Gender and Age Differences in Social Inequality on Adolescent Life Satisfaction: A Comparative Analysis of Health Behaviour Data from 41 Countries


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects and Study Design
2.2. Measures
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Marmot, M.; Feeney, A. General explanations for social inequalities in health. IARC Sci. Publ. 1997, 138, 207–228. [Google Scholar]
- Marmot, M.G. Understanding social inequalities in health. Perspect. Biol. Med. 2003, 46 (Suppl. 3), S9–S23. [Google Scholar] [CrossRef] [PubMed]
- Social Inequalities in Environment and Health. World Health Organization Regional Office for Europe. Available online: http://www.euro.who.int/en/health-topics/environment-and-health/social-inequalities-in-environment-and-health (accessed on 28 May 2018).
- Judge, K.; Platt, S.; Costongs, C.; Jurczak, K. Health Inequalities: A Challenge for Europe. 2005. Available online: https://eurohealthnet.eu/sites/eurohealthnet.eu/files/publications/pu_2.pdf (accessed on 28 May 2018).
- Marmot, M.; Allen, J.; Bell, R.; Bloomer, E.; Goldblatt, P.; Consortium for the European Review of Social Determinants of Health and the Health Divide. WHO European review of social determinants of health and the health divide. Lancet 2012, 380, 1011–1029. [Google Scholar] [CrossRef]
- Reiss, F. Socioeconomic inequalities and mental health problems in children and adolescents: A systematic review. Soc. Sci. Med. 2013, 90, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Social Inequality in Health. Public Health Report. Norwegian Institute of Public Health. 2017. Available online: https://www.fhi.no/en/op/hin/helse-i-ulike-befolkningsgrupper/social-inequalities/#inequalities-in-health-among-children-and-adolescents (accessed on 28 May 2018).
- Viner, R.M.; Ozer, E.M.; Denny, S.; Marmot, M.; Resnick, M.; Fatusi, A.; Currie, C. Adolescence and the social determinants of health. Lancet 2012, 379, 1641–1652. [Google Scholar] [CrossRef]
- Levin, K.A.; Torsheim, T.; Vollebergh, W.; Richter, M.; Davies, C.A.; Schnohr, C.W.; Due, P.; Currie, C. National income and income inequality, family affluence and life satisfaction among 13 years old boys and girls: A multilevel study in 35 countries. Soc. Indic. Res. 2011, 104, 179–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosseinpoor, A.R.; Stewart Williams, J.A.; Itani, L.; Chatterji, S. Socioeconomic inequality in domains of health: Results from the World Health Surveys. BMC Public Health 2012, 12, 198. [Google Scholar] [CrossRef] [PubMed]
- HBSC. Health Behaviour in School-aged Children: World Health Organization Collaborative Cross-national Survey. Available online: http://www.hbsc.org (accessed on 28 May 2018).
- Currie, C.; Zanotti, C.; Morgan, A.; Currie, D.; de Looze, M.; Roberts, C.; Samdal, O.; Smith, O.R.F.; Barnekow, V. (Eds.) Social Determinants of Health and Well-Being among Young People. Health Behaviour in School-Aged Children (HBSC) Study: International Report from the 2009/2010 Survey; Health Policy for Children and Adolescents, No. 6; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2012; ISBN 978 92 890 1423 6. [Google Scholar]
- Inchley, J.; Currie, D.; Young, T.; Samdal, O.; Torsheim, T.; Augustson, L.; Mathison, F.; Aleman-Diaz, A.; Molcho, M.; Weber, M.; et al. (Eds.) Growing Up Unequal: Gender and Socioeconomic Differences in Young People’s Health and Well-Being. Health Behaviour in School-Aged Children (HBSC) Study: International Report from the 2013/2014 Survey; Health Policy for Children and Adolescents, No. 7; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2016; ISBN 978 92 890 5136 1. [Google Scholar]
- Bakken, A.; Frøyland, L.R.; Sletten, M.A. Sosiale Forskjeller i Unges liv. Hva sier Ungdata-Undersøkelsene? (Social Differences in Young People’s Lives. What Do the youth Data Surveys Say?) [Report] NOVA Report 3/16; Høgskolen i Oslo og Akershus: Oslo, Norway, 2016; ISBN 978-82-7894-578-0. Available online: http://www.hioa.no/Om-HiOA/Senter-for-velferds-og-arbeidslivsforskning/NOVA/Publikasjonar/Rapporter/2016/Sosiale-forskjeller-i-unges-liv (accessed on 28 May 2018).
