Effect of an Intervention Program Based on Active Video Games and Motor Games on Health Indicators in University Students: A Pilot Study

 , , , and
, , , and 
Abstract
:1. Introduction
1.1. Theoretical Framework
1.2. State of the Question
- Hypothesis 1 (H1): The basic descriptive will show a higher prevalence of lean mass and VO2max in men. Women will present greater flexibility and adherence to the Mediterranean diet. The problematic use of video games will be more widespread in men. Women will be more resilient.
- Hypothesis 2 (H2): The intervention program will improve the percentage of fat and lean mass, VO2max and the flexibility of university students.
- Hypothesis 3 (H3): After the intervention program the problematic use of video games will decrease and it will improve the levels of resilience and adherence to the Mediterranean diet.
2. Materials and Methods
2.1. Subjects and Design
2.2. Measures
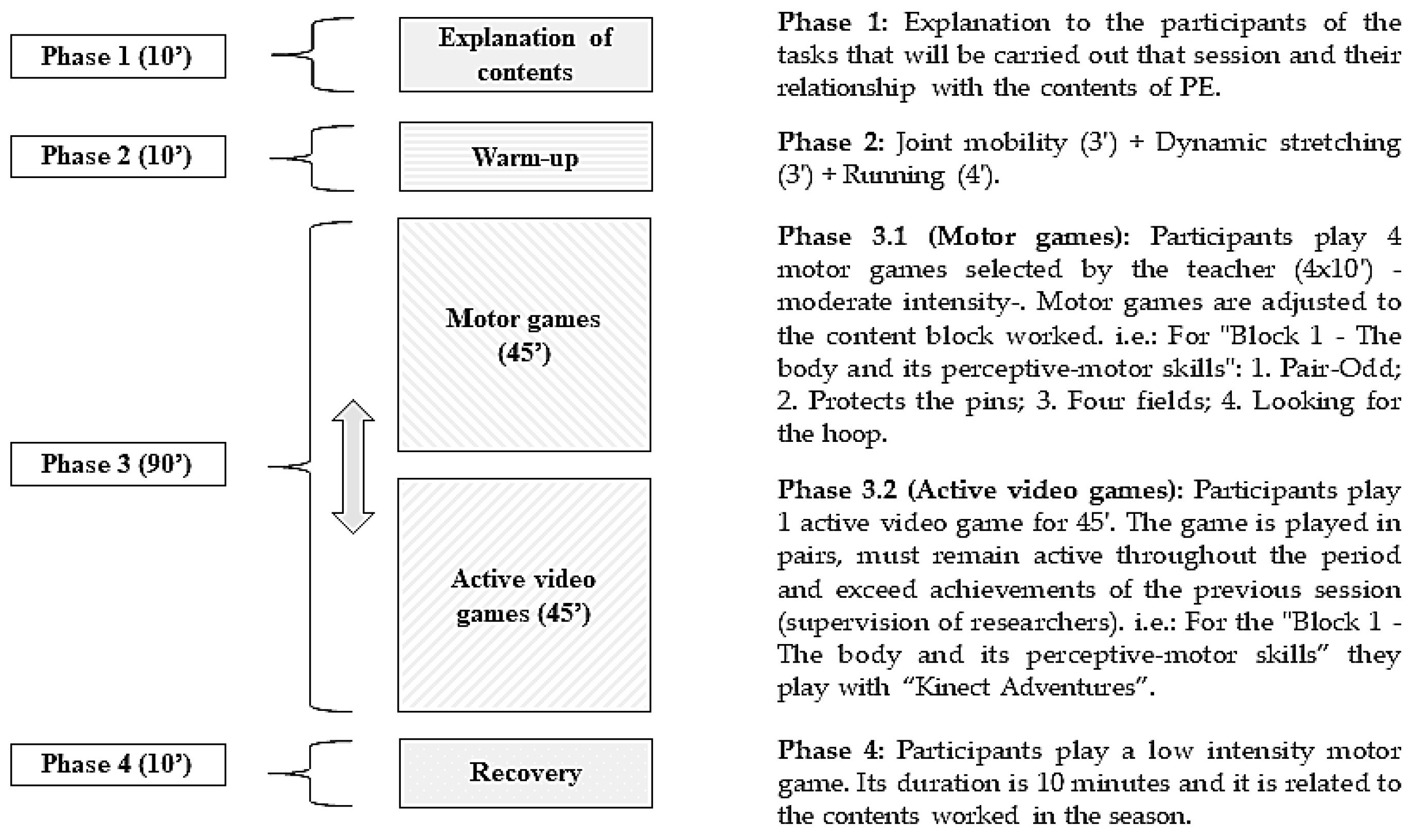
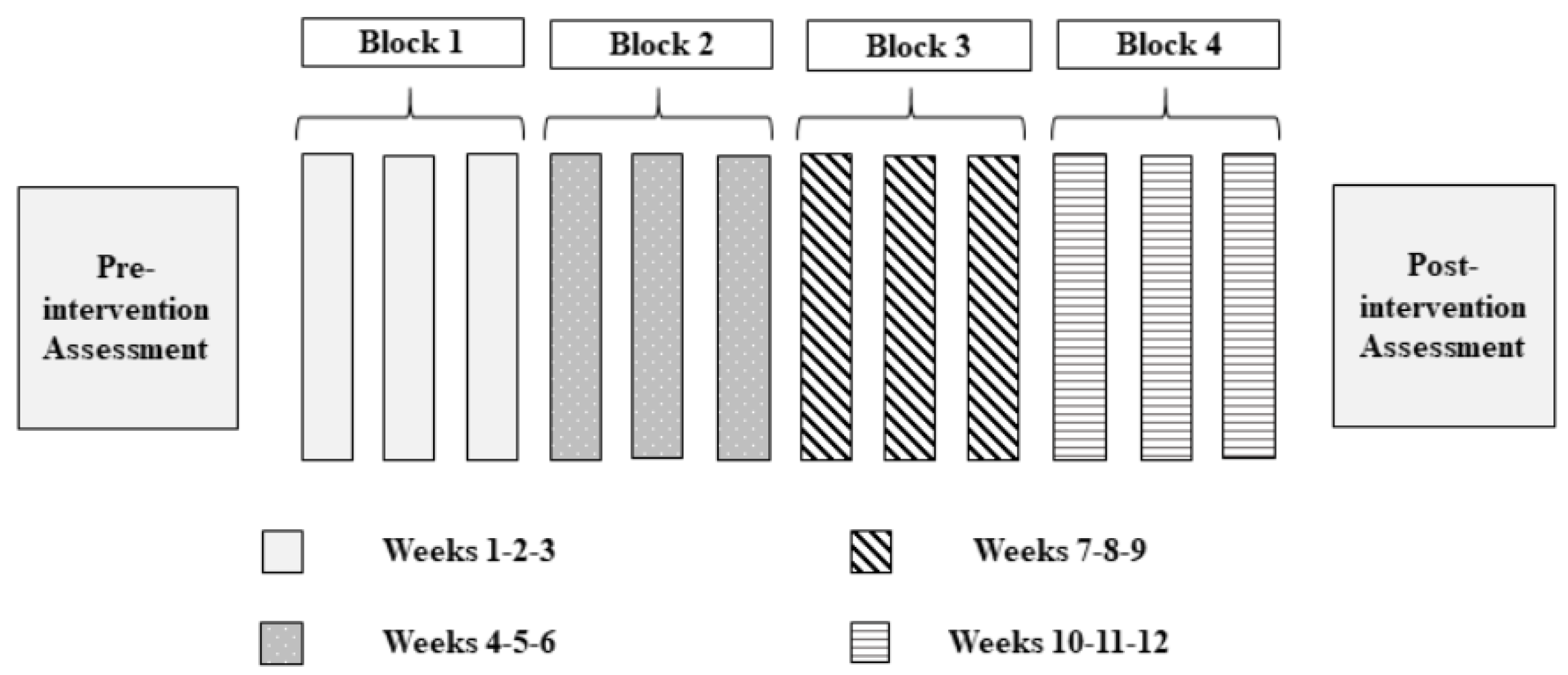
2.3. Procedure
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
- Hypothesis 1 (H1) was partially fulfilled, since lean mass was higher in men and lower in women, observing the opposite tendency for fat mass. In addition, the problematic use of video games was higher in men. On the contrary, the levels of resilience were higher in men, as well as the quality of the diet—not fulfilling what was established.
