Predictors of Participant Attendance Patterns in a Family-Based Intervention for Overweight and Obese Hispanic Adolescents

 , and
, and
Abstract
:1. Introduction
1.1. Intervention Attendance: Rates versus Patterns
1.2. Predictors of Participant Attendance
1.2.1. Individual-Level Predictors of Attendance
1.2.2. Family-Level Predictors of Attendance
1.2.3. Cultural Level Predictors of Attendance
1.3. Current Study and Hypotheses
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Intervention Description
2.4. Measures
2.4.1. Participant Attendance
2.4.2. Anthropometric Measures
2.4.3. Participant Self-Reported Measures
Demographics
Physical Activity
Fruit, Vegetable, and Added Sugar Intake
Positive Parenting
Parent–Adolescent Communication
Acculturation (Hispanicism, Americanism)
2.5. Data Analysis
3. Results
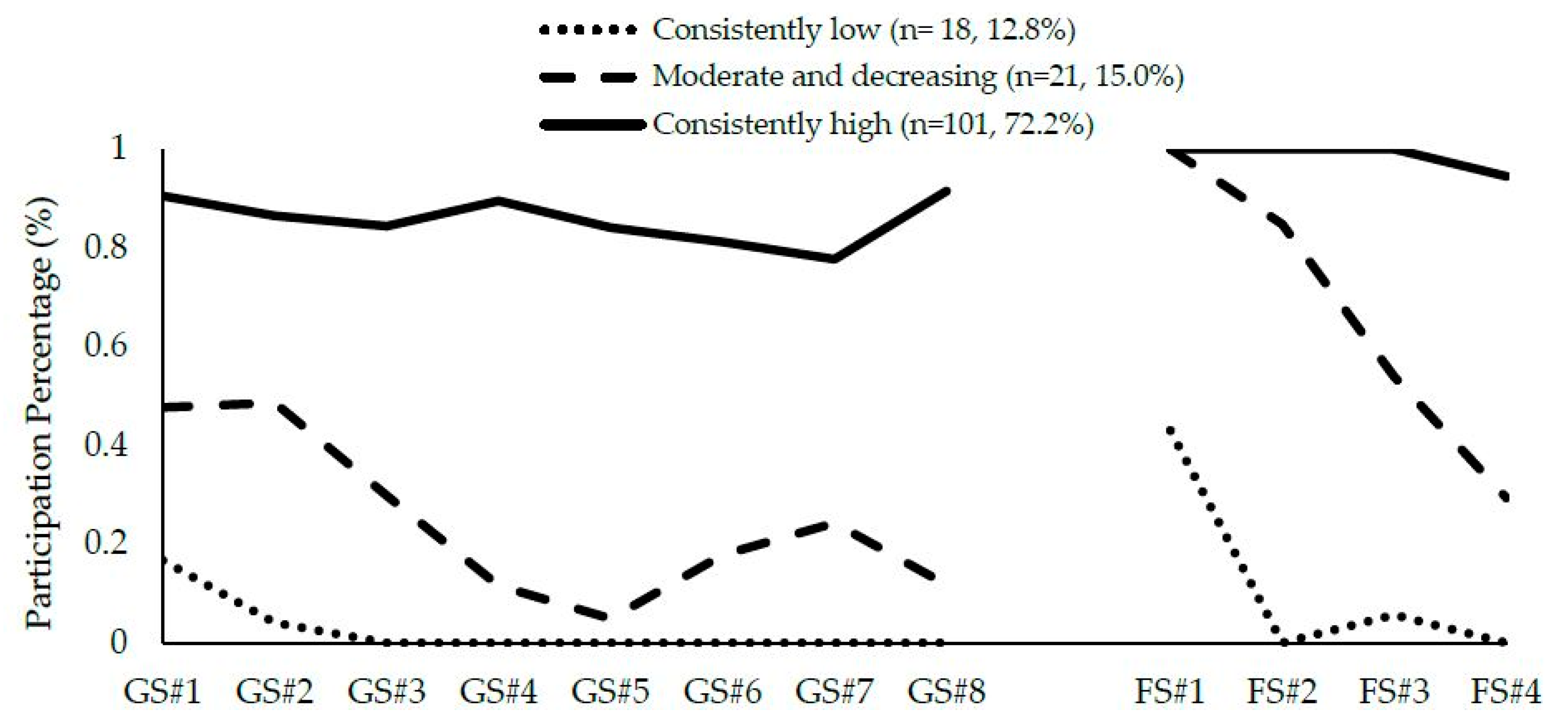
3.1. Identification and Interpretation of Participant Attendance Patterns
3.2. Predictors of Participant Attendance Patterns
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bauer, U.E.; Briss, P.A.; Goodman, R.A.; Bowman, B.A. Prevention of chronic disease in the 21st century: Elimination of the leading preventable causes of premature death and disability in the USA. Lancet 2014, 384, 45–52. [Google Scholar] [CrossRef]
- Sanderson, K.; Patton, G.C.; McKercher, C.; Dwyer, T.; Venn, A.J. Overweight and obesity in childhood and risk of mental disorder: A 20-year cohort study. Aust. N. Z. J. Psychiatry 2011, 45, 384–392. [Google Scholar] [CrossRef] [PubMed]
- Park, M.H.; Falconer, C.; Viner, R.A.; Kinra, S. The impact of childhood obesity on morbidity and mortality in adulthood: A systematic review. Obes. Rev. 2012, 13, 985–1000. [Google Scholar] [CrossRef] [PubMed]
- Umer, A.; Kelley, G.A.; Cottrell, L.E.; Giacobbi, P.; Innes, K.E.; Lilly, C.L. Childhood obesity and adult cardiovascular disease risk factors: A systematic review with meta-analysis. BMC Public Health 2017, 17, 683. [Google Scholar] [CrossRef] [PubMed]
- Skinner, A.C.; Ravanbakht, S.N.; Skelton, J.A.; Perrin, E.M.; Armstrong, S.C. Prevalence of obesity and severe obesity in US children, 1999–2016. Pediatrics 2018, 141, e20173459. [Google Scholar] [CrossRef] [PubMed]
- Fakhouri, T.H.; Hughes, J.P.; Brody, D.J.; Kit, B.K.; Ogden, C.L. Physical activity and screen-time viewing among elementary school–aged children in the United States from 2009 to 2010. JAMA Pediatr. 2013, 167, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Trost, S.G.; Mccoy, T.A.; Vander, S.V.; Mallya, G.; Duffy, M.L.; Foster, G.D. Physical activity patterns of inner-city elementary schoolchildren. Med. Sci. Sports Exerc. 2013, 45, 470–474. [Google Scholar] [CrossRef] [PubMed]
- Santiago-Torres, M.; Adams, A.K.; Carrel, A.L.; LaRowe, T.L.; Schoeller, D.A. Home food availability, parental dietary intake, and familial eating habits influence the diet quality of urban Hispanic children. Child. Obes. 2014, 10, 408–415. [Google Scholar] [CrossRef] [PubMed]