- van Zon, S.K.; Bültmann, U.; Mendes de Leon, C.F.; Reijneveld, S.A. Absolute and Relative Socioeconomic Health Inequalities across Age Groups. PLoS ONE 2015, 10, e0145947. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, D.R.; Kipp, K. Developmental Psychology: Childhood and Adolescence, 9th ed.; Wadsworth Cengage Learning: Belmont, CA, USA, 2014; ISBN-13: 978-1133491231. [Google Scholar]
- Steinberg, L.; Vandell, D.L.; Bornstein, M.H. Development: Infancy through Adolescence; Wadsworth Cengage Learning: Belmont, CA, USA, 2011; ISBN-13: 978-0618721559. [Google Scholar]
- Wickrama, K.A.; Noh, S.; Elder, G.H. An investigation of family SES-based inequalities in depressive symptoms from early adolescence to emerging adulthood. Adv. Life Course Res. 2009, 14, 147–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- West, P.; Sweeting, H. Evidence on equalisation in health in youth from the West of Scotland. Soc. Sci. Med. 2004, 59, 13–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajmil, L.; Herdman, M.; Ravens-Sieberer, U.; Erhart, M.; Alonso, J.; European KIDSCREEN Group. Socioeconomic inequalities in mental health and health-related quality of life (HRQOL) in children and adolescents from 11 European countries. Int. J. Public Health 2014, 59, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Ravens-Sieberer, U.; Torsheim, T.; Hetland, J.; Vollebergh, W.; Cavallo, F.; Jericek, H.; Alikasifoglu, M.; Välimaa, R.; Ottova, V.; Erhart, M.; et al. Subjective health, symptom load and quality of life of children and adolescents in Europe. Int. J. Public Health 2009, 54 (Suppl. 2), S151–S159. [Google Scholar] [CrossRef] [PubMed]
