Incorporating Spatial Statistics into Examining Equity in Health Workforce Distribution: An Empirical Analysis in the Chinese Context


Abstract
:1. Introduction
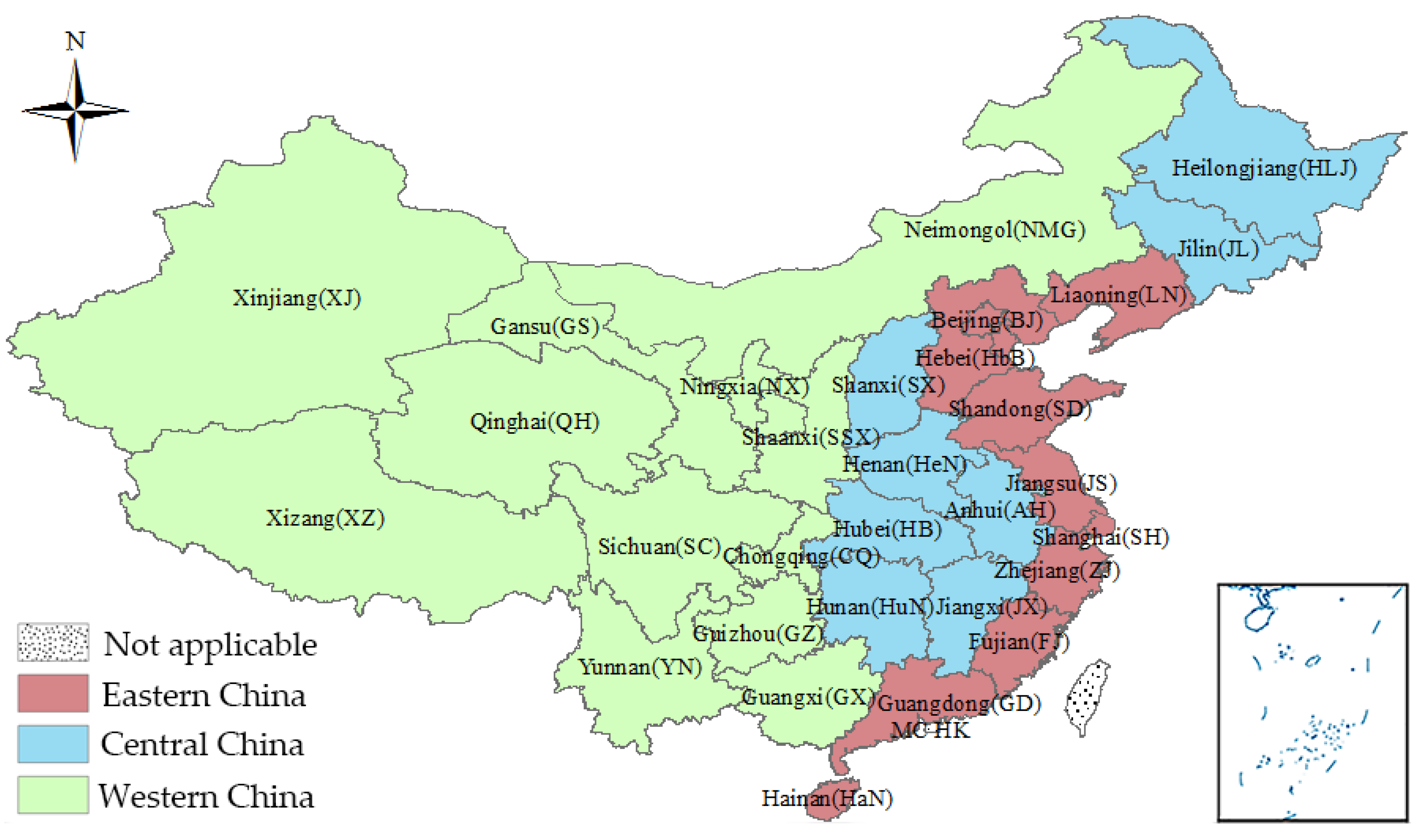
2. Health Workforce Distribution in China
3. Data and Methods
3.1. Data Resource and Indicators
3.2. Traditional Economic Method—Theil Index
- : proportion of population in one area accounting for the total population;
- : proportion of health workforce in one area accounting for the total health workforce.
- : degree of equity in health workforce distribution within the group.
- : degree of equity in health workforce distribution between the groups.
- : Theil index of health workforce distribution in subgroups.
- : proportion of population in one group accounting for the total population.
