2.2. Measuring Geographic Accessibility to Elderly Community Care Resources
A widely used criterion for access to facilities classifies access based on geographic factors, thus emphasizing the spatial separation between supply and demand as a barrier or a facilitator, or non-geographic factors, which stress non-spatial barriers or facilitators [
29]. This study measures the geographic accessibility of elderly community care centers in Taiwan to investigate the equality of long-term care resources distribution.
Common measurements of geographic accessibility include travel time or distance between the demand population’s location and the facility and the number of suppliers in each administrative district [
30,
31,
32]. Using travel time to the nearest supplier to assess geographic accessibility may relate to the number of the service suppliers [
33]. Thus, using travel time to evaluate accessibility is not always a determining factor, since other factors such as facility capacity, insurance acceptance, and travel costs can affect access [
34].
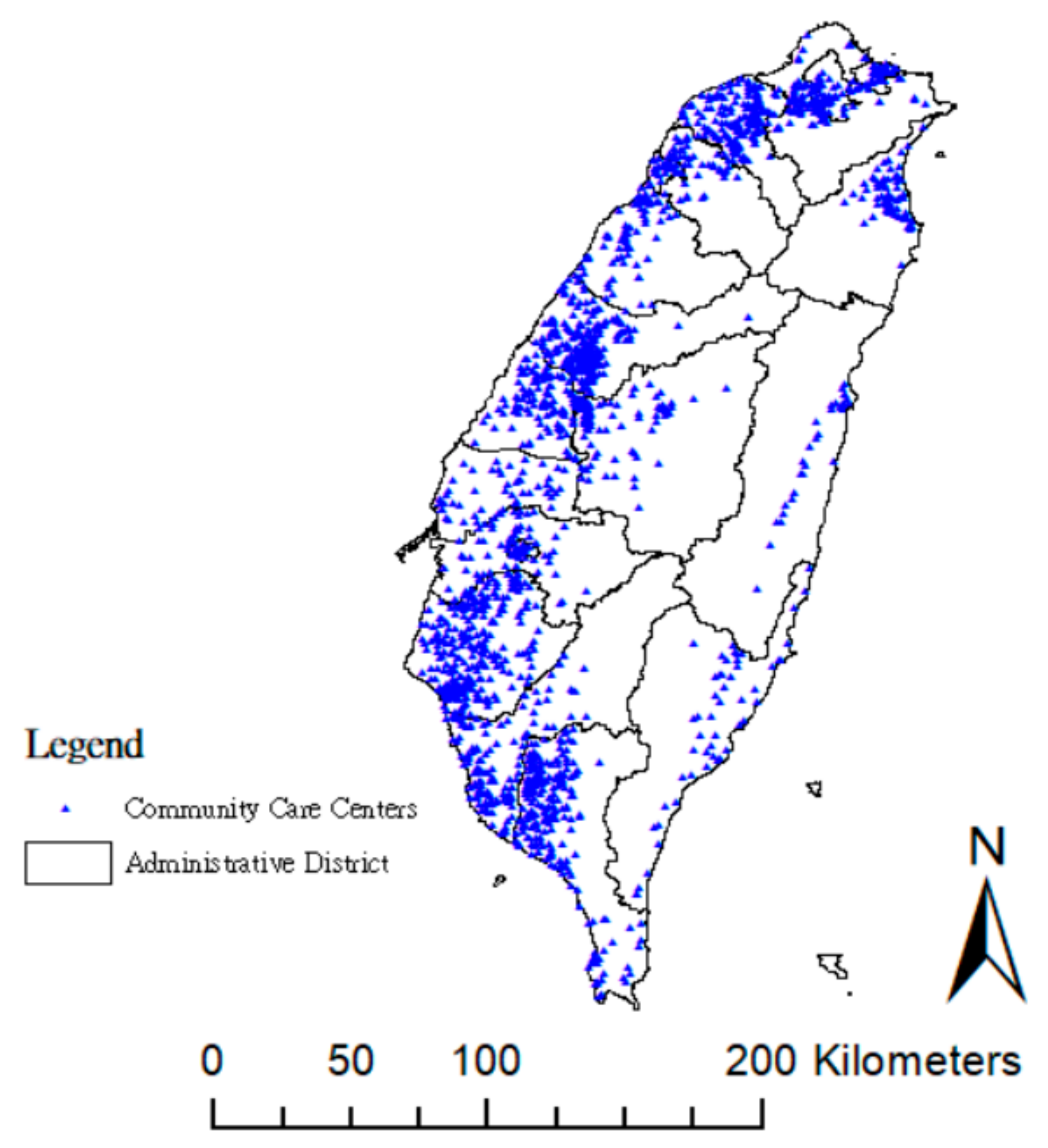
It is a complicated task to account for disparities in spatial relationships between the supply and demand sides. Thus, in this study, six accessibility measurements were evaluated to estimate levels of geographic accessibility from 7681 villages and 1941 elderly community care centers in Taiwan in 2017, taking into account both accounting factors of distance and the amount of community care centers, as well as supplier’ points (supplier loading) (
Table 1). The ESRI ArcGIS 10.5.1 (Esri, Redlands, CA, USA) “Model Builder” tool incorporated with the “Network Analyst extension” module and SQL programming from Microsoft SQL Server 2014 (Microsoft, Redmond, WA, USA) were used to calculate the accessibility measures.
The main goal of the Taiwanese government’s long-term care policy [
28] is to achieve “aging in place”, and its primary mission is to establish a good-quality neighborhood and a community-based accessible, affordable, universal, long-term care service system. To create a comprehensive care system that integrates medical care, long-term care services, housing, prevention, and social supports for the elderly within a 30-min drive, the system (“Long-Term Care 2.0,” 2017) includes “Tier A–Community integrated service centers”, “Tier B–Combined service centers”, and “Tier C–LTC stations around the blocks.” The basic