- U.S. Census Bureau. 2017 National Population Projections. Available online: https://www.census.gov/data/tables/2017/demo/popproj/2017-summary-tables.html (accessed on 19 March 2018).
- Resnick, M.D.; Bearman, P.S.; Blum, R.W.; Bauman, K.E.; Harris, K.M.; Jones, J.; Tabor, J.; Beuhring, T.; Sieving, R.E.; Shew, M. Protecting adolescents from harm: Findings from the National Longitudinal Study on Adolescent Health. JAMA 1997, 278, 823–832. [Google Scholar] [CrossRef] [PubMed]
- Bronfenbrenner, U. Ecology of the family as a context for human development: Research perspectives. Dev. Psychol. 1986, 22, 723–742. [Google Scholar] [CrossRef]
- Toro-Morn, M.I. Familismo. In Encyclopedia of Immigrant Health; Sajatovic, S.L.M., Ed.; Springer: New York, NY, USA, 2015; pp. 672–674. [Google Scholar]
- Leung, M.M.; Cavalcanti, O.B.; El Dada, A.; Brown, M.; Mateo, K.F.; Yeh, M.C. Treating obesity in Latino children: A systematic review of current interventions. Int. J. Child Health Nutr. 2017, 6, 1–15. [Google Scholar] [CrossRef]
- Berge, J.M.; Everts, J.C. Family-based interventions targeting childhood obesity: A meta-analysis. Child. Obes. 2011, 7, 110–121. [Google Scholar] [CrossRef] [PubMed]
- Kalarchian, M.A.; Levine, M.D.; Arslanian, S.A.; Ewing, L.J.; Houck, P.R.; Cheng, Y.; Ringham, R.M.; Sheets, C.A.; Marcus, M.D. Family-based treatment of severe pediatric obesity: Randomized, controlled trial. Pediatrics 2009, 124, 1060–1068. [Google Scholar] [CrossRef] [PubMed]
- Theim, K.R.; Sinton, M.M.; Goldschmidt, A.B.; Van Buren, D.J.; Doyle, A.C.; Saelens, B.E.; Stein, R.I.; Epstein, L.H.; Wilfley, D.E. Adherence to behavioral targets and treatment attendance during a pediatric weight control trial. Obesity 2013, 21, 394–397. [Google Scholar] [CrossRef] [PubMed]
- Lochrie, A.S.; Wysocki, T.; Hossain, J.; Milkes, A.; Antal, H.; Buckloh, L.; Canas, J.A.; Bobo, E.; Lang, J. The effects of a family-based intervention (FBI) for overweight/obese children on health and psychological functioning. Clin. Pract. Pediatr. Psychol. 2013, 1, 159–170. [Google Scholar] [CrossRef]
- Williams, N.A.; Coday, M.; Somes, G.; Tylavsky, F.A.; Richey, P.A.; Hare, M. Risk factors for poor attendance in a family-based pediatric obesity intervention program for young children. J. Dev. Behav. Pediatr. 2010, 31, 705–712. [Google Scholar] [CrossRef] [PubMed]
- De Niet, J.; Timman, R.; Jongejan, M.; Passchier, J.; van den Akker, E. Predictors of participant dropout at various stages of a pediatric lifestyle program. Pediatrics 2011, 127, e164–e170. [Google Scholar] [CrossRef] [PubMed]
- Walker, S.E.; Smolkin, M.E.; O’Leary, M.L.L.; Cluett, S.B.; Norwood, V.F.; DeBoer, M.D.; Gurka, M.J. Predictors of retention and BMI loss or stabilization in obese youth enrolled in a weight loss intervention. Obes. Res. Clin. Pract. 2012, 6, e330–e339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhaliwal, J.; Nosworthy, N.M.; Holt, N.L.; Zwaigenbaum, L.; Avis, J.L.; Rasquinha, A.; Ball, G.D. Attrition and the management of pediatric obesity: An integrative review. Child. Obes. 2014, 10, 461–473. [Google Scholar] [CrossRef] [PubMed]