- : proportion of health workforce in one group accounting for the total health workforce.
3.3. Spatial Statistics
3.3.1. Global Moran’s I
3.3.2. Spatial Classification
3.3.3. Local Moran’s I
3.4. Software Tool
4. Results
4.1. Dynamics of Health Workforce Density
4.2. Theil Index of Health Workforce Distribution
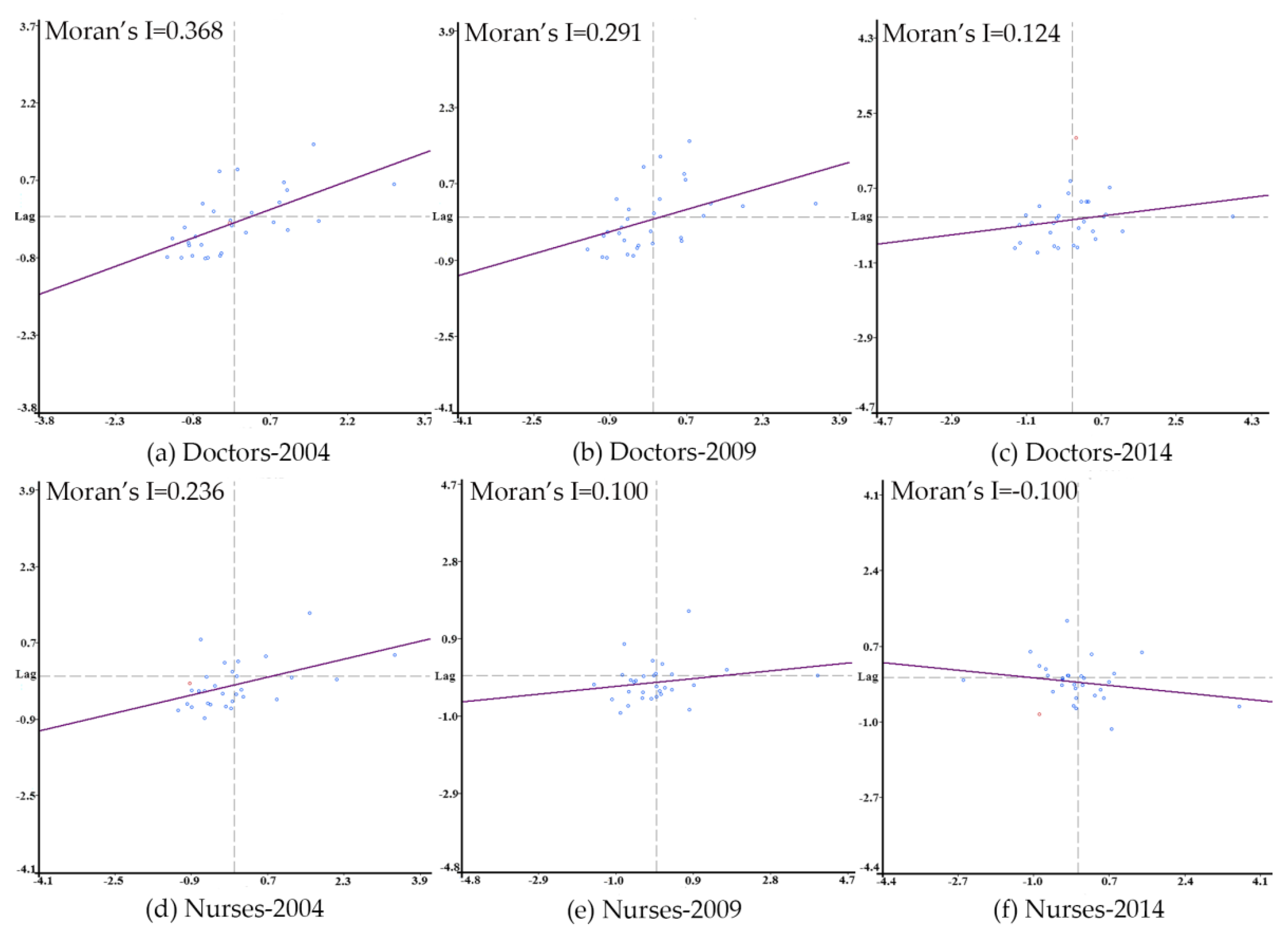
4.3. Global Spatial Autocorrelation
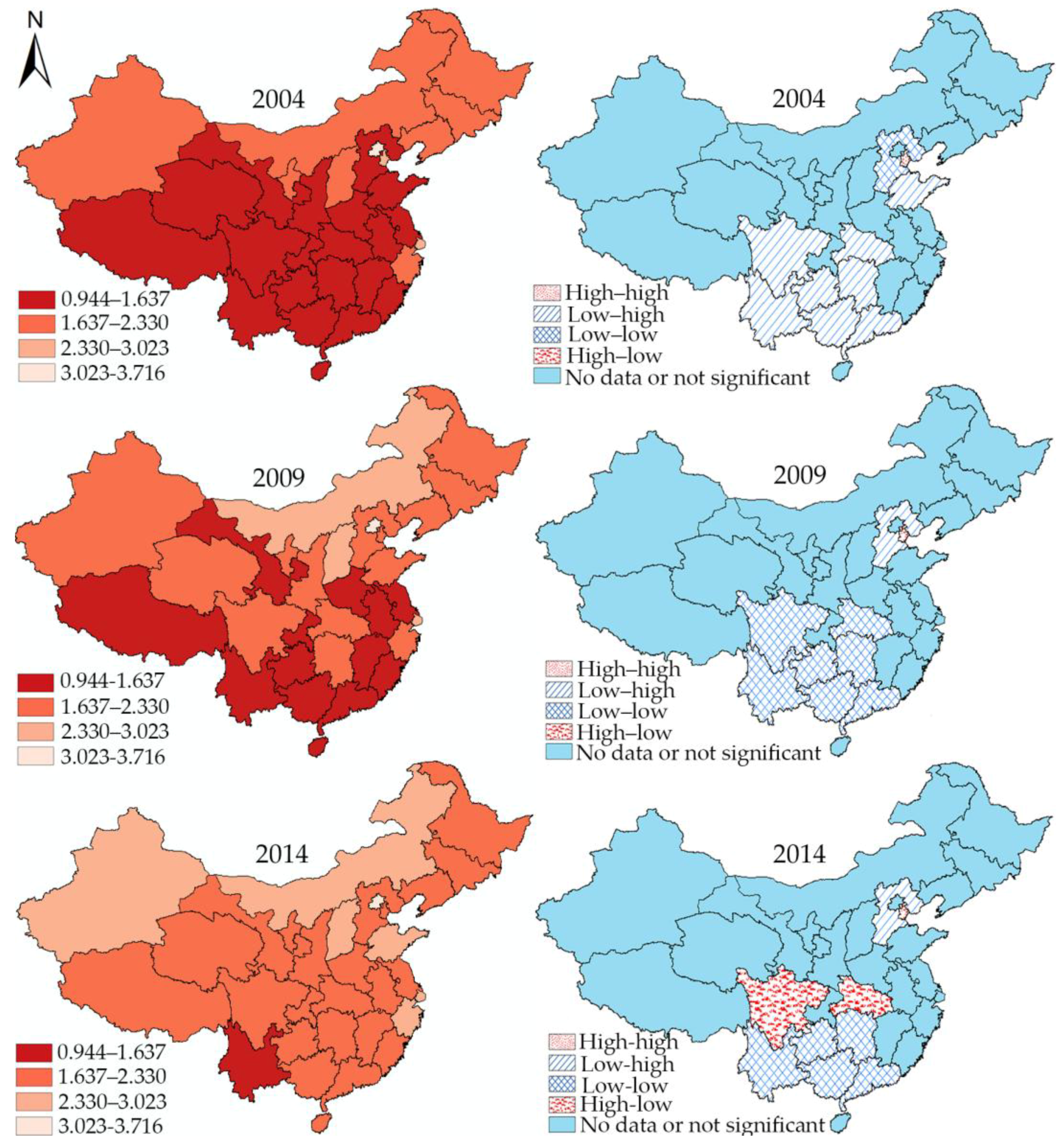
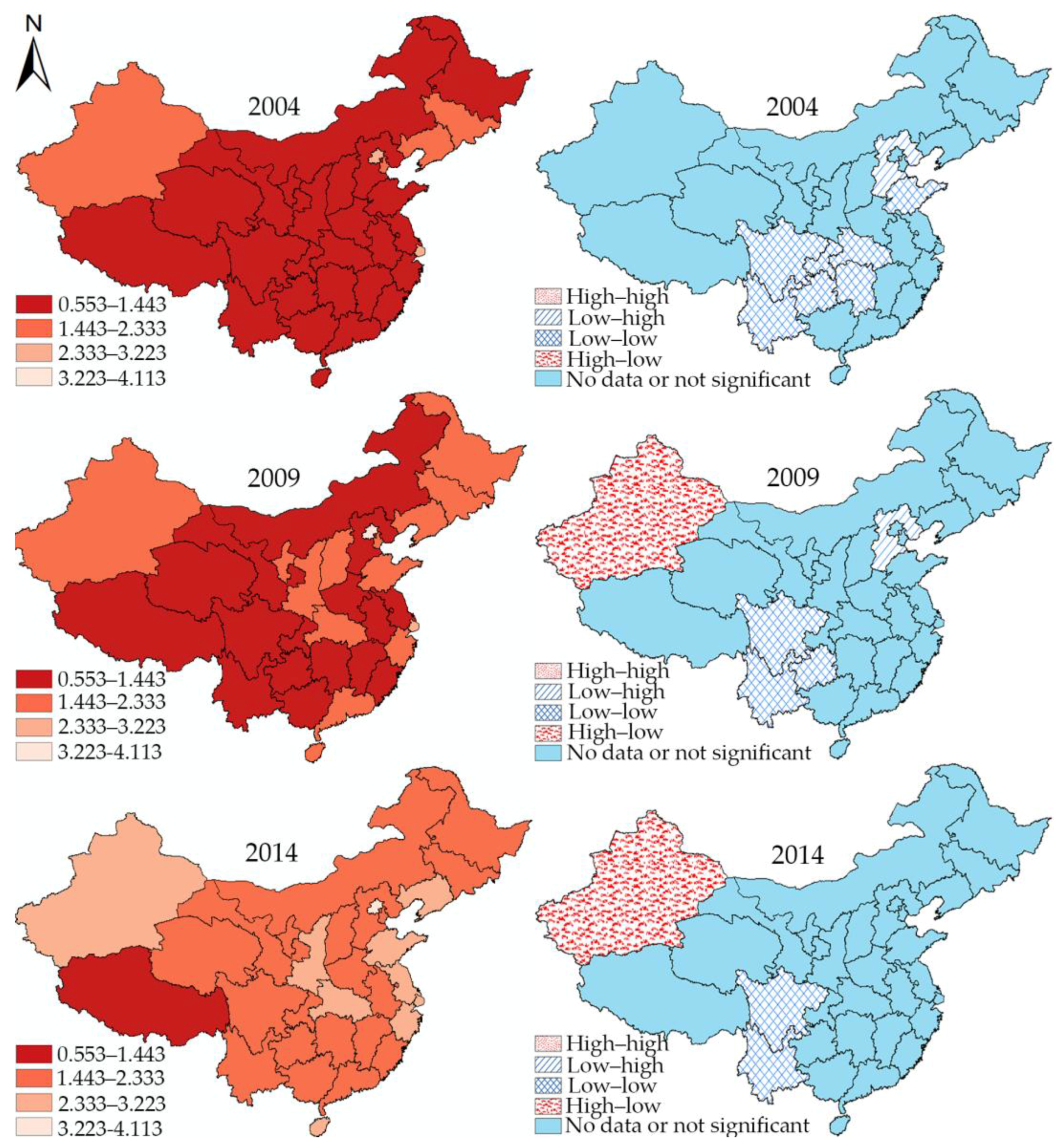
4.4. Spatial Classification
4.5. Local Spatial Autocorrelation
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Waters, H.R. Measuring equity in access to health care. Soc. Sci. Med. 2000, 51, 599–612. [Google Scholar] [CrossRef]
- WHO. Closing the gap in a generation: Health equity through action on the social determinants of health. Lancet 2008, 372, 1661–1669. [Google Scholar]
- Shadmi, E.; Wong, W.C.W.; Kinder, K.; Heath, I.; Kidd, M. Primary care priorities in addressing health equity: Summary of the WONCA 2013 health equity workshop. Int. J. Equity Health 2014, 13. [Google Scholar] [CrossRef] [PubMed]
- Sheldon, T.A.; Smith, P.C. Equity in the allocation of health care resources. Health Econ. 2000, 9, 571–574. [Google Scholar] [CrossRef]
