | 2 (0–10) | - | 1 (0–4) | 3 (0–10) | 0.054 | |
| ETS duration (h/week) Mean (minimum-maximum) | - | - | 10 (0–70) | - | 6 (0–28) | 18 (0–70) | 0.035 | |
| ETS duration (day/week) Mean (minimum-maximum) | - | - | 5 (1–7) | - | 4 (1–7) | 6 (2–7) | 0.002 | |
| COT-U (µg/L) Median (5th–95th percentile) | 0.47 (<0.1–3.91) | 0.39 (<0.1–1.78) | 1.38 (<0.1–9.06) | <0.001 | 0.40 (<0.1–1.32) | 3.63 (1.8–17.39) | <0.001 | |
| Analyte | All Subjects (N = 344) | ETS Exposure by Questionnaire | ETS Exposure by COT-U | ||||
|---|---|---|---|---|---|---|---|
| No-ETS Exposure (N = 286) | ETS Exposure (ETSQUEST) (N = 58) | p * | No-ETS Exposure (N = 306) | ETS Exposure (ETSCOT) (N = 38) | p * | ||
| Median (5–95 percentile); % > LOQ | Median (5–95 percentile); % > LOQ | Median (5–95 percentile); % > LOQ | Median (5–95 percentile); % > LOQ | Median (5–95 percentile); % > LOQ | |||
| 1-OHPYR µg/L | <0.05 (<0.05–0.13); 33 | <0.05 (<0.05–0.13); 34 | <0.05 (<0.05–0.11); 31 | 0.395 | <0.05 (<0.05–0.12); 32 | <0.05 (<0.05–0.17); 42 | 0.037 |
| U-NAP ng/L | 24.7 (13.4–78.7); 100 | 24.6 (13.0–80.0); 100 | 25.1 (14.2–65.3); 100 | 0.742 | 24.7 (13.4–80.0); 100 | 25.1 (12.5–63.3); 100 | 0.516 |
| U-ACY ng/L | 0.5 (<0.3–1.5); 95 | 0.5 (<0.3–1.5); 95 | 0.6 (<0.3–1.7); 95 | 0.517 | 0.5 (0.3–1.5); 95 | 0.6 (<0.3–1.5); 92 | 0.937 |
| U-ACE ng/L | 0.9 (<0.6–3.4); 79 | 0.9 (<0.6–3.4); 78 | 1.0 (<0.6–3.0); 85 | 0.889 | 0.9 (<0.6–3.5); 78 | 0.9 (<0.6–2.1); 89 | 0.768 |
| U-FLU ng/L | 1.5 (0.9–2.9); 96 | 1.5 (0.9–2.8); 96 | 1.5 (1.0–2.9); 97 | 0.798 | 1.5 (0.9–2.8); 96 | 1.7 (1.0–3.2); 100 | 0.028 |
| U-PHE ng/L | 7.2 (4.7–14.6); 100 | 7.2 (4.6–14.1); 100 | 7.1 (5.0–17.2); 100 | 0.566 | 7.1 (4.7–14.9); 100 | 7.7 (5.0–13.5); 100 | 0.274 |
| U-ANT ng/L | 2.1 (0.9–3.1); 100 | 2.0 (0.9–3.1); 100 | 2.2 (0.8–5.7); 100 | 0.102 | 2.1 (0.9–3.1); 100 | 2.3 (1.0–3.3); 100 | 0.028 |
| U-FLT ng/L | 0.7 (<0.6–1.3); 72 | 0.7 (<0.6–1.3); 72 | 0.6 (<0.6–1.4); 69 | 0.728 | 0.7 (<0.6–1.2); 71 | 0.8 (<0.6–1.5); 73 | 0.340 |
| U-PYR ng/L | 0.6 (<0.4–1.1); 92 | 0.6 (<0.4–1.1); 91 | 0.6 (<0.4–1.3); 95 | 0.323 | 0.6 (<0.4–1.1); 92 | 0.7 (<0.4–1.3); 89 | 0.052 |
| U-BaA ng/L | <0.3 (<0.3–0.8); 18 | <0.3 (<0.3–0.8); 19 | <0.3 (<0.3–1.4); 17 | 0.809 | <0.3 (<0.3–0.8); 19 | <0.3 (<0.3–2.1); 13 | 0.716 |
| U-CHR ng/L | 0.2 (<0.2–0.7); 65 | 0.2 (<0.2–0.6); 64 | 0.2 (<0.2–1.7); 67 | 0.223 | 0.2 (<0.2–0.7); 65 | 0.2 (<0.2–1.4); 66 | 0.398 |
| Analyte | Statistics a,b | Model 1 | Model 2 | Model 3 |
|---|---|---|---|---|
| COT-U (µg/L) | ETSCOT | ETSQUEST | ||
| 1-OHPYR * | Beta (std) | 0.043 (0.019) | 0.078 (0.194) | −0.017 (0.144) |