- Hypothesis 2 (H2) was partially fulfilled. The intervention program improved the percentage of fat mass and VO2max. Nevertheless, the percentage of lean mass and flexibility did not improve.
- Hypothesis 3 (H3) was partially fulfilled, since the intervention through active video games improved the quality of the diet but did not decrease the problematic use of video games.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References and Notes
- Lovell, G.P.; Nash, K.; Sharman, R.; Lane, B.R. A cross-sectional investigation of depressive, anxiety, and stress symptoms and health-behavior participation in Australian university students. Nurs. Health Sci. 2015, 17, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Arnett, J.J. Adolescence and Emerging Adulthood. A Cultural Aproach, 5th ed.; Pearson: Boston, MA, USA, 2014. [Google Scholar]
- Martínez-Martínez, A.; San Román, S.; Zurita, F.; Fernández-Revelles, A.B.; Cachón, J.; Pérez-Navio, E. University or labor market: Preferences of Young people to their future by terminating bachelor studies and professional training. J. Sport Health Res. 2017, 9, 177–186. [Google Scholar]
- Chacón, R.; Zurita, F.; Castro, M.; Espejo, T.; Martínez, A.; Pérez, A.J. Motivational climate in sport and its relationship with digital sedentary leisure habits in university students. Saúde Soc. 2017, 26, 29–39. [Google Scholar] [CrossRef]
- Boxer, P.; Groves, C.; Docherty, M. Video games do indeed influence children and adolescents’ aggression, prosocial behaviour, and academic performance. A clearer reading of Ferguson. Perspect. Psychol. Sci. 2015, 10, 671–673. [Google Scholar] [CrossRef] [PubMed]
- Sanders, G.J.; Rebold, M.; Peacock, C.A.; Williamson, M.L.; Santo, A.S.; Barkley, J.E. The physiologic and behavioral implications of playing active and sedentary video games in a seated and standing position. Int. J. Exerc. Sci. 2014, 7, 194–201. [Google Scholar] [PubMed]
- Falbe, J.; Willett, W.C.; Rosner, B.; Field, A.E. Body mass index, new modes of TV viewing and active video games. Pediatr. Obes. 2017, 12, 406–413. [Google Scholar] [CrossRef] [PubMed]
- González-Valero, G.; Zurita-Ortega, F.; Puertas-Molero, P.; Chacón-Cuberos, R.; Espejo-Garcés, T.; Castro-Sánchez, M. Education for health: Implementation of the program “Sportfruits” in schools of Granada. SPORT TK 2017, 6, 137–146. [Google Scholar] [CrossRef]
- Rivera-Torres, I.; Floody-Munita, M.; Delgado-Floody, P.; Schifferli-Castro, I.; Osorio-Poblete, A.; Salazar, C.M. Nutritional status, cardiovascular health, VO2max and habits in university students: A comparison between two health promotion careers. Rev. Facul. Med. 2017, 65, 447–451. [Google Scholar] [CrossRef]
- Vicente-Rodríguez, G.; Rey-López, J.P.; Martín-Matillas, M.; Moreno, L.A.; Wärnberg, J.; Redondo, C.; Tercedor, P.; Delgado, M.; Marcos, A.; Castillo, M.; et al. Television watching, videogames, and excess of body fat in Spanish adolescents: The AVENA study. Nutrition 2008, 24, 654–662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beydoun, M.A.; Powell, L.M.; Chen, X.; Wang, Y. Food Prices Are Associated with Dietary Quality, Fast Food Consumption, and Body Mass Index among US Children and Adolescents–3. J. Nutr. 2010, 141, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Pardo, V.; Jiménez, D.; Guillén, M.; Benítez, J.D. Physical activity, fitness and adiposity: Immigrants versus spanish scholars. Int. J. Med. Phys. Act. Sport Sci. 2014, 14, 319–338. [Google Scholar]