- Culyer, A.J.; Wagstaff, A. Equity and equality in health and health care. J. Health Econ. 1993, 12, 431–457. [Google Scholar] [CrossRef]
- Braveman, P. Health disparities and health equity: Concepts and measurement. Annu. Rev. Public Health 2006, 27, 167–194. [Google Scholar] [CrossRef] [PubMed]
- Kreng, V.B.; Yang, C.-T. The equality of resource allocation in health care under the national health insurance system in Taiwan. Health Policy 2011, 100, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Zhao, L.; Cui, Z.; Wang, Y. Study on equity and efficiency of health resources and services based on key indicators in China. PLoS ONE 2015, 10, 1–15. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Strategy on Human Resources for Health: Workforce 2030; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Tao, Y.; Henry, K.; Zou, Q.; Zhong, X. Methods for measuring horizontal equity in health resource allocation: a comparative study. Health Econ. Rev. 2014, 4. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Zhao, Y.; Du, J.; Wu, T.; Huang, Y.; Guo, A. Health workforce equity in urban community health service of China. PLoS ONE 2014, 9, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Kanchanachitra, C.; Lindelow, M.; Johnston, T.; Hanvoravongchai, P.; Lorenzo, F.M.; Huong, N.L.; Wilopo, S.A.; Dela