- Ligthart, K.A.; Buitendijk, L.; Koes, B.W.; van Middelkoop, M. The association between ethnicity, socioeconomic status and compliance to pediatric weight-management interventions—A systematic review. Obes. Res. Clin. Pract. 2017, 11, 1–51. [Google Scholar] [CrossRef] [PubMed]
- Jensen, C.D.; Aylward, B.S.; Steele, R.G. Predictors of attendance in a practical clinical trial of two pediatric weight management interventions. Obesity 2012, 20, 2250–2256. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.L.; Lippevelde, W.; Magarey, A.; Moores, C.J.; Croyden, D.; Esdaile, E.; Daniels, L. Parent engagement and attendance in PEACH™ QLD—An up-scaled parent-led childhood obesity program. BMC Public Health 2017, 17, 559. [Google Scholar] [CrossRef] [PubMed]
- Mauricio, A.M.; Mazza, G.L.; Berkel, C.; Tein, J.-Y.; Sandler, I.N.; Wolchik, S.A.; Winslow, E. Attendance trajectory classes among divorced and separated mothers and fathers in the New Beginnings Program. Prev. Sci. 2018, 19, 620–629. [Google Scholar] [CrossRef] [PubMed]
- Mauricio, A.M.; Tein, J.-Y.; Gonzales, N.A.; Millsap, R.E.; Dumka, L.E.; Berkel, C. Participation patterns among Mexican–American parents enrolled in a universal intervention and their association with child externalizing outcomes. Am. J. Community Psychol. 2014, 54, 370–383. [Google Scholar] [CrossRef] [PubMed]
- Baker, C.N.; Arnold, D.H.; Meagher, S. Enrollment and attendance in a parent training prevention program for conduct problems. Prev. Sci. 2011, 12, 126–138. [Google Scholar] [CrossRef] [PubMed]
- Mauricio, A.M.; Tein, J.-Y.; Gonzales, N.A.; Millsap, R.E.; Dumka, L.E. Attendance patterns and links to non-response on child report of internalizing among Mexican-Americans randomized to a universal preventive intervention. Prev. Sci. 2018, 19, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Coatsworth, J.D.; Duncan, L.G.; Pantin, H.; Szapocznik, J. Patterns of retention in a preventive intervention with ethnic minority families. J. Prim. Prev. 2006, 27, 171–193. [Google Scholar] [CrossRef] [PubMed]
- Perrino, T.; Estrada, Y.; Huang, S.; George, S.S.; Pantin, H.; Cano, M.Á.; Lee, T.K.; Prado, G. Predictors of participation in an eHealth, family-based preventive intervention for Hispanic youth. Prev. Sci. 2018, 19, 630–641. [Google Scholar] [CrossRef] [PubMed]
- Coatsworth, J.D.; Duncan, L.G.; Pantin, H.; Szapocznik, J. Differential predictors of African American and Hispanic parent retention in a family-focused preventive intervention. Fam. Relat. 2006, 55, 240–251. [Google Scholar] [CrossRef] [PubMed]
- Szapocznik, J.; Coatsworth, J.D. An ecodevelopmental framework for organizing the influences on drug abuse: A developmental model of risk and protection. In Drug Abuse: Origins & Interventions; Glantz, M.D., Hartel, C.R., Eds.; American Psychological Association: Washington, DC, USA, 1999; pp. 331–366. [Google Scholar]