executive unit (“Tier C–LTC stations around the blocks”) relies on village-level community care centers to satisfy the elderly’s accessibility. Restricted by governmental funding policy, the elderly can choose one community care center only within their census-registered county, and most choose the one with the shortest distance. Thus, all six methods estimate accessibility based on the assumption of the nearest road distance in this study.
Mxi (i.e., M1i, M3i, M4i, M5i, and M6i) is the score of geographic accessibility at the centroid of village i using method Mx. M2j is the score of supplier loading at the elderly community care center j using method M2. Sj is the capacity of the elderly community care center j. Si is the capacity of the elderly community care centers at the centroid of village i. Pi is the demand population over 65 years in village i, and dij is the road network travel distance between village i and the elderly community care center j.
Method M1 employed road network distance [
31] to measure the impact of travel time on geographic accessibility and estimated the within-jurisdiction road network travel distance from the centroid of each village to the nearest elderly community care center within every jurisdiction (i.e., county). Method M1 shows the real traffic distance between the elderly at every village and the nearest center within every county.
Method M2 estimated the nearest distance supplier loading within every county, whereby a larger score denoted lower geographic accessibility. For example, if the community care center is the common nearest supplier to several within-jurisdiction villages, summing up the total demand population at those nearby villages obtains the nearest supplier loading.
Method M3 measured the supplier–population ratio of the elderly community care centers within an “official region”, defined by village level in this study. As an easy and simple method to calculate the ratio, often, method M3 is used as a basic indicator to evaluate resource shortage areas; however, it has two disadvantages for evaluating geographic accessibility: it cannot explain the related spatial variations within a specific area, and it assumes that the demand population would not seek resources across the region’s borders [
35]. In other words, method M3 assumes that the elderly in a specific area have equal opportunity to acquire resources regardless of the travel distance.