Rosa, J.F. Human resources for health in southeast Asia: Shortages, distributional challenges, and international trade in health services. Lancet 2011, 377, 769–781. [Google Scholar] [CrossRef]
- Anand, S.; Fan, V.Y.; Zhang, J.; Zhang, L.; Ke, Y.; Dong, Z.; Chen, L.C. China’s human resources for health: quantity, quality, and distribution. Lancet 2008, 372, 1774–1781. [Google Scholar] [CrossRef]
- Song, P.; Ren, Z.; Chang, X.; Liu, X.; An, L. Inequality of paediatric workforce distribution in China. Int. J. Environ. Res. Public Health 2016, 13, 703. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Liu, Y.; Twum, P.; Li, S. National equity of health resource allocation in China: Data from 2009 to 2013. Int. J. Equity Health 2016, 15. [Google Scholar] [CrossRef] [PubMed]
- Dussault, G.; Franceschini, M.C. Not enough there, too many here: Understanding geographical imbalances in the distribution of the health workforce. Hum. Resour. Health 2006, 4, 12. [Google Scholar] [CrossRef] [PubMed]
- Scott, L.M.; Janikas, M.V. Spatial statistics in ArcGIS. In Handbook of Applied Spatial Analysis; Springer: Berlin, Germany, 2010. [Google Scholar]
- Cromley, E.K.; McLafferty, S.L. GIS and Public Health, 2nd ed.; Guilford Press: New York, NY, USA, 2003. [Google Scholar]