- Bronfenbrenner, U. The Ecology of Human Development: Experiments by Design and Nature; Harvard University Press: Cambridge, MA, USA, 1979. [Google Scholar]
- Zeller, M.; Kirk, S.; Claytor, R.; Khoury, P.; Grieme, J.; Santangelo, M.; Daniels, S. Predictors of attrition from a pediatric weight management program. J. Pediatr. 2004, 144, 466–470. [Google Scholar] [CrossRef] [PubMed]
- Welsby, D.; Nguyen, B.; O’Hara, B.J.; Innes-Hughes, C.; Bauman, A.; Hardy, L.L. Process evaluation of an up-scaled community based child obesity treatment program: NSW Go4Fun®. BMC Public Health 2014, 14, 140. [Google Scholar] [CrossRef] [PubMed]
- Fagg, J.; Cole, T.J.; Cummins, S.; Goldstein, H.; Morris, S.; Radley, D.; Sacher, P.; Law, C. After the RCT: Who comes to a family-based intervention for childhood overweight or obesity when it is implemented at scale in the community? J. Epidemiol. Community Health 2014. [Google Scholar] [CrossRef] [PubMed]
- Jelalian, E.; Hart, C.N.; Mehlenbeck, R.S.; Lloyd-Richardson, E.E.; Kaplan, J.D.; Flynn-O’Brien, K.T.; Wing, R.R. Predictors of attrition and weight loss in an adolescent weight control program. Obesity 2008, 16, 1318–1323. [Google Scholar] [CrossRef] [PubMed]
- Perrino, T.; Coatsworth, J.D.; Briones, E.; Pantin, H.; Szapocznik, J. Initial engagement in parent-centered preventive interventions: A family systems perspective. J. Prim. Prev. 2001, 22, 21–44. [Google Scholar] [CrossRef]
- Díaz, S.A.-H.; Díaz, S.A.-H.; Secades-Villa, R.; Errasti Pérez, J.M.; Fernández-Hermida, J.R.; García-Rodríguez, O.; Carballo Crespo, J.L. Family predictors of parent participation in an adolescent drug abuse prevention program. Drug Alcohol Rev. 2006, 25, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Bamberger, K.T.; Coatsworth, J.D.; Fosco, G.M.; Ram, N. Change in participant engagement during a family-based preventive intervention: Ups and downs with time and tension. J. Fam. Psychol. 2014, 28, 811–820. [Google Scholar] [CrossRef] [PubMed]
- Prado, G.; Pantin, H.; Schwartz, S.J.; Lupei, N.S.; Szapocznik, J. Predictors of engagement and retention into a parent-centered, ecodevelopmental HIV preventive intervention for Hispanic adolescents and their families. J. Pediatr. Psychol. 2006, 31, 874–890. [Google Scholar] [CrossRef] [PubMed]
- Connell, A.M.; Dishion, T.J.; Yasui, M.; Kavanagh, K. An adaptive approach to family intervention: Linking engagement in family-centered intervention to reductions in adolescent problem behavior. J. Consult. Clin. Psychol. 2007, 75, 568–579. [Google Scholar] [CrossRef] [PubMed]
- Gorman-Smith, D.; Tolan, P.H.; Henry, D.B.; Leventhal, A.; Schoeny, M.; Lutovsky, K.; Quintana, E. Predictors of participation in a family-focused preventive intervention for substance use. Psychol. Addict. Behav. 2002, 16, S55–S64. [Google Scholar] [CrossRef] [PubMed]
- Dillman Carpentier, F.R.; Mauricio, A.M.; Gonzales, N.A.; Millsap, R.E.; Meza, C.M.; Dumka, L.E.; Germán, M.; Genalo, M.T. Engaging Mexican origin families in a school-based preventive intervention. J. Prim. Prev. 2007, 28, 521–546. [Google Scholar] [CrossRef] [PubMed]