A comprehensive accessibility measure should include possible influencing factors for the elderly’s access to these community care resources, and methods M4–M6 simultaneously account for the demand population of villages, supplier capacity, supplier loading, and distance. Methods M4–M6 consider the different distance-decay function to estimate the impact of different distance scales (
Table 1), since the elderly’s physical activity can be restricted by these. For each factors’ weights are not known, and there are no surveys that have been done to estimate the importance of these factors. We applied “equal weighting” method to minimize maximum possible disagreement over all possible distributions [
36].
Methods M4 and M5 assume that the nearest community care center is always accessible whatever the nearest distance scale for the elderly within each county—that is, the elderly in each village can access the nearest resources; however, this neglects the travel distance-decay factor in elderly walkability. Method M4 calculated the nearest distance-decay effect by considering within-jurisdiction accessible resources and the nearest road distances to estimate accessibility. Method M5 estimated accessibility by additionally considering the supplier’s loading, such that the elderly population of villages near the common elderly community center were summed up and were considered as sharing that center’s resources. Thus, method M5 can enhance the assessment of the adequacy of resource allocation.
Walkability is a measure of how friendly an area is to walking. Often, the elderly are disadvantaged in terms of mobility; thus, method M6 is based on the same concept as method M5, but also accounts for elderly walkability. The walkable accessibility of community-based care resources can improve the elderly’s health and aging in place. Although walking seems like a simple activity, it is actually a complex symphony involving many of the body’s systems, whereby our bodies must coordinate balance, muscle contraction, and relaxation, as well as adjust the cardiovascular system. Therefore, a friendly, community-based elderly care center should consider the elderly’s neighborhood walkability and physical abilities [