- Health Behaviour in School-Aged Children Study: A World Health Organization Collaborative Cross-National Study; Internal Protocol 2013/2014; University of St Andrews: St Andrews, UK, 2013; Available online: https://drive.google.com/file/d/0BxYI8UzU8n1faEZ4WUhmS0UxcVU/view (accessed on 28 May 2018).
- Cantril, H. The Pattern of Human Concerns; Rutgers University Press: New Brunswick, NJ, USA, 1965. [Google Scholar]
- Levin, K.A.; Currie, C. Reliability and validity of an adapted version of the Cantril Ladder for use with adolescent samples. Soc. Indic. Res. 2014, 119, 1047–1063. [Google Scholar] [CrossRef]
- Currie, C.; Molcho, M.; Boyce, W.; Holstein, B.; Torsheim, T.; Richter, M. Researching health inequalities in adolescents: The development of the Health Behaviour in School-Aged Children (HBSC) family affluence scale. Soc. Sci. Med. 2008, 66, 1429–1436. [Google Scholar] [CrossRef] [PubMed]
- Torsheim, T.; Cavallo, F.; Levin, K.A.; Schnohr, C.; Mazur, J.; Niclasen, B.; Currie, C.; FAS Development Study Group. Psychometric Validation of the Revised Family Affluence Scale: A Latent Variable Approach. Child Indic. Res. 2016, 9, 771–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kunst, A.E.; Mackenbach, J.P. Measuring Socio-Economic Inequalities in Health; World Health Organisation, Regional Office for Europe: Copenhagen, Denmark, 1995. [Google Scholar]
- Zaborskis, A.; Grincaite, M.; Lenzi, M.; Tesler, R.; Moreno-Maldonado, C.; Mazur, J. Social Inequality in Adolescent Life Satisfaction: Comparison of Measure Approaches and Correlation with Macro-level Indices in 41 Countries. Soc. Indic. Res. 2018. [Google Scholar] [CrossRef]
- von Rueden, U.; Gosch, A.; Rajmil, L.; Bisegger, C.; Ravens-Sieberer, U. Socioeconomic determinants of health related quality of life in childhood and adolescence: Results from a European study. J. Epidemiol. Community Health 2006, 60, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Bradley, R.H.; Corwyn, R.F. Socioeconomic status and child development. Annu. Rev. Psychol. 2002, 53, 371–399. [Google Scholar] [CrossRef] [PubMed]