| 95%CI | 0.005–0.080 | −0.304–0.461 | −0.300–0.266 | |
| p | 0.026 | 0.687 | 0.906 | |
| U-NAP | Beta (std) | 0.002 (0.003) | 0.014 (0.025) | 0.005 (0.024) |
| 95%CI | −0.004–0.009 | −0.035–0.064 | −0.043–0.053 | |
| p | 0.476 | 0.572 | 0.842 | |
| U-ACY | Beta (std) | −0.003 (0.012) | 0.076 (0.100) | −0.049 (0.087) |
| 95%CI | −0.027–0.020 | −0.119–0.271 | −0.221–0.123 | |
| p | 0.781 | 0.445 | 0.573 | |
| U-ACE * | Beta (std) | −0.003 (0.013) | 0.003 (0.103) | 0.060 (0.106) |
| 95%CI | −0.028–0.023 | −0.200–0.205 | −0.149–0.270 | |
| p | 0.821 | 0.979 | 0.572 | |
| U-FLU | Beta (std) | 0.003 (0.011) | 0.126 (0.067) | 0.035 (0.054) |
| 95%CI | −0.017–0.024 | −0.006–0.258 | −0.071–0.140 | |
| p | 0.743 | 0.061 | 0.520 | |
| U-PHE | Beta (std) | −0.000 (0.001) | 0.000 (0.010) | −0.008 (0.011) |
| 95%CI | −0.003–0.002 | −0.0189–0.019 | −0.030–0.015 | |
| p | 0.737 | 0.980 | 0.503 | |
| U-ANT | Beta (std) | 0.015 (0.010) | 0.024 (0.087) | 0–0.018 (0.073) |
| 95%CI | −0.005–0.034 | −0.147–0.194 | −0.162–0.126 | |
| p | 0.134 | 0.784 | 0.804 | |
| U-FLT | Beta (std) | 0.009 (0.008) | 0.0480 (0.067) | −0.032 (0.053) |
| 95%CI | −0.008–0.0247 | −0.084–0.179 | −0.135–0.071 | |
| p | 0.299 | 0.474 | 0.545 | |
| U-PYR | Beta (std) | 0.004 (0.007) | 0.040 (0.063) | 0.000 (0.049) |
| 95%CI | −0.010–0.017 | −0.085–0.163 | −0.097–0.097 | |
| p | 0.616 | 0.534 | 0.999 | |
| U-CHR * | Beta (std) | −0.015 (0.013) | −0.007 (0.100) | −0.056 (0.092) |
| 95%CI | −0.041–0.011 | −0.204–0.190 | −0.238–0.126 | |
| p | 0.254 | 0.944 | 0.547 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campo, L.; Polledri, E.; Bechtold, P.; Gatti, G.; Quattrini, G.; Olgiati, L.; Romolo, M.; Ranzi, A.; Lauriola, P.; Carrozzi, G.; et al. ETS Exposure and PAH Body Burden in Nonsmoking Italian Adults. Int. J. Environ. Res. Public Health 2018, 15, 1156. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15061156
Campo L, Polledri E, Bechtold P, Gatti G, Quattrini G, Olgiati L, Romolo M, Ranzi A, Lauriola P, Carrozzi G, et al. ETS Exposure and PAH Body Burden in Nonsmoking Italian Adults. International Journal of Environmental Research and Public Health. 2018; 15(6):1156. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15061156
Chicago/Turabian StyleCampo, Laura, Elisa Polledri, Petra Bechtold, Giulia Gatti, Giulia Quattrini, Luca Olgiati, Michael Romolo, Andrea Ranzi, Paolo Lauriola, Giuliano Carrozzi, and et al. 2018. "ETS Exposure and PAH Body Burden in Nonsmoking Italian Adults" International Journal of Environmental Research and Public Health 15, no. 6: 1156. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15061156