27,
37]. The appropriate walking speed for older pedestrians is 0.91 m/s [
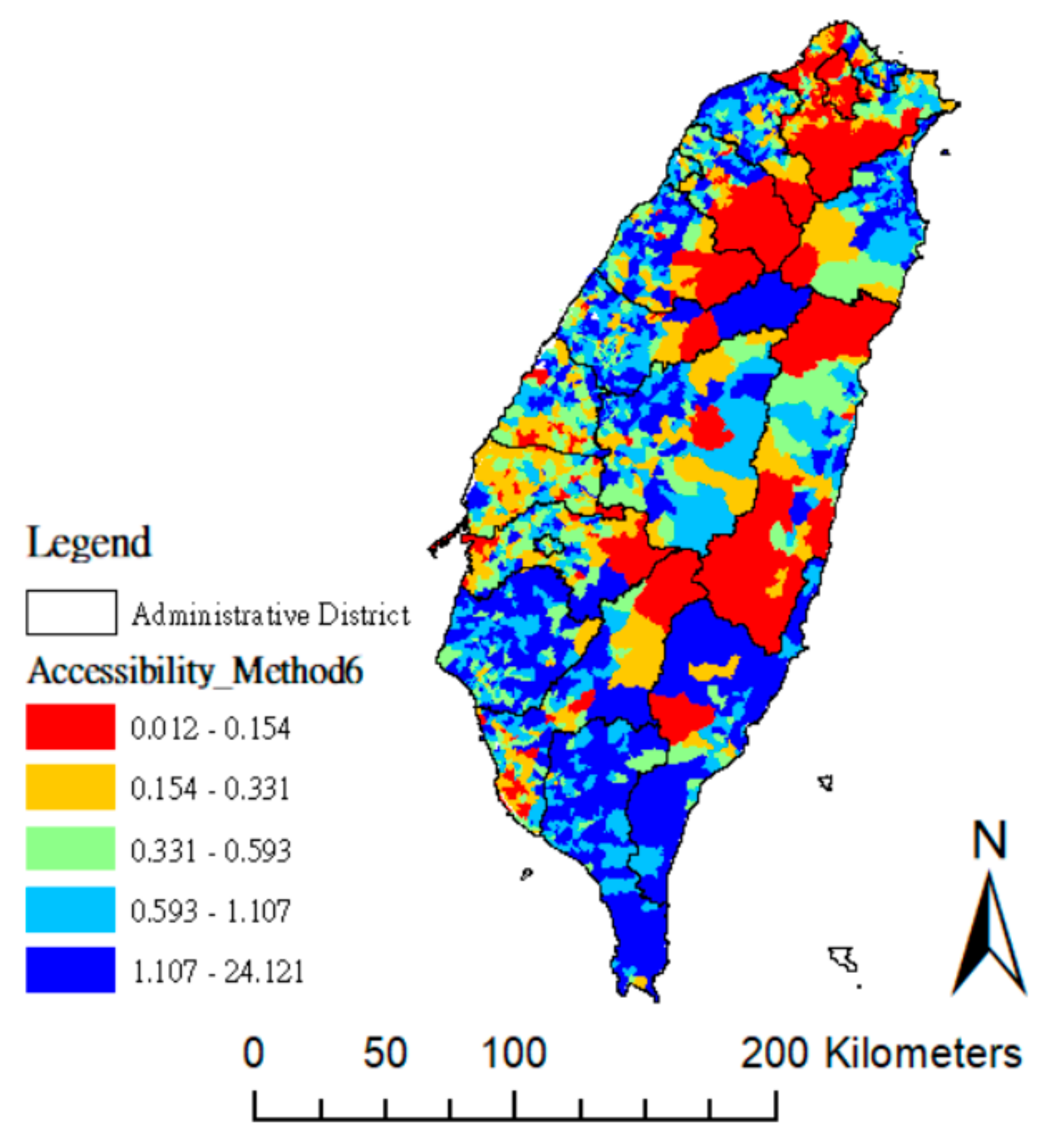
38]. Method M6 accounted for village population and supplier loading in calculating the accessibility of the nearest distance-decay. Method M6 presents a more realistic measure of accessibility, because it considers the elderly’s walkability and care in village-level neighborhood. Method M6 set 3 km as the appropriate nearest supplier’s distance. Considering that the elderly may decrease walking speed to rest, method M6 estimated about 60-min of walking time, and the nearest supplier’s road distance to the elderly was determined to be within 3 km. The distance-decay weight was set to one when the distance is within 3 km, and inversely varies the nearest distance after 3 km.
An extension to method M5, method M6 incorporated the elderly’s walkable distance, supplier loading, and the demand population in each village. Thus, the within-jurisdiction accessibility measure using method M6 provides the most comprehensive assessment of community care resources.
2.3. Domain Partition OD Cost Matrix Calculation Approach
In network-based geographical accessibility analysis, setting the searching distance is an important parameter in an origin-destination (OD) cost matrix calculation approach. Walsh, Cullinan, and Flannery [
31] examined the full study domain to consider all distance weights in their study; however, Cabrera-Barona, Blaschke, and Gaona [
32] used the maximum distance threshold of 1.2 km to identify supply services.
Under the existing public administrative system in Taiwan, the allocation of public service budgets is governed by county-level administrative units (such as the county-level governments), which often determines the service scope of resources, and qualified users of elderly community care resources are limited to the census-registered residents of each county. Therefore, the county-level administrative district is a suitable assessment unit with which to estimate the accessibility of community care resources in Taiwan. This study designated the administrative district as the county (or city), and each district has its own resource-searching distance.