- Holstein, B.E.; Currie, C.; Boyce, W.; Mogens, T.; Damsgaard, M.; Gobina, I.; Kökönyei, G.; Hetland, J.; de Looze, M.; Richter, M.; et al. Socio-economic inequalities in multiple health complaints among adolescents: International comparative study in 37 countries. Int. J. Public Health 2009, 54 (Suppl. 2), 260–270. [Google Scholar] [CrossRef] [PubMed]
- Ravens-Sieberer, U.; Wille, N.; Erhart, M.; Nickel, J.; Richter, M.; Suhrcke, M. Socioeconomic Inequalities in mental health among adolescents in Europe. In Social Cohesion for Mental Well-Being among Adolescents; WHO/HBSC Forum 2007; World Health Organization, Regional Office for Europe: Copenhagen, Denmark, 2008; pp. 26–42. ISBN 978 92 890 4288 8. [Google Scholar]
- Perry, D.G.; Pauletti, R.E. Gender and Adolescent Development. J. Res. Adolesc. 2011, 21, 61–74. [Google Scholar] [CrossRef]
- Chen, E.; Matthews, K.A.; Boyce, W.T. Socioeconomic differences in children’s health: How and why do these relationships change with age? Psychol. Bull. 2002, 128, 295–329. [Google Scholar] [CrossRef] [PubMed]
- Diener, E.; Inglehart, R.; Tay, L. Theory and validity of life satisfaction scales. Soc. Ind. Res. 2013, 112, 497–527. [Google Scholar] [CrossRef]
- Investing in Children: The European Child and Adolescent Health Strategy 2015–2020; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2014; Available online: http://www.euro.who.int/__data/assets/pdf_file/0010/253729/64wd12e_InvestCAHstrategy_140440.pdf (accessed on 12 June 2018).


{kind=link}
{kind=link}
| Variables and Categories | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| Exp(B) | (95% CI) | p | Exp(B) | (95% CI) | p | |