- Krieger, N. Place, space, and health: GIS and epidemiology. Epidemiology 2003, 14, 384–385. [Google Scholar] [CrossRef] [PubMed]
- Sloan, C.D.; Jacquez, G.M.; Gallagher, C.M.; Ward, M.H.; Raaschou-Nielsen, O.; Nordsborg, R.B.; Meliker, J.R. Performance of cancer cluster Q-statistics for case-control residential histories. Spat. Spatiotemporal. Epidemiol. 2012, 3, 297–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, B.; Liu, J.; Fu, Y.; Zhang, B.; Mao, Y. Spatio-temporal epidemiology of viral hepatitis in China (2003–2015): Implications for prevention and control policies. Int. J. Environ. Res. Public Health 2018, 15, 661. [Google Scholar] [CrossRef] [PubMed]
- Zhu, B.; Fu, Y.; Liu, J.; Mao, Y. Modeling the dynamics and spillovers of the health labor market: Evidence from China’s provincial panel data. Sustainability 2018, 10, 333. [Google Scholar] [CrossRef]
- National Health and Family Planning Commission of the PRC. Long-Term Medical Personnel Development Plan (2011–2020); National Health and Family Planning Commission of the PRC: Beijing, China, 2011.
- National Health and Family Planning Commission of the PRC. China Health and Family Planning Statistical Yearbook 2017; Chinese Peking Union Medical College Press: Beijing, China, 2017.