- St. George, S.M.; Messiah, S.E.; Sardinas, K.M.; Poma, S.; Lebron, C.; Tapia, M.I.; Velazquez, M.R.; Pantin, H.; Prado, G. Familias Unidas for Health and Wellness: Adapting an evidence-based substance use and sexual risk behavior intervention for obesity prevention in Hispanic adolescents. J. Prim. Prev. 2018, in press. [Google Scholar]
- Kuczmarski, R.J.; Ogden, C.L.; Guo, S.S.; Grummer-Strawn, L.M.; Flegal, K.M.; Mei, Z.; Wei, Z.; Curtin, L.R.; Roche, A.F.; Johnson, C.L. 2000 CDC growth charts for the United States: Methods and development. Vital Health Stat. Ser. 11 Data Natl. Health Surv. 2002, 246, 1–190. [Google Scholar]
- Stunkard, A.J.; Sorensen, T.; Schulsinger, F. Use of Danish adoption register for the study of obesity and thinness. In The Genetics of Neurological and Psychiatric Disorders; Kety, S., Sidman, R.L., Matthysse, S.W., Eds.; Raven: New York, NY, USA, 1983; pp. 115–120. [Google Scholar]
- Wei, L.; Lachin, J.M. Properties of the urn randomization in clinical trials. Control. Clin. Trials 1988, 9, 345–364. [Google Scholar] [CrossRef]
- Prado, G.; Pantin, H.; Briones, E.; Schwartz, S.J.; Feaster, D.; Huang, S.; Sullivan, S.; Tapia, M.I.; Sabillon, E.; Lopez, B.; et al. A randomized controlled trial of a parent-centered intervention in preventing substance use and HIV risk behaviors in Hispanic adolescents. J. Consult. Clin. Psychol. 2007, 75, 914–926. [Google Scholar] [CrossRef] [PubMed]
- Prado, G.; Pantin, H. Reducing substance use and HIV health disparities among Hispanic youth in the USA: The Familias Unidas program of research. Interv. Psicosoc. 2011, 20, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Estrada, Y.; Lee, T.K.; Huang, S.; Tapia, M.I.; Velázquez, M.-R.; Martinez, M.J.; Pantin, H.; Ocasio, M.A.; Vidot, D.C.; Molleda, L. Parent-centered prevention of risky behaviors among Hispanic youths in Florida. Am. J. Public Health 2017, 107, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; McKenzie, T.L.; Alcaraz, J.E.; Kolody, B.; Faucette, N.; Hovell, M.F. The effects of a 2-year physical education program (SPARK) on physical activity and fitness in elementary school students. Sports, Play and Active Recreation for Kids. Am. J. Public Health 1997, 87, 1328–1334. [Google Scholar] [CrossRef] [PubMed]
- Metzger, D.S.; Koblin, B.; Turner, C.; Navaline, H.; Valenti, F.; Holte, S.; Gross, M.; Sheon, A.; Miller, H.; Cooley, P. Randomized controlled trial of audio computer-assisted self-interviewing: Utility and acceptability in longitudinal studies. Am. J. Epidemiol. 2000, 152, 99–106. [Google Scholar] [CrossRef] [PubMed]
- NHANES (National Health and Nutrition Examination Survey). 2011–2012 National Health and Nutrition Examination Survey—Physical Activity and Physical Fitness Questionnaire. Available online: https://www.cdc.gov/nchs/data/nhanes/nhanes_11_12/paq.pdf (accessed on 17 October 2014).