| Gender | ||||||
| Boys | 1 | 1 | ||||
| Girls | 1.133 | (1.126–1.139) | <0.001 | 1.125 | (1.118–1.132) | <0.001 |
| Age group | ||||||
| 11-year-old | 1 | 1 | ||||
| 13-year-old | 1.283 | (1.274–1.293) | <0.001 | 1.285 | (1.275–1.295) | <0.001 |
| 15-year-old | 1.465 | (1.455–1.476) | <0.001 | 1.454 | (1.443–1.465) | <0.001 |
| Family structure | ||||||
| Both parents | 1 | 1 | ||||
| Not both parents | 1.270 | (1.262–1.279) | <0.001 | 1.218 | (1.210–1.226) | <0.001 |
| Family affluence | ||||||
| Extremely highest affluence | 1 | 1 | ||||
| Extremely lowest affluence b | 1.419 | (1.405–1.434) | <0.001 | 1.344 | (1.330–1.359) | <0.001 |
| Group of Adolescents | RII Value (95% CI) in the Total Sample a | RII Value (95% CI) in Selected Countries | |||
|---|---|---|---|---|---|
| 3 Countries with the Lowest RII Value | 3 Countries with the Highest Value | ||||
| All adolescents | 1.344 (1.330–1.359) | Malta | 1.088 (0.982–1.204) | Hungary | 1.777 (1.659–1.915) |
| Belgium (Flemish) | 1.129 (1.058–1.205) | Republic of Moldova | 1.736 (1.603–1.879) | ||
| Belgium (French) | 1.159 (1.092–1.231) | Israel | 1.673 (1.554–1.801) | ||
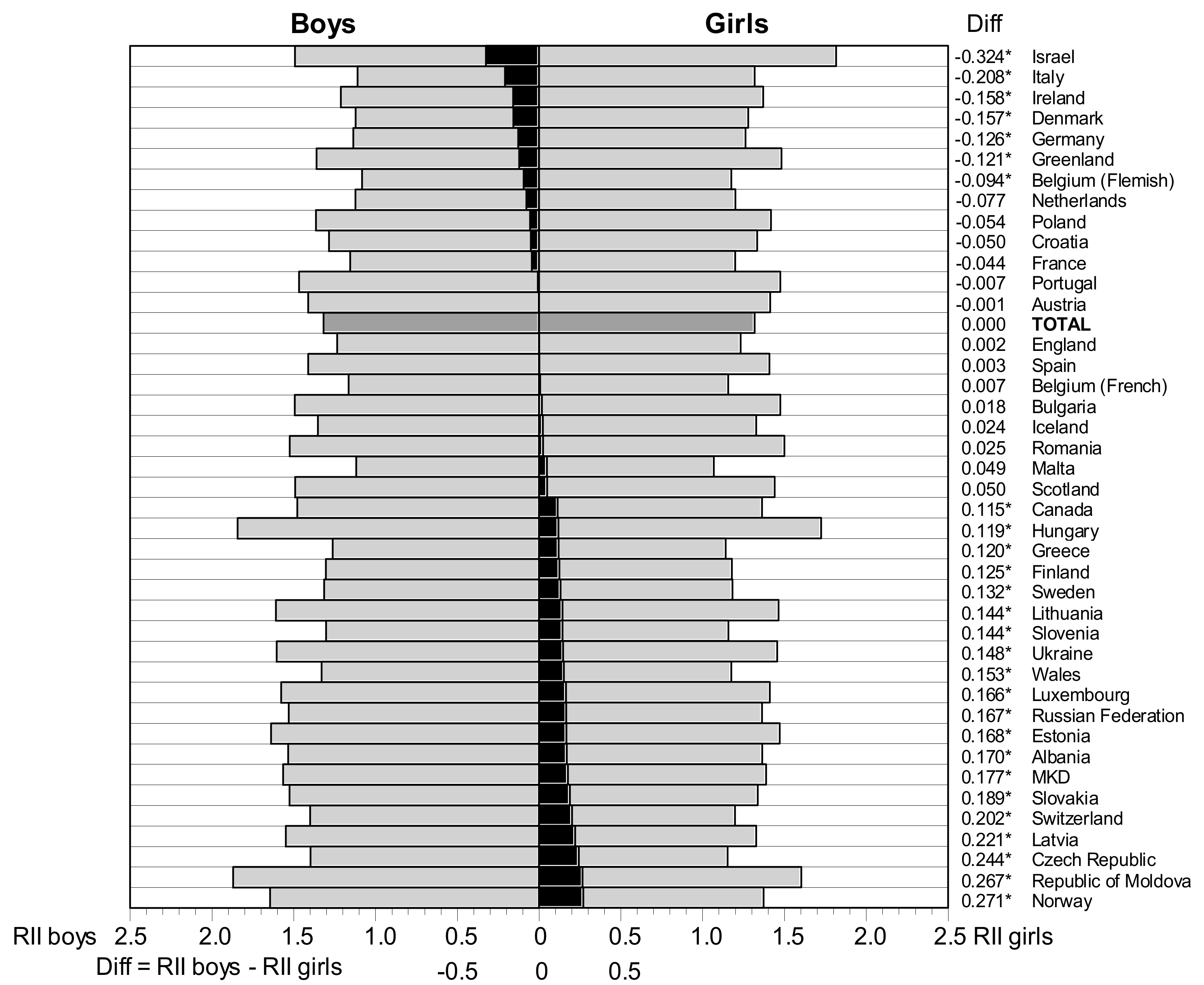
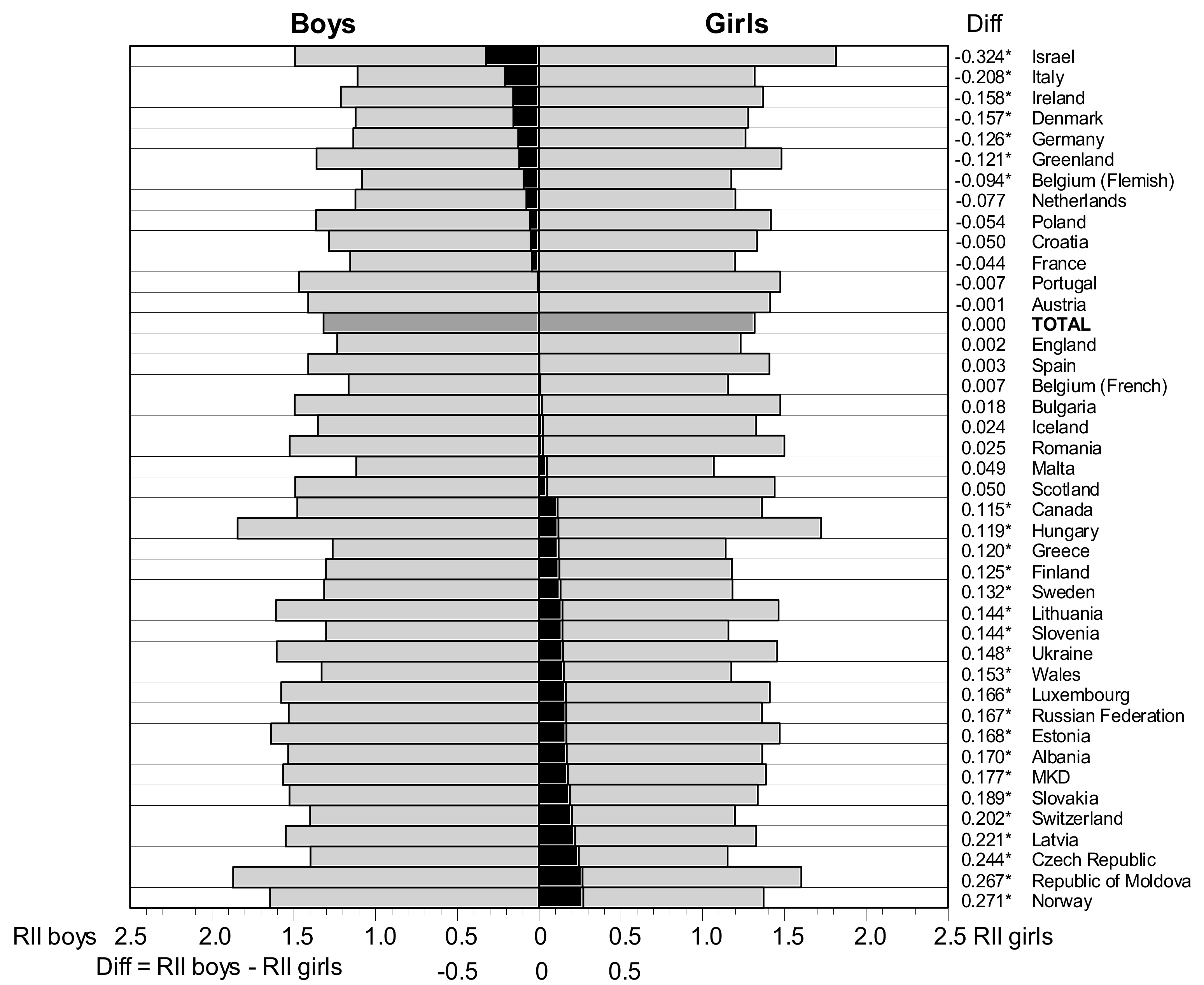
| Boys b | 1.318 (1.303–1.333) | Belgium (Flemish) | 1.082 (0.988–1.186) | Republic of Moldova | 1.870 (1.671–2.094) |
| Italy | 1.110 (1.000–1.232) | Hungary | 1.843 (1.653–2.055) | ||
| Malta | 1.118 (0.953–1.311) | Norway | 1.644 (1.427–1.893) | ||
| Girls b | 1.318 (1.299–1.337) | Malta | 1.069 (0.936–1.221) | Israel | 1.816 (1.697–2.003) |
| Greece | 1.141 (1.034–1.259) | Hungary | 1.724 (1.558–1.908) | ||
| Czech Republic | 1.153 (1.063–1.251) | Republic of Moldova | 1.603 (1.433–1.792) | ||
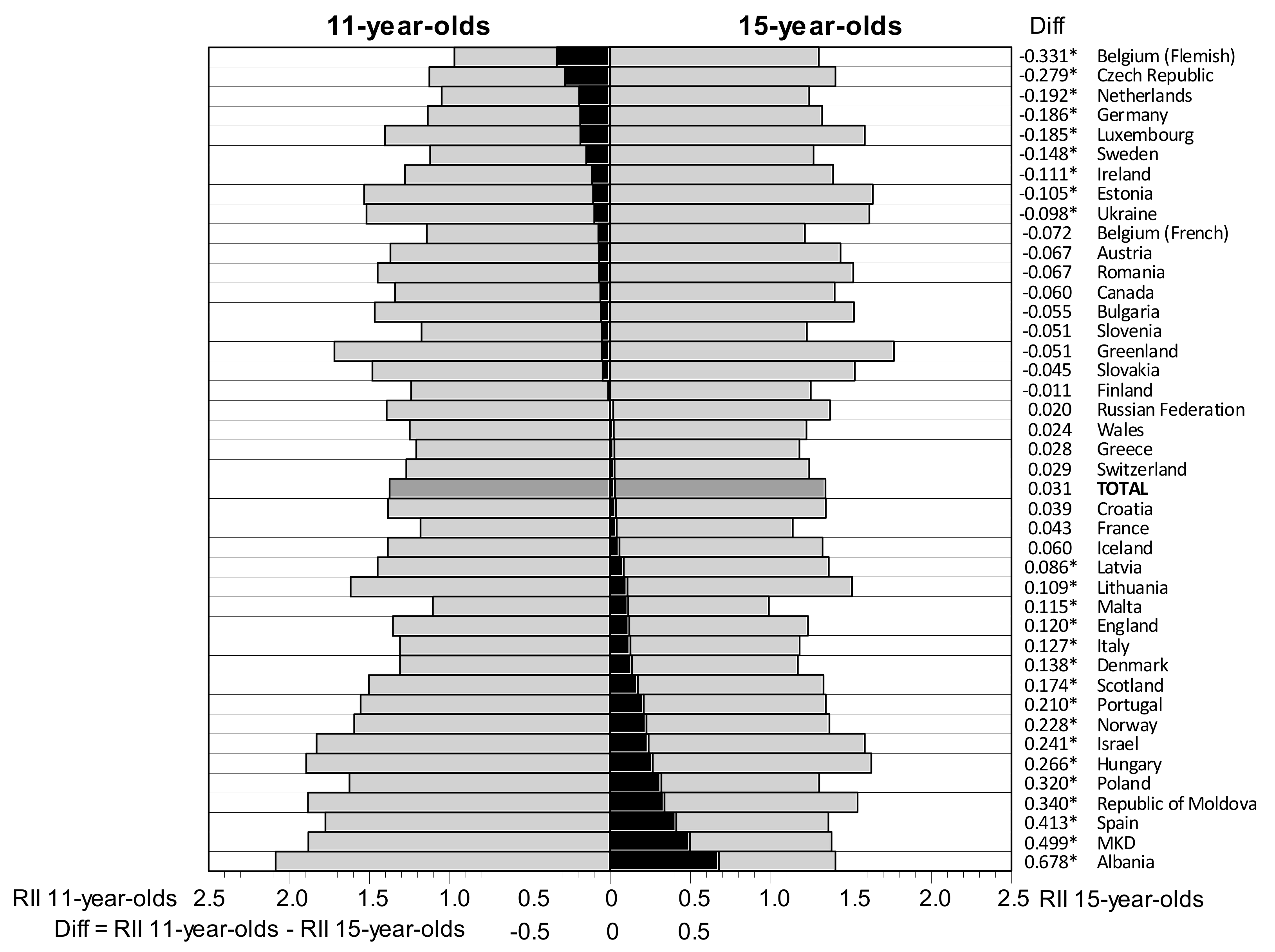