- Doull, L.; Campbell, F. Human resources for health in fragile states. Lancet 2008, 371, 626–627. [Google Scholar] [CrossRef]
- Chen, L.; Evans, T.; Anand, S.; Ivey Boufford, J.; Brown, H.; Chowdhury, M.; Cueto, M.; Dare, L.; Dussault, G.; Elzinga, G.; et al. Human resources for health: Overcoming the crisis. Lancet 2004, 364, 1984–1990. [Google Scholar] [CrossRef]
- World Health Organization. World Health Statistics 2017; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Zhou, K.; Zhang, X.; Ding, Y.; Wang, D.; Lu, Z.; Yu, M. Inequality trends of health workforce in different stages of medical system reform (1985–2011) in China. Hum. Resour. Health 2015, 13. [Google Scholar] [CrossRef] [PubMed]
- Starfield, B. Improving equity in health: A research agenda. Int. J. Health Serv. 2001, 31, 545–566. [Google Scholar] [CrossRef] [PubMed]
- Jacob, B.G.; De Alwiss, R.; Caliskan, S.; Griffith, D.A.; Gunawardena, D.; Novak, R.J. A random-effects regression specification using a local intercept term and a global mean for forecasting malarial Prevalance. Am. J. Comput. Appl. Math. 2013, 3, 49–67. [Google Scholar]
- Zhu, B.; Fu, Y.; Liu, J.; Mao, Y. Notifiable sexually transmitted infections in China: Epidemiologic trends and spatial changing patterns. Sustainability 2017, 9, 1784. [Google Scholar] [CrossRef]
- Li, Q.; Song, J.; Wang, E.; Hu, H.; Zhang, J.; Wang, Y. Economic growth and pollutant emissions in China: A spatial econometric analysis. Stoch. Environ. Res. Risk Assess. 2014, 28, 429–442. [Google Scholar] [CrossRef]
- Hao, Y.; Liu, Y.M. The influential factors of urban PM2.5 concentrations in China: A spatial econometric analysis. J. Clean. Prod. 2016, 112, 1443–1453. [Google Scholar] [CrossRef]
- Travnikar, T.; Juvancic, L. A winding road from investment support to the economic growth of farms: Evidence from spatial econometric analysis of agricultural holdings in Slovenia. Bulg. J. Agric. Sci. 2015, 21, 16–25. [Google Scholar]
- Anselin, L. Local indicators of spatial association—Lisa. Geogr. Anal. 1995, 27, 93–115. [Google Scholar] [CrossRef]
- Chen, J.; Yang, S.; Li, H.; Zhang, B.; Lv, J. Research on geographical environment unit division based on the method of natural breaks (jenks). Remote Sens. Spat. Inf. Sci. 2013. [Google Scholar] [CrossRef]
- Rey, S.J. Spatial empirics for economic growth and convergence. Geogr. Anal. 2001, 33, 195–214. [Google Scholar] [CrossRef]
- Pietrzak, B.; Modifiable, T.; Unit, A. The modifiable areal unit problem—Analysis of correlation and regression. Q. J. Econ. Econ. Policy 2014, 9, 87–100. [Google Scholar] [CrossRef]
- Reardon, S.F.; O’Sullivan, D. Measures of spatial segregation. Sociol. Methodol. 2004, 34, 121–162. [Google Scholar] [CrossRef]
- Moraga, P.; Montes, F. Detection of spatial disease clusters with LISA functions. Stat. Med. 2011, 30, 1057–1071. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Region | Density of Doctors 1 | Density of Nurses | Average Growth Rate of Doctors | Average Growth Rate of Nurses | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 2004 | 2009 | 2014 | 2004 | 2009 | 2014 | 2004–2009 | 2009–2014 | 2004–2009 | 2009–2014 | |