- Muros, J.J.; Cofre-Bolados, C.; Arriscado, D.; Zurita, F.; Knox, E. Mediterranean diet adherence is associated with lifestyle, physical fitness, and mental wellness among 10-y-olds in Chile. Nutrition 2017, 35, 87–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moljord, I.E.; Moksnes, U.K.; Espnes, G.A.; Hjemdal, O.; Eriksen, L. Physical activity, resilience, and depressive symptoms in adolescence. Ment. Health Phys. Act. 2014, 7, 79–85. [Google Scholar] [CrossRef]
- Liu, D.W.; Fairweather-Schmidt, A.K.; Burns, R.A.; Roberts, R.M. The Connor-Davidson Resilience Scale: Establishing invariance between gender across the lifespan in a large community based study. J. Psychopathol. Behav. Assess. 2015, 37, 340–348. [Google Scholar] [CrossRef]
- Windle, G. What is resilience? A review and concept analysis. Rev. Clin. Gerontol. 2010, 21, 152–169. [Google Scholar] [CrossRef]
- Denovan, A.; Macaskill, A. Stress, resilience and leisure coping among university students: Applying the broaden-and-build theory. Leis. Stud. 2017, 36, 852–865. [Google Scholar] [CrossRef]
- Valdivia-Moral, P.; Zafra, E.; Zurita, F.; Castro-Sánchez, M.; Muros, J.J.; Cofre-Bolados, C. Anxiety levels in Chilean judo. J. Sport Health Res. 2016, 8, 129–138. [Google Scholar]
- Gao, Z.; Chen, S.; Pasco, D.; Pope, Z. A meta-analysis of active video games on health outcomes among children and adolescents. Obes. Rev. 2015, 16, 783–794. [Google Scholar] [CrossRef] [PubMed]
- Oh, Y.; Yang, S. Defining exergames & exergaming. In Proceedings of the Meaningful Play 2010, East Lansing, MI, USA, 21–23 October 2010; Volume 1, pp. 1–17. [Google Scholar]
- Kahlbaugh, P.E.; Sperandio, A.J.; Carlson, A.L.; Hauselt, J. Effects of playing Wii on well-being in the elderly: Physical activity, loneliness, and mood. Act. Adapt. Aging 2011, 35, 331–344. [Google Scholar] [CrossRef]
- Agmon, M.; Perry, C.K.; Phelan, E.; Demiris, G.; Nguyen, H.Q. A pilot study of Wii Fit exergames to improve balance in older adults. J. Geriatr. Phys. Ther. 2011, 34, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Sun, H. Impact of exergames on physical activity and motivation in elementary school students: A follow-up study. J. Sport Health Sci. 2013, 2, 138–145. [Google Scholar] [CrossRef]
- López-Sánchez, G.F.; Nicolás-López, J.; Díaz-Suárez, A. Effects of a program of intense physical activity on the body composition of adolescents from Murcia. SPORT TK 2016, 5, 83–88. [Google Scholar]
- Borrego-Balsalobre, G.F.; López-Sánchez, G.F.; Díaz-Suárez, A. Effects of a vigorous physical activity program in the endurance of primary school children. ATHLOS 2015, 8, 31–46. [Google Scholar]
- Maddison, R.; Foley, L.; Ni, C.; Jiang, Y.; Jull, A.; Prapavessis, H.; Hohepa, M.; Rodgers, A. Effects of active video games on body composition: A randomized controlled trial−. Am. J. Clin. Nutr. 2011, 94, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Gribbon, A.; McNeil, J.; Jay, O.; Tremblay, M.S.; Chaput, J.P. Active video games and energy balance in male adolescents: A randomized crossover trial−. Am. J. Clin. Nutr. 2015, 101, 1126–1134. [Google Scholar] [CrossRef] [PubMed]
- Taylor, L.M.; Kerse, N.; Frakking, T.; Maddison, R. Active video games for improving physical performance measures in older people: A meta-analysis. J. Geriatr. Phys. Ther. 2018, 41, 108–123. [Google Scholar] [CrossRef] [PubMed]
- Official Bulletin of the Junta de Andalucía (2015). Order of March 17, 2015, which develops the curriculum for Primary Education in Andalusia (BOJA, 2015).