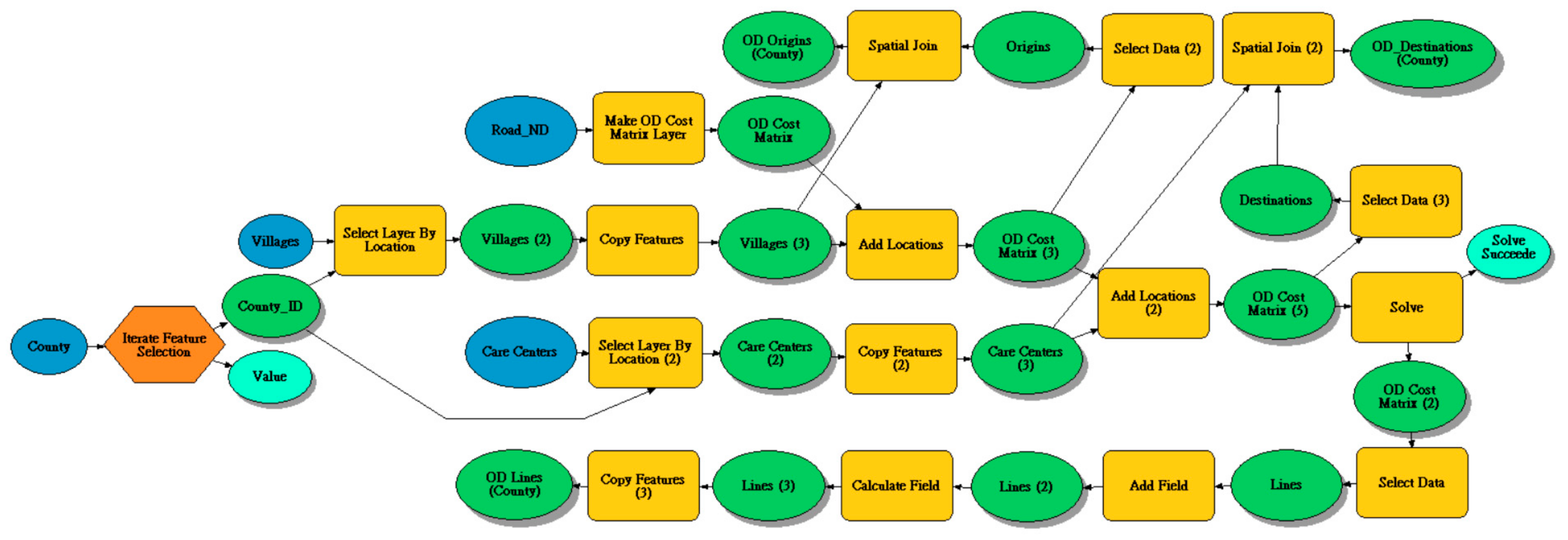
This study developed a domain partition OD cost matrix calculation approach (
Figure 1). First, we used the ESRI ArcGIS “Model Builder” (Esri, Redlands, CA, USA) programming to implement the domain partition algorithm for dividing the whole study area (Taiwan Main Island) into nineteen domains into county-level administrative districts to select within-jurisdiction feasible solutions. Then, we applied the ArcGIS “Network Analyst extension” to complete an origin–destination cost matrix calculation for each county. The within-jurisdiction feasible solution means that the accessibility calculation must meet practical policy restrictions for utilizing resources. That is, the elderly need to be residents registered in that specific region. Finally, we used Microsoft SQL Server 2014 to calculate the six geographic accessibility measurements.
2.4. Spatial Inequality Index of Elderly Community Care Resources
In addition to the accessibility of elderly community care resources, this study examined inequalities in elderly community care resource accessibility between counties by applying the Gini coefficient to compare geographic accessibility between administrative districts.
The Gini coefficient is a measure of statistical distribution that was first proposed as a measure of income or wealth inequality [
39] by showing the income distribution of a country’s population, and, often, it is applied to interpret relative deprivation in a society [
22,
40]. It measures inequality among values of a frequency distribution, whereby zero expresses perfect equality and one indicates maximal inequality.
Interpretation of the Gini coefficient is controversial, because it is a relative measure index. Its main disadvantage is its inability to explain different distributions with the same Gini coefficient. Therefore, we further calculated the scores of “median-mean” and “max-min” to show the range of distributions and disparities in each county.
To investigate the actual distribution in each administrative district, we used data drill-down techniques to deepen and, then, mine into the content of the datasets, accessing information by starting with a general category (the county-level Gini coefficient values) and moving through the hierarchy to calculate down to the village-level Gini coefficient distribution.







{kind=link}
{kind=link}
{kind=link}