| Eastern China | 1.64 | 1.88 | 2.30 | 1.19 | 1.58 | 2.37 | 2.7% | 4.1% | 5.8% | 8.4% |
| Beijing (BJ) | 3.29 | 3.58 | 3.72 | 2.78 | 3.52 | 4.11 | 1.7% | 0.7% | 4.8% | 3.2% |
| Tianjin (TJ) | 2.46 | 2.25 | 2.20 | 1.91 | 1.88 | 2.08 | −1.8% | −0.4% | −0.3% | 2.1% |
| Hebei (HeB) | 1.48 | 1.76 | 2.14 | 0.79 | 1.06 | 1.65 | 3.5% | 3.9% | 6.2% | 9.2% |
| Liaoning (LN) | 2.19 | 2.20 | 2.31 | 1.73 | 1.95 | 2.41 | 0.1% | 1.0% | 2.4% | 4.4% |
| Shanghai (SH) | 2.51 | 2.40 | 2.52 | 2.19 | 2.37 | 2.96 | −0.9% | 1.0% | 1.6% | 4.6% |
| Jiangsu (JS) | 1.43 | 1.60 | 2.24 | 1.04 | 1.42 | 2.37 | 2.4% | 6.9% | 6.5% | 10.8% |
| Zhejiang (ZJ) | 1.76 | 2.16 | 2.65 | 1.16 | 1.67 | 2.64 | 4.2% | 4.2% | 7.5% | 9.5% |
| Fujian (FJ) | 1.24 | 1.50 | 1.98 | 0.93 | 1.31 | 2.25 | 3.9% | 5.7% | 7.0% | 11.5% |
| Shandong (SD) | 1.51 | 1.86 | 2.36 | 1.05 | 1.47 | 2.51 | 4.3% | 4.9% | 7.1% | 11.2% |
| Guangdong (GD) | 1.36 | 1.59 | 2.02 | 1.11 | 1.51 | 2.18 | 3.2% | 4.9% | 6.4% | 7.5% |
| Central China | 1.38 | 1.70 | 2.01 | 0.94 | 1.33 | 2.06 | 4.3% | 3.4% | 7.2% | 9.1% |
| Shanxi (SX) | 2.05 | 2.47 | 2.46 | 1.23 | 1.67 | 2.17 | 3.8% | −0.1% | 6.3% | 5.3% |
| Jilin (JL) | 2.15 | 2.20 | 2.30 | 1.46 | 1.55 | 2.09 | 0.4% | 0.9% | 1.2% | 6.2% |
| Heilongjiang (HLJ) | 1.68 | 1.94 | 2.12 | 1.17 | 1.46 | 2.03 | 3.0% | 1.8% | 4.5% | 6.8% |
| Anhui (AH) | 1.00 | 1.38 | 1.71 | 0.70 | 1.14 | 1.83 | 6.7% | 4.3% | 10.4% | 9.9% |
| Jiangxi (JX) | 1.17 | 1.34 | 1.64 | 0.83 | 1.21 | 1.85 | 2.7% | 4.2% | 7.9% | 8.9% |
| Henan (HeN) | 1.13 | 1.59 | 2.01 | 0.77 | 1.18 | 2.03 | 7.2% | 4.7% | 9.0% | 11.4% |
| Hubei (HuB) | 1.49 | 1.71 | 2.17 | 1.10 | 1.53 | 2.48 | 2.8% | 4.9% | 6.8% | 10.2% |
| Hunan (HuN) | 1.34 | 1.65 | 1.98 | 0.86 | 1.30 | 2.02 | 4.2% | 3.7% | 8.5% | 9.3% |
| Western China | 1.36 | 1.66 | 1.99 | 0.85 | 1.21 | 2.12 | 4.0% | 3.7% | 7.4% | 11.8% |
| Neimenggu (NMG) | 2.10 | 2.82 | 2.48 | 1.11 | 1.44 | 2.26 | 6.0% | −2.5% | 5.3% | 9.5% |
| Guangxi (GX) | 1.09 | 1.38 | 1.82 | 0.89 | 1.29 | 2.19 | 4.7% | 5.8% | 7.9% | 11.1% |
| Chongqing (CQ) | 1.17 | 1.56 | 1.94 | 0.65 | 1.12 | 2.10 | 5.9% | 4.5% | 11.4% | 13.5% |
| Sichuan (SC) | 1.30 | 1.69 | 2.21 | 0.70 | 1.11 | 2.16 | 5.5% | 5.4% | 9.8% | 14.1% |
| Guizhou (GZ) | 0.94 | 1.17 | 1.65 | 0.55 | 0.90 | 1.92 | 4.4% | 7.1% | 10.3% | 16.2% |
| Yunnan (YN) | 1.21 | 1.32 | 1.60 | 0.83 | 1.01 | 1.76 | 1.9% | 3.9% | 4.1% | 11.6% |
| Xizang (XZ) | 1.59 | 1.53 | 1.76 | 0.67 | 0.68 | 0.85 | −0.7% | 2.8% | 0.0% | 4.8% |
| Shaanxi (SXX) | 1.61 | 1.87 | 2.03 | 1.01 | 1.47 | 2.58 | 3.0% | 1.6% | 7.8% | 11.8% |
| Gansu (GS) | 1.32 | 1.47 | 1.84 | 0.85 | 1.04 | 1.75 | 2.3% | 4.5% | 4.1% | 11.0% |
| Qinghai (QH) | 1.60 | 1.84 | 2.22 | 1.15 | 1.41 | 2.19 | 2.8% | 3.9% | 4.1% | 9.2% |
| Ningxia (NX) | 1.82 | 1.93 | 2.27 | 1.21 | 1.58 | 2.28 | 1.2% | 3.2% | 5.5% | 7.7% |
| Xinjiang (XJ) | 2.19 | 2.17 | 2.38 | 1.57 | 1.89 | 2.60 | −0.3% | 2.0% | 3.7% | 6.6% |
| SUM | 1.47 | 1.76 | 2.11 | 1.01 | 1.40 | 2.12 | 3.6% | 3.7% | 6.8% | 8.7% |