| 11-year-olds c | 1.373 (1.344–1.403) | Belgium (Flemish) | 0.969 (0.863–1.089) | Albania | 2.082 (1.784–2.430) |
| Netherlands | 1.049 (0.904–1.217) | Hungary | 1.893 (1.650–2.172) | ||
| Malta | 1.104 (0.900–1.354) | Republic of Moldova | 1.881 (1.612–2.193) | ||
| 13-year-olds c | 1.324 (1.301–1.348) | Greenland | 1.034 (0.779–1.373) | Hungary | 1.845 (1.632–2.085) |
| Belgium (Flemish) | 1.050 (0.916–1.203) | Republic of Moldova | 1.830 (1.600–2.094) | ||
| Belgium (French) | 1.116 (1.008–1.236) | Israel | 1.628 (1.433–1.850) | ||
| 15-year-olds c | 1.342 (1.320–1.366) | Malta | 0.989 (0.835–1.171) | Greenland | 1.768 (1.332–2.346) |
| France | 1.138 (1.029–1.259) | Estonia | 1.637 (1.449–1.850) | ||
| Denmark | 1.170 (1.032–1.326) | Hungary | 1.627 (1.434–1.846) | ||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zaborskis, A.; Grincaite, M. Gender and Age Differences in Social Inequality on Adolescent Life Satisfaction: A Comparative Analysis of Health Behaviour Data from 41 Countries. Int. J. Environ. Res. Public Health 2018, 15, 1297. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15071297
Zaborskis A, Grincaite M. Gender and Age Differences in Social Inequality on Adolescent Life Satisfaction: A Comparative Analysis of Health Behaviour Data from 41 Countries. International Journal of Environmental Research and Public Health. 2018; 15(7):1297. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15071297
Chicago/Turabian StyleZaborskis, Apolinaras, and Monika Grincaite. 2018. "Gender and Age Differences in Social Inequality on Adolescent Life Satisfaction: A Comparative Analysis of Health Behaviour Data from 41 Countries" International Journal of Environmental Research and Public Health 15, no. 7: 1297. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15071297