- Organic Law 8/2013, of December 9, for the Improvement of Educational Quality (LOMCE, 2013).
- Chacón, R.; Castro, M.; Zurita, F.; Espejo, T.; Martínez, A. Active Videogames as ICT Tool in Physical Education Classroom: Research from Digital Leisure Parameters. Digit. Educ. Rev. 2016, 29, 113–123. [Google Scholar]
- Chacón, R.; Zurita, F.; Puertas, P.; Knox, E.; Cofré, C.; Viciana, V.; Muros, J.J. Relationship between Healthy Habits and Perceived Motivational Climate in Sport among University Students: A Structural Equation Model. Sustainability 2018, 10, 938. [Google Scholar] [CrossRef]
- Merino-Marban, R.; Mayorga-Vega, D.; Fernandez-Rodríguez, E.; Estrada, F.; Viciana, J. Effect of a physical education-based stretching programme on sit-andreach score and its posterior reduction in elementary schoolchildren. Eur. Phys. Educ. Rev. 2015, 21, 83–92. [Google Scholar] [CrossRef]
- Portao, J.; Bescós, R.; Irurtia, A.; Cacciatori, E.; Vallejo, L. Assessment of body fat in physically active young people: Anthropometry vs bioimpedance. Nutr. Hosp. 2009, 24, 529–534. [Google Scholar] [PubMed]
- Okorodudu, D.O.; Jumean, M.F.; Montori, V.M.; Romero-Corral, A.; Somers, V.K.; Erwin, P.J.; Lopez-Jimenez, F. Diagnostic performance of body mass index to identify obesity as defined by body adiposity: A systematic review and meta-analysis. Int. J. Obes. 2010, 34, 791–799. [Google Scholar] [CrossRef] [PubMed]
- Rey, O.; Maïano, C.; Nicol, C.; Mercier, C.S.; Vallier, J.M. Psycho-Physiological Responses of Obese Adolescents to an Intermittent Run Test Compared with a 20-M Shuttle Run. J. Sports Sci. Med. 2016, 15, 451–459. [Google Scholar] [PubMed]
- García, G.C.; Secchi, J.D. 20 meters shuttle run test with stages of one minute. An original idea that has lasted for 30 years. Apunt. Med. Sport 2014, 49, 93–103. [Google Scholar] [CrossRef]
- Leger, L.A.; Lambert, J. A maximal multistage 20-m shuttle run test to predict V˙ O2 max. Eur. J. Appl. Physiol. Occup. Physiol. 1982, 49, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Canda, A.S.; Gómez, A.; Heras, E. Evaluation of trunk flexibility through the drawer test in different sports modalities. Rev. Esp. Med. Educ. Fís. Dep. 2004, 13, 148–154. [Google Scholar]
- Serrá-Majem, L.; Ribas, L.; Ngo, J.; Ortega, R.M.; García, A.; Pérez-Rodrigo, C.; Aranceta, J. Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean diet quality index in children and adolescents. Publ. Health Nutr. 2004, 7, 931–935. [Google Scholar] [CrossRef]
- Chamarro, A.; Carbonell, X.; Manresa, J.M.; Muñoz-Mirallles, R.; Ortega-González, R.; López-Morrón, M.R.; Carme, B.M.; Pere, T.M. The Questionnaire of Experiences Associated with Video games (CERV): An instrument to detect the problematic use of video games in Spanish adolescents. Adicciones 2014, 26, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Connor, K.; Davidson, J. Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyachi, M.; Yamamoto, K.; Ohkawara, K.; Tanaka, S. METs in adults while playing active video games: A metabolic chamber study. Med. Sci. Sport Exerc. 2010, 42, 1149–1153. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988; pp. 87–109. [Google Scholar]