- National Cancer Institute. Dietary Screener Questionnaire (DSQ) Website: Updated February 2018. Available online: http://riskfactor.cancer.gov/studies/nhanes/dietscreen/questionnaires.html (accessed on 22 March 2018).
- Thompson, F.E.; Midthune, D.; Kahle, L.; Dodd, K.W. Development and evaluation of the National Cancer Institute’s Dietary Screener Questionnaire scoring algorithms. J. Nutr. 2017, 147, 1226–1233. [Google Scholar] [CrossRef] [PubMed]
- Gorman-Smith, D.; Tolan, P.H.; Zelli, A.; Huesmann, L.R. The relation of family functioning to violence among inner-city minority youths. J. Fam. Psychol. 1996, 10, 115–129. [Google Scholar] [CrossRef]
- Barnes, H.L.; Olson, D.H. Parent-adolescent communication and the circumplex model. Child. Dev. 1985, 56, 438–447. [Google Scholar] [CrossRef]
- Zane, N.; Mak, W. Major approaches in the measurement of acculturation among ethnic minority populations: A content analysis and an alternative empirical strategy. In Acculturation: Advances in Theory, Measurement, and Applied Research; Chun, K., Organista, P.B., Marin, G., Eds.; American Psychological Association: Washington, DC, USA, 2003; pp. 39–60. [Google Scholar]
- Collins, L.M.; Lanza, S.T. Latent Class and Latent Transition Analysis: With Applications in the Social, Behavioral, and Health Sciences; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2013. [Google Scholar]
- Feldman, B.J.; Maysn, K.E.; Conger, R.D. New approaches to studying problem behaviors: A comparison of methods for modeling longitudinal, categorical adolescent drinking data. Dev. Psychol. 2009, 45, 652–676. [Google Scholar] [CrossRef] [PubMed]
- Nylund, K.L.; Asparouhov, T.; Muthen, B.O. Deciding on the number of classes in latent class analysis and growth mixture modeling: A Monte Carlo simulation study. Struct. Equ. Model. 2007, 14, 535–569. [Google Scholar] [CrossRef]
- Nagin, D.S. Group Based Modeling of Development; Harvard University Press: Cambridge, MA, USA, 2005. [Google Scholar]
- Muthén, B. Latent variable mixture modeling. In Advanced Structural Equation Modeling: New Developments and Techniques; Marcoulides, G.A., Schumacker, R.E., Eds.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 2000; pp. 1–33. [Google Scholar]
- Andruff, H.; Carraro, N.; Thompson, A.; Gaudreau, P. Latent class growth modelling: A tutorial. Tutor. Quant. Methods Psychol. 2009, 5, 11–24. [Google Scholar] [CrossRef]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 7th ed.; Muthén & Muthén: Los Angeles, CA, USA, 1998–2012. [Google Scholar]
- Kelleher, E.; Davoren, M.P.; Harrington, J.M.; Shiely, F.; Perry, I.J.; McHugh, S.M. Barriers and facilitators to initial and continued attendance at community-based lifestyle programmes among families of overweight and obese children: A systematic review. Obes. Rev. 2017, 18, 183–194. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, S.J.; Unger, J.B.; Zamboanga, B.L.; Szapocznik, J. Rethinking the concept of acculturation: Implications for theory and research. Am. Psychol. 2010, 65, 237–251. [Google Scholar] [CrossRef] [PubMed]
- Tapia, M.I.; Schwartz, S.J.; Prado, G.; Lopez, B.; Pantin, H. Parent-centered intervention: A practical approach for preventing drug abuse in Hispanic adolescents. Res. Soc. Work Pract. 2006, 16, 146–165. [Google Scholar] [CrossRef]