| Categories | Year | Theil Index | Contribution Rate | ||||
|---|---|---|---|---|---|---|---|
| Total | Western China | Central China | Eastern China | Within Groups | Among Groups | ||
| Doctors | 2004 | 0.032 | 0.028 | 0.029 | 0.028 | 87.5% | 12.5% |
| 2009 | 0.021 | 0.026 | 0.016 | 0.019 | 90.5% | 9.5% | |
| 2014 | 0.011 | 0.010 | 0.007 | 0.009 | 81.8% | 18.2% | |
| Nurses | 2004 | 0.048 | 0.034 | 0.026 | 0.049 | 77.1% | 22.9% |
| 2009 | 0.027 | 0.020 | 0.008 | 0.032 | 77.8% | 22.2% | |
| 2014 | 0.013 | 0.010 | 0.004 | 0.018 | 84.6% | 15.4% | |
| Year | Type | Number | Western China | Central China | Eastern China |
|---|---|---|---|---|---|
| 2004 | High–high | 7 | NX, NMG | HLJ, JL | BJ, LN, TJ |
| Low–high | 3 | GS | none | HeB, JS | |
| Low–low | 16 | GX, CQ, SC, GZ, YN, XZ, SXX, QH | HeN, HuB, AH, HuN, JX | SD, FJ, GD | |
| High–low | 4 | XJ | SX | SH, ZJ | |
| 2009 | High–high | 10 | SXX, NX, NMG | JL, SX, HLJ | TJ, SH, BJ, LN |
| Low–high | 3 | GS | none | JS, HeB | |
| Low–low | 15 | QH, GZ, GX, SC, YN, CQ, XZ | HeN, AH, JX, HuN, HuB | FJ, GD, SD | |
| High–low | 2 | XJ | none | ZJ | |
| 2014 | High–high | 8 | NMG | JL, SX | JS, SH, TJ, BJ, LN |
| Low–high | 5 | GS, SXX | AH, HLJ | HeB | |
| Low–low | 10 | XZ, GZ, YN, GX, CQ, | HeN, JX, HuN | GD, FJ | |
| High–low | 7 | NX, XJ, QH, SC | HuB | SD, ZJ |
| Year | Type | Number | Western China | Central China | Eastern China |
|---|---|---|---|---|---|
| 2004 | High–high | 5 | none | HLJ, JL | BJ, TJ, ZJ |
| Low–high | 3 | NMG | none | HeB, JS | |
| Low–low | 16 | GX, CQ, SC, GZ, YN, XZ, SXX, GS | HeN, HuB, AH, HuN, JX | SD, FJ, GD | |
| High–low | 6 | XJ, NX, QH | SX | SH, LN | |
| 2009 | High–high | 4 | none | JL | TJ, SH, ZJ |
| Low–high | 5 | GS, NMG | HLJ | JS, HeB | |
| Low–low | 12 | QH, GZ, GX, SC, YN, CQ, XZ | HeN, AH, JX, HuN | FJ | |
| High–low | 9 | XJ, SXX, NX | HuB, SX | BJ, SD, GD, LN | |
| 2014 | High–high | 4 | none | none | JS, SH, FJ, ZJ |
| Low–high | 7 | GS, CQ | AH, JL, JX | HeB, TJ | |
| Low–low | 11 | XZ, GZ, YN, GX, SC, QH | HeN, HLJ, HuN, SX | GD | |
| High–low | 8 | NX, XJ, NMG, SXX | HuB | SD, BJ, LN |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, B.; Hsieh, C.-W.; Zhang, Y. Incorporating Spatial Statistics into Examining Equity in Health Workforce Distribution: An Empirical Analysis in the Chinese Context. Int. J. Environ. Res. Public Health 2018, 15, 1309. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15071309
Zhu B, Hsieh C-W, Zhang Y. Incorporating Spatial Statistics into Examining Equity in Health Workforce Distribution: An Empirical Analysis in the Chinese Context. International Journal of Environmental Research and Public Health. 2018; 15(7):1309. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15071309
Chicago/Turabian StyleZhu, Bin, Chih-Wei Hsieh, and Yue Zhang. 2018. "Incorporating Spatial Statistics into Examining Equity in Health Workforce Distribution: An Empirical Analysis in the Chinese Context" International Journal of Environmental Research and Public Health 15, no. 7: 1309. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15071309