- Foley, L.; Jiang, Y.; Mhurchu, C.N.; Jull, A.; Prapavessis, H.; Rodgers, A.; Maddison, R. The effect of active video games by ethnicity, sex and fitness: Subgroup analysis from a randomised controlled trial. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Graf, D.L.; Pratt, L.V.; Hester, C.N.; Short, K.R. Playing active video games increases energy expenditure in children. Pediatrics 2009, 124, 534–540. [Google Scholar] [CrossRef] [PubMed]
- Trost, S.G.; Sundal, D.; Foster, G.D.; Lent, M.R.; Vojta, D. Effects of a pediatric weight management program with and without active video games: A randomized trial. JAMA Pediatr. 2014, 168, 407–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geer, E.B.; Shen, W. Gender differences in insulin resistance, body composition, and energy balance. Gender. Med. 2009, 6, 60–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrick-Ranson, G.; Hastings, J.L.; Bhella, P.S.; Shibata, S.; Fujimoto, N.; Palmer, D.; Boyd, K.; Levine, B.D. The effect of age-related differences in body size and composition on cardiovascular determinants of VO2max. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2012, 68, 608–616. [Google Scholar] [CrossRef] [PubMed]
- Zurita, F. Importance of flexor capacity and ligamentous hyperlaxity in the detection of school athletes. J. Sport Health Res. 2011, 3, 47–58. [Google Scholar]
- Espejo, T.; Chacón, R.; Castro, M.; Martínez, A.; Zurita, F.; Pinel, C. Descriptive analysis of the problematic use and habits of consumption of the video games with relation to the genre in university students. RELATEC 2015, 14, 86–93. [Google Scholar]
- Brunborg, G.S.; Mentzoni, R.A.; Frøyland, L.R. Is video gaming, or video game addiction, associated with depression, academic achievement, heavy episodic drinking, or conduct problems? J. Behav. Addict. 2014, 3, 27–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carbonell, X. The Internet Gaming Disorder in the DSM-5. Adicciones 2014, 26, 91–95. [Google Scholar] [CrossRef]
- Staiano, A.E.; Marker, A.M.; Beyl, R.A.; Hsia, D.S.; Katzmarzyk, P.T.; Newton, R.L. A randomized controlled trial of dance exergaming for exercise training in overweight and obese adolescent girls. Pediatr. Obes. 2017, 12, 120–128. [Google Scholar] [CrossRef] [PubMed]
- LeBlanc, A.G.; Chaput, J.P.; McFarlane, A.; Colley, R.C.; Thivel, D.; Biddle, S.J.; Maddison, R.; Leatherdale, S.T.; Tremblay, M.S. Active Video Games and Health Indicators in Children and Youth: A Systematic Review. PLoS ONE 2013, 8, e65351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bethea, T.C.; Berry, D.; Maloney, A.E.; Sikich, L. Pilot study of an active screen time game correlates with improved physical fitness in minority elementary school youth. Games Health Res. Dev. Clin. Appl. 2012, 1, 29–36. [Google Scholar] [CrossRef] [PubMed]
- McArdle, W.D.; Katch, F.I.; Katch, V.L. Exercise Physiology: Nutrition, Energy, and Human Performance; Lippincott Williams & Wilkins: New York, NY, USA, 2010; pp. 48–59. [Google Scholar]