- Coatsworth, J.D.; Hemady, K.T.; George, M.W. Predictors of Group Leaders’ Perceptions of Parents’ Initial and Dynamic Engagement in a Family Preventive Intervention. Prev. Sci. 2018, 19, 609–619. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Intervention Condition (n = 140) |
|---|---|
| Adolescents | |
| Female, n (%) | 69 (49.3%) |
| Age, M ± SD | 13.04 ± 0.87 |
| Country of Origin/Birth, n (%) | |
| US | 85 (60.7%) |
| Cuba | 29 (20.7%) |
| Honduras | 3 (2.1%) |
| Venezuela | 5 (3.6%) |
| Others | 18 (12.9%) |
| BMI (kg/m2), M ± SD | 28.29 ± 4.44 |
| BMI percentile, M ± SD | 95.28 ± 3.67 |
| Weight Status, n (%) | |
| Overweight (BMI percentile 85th–95th) | 50 (35.7%) |
| Obese (BMI percentile ≥ 95th) | 90 (64.3%) |
| Parents | |
| Female, n (%) | 122 (87.1%) |
| Age, M ± SD | 42.09 ± 6.30 |
| Country of Origin/Birth, n (%) | |
| US | 14 (10.0%) |
| Cuba | 50 (35.7%) |
| Nicaragua | 17 (12.1%) |
| Honduras | 17 (12.1%) |
| Others | 42 (30.0%) |
| BMI (kg/m2), M ± SD | 30.99 ± 6.14 |
| Weight Status, n (%) | |
| Normal weight (BMI 18.5–24.9) | 18 (12.9%) |
| Overweight (BMI 25–29.9) | 48 (34.3%) |
| Obese (BMI ≥ 30) | 73 (52.1%) |
| Unknown | 1 (0.7%) |
| Marital Status, n (%) | |
| Partnered | 112 (80.0%) |
| Unpartnered | 28 (20.0%) |
| Full-time employment, n (%) | 72 (51.4%) |
| Annual Income, n (%) | |
| <$30,000 | 84 (60.0%) |
| $30,000–$49,999 | 29 (20.7%) |
| ≥$50,000 | 21 (15.0%) |
| Not reported | 6 (4.3%) |
| Session | Session Topic | Activities |
|---|---|---|
| Family Session 1 | Engagement and Orientation | Discussion on helping parents protect adolescents from health risks (e.g., diabetes, heart disease) and risky behaviors |
| Group Session 1 | Parent Involvement in Adolescent Worlds |
|
| Group Session 2 | Communication |
|
| Family Session 2 | Family Communication | Guided discussions and role plays about adolescent lifestyle behaviors and risky behaviors |
| Group Session 3 | Behavior Management |
|
| Group Session 4 | Monitoring of Peers |
|
| Group Session 5 | Substance Use and Other Unhealthy Behaviors |
|
| Family Session 3 | Monitoring of Peers and Unhealthy Behaviors | Guided discussions and role plays about substance use and other unhealthy behaviors |
| Group Session 6 | Parental Investment in School World |
|
| Group Session 7 | Adolescent Risky Sexual Behavior and HIV |
|
| Family Session 4 | Adolescent Risky Sexual Behavior and HIV | Guided discussions and role plays about adolescent risky sex |
| Group Session 8 | Prevention Every Day |
|
| Number of Classes | AIC | BIC | SABIC | Adj. LMR-LRT (p-Value) | Entropy | Class Size | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | ||||||
| 1 | 1960.95 | 1996.25 | 1958.28 | 140 | ||||||
| 2 | 1356.58 | 1430.12 | 1351.03 | 620.704 (0.00) | 0.98 | 103 | 37 | |||
| 3 | 1335.11 | 1431.58 | 1311.35 | 61.82 (0.01) | 0.97 | 101 | 21 | 18 | ||
| 4 | 1319.79 | 1455.72 | 1326.00 | 19.34 (0.09) | 0.97 | 100 | 17 | 12 | 11 | |
| 5 | 1315.30 | 1474.15 | 1303.30 | 16.97 (0.17) | 0.89 | 52 | 48 | 17 | 12 | 11 |
| Variables | Total Sample n = 140 | Consistently Low a n = 18 | Moderate and Decreasing b n = 21 | Consistently High c n = 101 | F- or χ2 Value, df = 2 (Post-Hoc Test) |