- Roopchand-Martin, S.; Nelson, G.; Gordon, C.; Sing, S.Y. A pilot study using the XBOX Kinect for exercise conditioning in sedentary female university students. Technol. Health Care 2015, 23, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Schneider, K.L.; Ferrara, J.; Lance, B.; Karetas, A.; Druker, S.; Panza, E.; Olendzki, B.; Andersen, V.; Pbert, L. Acceptability of an online health videogame to improve diet and physical activity in elementary school students: “Fitter Critters”. Games Health Res. Dev. Clin. Appl. 2012, 1, 262–268. [Google Scholar] [CrossRef] [PubMed]
- Chaput, J.P.; Tremblay, A.; Pereira, B.; Boirie, Y.; Duclos, M.; Thivel, D. Food intake response to exercise and active video gaming in adolescents: Effect of weight status. Br. J. Nutr. 2016, 115, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Chaput, J.P.; Schwartz, C.; Boirie, Y.; Duclos, M.; Tremblay, A.; Thivel, D. Energy intake adaptations to acute isoenergetic active video games and exercise are similar in obese adolescents. Eur. J. Clin. Nutr. 2015, 69, 1267–1271. [Google Scholar] [CrossRef] [PubMed]
- Hartfiel, N.; Havenhand, J.; Khalsa, S.B.; Clarke, G.; Krayer, A. The effectiveness of yoga for the improvement of well-being and resilience to stress in the workplace. Scand. J. Work Environ. Health 2011, 37, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Lyons, E.J.; Tate, D.F.; Ward, D.S.; Ribisl, K.M.; Bowling, J.M.; Kalyanaraman, S. Engagement, enjoyment, and energy expenditure during active video game play. Health Psychol. 2014, 33, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Chacón-Cuberos, R.; Puertas-Molero, P.; Pérez-Cortés, A.J. Levels of resilience depending on practice of physical activity in university students. ESHPA Educ. Sport Health Phys. Act. 2017, 1, 59–67. [Google Scholar]
- Schumann, M.; Küüsmaa, M.; Newton, R.U.; Sirparanta, A.I.; Syväoja, H.; Häkkinen, A.; Häkkinen, K. Fitness and lean mass increases during combined training independent of loading order. Med. Sci. Sports Exerc. 2014, 46, 1758–1768. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Program Variables | Levene’s Test | T Test Sig. (Bilateral) | ||||
|---|---|---|---|---|---|---|
| Gender | M | SD | F | Sig. | ||
| Body Weight | Man | 74.87 | 11.21 | 0.910 | 0.344 | 0.001 * |
| Woman | 55.79 | 8.11 | ||||
| BMI | Man | 24.08 | 3.70 | 0.003 | 0.957 | 0.003 * |
| Woman | 21.09 | 3.41 | ||||
| Fat Mass | Man | 12.00 | 5.56 | 1.203 | 0.277 | 0.626 |
| Woman | 12.75 | 5.91 | ||||
| Lean Mass | Man | 62.84 | 6.55 | 10.936 | 0.002 | 0.001 * |
| Woman | 43.03 | 2.78 | ||||
| Flexibility | Man | 28.91 | 7.54 | 2.322 | 0.133 | 0.578 |
| Woman | 29.96 | 5.82 | ||||
| VO2max | Man | 51.12 | 12.79 | 0.301 | 0.586 | 0.001 * |
| Woman | 38.54 | 12.56 | ||||
| Diet | Man | 6.68 | 2.17 | 0.461 | 0.500 | 0.376 |
| Woman | 6.09 | 2.81 | ||||
| Video games | Man | 35.94 | 11.01 | 13.178 | 0.001 | 0.001 * |
| Woman | 24.52 | 5.43 | ||||
| Program Variables | Gender | M | SD | Levene’s Test | T Test Sig. (Bilateral) | |
|---|---|---|---|---|---|---|
| F | Sig. | |||||
| F1 | Man | 3.45 | 0.39 | 0.574 | 0.452 | 0.200 |
| Woman | 3.32 | 0.36 | ||||
| F2 | Man | 3.05 | 0.25 | 5.538 | 0.022 | 0.231 |
| Woman | 2.93 | 0.41 | ||||
| F3 | Man | 3.45 | 0.41 | 0.387 | 0.536 | 0.175 |