|---|---|---|---|---|---|
| Adolescents | |||||
| Female (vs male) | 69 (49.3%) | 9 (50.0%) | 12 (57.1%) | 48 (47.5%) | 0.65 |
| BMI %ile | 95.27 (3.67) | 94.97 (4.01) | 94.93 (4.31) | 95.40 (3.49) | 0.21 |
| Physical activity (days/week d) | 3.71 (2.37) | 4.17 (1.68) | 3.86 (2.53) | 3.58 (2.44) | 0.51 |
| Fruit and vegetable intake (cups/day) | 1.71 (0.61) | 1.65 (0.53) | 1.60 (0.63) | 1.75 (0.63) | 0.61 |
| Sugar intake (tsp/day) | 3.89 (1.66) | 4.46 (1.69) | 3.64 (1.33) | 3.83 (1.70) | 1.35 |
| Positive parenting | 21.03 (5.22) | 23.61 (4.36) | 21.57 (5.90) | 20.44 (5.10) | 3.02 |
| Parent–adolescent communication | 75.21 (12.45) | 76.55 (12.54) | 76.70 (14.49) | 74.64 (12.06) | 0.35 |
| Hispanicism | 37.94 (8.74) | 41.50 (8.24) | 40.19 (8.24) | 36.84 (8.56) | 3.07 * (c < a = b) p = 0.036 |
| Americanism | 48.03 (6.88) | 49.94 (5.80) | 48.71 (7.06) | 47 .52 (7.00) | 1.06 |
| Parents | |||||
| Education | 12.47 (3.18) | 12.38 (3.43) | 12.47 (2.50) | 12.49 (3.29) | 0.01 |
| Annual Household Income (<$25,000) | 73 (54.5%) | 10 (58.8%) | 9 (42.9%) | 54 (56.3%) | 1.39 |
| Partnered (vs unpartnered) | 80 (57.1%) | 9 (50.0%) | 9 (42.9%) | 62 (61.4%) | 2.87 |
| Body mass index (BMI) | 30.99 (6.14) | 30.23 (5.04) | 30.66 (6.34) | 31.20 (6.31) | 0.22 |
| Physical activity (days/week d) | 3.48 (2.51) | 3.59 (2.37) | 3.90 (2.27) | 3.37 (2.59) | 0.38 |
| Fruit and vegetable intake (cups/day) | 2.67 (1.34) | 2.74 (1.27) | 3.19 (1.52) | 2.56 (1.31) | 1.89 |
| Sugar intake (tsp/day) | 14.66 (11.47) | 18.79 (20.01) | 15.59 (12.18) | 13.74 (9.01) | 1.57 |
| Positive parenting | 24.05 (4.29) | 24.72 (4.68) | 25.15 (3.78) | 23.72 (4.31) | 1.17 |
| Parent–adolescent communication | 78.13 (10.98) | 75.83 (9.83) | 83.10 (9.19) | 77.55 (11.31) | 2.64 |
| Hispanicism | 48.52 (5.98) | 51.67 (4.27) | 46.71 (7.94) | 48.42 (5.66) | 2.80 |
| Americanism | 36.92 (11.99) | 37.08 (12.70) | 43.42 (10.73) | 35.54 (11.78) | 3.91 * (c < b = a) p = 0.006 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
St. George, S.M.; Petrova, M.; Kyoung Lee, T.; Sardinas, K.M.; Kobayashi, M.A.; Messiah, S.E.; Prado, G. Predictors of Participant Attendance Patterns in a Family-Based Intervention for Overweight and Obese Hispanic Adolescents. Int. J. Environ. Res. Public Health 2018, 15, 1482. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15071482
St. George SM, Petrova M, Kyoung Lee T, Sardinas KM, Kobayashi MA, Messiah SE, Prado G. Predictors of Participant Attendance Patterns in a Family-Based Intervention for Overweight and Obese Hispanic Adolescents. International Journal of Environmental Research and Public Health. 2018; 15(7):1482. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15071482
Chicago/Turabian StyleSt. George, Sara M., Mariya Petrova, Tae Kyoung Lee, Krystal M. Sardinas, Marissa A. Kobayashi, Sarah E. Messiah, and Guillermo Prado. 2018. "Predictors of Participant Attendance Patterns in a Family-Based Intervention for Overweight and Obese Hispanic Adolescents" International Journal of Environmental Research and Public Health 15, no. 7: 1482. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph15071482