| Woman | 3.30 | 0.41 | ||||
| F4 | Man | 3.27 | 0.43 | 0.623 | 0.433 | 0.906 |
| Woman | 3.28 | 0.54 | ||||
| F5 | Man | 2.63 | 0.66 | 0.966 | 0.330 | 0.394 |
| Woman | 2.78 | 0.61 | ||||
| Program Variables | M | SD | T | Sig. | d | I.C. 95% | |
|---|---|---|---|---|---|---|---|
| Fat mass | (Pre-test) | 12.30 | 5.67 | 2.509 | 0.015 * | −0.11 | (−0.45–0.28) |
| (Post-test) | 11.83 | 5.28 | |||||
| Lean Mass | (Pre-test) | 54.85 | 11.15 | −0.821 | 0.415 | 0.03 | (−0.33–0.40) |
| (Post-test) | 55.22 | 11.09 | |||||
| Flexibility | (Pre-test) | 29.33 | 6.87 | 1.233 | 0.223 | −0.11 | (−0.48–0.25) |
| (Post-test) | 28.51 | 7.30 | |||||
| VO2max | (Pre-test) | 45.91 | 15.03 | −2.767 | 0.008 * | 0.13 | (−0.28–0.46) |
| (Post-test) | 47.19 | 13.53 | |||||
| RF1 | (Pre-test) | 3.40 | 0.38 | −0.712 | 0.479 | 0.08 | (−0.29–0.44) |
| (Post-test) | 3.43 | 0.41 | |||||
| RF2 | (Pre-test) | 3.00 | 0.33 | −3.360 | 0.001 * | 0.42 | (−0.02–0.76) |
| (Post-test) | 3.14 | 0.38 | |||||
| RF3 | (Pre-test) | 3.49 | 0.45 | −1.761 | 0.084 | 0.04 | (−0.32–0.41) |
| (Post-test) | 3.51 | 0.46 | |||||
| RF4 | (Pre-test) | 3.28 | 0.47 | −1.373 | 0.175 | 0.14 | (−0.23–0.51) |
| (Post-test) | 3.35 | 0.51 | |||||
| RF5 | (Pre-test) | 2.69 | 0.64 | 1.427 | 0.159 | −0.17 | (−0.53–0.20) |
| (Post-test) | 2.58 | 0.68 | |||||
| Video games | (Pre-test) | 31.33 | 10.71 | 0.204 | 0.839 | −0.02 | (−0.38–0.35) |
| (Post-test) | 31.14 | 11.70 | |||||
| Diet | (Pre-test) | 6.44 | 2.44 | −2.315 | 0.024 * | 0.32 | (−0.08–0.66) |
| (Post-test) | 7.11 | 2.20 | |||||
| Program Variables | Lean Mass | Flexibility | VO2max | Resilience | Video Games | Diet |
|---|---|---|---|---|---|---|
| Fat Mass | 0.236 | −0.296 * | −0.476 ** | −0.023 | −0.122 | −0.262 * |
| Lean Mass | −0.258 | 0.323 * | 0.314 * | 0.424 ** | 0.086 | |
| Flexibility | 0.142 | −0.144 | −0.127 | 0.018 | ||
| VO2max | 0.153 | 0.201 | 0.291 * | |||
| Resilience | 0.083 | −0.016 | ||||
| Video games | −0.076 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zurita-Ortega, F.; Chacón-Cuberos, R.; Castro-Sánchez, M.; Gutiérrez-Vela, F.L.; González-Valero, G. Effect of an Intervention Program Based on Active Video Games and Motor Games on Health Indicators in University Students: A Pilot Study. Int. J. Environ. Res. Public Health 2018, 15, 1329. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15071329
Zurita-Ortega F, Chacón-Cuberos R, Castro-Sánchez M, Gutiérrez-Vela FL, González-Valero G. Effect of an Intervention Program Based on Active Video Games and Motor Games on Health Indicators in University Students: A Pilot Study. International Journal of Environmental Research and Public Health. 2018; 15(7):1329. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15071329
Chicago/Turabian StyleZurita-Ortega, Félix, Ramón Chacón-Cuberos, Manuel Castro-Sánchez, Francisco Luis Gutiérrez-Vela, and Gabriel González-Valero. 2018. "Effect of an Intervention Program Based on Active Video Games and Motor Games on Health Indicators in University Students: A Pilot Study" International Journal of Environmental Research and Public Health 15, no. 7: 1329. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15071329